

Abstract
Background:
Cisplatin (Cis), carboplatin (Carb), and ifosfamide (Ifos) are common nephrotoxic chemotherapies. Biomarkers of tubular injury may allow for early acute kidney injury (AKI) diagnosis.
Procedure:
We performed a two-center (Canada, United States) pilot study to prospectively measure serum creatinine (SCr), urine neutrophil gelatinase-associated lipocalin (NGAL), and interleukin-18 (IL-18) in children receiving Cis/Carb (27 episodes), Ifos (30 episodes), and in 15 hospitalized, nonchemotherapy patients. We defined AKI using the Kidney Disease Improving Global Outcomes (KDIGO) definition. We compared postchemotherapy infusion NGAL and IL-18 concentrations (immediate postdose to 3 days later) to pre-infusion concentrations. We calculated area under the receiver operating characteristic curve (AUC) for postinfusion biomarkers to discriminate for AKI.
Results:
Prechemotherapy infusion NGAL and IL-18 concentrations were not higher than nonchemotherapy control concentrations. Increasing chemotherapy dose was associated with increasing postinfusion (0–4 hr after infusion) NGAL (P < 0.05). Post-Ifos, immediate postdose, and daily postdose NGAL and IL-18 were significantly higher than pre-infusion biomarker concentrations (P < 0.05), during AKI episodes. NGAL and IL-18 did not rise significantly after Cis–Carb infusion, relative to predose concentrations (P > 0.05). NGAL and IL-18 measured immediately after Ifos infusion discriminated for AKI with AUCs is 0.80 (standard error = 0.13) and 0.73 (standard error = 0.16), respectively. NGAL and IL-18 were not diagnostic of Cis–Carb-associated AKI. When AUCs were adjusted for age, all biomarker AUCs (Cis–Carb and Ifos) improved.
Conclusion:
Urine NGAL and IL-18 show promise as early AKI diagnostic tests in children treated with ifosfamide and may have a potential role in drug toxicity monitoring.
Keywords: acute kidney injury, carboplatin, cisplatin, ifosfamide, nephrotoxicity, urine biomarkers
1 |. INTRODUCTION
Acute kidney injury (AKI) is common and associated with morbidity and mortality in critically ill children.1,2 Nephrotoxicity is a common cause of pediatric AKI3 and has been shown to be associated with longer hospital stay and progression to chronic kidney disease.4
AKI during cancer treatment has been associated with increased mortality, long-term chronic kidney disease, and hypertension.5–7 Children treated for cancer are exposed to many nephrotoxins.8 Cisplatin (Cis), carboplatin (Carb), and ifosfamide (Ifos) are commonly used to treat solid tumors, and well known to cause AKI5–7 via renal tubular damage secondary to oxidative stress, vasoconstriction, and inflammation.9 Animal studies have identified several agents to treat AKI,10–12 which have not been translated to human AKI treatment.13 A barrier to performing AKI clinical therapeutic trials has been the lack of early diagnosis (earlier than serum creatinine [SCr]) and lack of specific biomarkers of AKI, which might allow for implementation of novel AKI therapies within the narrow AKI therapeutic window.14 SCr is a late functional, and not a tissue/structural, AKI biomarker, limiting its use for determining patient eligibility for clinical trials to limit nephrotoxicity, as well as its use as a specific nephrotoxicity marker in clinical care and drug development.
Urine neutrophil gelatinase-associated lipocalin (NGAL) and interleukin-18 (IL-18) are two of the most extensively studied biomarkers for early AKI diagnosis in pediatric cardiac surgery15 and critical illness populations.16–18 Both biomarkers are proteins extruded from injured proximal tubular cells into urine as a result of injury. NGAL is involved in tubular cell injury and repair and is an iron chelator19; IL-18 activates macrophages and mediates tubular cell inflammatory injury.20 Few human studies have evaluated new AKI biomarkers in Cis, Carb, or Ifos nephrotoxicity.21,22 Given previous research on NGAL and IL-18 and because Cis, Carb, and Ifos cause proximal tubular damage, they may potentially serve important roles in AKI prevention and treatment of Cis-Carb or Ifos-associated AKI, monitoring toxicity, or to risk-stratify for long-term renal damage. A first step in studying new biomarkers for chemotherapy nephrotoxicity is understanding excretion patterns during treatment and examine for evidence of AKI association.
We performed a pilot study to evaluate NGAL and IL-18 in children treated with Cis, Carb, and Ifos. We characterized their temporal excretion in relation to chemotherapy infusion and evaluated if they are associated with AKI development.
2 |. METHODS
2.1 |. Study design, setting, and patient selection
This was a two-center prospective observational cohort study conducted at the Montreal Children’s Hospital (MCH, Montreal, Canada) and Cincinnati Children’s Hospital Medical Center (CCHMC, Cincinnati, OH). Children less than 18 years old treated with at least one dose of Cis, Carb, or Ifos between September 2008 and March 2012 were eligible. The study was initiated later at CCHMC (enrollment between June 2011 and July 2012). Exclusion criteria were age less than 3 months (renal tubular immaturity), renal transplant or chronic dialysis, admitted for primary renal condition (including urinary infection), and treatment with nephrotoxins within 2 weeks before enrollment. A nonchemotherapy-treated hospitalized control group was also recruited, to determine if control (nonchemotherapy) biomarker concentrations were different from prechemotherapy infusion biomarker concentrations in study patients. Nonchemotherapy controls were 3 months to 18 years old, admitted for more than 48 hr to medical, surgical, or oncology wards, with no history of renal disease, who never received Cis, Carb, or Ifos, received no nephrotoxic medication during the admission or in the previous 2 weeks and did not develop AKI. Approval to conduct the study was obtained by institutional research ethics or review board before initiating study activities. Parents or guardians provided informed consent, with child assent when appropriate. Analysis and reporting were directed by guidelines outlined in the Strengthening the Reporting of Observational studies in Epidemiology statement.23
2.2 |. Recruitment
The research team was informed daily of patients initiating Cis, Carb, or Ifos by the hospital pharmacy and oncology clinics. Eligible patients were approached prior to or on the first day of a given chemotherapy infusion episode or cycle. Subjects were followed for up to 14 days of the admission associated with that infusion episode. Most patients’ overall cancer treatments consisted of several infusion episodes, or cycles (lasting one to several days), which were repeated at least one or more times, typically between 3 and 6 weeks apart. Patients could be recruited during any of their chemotherapy cycles and be recruited into the study more than once.
