

Abstract
Aim
Stonefish, known in Japan as “Oni‐daruma‐okoze” (Synanceia verrucosa Block et Schneider), inhabit the waters surrounding the Okinawa/Amami districts. By far, habubites have been limited to these areas mainly due to climatic conditions. Due to changes promoted by global warming and increasing tourism, concerns regarding the potential for stonefish envenomation as well as jellyfish stings on the main island of Japan are increasing. However, few studies of stonefish envenomation have been reported in Japan. The current study aimed to comprehensively examine for the first time the clinical characteristics of stonefish envenomation in Japan.
Methods
We administered retrospective questionnaire surveys between January 2013 and December 2017 to determine patient characteristics, treatment, and clinical outcomes of stonefish envenomation. We compared patient characteristics between tourists and non‐tourists.
Results
Over the 5‐year study period, 15 patients were identified from four hospitals. More than 70% of stonefish envenomation cases occurred in the northern part of Okinawa Main Island. All patients recovered well, including four patients with severe stonefish envenomation. In two severe cases, the length of hospitalization was more than 1 week (8–9 days). Antivenom was not given. There were no significant differences between tourists and non‐tourists with regard to baseline characteristics.
Conclusions
During a 5‐year period, 15 cases of stonefish envenomation occurred in Japan. The patients recovered well without treatment with antivenom.
Keywords: Antivenin, climate, Japan, survey, toxins
During a 5‐year period, 15 cases of stonefish envenomation occurred in Japan. The patients recovered well without treatment with antivenom.
![]()
Introduction
Stonefish are venomous and can cause severe injury. They are primarily found in the coastal waters of the Indo‐Pacific region, including the USA, Australia, Malaysia, Hong Kong, and Singapore.1, 2, 3, 4, 5 In Japan, stonefish, also termed “Oni‐daruma‐okoze” (Synanceia verrucosa Block et Schneider) (Fig. 1), inhabit the waters surrounding the Okinawa/Amami districts located in the southern part of Japan. The species has been limited to these areas mainly due to climatic conditions. Due to changes promoted by global warming and increasing tourism, concerns regarding the potential for stonefish envenomation as well as jellyfish stings on the main island of Japan are increasing.6, 7, 8
Figure 1.

Synanceia verrucosa Block et Schneider. Photograph courtesy of Okinawa Prefectural Institute of Health and Environment, Japan
However, few studies of stonefish envenomation have been reported in Japan,9, 10 and studies comprehensively examining the clinical characteristics are limited. Therefore, physicians in the emergency department have limited information with regard to stonefish envenomation.
Thus, the current study aimed to examine for the first time the clinical characteristics of stonefish envenomation in Japan and determine the clinical characteristics of stonefish envenomation among tourists.
Methods
The institutional review board of St. Luke’s International Hospital (Tokyo, Japan) has approved this cross‐sectional, survey‐based study (approval no. 18‐R052).
Patients and setting
We prepared a questionnaire to examine the clinical characteristics of stonefish envenomation in Japan. The questionnaire comprised basic and advanced (1 and 2) items. The basic questionnaire was distributed to four medical institutions (Okinawa Main Island: Okinawa Prefectural Chubu Hospital, Okinawa Prefectural Hokubu Hospital, and Northern Okinawa Medical Center; and other areas: Okinawa Prefectural Yaeyama Hospital) originally listed in reports from the Okinawa Prefectural Government.11 The basic questionnaire was distributed in February 2019 and collected by March 2019.8 The advanced questionnaire 1 was distributed to two hospitals that had treated patients with severe stonefish envenomation, as stated in the basic questionnaire. The advanced questionnaire 1 was distributed in May 2019 and collected by July 2019. The advanced questionnaire 2 was distributed to four hospitals that had treated patients with mild‐to‐moderate stonefish envenomation, as stated in the basic questionnaire. The questionnaire was distributed in August 2019 and collected by September 2019.
The surveillance period of the questionnaire spanned 5 years, from January 2013 to December 2017 (Fig. 2).
Figure 2.
