

Key Points
Question
What is the association of legal market cannabis flower and concentrates with cannabis intoxication and neurobehavioral impairment?
Findings
In this cohort study of 121 cannabis flower users and concentrate users randomly assigned to higher- vs lower-THC products within user groups, use of legal market cannabis concentrates (ranging from 70%-90% tetrahydrocannabinol [THC]) produced significantly higher THC blood plasma levels compared with use of legal market cannabis flower (ranging from 16%-24% THC). Despite differences in THC exposure, flower and concentrate users showed similar neurobehavioral patterns after acute cannabis use and the domains of verbal memory and proprioception-focused postural stability for both groups were associated with THC.
Meaning
Use of cannabis concentrates was associated with higher THC exposure and potentially greater risk, but differences in short-term subjective and neurobehavioral impairments did not track specifically with strength of the cannabis consumed.
Abstract
Importance
The rapidly growing legal cannabis market includes new and highly potent products, the effects of which, to our knowledge, have not previously been examined in biobehavioral research studies because of federal restrictions on cannabis research.
Objective
To use federally compatible, observational methods to study high-∆9-tetrahydrocannabinol (THC) legal market forms of cannabis.
Design, Setting, and Participants
In this cohort study with a between-groups design that was conducted in a community and university setting, cannabis flower users and concentrate users were randomly assigned to higher- vs lower-THC products within user groups. Participants completed a baseline and an experimental mobile laboratory assessment that included 3 points: before, immediately after, and 1 hour after ad libitum legal market flower and concentrate use. Of the 133 individuals enrolled and assessed, 55 regular flower cannabis users (41.4%) and 66 regular concentrate cannabis users (49.6%) complied with the study’s cannabis use instructions and had complete data across primary outcomes.
Exposures
Flower users were randomly assigned to use either 16% or 24% THC flower and concentrate users were randomly assigned to use either 70% or 90% THC concentrate that they purchased from a dispensary.
Main Outcomes and Measures
Primary outcome measures included plasma cannabinoids, subjective drug intoxication, and neurobehavioral tasks testing attention, memory, inhibitory control, and balance.
Results
A total of 121 participants completed the study for analysis: 55 flower users (mean [SD] age, 28.8 [8.1] years; 25 women [46%]) and 66 concentrate users (mean [SD] age, 28.3 [10.4] years; 30 women [45%]). Concentrate users compared with flower users exhibited higher plasma THC levels and 11-hydroxyΔ9-THC (THC’s active metabolite) across all points. After ad libitum cannabis administration, mean plasma THC levels were 0.32 (SE = 0.43) μg/mL in concentrate users (to convert to millimoles per liter, multiply by 3.18) and 0.14 (SE = 0.16) μg/mL in flower users. Most neurobehavioral measures were not altered by short-term cannabis consumption. However, delayed verbal memory (F1,203 = 32.31; P < .001) and balance function (F1,203 = 18.88; P < .001) were impaired after use. Differing outcomes for the type of product (flower vs concentrate) or potency within products were not observed.
Conclusions and Relevance
This study provides information about the association of pharmacological and neurobehavioral outcomes with legal market cannabis. Short-term use of concentrates was associated with higher levels of THC exposure. Across forms of cannabis and potencies, users’ domains of verbal memory and proprioception-focused postural stability were primarily associated with THC administration.
This cohort study examines association of legal market cannabis flower and concentrates in Colorado with cannabis intoxication and neurobehavioral impairment.
Introduction
As of early 2020, 33 states have legalized medical cannabis and 11 states and the District of Columbia have legalized recreational cannabis. The rapidly growing legal market has produced the demand for and availability of various products that may pose substantial public health risks but, to our knowledge, have previously not been considered in biobehavioral research because of federal restrictions on cannabis research.
The Cannabis sativa L plant contains hundreds of phytocannabinoids, but most important to public health is the psychoactive cannabinoid Δ9-tetrahydrocannabinol (THC). The average flower potency for legal market strains in Colorado is 16% to 19% THC, with strains of up to 30% THC commonly available,1,2 and the use of concentrated forms of cannabis is increasing.3,4 Concentrates are made by extracting plant cannabinoids into a form with a much higher THC concentration5 (eg, 80%-90%6). To our knowledge, there are virtually no data on the relative risks associated with use of these higher-strength products.