2.3 |. Clinical data collection
The following pretreatment variables were collected: demographic data, medical history/ diagnoses, admission reason, cancer type, medications before hospitalization, or study start. During treatment, the following variables were collected prospectively: drug details (e.g., doses, number of treatment days), height, weight, and use of other nephrotoxins. Length of stay, need for intensive care unit admission, infection (defined by positive blood culture and documentation), need for dialysis, and mortality were documented.
2.4 |. Biospecimen handling
In study drug (Cis, Carb, or Ifos) subjects, blood and urine were collected from before chemotherapy infusion (presample), immediately postinfusion (0–4 hr or “Day 1”) and then daily during the study episode hospitalization. Blood was collected simultaneous to routine blood work and fresh urine was collected by bladder catheter, midstream clean catch, or diaper cotton balls in infants. In nonchemotherapy controls, urine collected from the first 24 hr of study was used to compare biomarkers with chemotherapy-treated subjects; blood was obtained with routine blood work or additional testing. Urine and blood samples were centrifuged (2,000 rpm, 15 min, room temperature) and urine supernatant and serum were aliquoted/stored at −80°C.
2.5 |. Laboratory measurements
SCr was measured at the MCH central biochemistry laboratory using an isotope dilution mass spectrometry-traceable assay. Urine NGAL and IL-18 were measured at the CCHMC Biomarker Laboratory, Ohio.15 NGAL was measured by commercial enzyme-linked immunosorbent assay (ELISA) kit (Bioporto, Gentofte, Denmark). The average intra-/interassay coefficient of variations (CVs) were 2.5/6.3%. IL-18 was measured using an IL-18 ELISA kit (Medical & Biological Laboratories, Nagoya, Japan). Intra-/interassay CVs are 3–10%. Individuals performing biomarker measurements were blinded to clinical data.
2.6 |. AKI definition
AKI was defined based on the SCr criteria of the Kidney Disease Improving Global Outcomes (KDIGO) guideline.24 Urine output criteria of the KDIGO definition could not be evaluated, since most patients did not have urinary catheters or detailed urine records. Baseline SCr was defined as the lowest SCr in the 3 months before recruitment. If no baseline SCr was available, a normal estimated glomerular filtration rate (eGFR) = 120 ml/min/1.73 m2 was assumed, and SCr was back-calculated from the Chronic Kidney Disease in Children (CKiD) formula24,25; peak SCr during study was defined as the highest SCr value obtained during the study period after drug infusion (or admission for controls). AKI was defined as Stage 1 or 50% or higher rise in peak SCr from baseline (within 7 days) or absolute increase 26.5 μmol/l or more (within 48 hr); Stage 2 or doubling of peak SCr; Stage 3 or tripling of peak SCr from baseline, decrease in eGFR to less than 35 ml/min/1.73 m2 or need for dialysis.
2.7 |. Statistical analysis
Continuous variables were expressed as mean ± standard deviation (SD), median and compared between groups by Mann-Whitney test or Kruskal-Wallis test (more than two groups). Categorical variables were compared between groups using chi-square or Fisher exact tests, as appropriate.
Box plots of serial biomarker concentrations were derived to evaluate biomarker excretion post-Cis-Carb and post-Ifos infusion (pre-infusion, Day 1 or immediate postinfusion [0–4 hr], 24 hr [Day 2] postinfusion, Day 3 and Day 4). Mann-Whitney tests were used to evaluate if biomarkers after chemotherapy dose increased significantly from pre-infusion. Box plots of biomarker excretion were derived for AKI and non-AKI patients separately. Nonchemotherapy control biomarkers collected within the first 24 hr of study were compared to pre-infusion biomarker concentrations in study patients.
To evaluate for a chemotherapy dose—biomarker relation— chemotherapy first infusion dose (in mg/m2) was divided into tertiles and immediate postinfusion (Day 1) biomarker concentrations were compared across increasing dose tertiles (Kruskal-Wallis test). Spearman correlation analysis was used to evaluate the relation between chemotherapy dose (mg/m2) and immediate postdose biomarker concentrations. Carb-treated subjects were not included in the latter analyses due to low number (n = 3). Given research showing an effect of age on biomarker concentrations,26 we performed Spearman correlation analysis of age versus pre-infusion and peak biomarker concentrations (maximum concentration during infusions; using only one infusion episode per subject).
To evaluate biomarkers to discriminate for AKI, area under the receiver operating characteristics curve (AUC, with standard error [SE]) for biomarkers measured from immediate postinfusion and from Day 2, was calculated. Analyses were performed using STATA 10® statistical software package (Stata Corp., College Station, TX, USA).