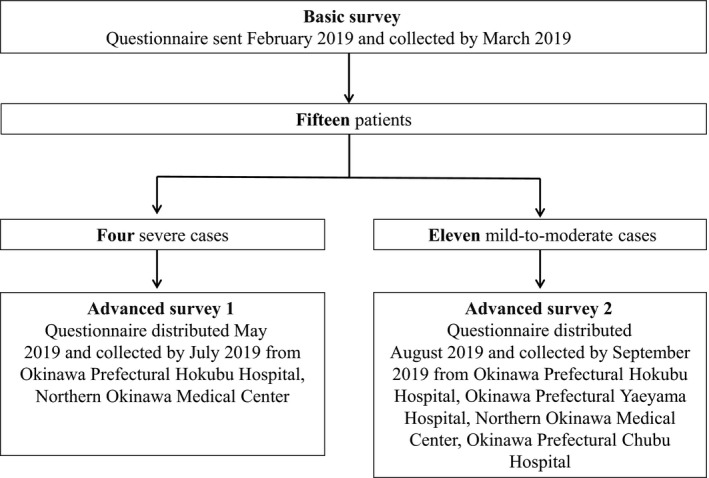
Flowchart of the enrolment of study participants in Okinawa Prefecture, Japan, 2013–2017.
Data collection
In the basic questionnaire, the following parameters were recorded: age, sex, severity, date of injury, and hospital name. In advanced questionnaires 1 and 2, the following parameters were recorded: age, sex, severity, date of injury, time interval from sting to hospital arrival, department visited, prehospital management (immersion in hot water), vital signs (systolic blood pressure and heart rate), clinical symptoms (local pain, swelling, and numbness), in‐hospital management (analgesics, tetanus vaccination, and antivenom), and clinical outcomes (hospital admission and recovery rate).
Diagnosis of stonefish envenomation
Currently, there are no definitive diagnostic criteria for stonefish envenomation. The diagnosis of stonefish envenomation is based on the patient’s history or the positive identification of stonefish presented by the patient.
Severity of stonefish envenomation
We defined the severity of stonefish envenomation as follows: (i) mild stings limited to local envenomation, with local symptoms confined to mild pain and swelling at the sting site; (ii) moderate stings resulted in moderate pain and swelling at the sting site, but rarely required admission to hospital; and (iii) severe stings resulted in systemic envenomation (e.g., anaphylaxis) and in most cases required hospital admission.
Definition of tourists
Tourists are defined as individuals residing outside Okinawa.
Location of hospitals that had treated patients with mild‐to‐severe stonefish envenomation
The location of hospitals that had treated patients with mild‐to‐severe stonefish envenomation, as stated in the basic questionnaire, are shown in Figure 3. Okinawa Main Island: Okinawa Prefectural Chubu Hospital, Okinawa Prefectural Hokubu Hospital, Northern Okinawa Medical Center. Other areas: Okinawa Prefectural Yaeyama Hospital.
Figure 3.
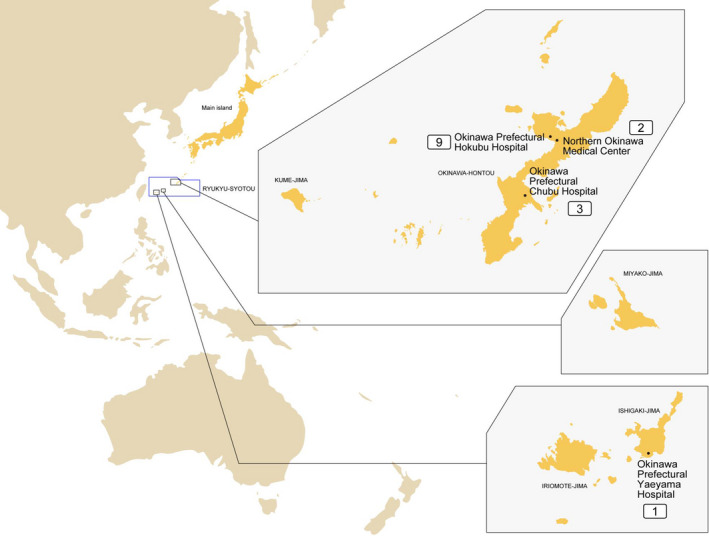
Distribution of stonefish envenomation cases in Okinawa Prefecture, Japan, 2013–2017. Numbers indicate the number of stonefish envenomation cases.