THC Blood Levels and Subjective Drug Effects
Recent reviews have suggested that current higher-potency cannabis may lead to more intoxication and impairment.7 Numerous studies suggest that cannabis is associated with a short-term increase in intoxication and positive mood but also may increase negative moods, such as tension and negative affect,8,9,10,11 generally following a dose-dependent function based on THC potency.12,13 More recent studies have similarly found that short-term cannabis use increases subjective positive effects, such as feeling “high”14,15 even when using a balanced placebo design to control for participant drug expectancies.16,17
When considering the association of THC blood levels with cannabis intoxication, older18,19 and more recent work supports a titration model (ie, individuals self-titrate to consume less cannabis as THC potency increases).20,21,22 However, blood THC levels and subjective intoxication ratings increase as a function of THC in the product, suggesting that despite titration, users can still experience greater intoxication—and potentially greater harms—from higher-potency cannabis.21 In addition, as THC is rapidly metabolized into its active metabolite 11-hydroxyΔ9-THC (11-OH-THC),23 measuring this metabolite along with THC is relevant to total THC exposure and short-term intoxication.
Neurobehavioral Effects
Studies have demonstrated negative short-term and long-term neurobehavioral effects of cannabis,24 including harmful cognitive25,26,27,28 and motor effects, especially associated with verbal recall, selective attention,29,30 and inhibitory motor control.31 Over time, THC exposure may confer negative associations with brain regions associated with the control of coordinated movement,32 and deficits in brain activation in motor control regions that persist beyond short-term intoxication.33 Importantly, to our knowledge, none of these effects have been tested with legal market products.
The existing literature is limited by the use of low-THC products and drug administration approaches that do not reflect legal market cannabis use.9 For example, the use of low-potency cannabis cigarettes with a standardized puffing procedure14,18 controls dosing but may not translate directly to real-world cannabis use. Laboratory studies emphasizing internal validity are important, but it is critical that the knowledge base also include studies emphasizing external validity.
Current Study
This study addresses these limitations with a mobile laboratory and naturalistic administration of legal market flower (either 16% or 24% THC) and concentrates (either 70% or 90% THC). We assessed outcomes after ad libitum use to answer the following questions:
How is short-term use of legal market cannabis flower and concentrates associated with THC plasma levels, subjective intoxication and mood, cognitive performance, and balance?
Do these associations differ between flower and concentrate users?
Do these associations differ by THC potency within the form of cannabis (16% vs 24% flower or 70% vs 90% concentrate)?
We hypothesized that concentrates would be associated with greater THC plasma levels, subjective intoxication, and neurobehavioral impairment compared with flower use but did not expect potency differences based on prior work supporting titration.
Methods
Participants
The study was approved by the University of Colorado–Boulder institutional review board. Participants were recruited using social media postings and mailed flyers advertising to either flower or concentrate users. Participants provided written informed consent and were compensated for their time and effort during baseline ($50) and mobile laboratory appointments ($100). Funds were not provided for the purchase of state legal market cannabis. The study was registered as an observational study in ClinicalTrials.gov (NCT03522103) and the study protocol is included in Supplement 1.
Trained research staff screened participants via telephone. The criteria for inclusion were:
Age between 21 and 70 years.
Used cannabis at least 4 times in the past month.
Prior use (at least once by self-report) of the highest potency of cannabis that could be assigned in the study (24% THC flower or 90% THC for concentrate) with no adverse reaction.
No other non–prescription drug use in the past 60 days as confirmed with urine toxicology screening results.
No daily tobacco use.
Drinking 2 times or fewer per week and 3 drinks or fewer per occasion.
Not pregnant (verified via pregnancy test results) or trying to become pregnant.
Not receiving treatment for psychotic disorder or bipolar disorder.