3 |. RESULTS
3.1 |. Patient characteristics
The analysis sample included 27 Cis-Carb infusion episodes (21 patients: 38% boys, median [interquartile range] age = 7.5 [7.8] years, 62% Montreal), 30 Ifos infusion episodes (14 patients: 50% boys, age 8.9 [8.7] years, 57% Montreal), and 15 control (nonchemotherapy) hospital episodes (15 patients: 4% boys, 47% medical, 40% surgical, 13% hematologic diagnosis), age 7.7 [6.9] years, baseline eGFR 120 [30] ml/min/1.73 m2, length of stay 6 [5] days, all Montreal). Cancer diagnoses included osteosarcoma, Ewing sarcoma, angiosarcoma, neuroblastoma, rhabdomyosarcoma, hepatocellular carcinoma/hepatoblastoma, mediastinal tumor, germ cell tumor, medulloblastoma, pineal tumor, adrenocortical carcinoma, retinoblastoma, chronic myelocytic leukemia, and acute lymphoblastic leukemia. Control diagnoses included eating disorders, gastrointestinal, appendicitis, neurologic or orthopedic, pneumonia, osteomyelitis, or malignancy investigation. No patients required dialysis or intensive care unit admission. No patients died during the study. AKI occurred during 10 (36%) and 15 (50%) of Cis-Carb and Ifos study episodes, respectively (Table 1).
TABLE 1.
Characteristics of study drug infusion episodes
| Characteristic | Cis-Carb AKI, n = 10 | Non-AKI, n = 17 | Ifos AKI, n = 15 | Non-AKI, n = 15 |
|---|---|---|---|---|
| Predrug dose estimated glomerular filtration rate (ml/min/1.73 m2) | 245 ±145 (187)* | 158 ± 39 (157) | 332 ± 196 (277)* | 180 ± 58 (156) |
| Treatment episode (cycle) duration, days | 2.3 ± 1.1 (2.0) | 1.9 ± 1.0 (2.0) | 4.5 ± 0.9 (5.0) | 3.9 ± 1.4 (5.0) |
| Dose of first infusion during episode (mg/m2)£ | 56 ± 12 (60) | 59 ± 17 (60) | 2,174 ± 550 (1,800) | 2,150 ± 640 (1,800) |
| Total chemo cycle dose (mg/m2) | 129 ± 42 (120) | 103.0 ± 20.9 (120.0) | 9,428 ± 2,075 (9,000)* | 7,912 ± 1,946 (9,000) |
| Other nephrotoxins during infusion episode | 1 (10%) | 0 | 4 (27%) | 4 (27%) |
| Infection | 0 | 3 (18%) | 0 | 0 |
| Length of stay, days | 5.2 ± 2.0 (5.0) | 5.9 ± 8.1 (4.0) | 6.2 ± 1.6 (6.0) | 5.3 ± 1.5 (6.0) |
| Worst AKI severity stage | ||||
| 1 | 7/10 (70%) | N/A | 9/15 (60%) | N/A |
| 2 | 2/10 (20%) | 3/15 (20%) | ||
| 3 | 1/10(10%) | 3/15 (20%) | ||
chemo, chemotherapy.
Dosing results exclude the three patients who received Carb (initial dose was 280 ± 173 (375) mg/m2; total cycle dose was 405 ± 335 (385) mg/m2).
P value less than 0.05 for test of difference between AKI and non-AKI groups.
Pre-infusion cycle eGFR was higher in AKI episodes for both Cis-Carb and Ifos groups (Table 1). Total cycle infusion doses were higher in Ifos episodes with AKI versus non-AKI episodes (P < 0.05; Table 1); there was no significant association between drug dose and AKI in the Cis-Carb group. Treatment episode durations, length of stay, infection, and use of other nephrotoxins during admission were not significantly different between AKI and non-AKI groups (Table 1).
3.2 |. Temporal excretion of biomarkers on therapy
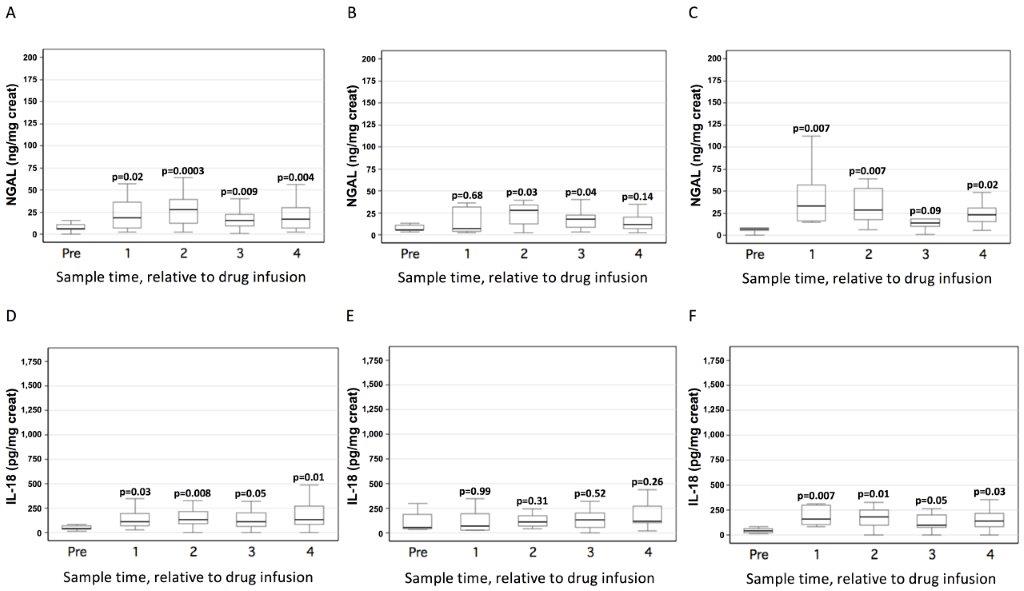
Supplementary Figures S1 and S2 show biomarker excretion from pre-infusion to Day 4 postinfusion (3 days after infusion) for Cis-Carb and Ifos treatments, respectively. Nonchemotherapy control NGAL and IL-18 concentrations (median [interquartile range]) were 40 [106] ng/mg creatinine and 90 [302] pg/mg creatinine; these were not significantly different from pre-infusion Cis-Carb NGAL or IL-18 (Supplementary Figs. S1A and 1D for all Cis-Carb episodes [P > 0.05 for difference]). Pre-infusion Ifos NGAL and IL-18 concentrations (6 [6] ng/mg creatinine and 44 [39] pg/mg creatinine, respectively) were significantly lower than nonchemotherapy control values (P < 0.05 for both).