Study end‐points
The primary end‐point of the present study was to determine the clinical characteristics of stonefish envenomation.
Primary data analysis
Patient characteristics, treatment‐related factors, and clinical outcomes were compared between the tourist and non‐tourist groups using the Mann–Whitney U‐test and Fisher’s exact tests for categorical variables, as appropriate. Comparison of the severity of stonefish envenomation between tourists and non‐tourists was carried out using Pearson’s χ2‐test. Two‐tailed P‐values ≤0.05 denoted statistical significance. Statistical analysis was undertaken using JMP version 11 software (SAS, Cary, NC, USA).
Results
Baseline characteristics of the study population
Over the 5‐year study period, 15 patients were identified from four hospitals based on the basic questionnaire. The patient characteristics are summarized in Table 1; 80.0% were males, and the median age was 21 years. Nine patients (60%) developed mild symptoms, and four patients (26.7%) suffered severe envenomation. Four patients (26.7%) received prehospital immersion in hot water.
Table 1.
Baseline characteristics of patients affected by stonefish envenomation in Okinawa Prefecture, Japan, 2013–2017
| Variable | n = 15 |
|---|---|
| Age (years) | 21 (15–50) |
| Gender, male (%) | 12 (80.0) |
| Date of injury (year) | |
| 2013 | 4 (26.6) |
| 2014 | 5 (33.4) |
| 2015 | 2 (13.3) |
| 2016 | 2 (13.3) |
| 2017 | 2 (13.3) |
| Severity of stonefish envenomation | |
| Mild | 9 (60.0) |
| Moderate | 2 (13.3) |
| Severe | 4 (26.7) |
| Hospital | |
| Okinawa Main Island (Okinawa Prefectural Chubu Hospital, Okinawa Prefectural Hokubu Hospital, Northern Okinawa Medical Center) | 14 (93.3) |
| Others (Okinawa Prefectural Yaeyama Hospital) | 1 (6.7) |
| Prehospital management | |
| Immersion in hot water | 4 (26.7) |
Data are expressed as number (%), or median (interquartile range).
The distribution of cases with stonefish envenomation is shown in Figure 3. Only one case developed outside of Okinawa Main Island. More than 70% (11/15) of stonefish envenomation cases occurred in the northern part of Okinawa Main Island.
Baseline characteristics and comparison between tourists and non‐tourists with stonefish envenomation
There were no significant differences observed between the two groups with regard to age, sex, severity, time from envenomation to hospital arrival, department visited, prehospital management, vital signs, symptoms, or in‐hospital management (Table 2). All patients recovered well, and antivenom was not given.
Table 2.
Baseline characteristics and comparison between tourist and non‐tourist patients with moderate‐to‐severe pain following stonefish envenomation in Okinawa Prefecture, Japan, 2013–2017
| Variable | Tourist patients (n = 8) | Non‐tourist patients (n = 7) | P‐value |
|---|---|---|---|
| Age (years) | 23 (11–39) | 21 (12–75) | 0.772 |
| Gender, male (%) | 5 (62.5) | 7 (100.0) | 0.200 |
| Severity of stonefish envenomation | |||
| Mild | 5 (62.5) | 4 (57.1) | 0.217 |
| Moderate | 3 (37.5) | 1 (14.3) | |
| Severe | 0 (0.0) | 2 (28.6) | |
| Time from sting to hospital arrival (h) | |||
| <1 | 4 (50.0) | 5 (71.4) | 0.240 |
| 1–3 | 4 (50.0) | 1 (14.3) | |
| 3–6 | 0 (0.0) | 1 (14.3) | |
| Department visited | |||
| Emergency medicine | 8 (100.0) | 7 (100.0) | 1.000 |
| Prehospital management | |||
| Immersion in hot water | 3 (37.5) | 1 (14.3) | 0.569 |
| Vital signs | |||
| SBP | 127 (121–140) | 143 (122–164) | 0.417 |
| HR | 80 (63–90) | 89 (72–95) | 0.246 |
| Symptoms | |||
| Local pain | 8 (100.0) | 4 (57.1) | 0.038 |
| Swelling | 4 (50.0) | 4 (57.1) | 1.000 |
| Numbness | 0 (0.0) | 3 (42.9) | 0.077 |
| In‐hospital management | |||
| Analgesics | 8 (100.0) | 5 (71.4) | 0.200 |
| Tetanus vaccine | 4 (50.0) | 4 (57.1) | 1.000 |
| Antivenom | 0 (0.0) | 0 (0.0) | 1.000 |
| Outcome | |||
| Hospital admission | 3 (37.5) | 1 (14.3) | 0.569 |
| Good recovery | 8 (100.0) | 7 (100.0) | 1.000 |
Tourists are defined as individuals residing outside Okinawa.