Baseline Appointment
Participants were instructed not to use cannabis on the day of their baseline appointment, which took place on campus (University of Colorado, Boulder). A breathalyzer and urinalysis test were administered to test for alcohol and other drug use, respectively. Participants completed questionnaires on demographics, lifestyle, substance use, and medical history and underwent a blood draw, completed self-report measures of subjective drug effects, and completed neurobehavioral tests. The demographics form asked participants to classify their race. Options were defined by the investigator, including an “other” option. Race was considered only as a baseline variable to compare across groups but was not included in any analyses.
Before leaving the appointment, participants were randomly assigned to a potency condition based on a random-number table generated by the study statistician and asked to purchase the assigned product at a local dispensary (The Farm; https://thefarmco.com/). Specific allotments of the 2 different flower and concentrate products were set aside for research participants to purchase. Flower users were randomized to purchase 3 g of either strain A (16% THC) or strain B (24% THC) flower. Concentrate users were randomized to purchase 1 g of either concentrate A (70% THC) or concentrate B (90% THC). Consistent with State of Colorado requirements, the THC potency of each study product was labeled following testing in an International Organization of Standards 17025–accredited laboratory.
Experimental Appointment
Between the baseline and experimental sessions, there was a 5-day ad libitum use period during which participants could familiarize themselves with their study cannabis. On the fifth day, the mobile laboratory traveled to the participant’s place of residence for the experimental appointment. Participants were asked to abstain from using cannabis that day before the experiment. At this appointment, participants self-reported whether they purchased their study product and also provided a receipt to verify their purchase to the research staff. At the first assessment (preuse), participants completed a breath alcohol test and the primary outcome measures (described later; additional details are provided in the eMethods in Supplement 2) then returned home to use their study cannabis ad libitum through their preferred mode of administration. Participants weighed their product before and after use (Table 1). After use (mean [SD] total time away from mobile lab, 13.3 [7] minutes; range, 3-47 minutes1), they returned to the mobile laboratory to complete the outcome measures while intoxicated in the short term (short-term postuse). Individuals generally centered around the mean of 13 minutes and only 3 individuals were away from the mobile laboratory for more than 24 minutes (specifically, 30, 32, and 47 minutes). Removing the outlier who was away from the mobile laboratory for 47 minutes from the models did not change any of the patterns of significant or nonsignificant results presented. They remained in the mobile laboratory until 1 hour after using their product and then completed the measures a final time (1 hour postuse).
Table 1. Sample Demographics and Baseline Characteristics by Form and Potency of Cannabis User Groups.
| Characteristic | Flower overall (n = 55) | Flower, 24% THC (n = 29) | Flower, 16% THC (n = 26) | Concentrate overall (n = 65) | Concentrate, 90% THC (n = 32) | Concentrate, 70% THC (n = 33) |
|---|---|---|---|---|---|---|
| Demographics | ||||||
| Age, mean (SD), y | 28.76 (8.1) | 28.31 (9.3) | 29.27 (6.7) | 28.26 (10.4) | 26.38 (5.3) | 30.09 (13.5) |
| Women, No. (%) | 23 (42) | 12 (41) | 11 (42) | 31 (48) | 15 (47) | 16 (48) |