During Cis-Carb treatments, immediate postdose to Day 4 urine NGAL (Supplementary Figs. S1A to 1C) and urine IL-18 (Supplementary Figs. S1D–1F) were never statistically significantly higher than pre-infusion biomarker concentrations.
During non-AKI and AKI treatment episodes, post-Ifos infusion NGAL was significantly higher than pre-infusion, but the rise occurred earlier and was more striking in AKI episodes (Supplementary Figs. S2B [non-AKI] and S2C [AKI]). Post-Ifos infusion IL-18 was also significantly higher than pre-Ifos concentrations during AKI episodes (Supplementary Fig. S2F), but not during non-AKI episodes (Supplementary Fig. S2E).
3.3 |. Association of biomarkers with chemotherapy dose and age
During Cis (n = 3 Carb excluded), immediate postinfusion NGAL and IL-18 concentrations were associated with increasing Cis dose (Fig. 1A and 1B), but this association was only statistically significant for post-Cis NGAL (Fig. 1A). Cis dose correlated significantly with increasing NGAL and IL-18 (Spearman r = 0.73 and 0.64, respectively, detailed Figs. 1A and 1B). Immediate post-Ifos NGAL and IL-18 were associated with increasing Ifos dose (Figs. 1C and 1D); this association was only statistically significant for NGAL (Fig. 1C). Ifos dose correlated moderately with post-Ifos IL-18 (Spearman r = 0.52, Fig. 1D), but not with post-dose NGAL (Fig. 1C).
FIGURE 1.

Association of immediate post-infusion biomarkers with chemotherapy dose. Graph shows box plots of biomarker concentrations (expressed per mg creatinine) measured immediately after chemotherapy dose, across increasing chemotherapy infusion dose (first dose given during a given study episode or cycle). Post-Cis biomarkers are shown in (A) and (B); post-Ifos biomarkers are shown in (C) and (D). (A) Urine NGAL excretion vs. Cis dose. (B) Urine IL-18 excretion vs. Cis dose. (C) Urine NGAL excretion vs. Ifos dose. (D) Urine IL-18 excretion vs. Ifos dose. Carb treatment episodes are excluded. Solid lines within the boxes represent median values; lower and upper box lines represent 25th and 75th percentile values and lower and upper stems represent 5th and 95th percentile values. P values shown are from the Kruskal-Wallis test comparing biomarker concentrations across the three dose groups. Correlation coefficients shown represent the Spearman correlation (r) of chemotherapy dose (continuous measure mg/m2) vs. immediate postdose biomarker concentration. creat, creatinine
Prechemotherapy infusion NGAL and IL-18 correlated with younger age (NGAL: Spearman r = –0.35, P = 0.13; IL-18: r = –0.47, P = 0.05); peak biomarker concentrations during infusions also correlated with younger age (NGAL: r = –0.49, P = 0.002; IL-18: r = –0.56, P = 0.0005).
3.4 |. Biomarkers to discriminate for chemotherapy AKI
Table 2 displays AUCs for immediate postinfusion (Day 1) and day postinfusion (Day 2) NGAL and IL-18 to discriminate for AKI during Cis-Carb and Ifos episodes. Given the correlation of biomarkers with age (above), we also performed a posthoc analysis whereby AUC was calculated, adjusted for age (shown in Table 2). When age was not adjusted for, NGAL and IL-18 were not discriminatory for Cis-Carb-AKI (Table 2). However, immediate post-Ifos (Day 1) NGAL and IL-18 discriminated for AKI with AUCs of 0.80 and 0.73, respectively (Table 2); Day 2 urine NGAL and IL-18 AUCs were lower but still modestly discriminatory (0.68 and 0.60, respectively; Table 2). When age was adjusted for, all AUCs improved, especially to discriminate for AKI during Cis-Carb infusions (detailed; Table 2).
TABLE 2.
AUCs for biomarkers obtained post-Cis-Carb and -Ifos infusion to discriminate for presence of AKI
| Cis-Carb group | Ifos group | |||
|---|---|---|---|---|
| Biomarker | AUC (SE) for AKI | AUC (SE) for AKI, adjusted for age | AUC [SE] for AKI | AUC (SE) for AKI, adjusted for age* |
| NGAL (ng/mg creatinine) | ||||
| Day 1 (postinfusion) | 0.40 (0.15) | 0.64 (0.15) | 0.80 (0.13) | 0.82 (0.12) |
| Day 2 (morning post) | 0.38 (0.13) | 0.63 (0.14) | 0.60 (0.15) | 0.72 (0.13) |
| IL-18 (pg/mg creatinine) | ||||
| Day 1 (postinfusion) | 0.41 (0.17) | 0.57 (0.16) | 0.73 (0.16) | 0.74 (0.15) |
| Day 2 (morning post) | 0.47 (0.15) | 0.68 (0.17) | 0.68 (0.13) | 0.69 (0.13) |
Adjustment for age was performed using logistic regression whereby the outcome was AKI and both the biomarker and age were included in the logistic regression analysis, with postregression calculation of AUC.