Data are expressed as number (percentage), or median (interquartile range).
HR, heart rate; SBP, systolic blood pressure.
Details of the four severe cases
The details of the severe cases of stonefish envenomation are shown in Table 3. In two cases, the length of hospitalization was more than 1 week (8–9 days); hyperbaric oxygen therapy was initiated in both cases.
Table 3.
Details of four severe cases of stonefish envenomation in Okinawa Prefecture, Japan
| Case | Age, years | Sex | Tourist | Site of injury | Time from sting to hospital arrival (h) | Immersion in hot water | Department visited | HR (/min) | SB (mmHg) | Local pain | Swelling | Numbness | Hospital admission | Length of hospitalization (days) | Length of ICU stay | In‐hospital treatment | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 21 | F | Yes | Foot | 1–3 | Yes | EM | 60 | 131 | Yes | Yes | No | Yes | 9 | 0 | Analgesics, antibiotics, HBO | GR |
| 2 | 12 | M | Yes | Foot | <1 | No | EM | 94 | 100 | No | No | No | Yes | 1 | 0 | Analgesics, antibiotics, tetanus vaccine, immersion in hot water | GR |
| 3 | 24 | F | No | Lower leg | <1 | No | EM | 88 | 139 | Yes | No | No | Yes | 8 | 0 | Analgesics, antibiotics, tetanus vaccine, immersion in hot water, HBO | GR |
| 4 | 28 | M | No | Foot | 1–3 | Yes | EM | 70 | 146 | Yes | No | No | Yes | 2 | 0 | Analgesics, antibiotics, tetanus vaccine, immersion in hot water | GR |
EM, emergency medicine; F, female; GR, good recovery; HBO, hyperbaric oxygen; HR, heart rate; ICU, intensive care unit; M, male; SBP, systolic blood pressure.
Discussion
The current study is the first to comprehensively describe the clinical characteristics of stonefish envenomation in Japan. In a report released by the Hong Kong Poison Information Center, a total of 32 cases were observed during a 10‐year period.5 Thus, the annual number of stonefish envenomation cases in the current study was similar to that reported in Hong Kong. However, a hospital in Singapore reported 30 cases during a 2‐year observation period2 (i.e., five‐fold higher incidence versus that reported in Japan). With regard to prehospital management, only 25% of the patients received prehospital immersion in hot water. In contrast, a study undertaken in Hong Kong reported prehospital immersion in hot water for all patients (100%).5 This suggests that there is an unmet need for public health interventions and appropriate prehospital management in Japan.
Unlike in our current examination of jellyfish stings in Japan,8 in the current study, there were no significant differences observed between tourist and non‐tourist groups with regard to baseline characteristics. A possible reason for this result could be that, owing to the severe pain caused by the stonefish venom verrucotoxin, patients (tourists and non‐tourists) tended to promptly visit the emergency department.
Although all patients recovered well without treatment with antivenom (i.e. antivenom was not available in Japan) in the current study, approximately 30% of patients developed a severe reaction that required admission to hospital (two cases required >1 week of hospitalization). Notably, two deaths related to stonefish envenomation have been reported in Japan.12 In the study undertaken in Hong Kong, 25% of patients received treatment with antivenom.5 The only commercially available fish antivenom is the stonefish antivenom produced by CSL (Melbourne, Australia). This antivenom consists of the purified F(ab)2 fragment of equine immunoglobulin G antibodies raised against the venom of S. trachynis.13 Considering the current clinical practice against stonefish envenomation in Japan, the preparation of antivenom might be necessary.