| Marital status, married, No. (%) | 9 (16) | 6 (21) | 3 (12) | 8 (12) | 5 (16) | 3 (9) |
| Education, bachelor’s degree or higher, No. (%) | 35 (64) | 18 (62) | 17 (65) | 29 (45) | 14 (44) | 15 (45) |
| Employment, full-time No. (%) | 23 (42) | 11 (38) | 12 (46) | 32 (49) | 16 (50) | 16 (48) |
| Race, white, No. (%) | 43 (78) | 22 (76) | 21 (81) | 51 (79) | 21 (66)d | 30 (91)d |
| Prescribed psychiatric medications, No. (%) | 2 (4) | 1 (3) | 1 (4) | 8 (12) | 5 (16) | 3 (9) |
| Cannabis history and use measures | ||||||
| Age at onset of regular cannabis use, mean (SD), y | 20.04 (6.6) | 20.37 (6.1) | 19.68 (7.3) | 17.73 (5.7) | 16.69 (2.8) | 18.83 (7.6) |
| Days of concentrate use,a mean (SD) (past 30 d) | 3.49 (7.9)b | 4.83 (9.2) | 1.78 (5.6) | 16.49 (11.1)d | 16.56 (10.4) | 16. 42 (11.8) |
| Days of flower use,c mean (SD) (past 30 d) | 20.55 (10.0) | 22.27 (8.3) | 18.44 (11.6) | 15.40 (10.7) | 15.50 (10.4) | 15. 30 (11.2) |
| Cannabis use disorder symptoms, No. (%) | 2.96 (2.7) | 3.32 (2.7) | 2.58 (2.6) | 3.09 (2.1) | 3.19 (2.2) | 3.0 (2.2) |
| Baseline plasma THC, μg/mL | 0.004 (0.007)d | 0.004 (0.005) | 0.004 (0.008) | 0.009 (0.011)a | 0.010 (0.013) | 0.008 (0.008) |
| Baseline plasma 11-OH-THC, μg/mL | 0.002 (0.003) | 0.002 (0.002) | 0.002 (0.003) | 0.003 (0.005) | 0.004 (0.006) | 0.003 (0.004) |
| Baseline plasma THC-COOH, μg/mL | 0.044 (0.065)d | 0.043 (0.054) | 0.045 (0.076) | 0.087 (0.083)d | 0.083 (0.083) | 0.091 (0.083) |
| Other substance use and psychological factors | ||||||
| Days of alcohol use,b mean (SD) (past 30 d) | 7.44 (7.9) | 8.62 (8.8) | 6.08 (6.6) | 8.97 (6.2) | 8.44 (6.1) | 9.48 (6.4) |
| Days of tobacco use,b mean (SD) (past 30 d) | .48 (2.0) | .21 (.9) | .8 (2.8) | 1.83 (5.5) | 2.25 (6.2) | 1.42 (4.8) |
| AUDIT total, No. (%) | 5.38 (3.13) | 5.36 (2.9) | 3.45 (.7) | 6.62 (4.8) | 7.25 (5.4) | 6.00 (4.2) |
| Depression (BDI total), No. (%) | 4.26 (5.3) | 3.96 (3.7) | 4.58 (6.6) | 6.42 (6.1) | 6.56 (5.8) | 6.27 (6.5) |
| Anxiety (BAI total), No. (%) | 4.85 (4.9) | 5.41 (5.0) | 4.23 (4.9) | 5.77 (5.8) | 5.00 (4.3) | 6.52 (7.0) |
| Cannabis use during ad libitum administration | ||||||
| Grams used during experimental appointment,e mean (SD) | .22 (.18)d | .24 (.21) | .19 (.15) | .11 (.14)a | .10 (.1) | .13 (.18) |
| Mode of ad libitum administration, No. (%) | ||||||
| Glass rig/tube | NA | NA | NA | 60 (92) | 30 (94) | 30 (91) |
| Hash pen | NA | NA | NA | 5 (8) | 2 (6) | 3 (9) |
| Joint | 4 (7) | 2 (7) | 2 (8) | NA | NA | NA |
| Bong | 17 (31) | 10 (35) | 7 (27) | NA | NA | NA |
| Pipe | 28 (51) | 14 (48) | 14 (54) | NA | NA | NA |
| Vaporizer | 6 (11) | 3 (10) | 3 (12) | NA | NA | NA |
Abbreviations: 11-OH-THC, 11-hydroxyΔ9-THC; AUDIT, alcohol use disorders identification test; BAI, back anxiety inventory; BDI, Beck Depression Inventory-II; NA, not applicable; THC, tetrahydrocannabinol; THC-COOH, tetrahydrocannabinol caroxylic acid.
SI conversion factors: To convert to millimoles per liter for TCH, multiply by 3.18.
Using a 30-day timeline follow-back (TLFB), also note that some TLFB data were missing for the flower users (total flower, 41; 24%, 23; 16%, 18).
P < .001. Other than a difference in race between the 2 concentrate groups (P < .01), no significant differences emerged when comparing the potency groups within each user group (16% vs 24% flower or 70% vs 90% concentrate), including the amount used during the experimental appointment, suggesting that random assignment to potency within each form of cannabis was successful. Note that for 1 individual in the concentrates group, baseline demographics data were unavailable, so n = 120 in the Table and n=65 for the concentrates group, while n = 121 participants were included in the analysis (n=66 in the concentrates group).