4 |. DISCUSSION
This is a novel study evaluating urine NGAL and IL-18 excretion in children treated with chemotherapy. With Cis–Carb, NGAL and IL-18 did not rise significantly and were not diagnostic of AKI. With Ifos infusion, both biomarkers rose, particularly with AKI, and postinfusion NGAL and IL-18 were diagnostic of AKI.
Ifos causes tubular damage through its toxic metabolite, chloroacetaldehyde, which causes local oxidative stress.27 Damage is primarily to the proximal tubule, but can occur in the distal tubule.27 Cisplatin is a renally excreted DNA cross-linking agent causing AKI in 20–80% of children.28 It damages the proximal, as well as distal, tubule, through various mechanisms (inflammation, oxidative stress injury, apoptosis).29 Carboplatin causes injury through similar mechanisms, but less severely.30 Animal studies have shown elevations of NGAL31–33 in Cis-nephrotoxicity. Proximal tubule NGAL expression was upregulated after Cis infusion in rodents.19 IL-18 is a proinflammatory cytokine induced in proximal tubular cells and excreted in the urine after ischemic kidney injury.20 Animal studies characterizing IL-18 excretion after Cis-Carb or Ifos infusion are lacking.
Substantial literature exists on AKI biomarkers in intensive care and cardiac surgery populations.15,16,18,34 This research led to recommendations that new biomarkers should be incorporated into AKI definition to reflect acute renal function change with AKI (SCr, urine output) and tissue damage evidence (biomarkers).14 AKI biomarker research lagged in the cancer population, despite the fact that these children are at high AKI risk and may benefit from specific and early AKI diagnosis. AKI biomarker research has highlighted the importance of validating novel biomarkers in different populations. Some biomarkers may be better for AKI diagnosis in children versus adults35 or with specific AKI mechanisms; different diseases may affect biomarkers independent of AKI (e.g., sepsis increases NGAL and IL-18 concentrations).16,18 It is important to study new AKI biomarkers in the cancer population to determine if recent biomarker research applies to these patients and determine the most relevant ways to apply biomarkers in these patients.
Few studies (almost only in adults) evaluated AKI biomarkers in chemotherapy AKI.21,22,36–40 In Cis-treated adults, AKI biomarker concentrations were elevated before treatment.41 In our cohort, pre-Cis-Carb or Ifos infusion NGAL and IL-18 were not higher than in nonchemotherapy controls. This is relevant, indicating that these biomarkers should be expected to be normal before chemotherapy and may potentially be used as nephrotoxicity markers.
In 33 Cis-treated adults, urine NGAL predicted AKI with AUC over 0.85.22 Another study in Cis-treated elderly adults showed that AKI prediction using NGAL (3 days postinfusion) was modest (AUC ~ 0.65).42 An Egyptian study measured NGAL in 30 Cis-treated children with solid tumors, pre-Cis, 1 week after treatment start and at cancer treatment end. Posttreatment NGAL discriminated for AKI with AUC nearly 0.8543; however, it was unclear whether AKI had occurred by the time urine NGAL was measured. Our study’s focus was on early nephrotoxicity detection. Cis-Carb treatment was not associated with significant NGAL or IL-18 rise. Differences in characteristics (age, cancer types, morbidities) of our cohort may explain discordance of these results with past literature. There may have been unmeasured/unknown factors affecting NGAL and IL-18 concentrations during Cis-Carb treatment, independent of AKI. It is possible that in Cis-Carb nephrotoxicity, a more severe injury phenotype is required before seeing substantial urine biomarker elevations. Regardless, there was not a strong relationship between NGAL and IL-18 concentrations with Cis-Carb-AKI. NGAL and IL-18 are two highly studied AKI biomarkers in children, likely to be incorporated into clinical care in coming years, with commercial kit development. Thus, it is important to elucidate that they may not be useful for AKI diagnosis in Cis-Carb treated children and pursue other novel biomarker research.
With Ifos, both biomarkers were diagnostic of AKI when measured immediately postdose. If confirmed in larger populations, NGAL and IL-18 may be used as early markers of Ifos-AKI. This could enable research evaluating early Ifos-AKI interventions (e.g., early targeted fluid to prevent nephrotoxicity; incorporating biomarkers in timing of Ifos dosing decisions; active nephrotoxin avoidance) and ultimately pharmacologic interventions. Interestingly, although NGAL and IL-18 rise were more pronounced during Ifos-AKI episodes, they rose in non-AKI episodes. This finding was shown in adults treated with Cis.41 This suggests that there could be subclinical (no SCr rise) renal injury with Ifos; this is relevant in this population, who commonly receive large amounts of fluids, which may affect ability to detect SCr rise (SCr concentration dilution). This finding is consistent with international consensus that AKI biomarkers may be useful for detecting subclinical AKI.14 Biomarkers need to be validated in larger pediatric studies to control for other variables that may affect biomarker concentrations. A further challenge in using validated AKI biomarkers in cancer treatment will be developing and testing safe AKI treatments and using biomarkers for timely treatment application. This is more complex in the cancer population, as there is the added concern of drugs that may impact on tumor growth. Several potential treatments of both Cis- and Ifos-mediated AKI have been shown to mitigate renal tissue damage.11,44,45 A few human studies suggest that ameliorating chemotherapy-associated AKI with medication is possible.27,46 Early and specific AKI markers will enhance future trials of Cis- and Ifos-nephrotoxicity prevention.