This study had several limitations. First, the sample size was too small to obtain robust conclusions. Second, details regarding dermatological examinations or long‐term dermatological outcomes were not studied, as the dataset was unavailable.14 Third, the difference between mild and moderate pain is subjective, and there is no distinct definition with regard to pain. Finally, cases occurring outside Okinawa Prefecture (i.e., mainland Japan) were not included in this analysis.
Conclusions
During a 5‐year period, 15 cases of stonefish envenomation occurred in Okinawa Prefecture. All patients recovered well without antivenom. More than 70% of stonefish envenomation cases occurred in the northern part of Okinawa Main Island. There were no significant differences observed with regard to baseline characteristics between tourists and non‐tourists.
Disclosure
Approval of the research protocol: The institutional review board of St. Luke’s International Hospital approved this cross‐sectional, survey‐based study (approval no. 18‐R052).
Informed consent: N/A.
Registry and registration no. of the study/trial: N/A.
Animal studies: N/A.
Conflict of interest: None.
Acknowledgments
We would like to thank all participants for enrolling and providing data for the study.
Funding information
This work was supported by the Japanese Society for Clinical Toxicology.
References
- 1. Tay TK, Chan HZ, Ahmad TS, Teh KK, Low TH, Wahab NA. Stonefish envenomation of hand with impending compartment syndrome. J. Occup. Med. Toxicol. 2016; 11: 23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Ngo SY, Ong SH, Ponampalam R. Stonefish envenomation presenting to a Singapore hospital. Singapore Med. J. 2009; 50: 506–9. [PubMed] [Google Scholar]
- 3. Prentice O, Fernandez WG, Luyber TJ, McMonicle TL, Simmons MD. Stonefish envenomation. Am. J. Emerg. Med. 2008; 26: 972 e1–2. [DOI] [PubMed] [Google Scholar]
- 4. Isbister GK. Venomous fish stings in tropical northern Australia. Am. J. Emerg. Med. 2001; 19: 561–5. [DOI] [PubMed] [Google Scholar]
- 5. Poon KM, Ng CHV, Tse Ml. A 10‐year retrospective review of stonefish sting injury in Hong Kong. Hong Kong J. Emerg. Med. 2019; 1–4. [Google Scholar]
- 6. Hifumi T. Treatments of venomous snake bites. Nihon Iji Shinpo. 2015; 4772: 56. [Google Scholar]
- 7. Haines A, Ebi K. The imperative for climate action to protect health. N. Engl. J. Med. 2019; 380: 263–73. [DOI] [PubMed] [Google Scholar]
- 8. Hifumi TFY, Otani N, Kondo Y, Kitamoto T, Kobayashi K, Nakaya N, Tomioka J. Clinical characteristics of jellyfish stings in Japan. Acute Med. Surg 2019; 7:e469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Yamamoto R, Suzuki M, Hori S, Aikawa N. Stonefish, "Okoze" envenomation during food preparation. Keio J. Med. 2010; 59: 19–22. [DOI] [PubMed] [Google Scholar]
- 10. Hashimoto A, Nakao A, Inoue T et al Incorrect first aid treatment information about stonefish envenomation on medical websites. Chudoku Kenkyu. 2013; 26: 292–4. [PubMed] [Google Scholar]
- 11. Government OP . Reports of Chiroplsalmus quadrigatus Hackel stings.
- 12. Azama YFY, Morine N, Tsuha A, Kudaka J. Injury cases by Marine Animals in Okinawa, Japan in 2012–2013. Okinawa Eisei kenkyujo‐Hou. 2016. 50: 33–7.
- 13. Church JE, Hodgson Wayne C. Stonefish (Synanceia trachynis) antivenom. In vitro efficacy and clinical use. J. Toxicol. Toxin Rev. 2003; 22: 69–76. [Google Scholar]
- 14. Dall GF, Barclay Kl, Knight D. Severe sequelae after stonefish envenomation. Surg. 2006; 4: 384–5. [DOI] [PubMed] [Google Scholar]