Of the 10 participants (8.3%) endorsing psychiatric medications, 6 (5.0%) endorsed medications for mood/anxiety, 2 (1.6%) endorsed medications for attention-deficit/hyperactivity disorder (ADHD), and 2 (1.7%) endorsed medications for mood/anxiety and ADHD. Additionally, 12 participants (10.0%) (flower, 4 [3.3%]; concentrates, 8 [6.7%]) reported medications for the following nonpsychiatric conditions: gastrointestinal tract conditions (6 [5.0%]), blood pressure (5 [4.2%]), and pain (3 [2.5%]) (with 2 participants reporting medications for multiple nonpsychiatric problems).
P < .01.
Participants brought our scale into their home to measure the amount of study cannabis used during the experimental appointment.
Primary Measures
Blood Cannabinoids
A certified phlebotomist collected 32 mL of blood using standard, sterile phlebotomy techniques, which was stored on ice in the mobile laboratory. On return to the laboratory, plasma was separated from erythrocytes by centrifugation at 400g for 15 minutes, transferred to a fresh microcentrifuge tube, and stored at −80 °C. Plasma samples were sent to the iC42 Laboratory at the Anschutz Medical Campus (Colorado). In total, we quantified concentration of THC, 11-OH-THC (direct and active THC metabolite), and 11-nor-9-carboxy-Δ9-THC (inactive and stable THC metabolite, analyzed at baseline only23) using validated high-performance liquid chromatography/mass spectroscopy (API550034). Another primary outcome in the larger study, change in inflammation markers from before to after cannabis associated with THC and cannabidiol blood levels, will be reported elsewhere.
Subjective Intoxication and Mood
Subjective cannabis intoxication was determined using the 12-item Addiction Research Center Inventory–marijuana (ARCI-M) effects scale.35,36,37 Three additional cannabis intoxication items were assessed, mentally stoned, physically stoned (5-point scale), and feeling high (1 to 10), forming a 3-item cannabis intoxication scale (Cronbach α = .69).38 A modified Profile of Mood States (POMS39) questionnaire assessed state affect consistent with prior cannabis research40 and included the POMS vigor (eg, elated) and tension (eg, anxious) subscales; items were on a 5-point Likert-type scale, with responses ranging from not at all to extremely.
Neurobehavioral Outcomes
Cognition
Participants completed 4 cognitive tasks in domains that have been associated with cannabis use,38,41,42,43 including a 30-minute delayed verbal recall memory assessed by the International Shopping List Task44 and working memory, episodic memory, and inhibitory control assessed by 3 tasks from the National Institutes of Health toolbox.45
Balance Function
A smart device-based measurement of quiet standing balance under 3 different conditions was used to impose varying challenges on the proprioceptive and neuromuscular systems. These were eyes open, eyes closed, and eyes closed with head tilted back (eMethods in Supplement 2).
Statistical Analysis
Repeated measures analyses of variance were conducted separately for cannabinoid blood levels, subjective intoxication, and cognitive and balance performance across 3 assessments: preuse, short-term postuse, and 1 hour postuse using the emmeans package in R (R Foundation). Baseline measures of the relevant outcome were included as a covariate for each outcome. Removing baseline variables as covariates from the models did not change any of the patterns of significant or nonsignificant results. Linear and quadratic effects of time were tested to examine the possibility of sustained and recovery effects. Interaction effects tested whether linear and quadratic change over time varied by form (flower vs concentrate) of cannabis and THC potency within flower (16% vs 24%) vs concentrates (70% vs 90%). Potency effects for all outcomes are reported in eResults and eTables 1 and 2 in Supplement 2. Across all analyses, when linear and quadratic effects of time were significant, we focused on the higher-order quadratic effect. Given the number of outcomes tested, we set an a priori significance threshold of P < .01 (Table 2).