We found that the Ifos treatment group had pre-infusion biomarker concentrations lower than nonchemotherapy controls did. Reasons for this are unclear; however, pre-Ifos fluid therapy may affect biomarker concentrations, even if corrected for urine creatinine. The effect of high fluid administration on biomarker concentrations should be a topic of future research. Another related finding was that pre-drug eGFR was high overall in the cohort. This may be due to the high fluid typically administered with Cis or Ifos treatments, leading to SCr dilution. However, we found that patients with AKI had higher pre-infusion GFR than non-AKI patients. This has been shown in noncancer-treated child populations1,2 and never been well explained. It is possible that children with lower baseline SCr (thus higher eGFR) may have lower muscle mass, be less well-nourished, and thus be at higher AKI risk. However, this has never been proven. We believe that such uncertainty associated with using SCr to evaluate for renal damage supports the need for novel AKI biomarkers.
We found a dose-response relationship between increasing initial chemotherapy dose and immediate postinfusion biomarkers concentrations. Although our sample was limited and these findings should be cautiously interpreted, this approach to studying biomarkers could serve as a model in using biomarkers to evaluate nephrotoxicity, both clinically and in drug development.37
Our study had limitations. We had a small sample size, including multiple infusions from some subjects. Our data collection and sample size did not allow us to evaluate if biomarker concentrations differ with by prior exposure to chemotherapies, nor whether injury biomarkers “recover” between cycle infusions. This is an important area for future studies to examine biomarker excretion with repeated Cis or Ifos infusions and understand whether biomarkers may indicate injury recovery between infusions. The sample size limited our ability to control for confounders (e.g., cancer type). However, we found that younger age was associated with higher biomarker concentrations, as shown in previous research.26 Also, biomarker AUCs for AKI discrimination increased when adjusted for age, suggesting that future research should control for age or analyze age subgroups, when evaluating biomarkers for Cis- or Ifos-AKI diagnosis. We did not collect specimens to clinically characterize nephrotoxicity (magnesium, potassium, other electrolytes). Despite the fact that current internationally accepted AKI definition relies on evaluating SCr rise, it is likely that Cis-Carb- and Ifos-AKI definition should include tubular injury measures (e.g., hypophosphatemia).47 Future studies should elucidate whether including traditional tubular injury markers in Cis-Carb- or Ifos-AKI definition leads to stronger AKI-outcome associations and to stronger associations with AKI biomarkers. Our study had several strengths, in addition to being novel in approach and population. The study was conducted in two North American centers, increasing generalizability. Our nonchemotherapy control group helped interpretation of predrug biomarker concentrations. We evaluated biomarkers serially postinfusion, maximizing interpretation for potential application. Our results are biologically plausible, as Ifos primarily causes proximal tubular injury, and urine NGAL and IL-18 are known to be upregulated in proximal tubular damage.
Urinary AKI biomarkers have the potential to play an important role in caring for children treated with chemotherapy. Our study supports that additional research in larger cohorts is needed to further elucidate whether biomarkers consistently and reliably discriminate for AKI in this population and understand other modifiers that may enhance or reduce performance.
Supplementary Material
{kind=link}
{kind=link}
Abbreviations:
- AKI
acute kidney injury
- AUC
area under the receiver operating characteristic curve
- CCHMC
cincinnati children’s hospital medical centre
- Carb
carboplatin
- CKiD
chronic kidney disease in children
- Cis
cisplatin
- CV
coefficient of variation
- eGFR
estimated glomerular filtration rate
- ELISA
enzyme-linked immunosorbent assay
- IDMS
isotope dilution mass spectrometry
- Ifos
ifosfamide
- IL-18
interleukin-18
- KDIGO
kidney disease improving global outcomes
- MCH
montreal children’s hospital
- NGAL
neutrophil gelatinase-associated lipocalin
- SCr
serum creatinine
- SD
standard deviation
- SE
standard error
Footnotes
CONFLICT OF INTEREST
MZ was supported by grants from Fonds de Recherches du Quebec-Sante and KRESCENT. PD is supported by National Institutes of Health grants (NIH, P50DK096418). PD is a co-inventor on patents for NGAL as a biomarker of kidney injury.
SUPPORTING INFORMATION
Additional Supporting Information may be found online in the supporting information tab for this article.