Table 2. Means, Standard Errors, and Results From Mixed-Effect Models, Repeated Measures of Analyses of Variance, and Testing of Main and Interaction Effects of Change and Form.
| Measurea | Mean (SE) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Flower | Concentrates | ||||||||||
| Preuse | Short-term use | 1 h Postuse | Preuse | Short-term use | 1 h Postuse | ||||||
| Cannabinoids | |||||||||||
| THC | 0.004 (0.03) | 0.14 (0.03) | 0.02 (0.03) | 0.01 (0.02) | 0.32 (0.02) | 0.03 (0.03) | |||||
| 11-OH-THC | 0.001 (0.001) | 0.005 (0.001) | 0.004 (0.001) | 0.004 (0.001) | 0.011 (0.001) | 0.008 (0.001) | |||||
| Subjective drug effects | |||||||||||
| ARCI-marijuana effects scale | 0.17 (0.03) | 0.53 (0.03) | 0.47 (0.03) | 0.20 (0.02) | 0.50 (0.02) | 0.41 (0.02) | |||||
| Tension | 0.35 (0.07) | 0.60 (0.07) | 0.40 (0.07) | 0.36 (0.06) | 0.38 (0.06) | 0.22 (0.06) | |||||
| Vigor | 1.29 (0.11) | 1.83 (0.12) | 1.66 (0.12) | 0.98 (0.10) | 1.56 (0.10) | 1.25 (0.11) | |||||
| Intoxication | 0.08 (0.08) | 2.40 (0.08) | 1.93 (0.08) | 0.14 (0.08) | 2.35 (0.08) | 1.63 (0.08) | |||||
| Cognition | |||||||||||
| Inhibitory control (flanker) | 99.20 (2.00) | 101.45 (2.02) | 104.38 (2.02) | 96.13 (1.84) | 99.37 (1.83) | 100.63 (1.83) | |||||
| Episodic memory (picture) | 110.37 (2.47) | 112.04 (2.49) | 114.32 (2.49) | 111.49 (2.28) | 113.52 (2.27) | 115.19 (2.27) | |||||
| Working memory | 107.50 (1.58) | 107.68 (1.59) | 113.89 (1.59) | 105.33 (1.45) | 110.35 (1.44) | 112.37 (1.44) | |||||
| Verbal recall errors (shopping list) | 0.65 (0.30) | 2.21 (0.31) | 1.88 (0.39) | 0.90 (0.28) | 1.50 (0.28) | 2.33 (0.28) | |||||
| Balance | |||||||||||
| Eyes open | 0.46 (0.03) | 0.51 (0.03) | 0.47 (0.03) | 0.47 (0.03) | 0.49 (0.03) | 0.48 (0.03) | |||||
| Eyes closed | 0.63 (0.04) | 0.73 (0.04) | 0.63 (0.04) | 0.64 (0.03) | 0.69 (0.03) | 0.64 (0.03) | |||||
| Eyes closed, head back | 0.73 (0.04) | 0.75 (0.04) | 0.65 (0.04) | 0.73 (0.04) | 0.70 (0.04) | 0.69 (0.04) | |||||
| Measure | Time effects for preuse, short-term postuse, and 1 h postuse | Cannabis form effects (ie, flower vs concentrate groups) | |||||||||
| Linear effect | P value | Quadratic effect | P value | Form effect | P value | Form × linear change | P value | Form × quadratic change | P value | ||
| Cannabinoids | |||||||||||
| THC | F1,231 = 0.20 | .65 | F1,231 = 104.50 | <.001 | F1,228 = 11.00 | <.01 | F1,228 = 0.04 | .84 | F1,228 = 15.07 | <.001 | |
| 11-OH-THC | F1,231 = 17.00 | <.001 | F1,231 = 41.06 | <.001 | F1,228 = 46.82 | <.001 | F1,228 = 1.60 | .21 | F1,228 = 3.76 | .05 | |
| Subjective drug effects | |||||||||||
| ARCI-marijuana effects | F1,235 = 177.22 | <.001 | F1,235 = 153.01 | <.001 | F1,233 = 1.84 | .18 | F1,233 = 6.37 | .01 | F1,233 = 0.33 | .56 | |
| Tension | F1,232 = 1.23 | .27 | F1,232 = 12.13 | <.001 | F1,230 = 9.90 | <.01 | F1,230 = 3.09 | .08 | F1,230 = 2.43 | .12 | |
| Vigor | F1,224 = 18.67 | <.001 | F1,224 = 49.86 | <.001 | F1,222 = 34.38 | <.001 | F1,222 = 0.09 | .77 | F1,222 = 0.35 | .56 | |
| Intoxication | F1,232 = 589.78 | <.001 | F1,232 = 599.26 | <.001 | F1,230 = 2.57 | .11 | F1,230 = 6.66 | .01 | F1,230 = 0.35 | .56 | |