REFERENCES
- 1.Alkandari O, Eddington KA, Hyder A, et al. Acute kidney injury is an independent risk factor for pediatric intensive care unit mortality, longer length of stay and prolonged mechanical ventilation in critically ill children: a two-center retrospective cohort study. Crit Care. 2011;15:R146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Li S, Krawczeski CD, Zappitelli M, et al. Incidence, risk factors, and outcomes of acute kidney injury after pediatric cardiac surgery: a prospective multicenter study. Crit Care Med. 2011;39:1493–1499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hui-Stickle S, Brewer ED, Goldstein SL. Pediatric ARF epidemiology at a tertiary care center from 1999 to 2001. Am J Kidney Dis. 2005;45:96–101. [DOI] [PubMed] [Google Scholar]
- 4.Menon S, Kirkendall ES, Nguyen H, Goldstein SL. Acute kidney injury associated with high nephrotoxic medication exposure leads to chronic kidney disease after 6 months. J Pediatr. 2014;165:522–527.e522. [DOI] [PubMed] [Google Scholar]
- 5.Stohr W, Paulides M, Bielack S, et al. Nephrotoxicity of cisplatin and carboplatin in sarcoma patients: a report from the late effects surveil-lance system. Pediatr Blood Cancer. 2007;48:140–147. [DOI] [PubMed] [Google Scholar]
- 6.Stohr W, Paulides M, Bielack S, et al. Ifosfamide-induced nephrotoxicity in 593 sarcoma patients: a report from the Late Effects Surveillance System. Pediatr Blood Cancer. 2007;48:447–452. [DOI] [PubMed] [Google Scholar]
- 7.Knijnenburg SL, Mulder RL, Schouten-Van Meeteren AY, et al. Early and late renal adverse effects after potentially nephrotoxic treatment for childhood cancer. Cochrane Database Syst Rev. 2013;10:CD008944. [DOI] [PubMed] [Google Scholar]
- 8.Jones DP, Spunt SL, Green D, Springate JE. Renal late effects in patients treated for cancer in childhood: a report from the Children’s Oncology Group. Pediatr Blood Cancer. 2008;51:724–731. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Perazella MA, Moeckel GW. Nephrotoxicity from chemotherapeutic agents: clinical manifestations, pathobiology, and prevention/therapy. Semin Nephrol. 2010;30:570–581. [DOI] [PubMed] [Google Scholar]
- 10.Ding H, Kopple JD, Cohen A, Hirschberg R. Recombinant human insulin-like growth factor-I accelerates recovery and reduces catabolism in rats with ischemic acute renal failure. J Clin Invest. 1993;91:2281–2287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chen N, Aleksa K, Woodland C, Rieder M, Koren G. N-Acetylcysteine prevents ifosfamide-induced nephrotoxicity in rats. Br J Pharmacol. 2008;153:1364–1372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Omurtag GZ, Tozan A, Sehirli AO, Sener G. Melatonin protects against endosulfan-induced oxidative tissue damage in rats. J Pineal Res. 2008;44:432–438. [DOI] [PubMed] [Google Scholar]
- 13.Faubel S, Chawla LS, Chertow GM, Goldstein SL, Jaber BL, Liu KD. Ongoing clinical trials in AKI. Clin J Am Soc Nephrol 2012;7:861–873. [DOI] [PubMed] [Google Scholar]
- 14.Endre ZH, Kellum JA, Di Somma S, et al. Differential diagnosis of AKI in clinical practice by functional and damage biomarkers: workgroup statements from the tenth Acute Dialysis Quality Initiative Consensus Conference. Contrib Nephrol. 2013;182:30–44. [DOI] [PubMed] [Google Scholar]
- 15.Parikh CR, Devarajan P, Zappitelli M, et al. Postoperative biomarkers predict acute kidney injury and poor outcomes after pediatric cardiac surgery. J Am Soc Nephrol. 2011;22:1737–1747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Zappitelli M, Washburn KK, Arikan AA, et al. Urine neutrophil gelatinase-associated lipocalin is an early marker of acute kidney injury in critically ill children: a prospective cohort study. Crit Care. 2007;11:R84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.McWilliam SJ, Antoine DJ, Sabbisetti V, et al. Mechanism-based urinary biomarkers to identify the potential for aminoglycoside-induced nephrotoxicity in premature neonates: a proof-of-concept study. PLoS ONE. 2012;7:e43809. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Washburn KK, Zappitelli M, Arikan AA, et al. Urinary interleukin-18 is an acute kidney injury biomarker in critically ill children. Nephrol Dial Transplant. 2008;23:566–572. [DOI] [PubMed] [Google Scholar]
- 19.Mishra J, Mori K, Ma Q, Kelly C, Barasch J, Devarajan P. Neutrophil gelatinase-associated lipocalin: a novel early urinary biomarker for cisplatin nephrotoxicity. Am J Nephrol. 2004;24:307–315. [DOI] [PubMed] [Google Scholar]
- 20.Melnikov VY, Faubel S, Siegmund B, Lucia MS, Ljubanovic D, Edelstein CL. Neutrophil-independent mechanisms of caspase-1- and IL-18-mediated ischemic acute tubular necrosis in mice. J Clin Invest. 2002;110:1083–1091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Tekce BK, Uyeturk U, Tekce H, Uyeturk U, Aktas G, Akkaya A. Does the kidney injury molecule-1 predict cisplatin-induced kidney injury in early stage? Ann Clin Biochem. 2015;52:88–94. [DOI] [PubMed] [Google Scholar]
- 22.Lin HY, Lee SC, Lin SF, et al. Urinary neutrophil gelatinase-associated lipocalin levels predict cisplatin-induced acute kidney injury better than albuminuria or urinary cystatin C levels. Kaohsiung J Med Sci. 2013;29:304–311. [DOI] [PubMed] [Google Scholar]
- 23.von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61:344–349. [DOI] [PubMed] [Google Scholar]
- 24.Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO clinical practice guideline for acute kidney injury. Kidney Inter. 2012;2(Suppl):1–138. [Google Scholar]
- 25.Schwartz GJ, Work DF. Measurement and estimation of GFR in children and adolescents. Clin J Am Soc Nephrol. 2009;4:1832–1843. [DOI] [PubMed] [Google Scholar]
- 26.Zappitelli M, Coca SG, Garg AX, et al. The association of albumin/creatinine ratio with postoperative AKI in children undergoing cardiac surgery. Clin J Am Soc Nephrol. 2012;7:1761–1769. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Hanly L, Chen N, Rieder M, Koren G. Ifosfamide nephrotoxicity in children: a mechanistic base for pharmacological prevention. Expert Opin Drug Saf. 2009;8:155–168. [DOI] [PubMed] [Google Scholar]
- 28.Skinner R, Parry A, Price L, Cole M, Craft AW, Pearson AD. Persistent nephrotoxicity during 10-year follow-up after cisplatin or carboplatin treatment in childhood: relevance of age and dose as risk factors. Eur J Cancer. 2009;45:3213–3219. [DOI] [PubMed] [Google Scholar]
- 29.Yao X, Panichpisal K, Kurtzman N, Nugent K. Cisplatin nephrotoxicity: a review. Am J Med Sci. 2007;334:115–124. [DOI] [PubMed] [Google Scholar]
- 30.English MW, Skinner R, Pearson AD, Price L, Wyllie R, Craft AW. Dose-related nephrotoxicity of carboplatin in children. Br J Cancer. 1999;81:336–341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Sinha V, Vence LM, Salahudeen AK. Urinary tubular protein-based biomarkers in the rodent model of cisplatin nephrotoxicity: a comparative analysis of serum creatinine, renal histology, and urinary KIM-1, NGAL, and NAG in the initiation, maintenance, and recovery phases of acute kidney injury. J Invest Med. 2013;61:564–568. [DOI] [PubMed] [Google Scholar]
- 32.Paragas N, Qiu A, Zhang Q, et al. The NGAL reporter mouse detects the response of the kidney to injury in real time. Nat Med. 2011;17:216–222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Won AJ, Kim S, Kim YG, et al. Discovery of urinary metabolomic biomarkers for early detection of acute kidney injury. Mol Biosyst. 2016;12:133–144. [DOI] [PubMed] [Google Scholar]
- 34.Bennett M, Dent CL, Ma Q, et al. Urine NGAL predicts severity of acute kidney injury after cardiac surgery: a prospective study. Clin J Am Soc Nephrol. 2008;3:665–673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Parikh CR, Thiessen-Philbrook H, Garg AX, et al. Performance of kidney injury molecule-1 and liver fatty acid-binding protein and combined biomarkers of AKI after cardiac surgery. Clin J Am Soc Nephrol. 2013;8:1079–1088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Shahbazi F, Sadighi S, Dashti-Khavidaki S, Shahi F, Mirzania M. Urine ratio of neutrophil gelatinase-associated lipocalin to creatinine as a marker for early detection of cisplatin-associated nephrotoxicity. Iran J Kidney Dis. 2015;9:306–310. [PubMed] [Google Scholar]
- 37.Seker MM, Deveci K, Seker A, et al. Predictive role of neutrophil gelatinase-associated lipocalin in early diagnosis of platin-induced renal injury. Asian Pac J Cancer Prev. 2015;16:407–410. [DOI] [PubMed] [Google Scholar]
- 38.Peres LA, da Cunha AD Jr., Assumpcao RA, et al. Evaluation of the cisplatin nephrotoxicity using the urinary neutrophil gelatinase-associated lipocalin (NGAL) in patients with head and neck cancer. J Bras Nefrol. 2014;36:280–288. [DOI] [PubMed] [Google Scholar]
- 39.Kos FT, Sendur MA, Aksoy S, et al. Evaluation of renal function using the level of neutrophil gelatinase-associated lipocalin is not predictive of nephrotoxicity associated with cisplatin-based chemotherapy. Asian Pac J Cancer Prev. 2013;14:1111–1114. [DOI] [PubMed] [Google Scholar]
- 40.Carvalho Pedrosa D, Macedo de Oliveira Neves F, Cavalcante Meneses G, et al. Urinary KIM-1 in children undergoing nephrotoxic antineoplastic treatment: a prospective cohort study. Pediatr Nephrol. 2015;30:2207–2213. [DOI] [PubMed] [Google Scholar]
- 41.Pavkovic M, Robinson-Cohen C, Chua AS, et al. Detection of drug-induced acute kidney injury in humans using urinary KIM-1, miR-21, −200c, and −423. Toxicol Sci. 2016;152:205–213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Hosohata K, Washino S, Kubo T, et al. Early prediction of cisplatin-induced nephrotoxicity by urinary vanin-1 in patients with urothelial carcinoma. Toxicology. 2016;359–360:71–75. [DOI] [PubMed] [Google Scholar]
- 43.Almalky MA, Hasan SA, Hassan TH, et al. Detection of early renal injury in children with solid tumors undergoing chemotherapy by urinary neutrophil gelatinase-associated lipocalin. Mol Clin Oncol. 2015;3:1341–1346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Akyol s, Ugurcu V, Altuntas A, Hasgul R, Cakmak O. Caffeic acid phenethyl ester as a protective agent against nephrotoxicity and/or oxidative kidney damage: a detailed systematic review. Sci World J. 2014;2014:561971. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.dos Santos NA, Carvalho Rodrigues MA, Martins NM, dos Santos AC. Cisplatin-induced nephrotoxicity and targets of nephroprotection: an update. Arch Toxicol. 2012;86:1233–1250. [DOI] [PubMed] [Google Scholar]
- 46.Karademir LD, Dogruel F, Kocyigit I, et al. The efficacy of theophylline in preventing cisplatin-related nephrotoxicity in patients with cancer. Ren Fail. 2016;38:806–814. [DOI] [PubMed] [Google Scholar]
- 47.Jimenez-Triana CA, Castelan-Martinez OD, Rivas-Ruiz R, et al. Cisplatin nephrotoxicity and longitudinal growth in children with solid tumors: a retrospective cohort study. Medicine (Baltimore). 2015;94:e1413. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.