| Cognition | |||||||||||
| Inhibitory control (flanker) | F1,232 = 26.69 | <.001 | F1,232 = 0.12 | .73 | F1,229 = 21.16 | <.001 | F1,229 = 0.14 | .71 | F1,229 = 0.71 | .40 | |
| Episodic memory (picture) | F1,226 = 3.47 | .06 | F1,226 = 0.01 | .93 | F1,223 = 1.03 | .31 | F1,223 = 0.16 | .69 | F1,223 = 0.01 | .93 | |
| Working memory | F1,234 = 42.65 | <.001 | F1,234 = 0.36 | .55 | F1,231 = 0.16, | .69 | F1,231 = 0.01 | .93 | F1,231 = 5.76 | .02 | |
| Verbal recall errors (shopping list) | F1,203 = 32.31 | <.001 | F1,203 = 1.59 | .21 | F1,200 = 0.20 | .65 | F1,200 = 0.02 | .89 | F1,200 = 5.18 | .02 | |
| Balance | |||||||||||
| Eyes open | F1,203 = 0.93 | .34 | F1,203 = 3.89 | .05 | F1,200) = 0.04 | .85 | F1,200 = 0.43 | .51 | F1 200 = 0.09 | .77 | |
| Eyes closed | F1,203 = 0.00 | .98 | F1,203 = 18.88 | <.001 | F1,200 = 0.04 | .85 | F1,200 = 0.17 | .68 | F1,200 = 1.49 | .22 | |
| Eyes closed, head back | F1,203 = 2.77 | .10 | F1,203 = 1.41 | .24 | F1,200 = 0.03 | .86 | F1,200 = 2.86 | .09 | F1,200 = 1.62 | .20 | |
Abbreviations: 11-OH-TCH; 11-hydroxyΔ9-THC; ARCI, Addiction Center Research Inventory; THC, tetrahydrocannabinol.
For each measure, models included the baseline measures as a covariate.
Results
Descriptive Information
A total of 64 participants (48.1%) in the flower group and 69 (51.9%) in the concentrates group completed the baseline and experimental measures. Twelve participants were excluded from analyses because of very low THC levels during the postuse assessment (THC, <0.02 μg/mL vs study mean [SD] of 0.24 [0.35] μg/mL), suggesting they had not followed study instructions to use their cannabis in their home and immediately return to the mobile laboratory. Therefore, a total of 121 participants were analyzed: 55 flower users (mean [SD] age 28.8 [8.1 years; 42% women) and 66 concentrate users (mean [SD] 28.3 [10.4] years; 48% women). Compared with the flower group, the concentrate group reported more frequent current concentrate use and exhibited greater blood levels of THC and metabolites at baseline (reflective of greater and more long-term THC exposure; Table 1). Most demographic variables did not differ by potency level within each user group, indicating that random assignment to potency was successful.
Cannabinoids
The THC and 11-OH-THC levels exhibited significant quadratic effects of time, such that levels peaked at the short-term postuse assessment and then dropped (Figure 1). After ad libitum cannabis administration, mean plasma THC levels were 0.32 (SE, 0.43) μg/mL in concentrate users and (to convert to millimoles per liter, multiply by 3.18) and 0.14 (SE, 0.16) μg/mL in flower users. Participants in concentrates group exhibited consistently higher THC and 11-OH-THC levels. Further, there was a significant form by quadratic time interaction, with a simple effect test indicating that the concentrates group had higher THC levels after short-term use but no effects of potency.
Figure 1. Blood Levels by Cannabis Form and Potency During Acute Mobile Laboratory Session.
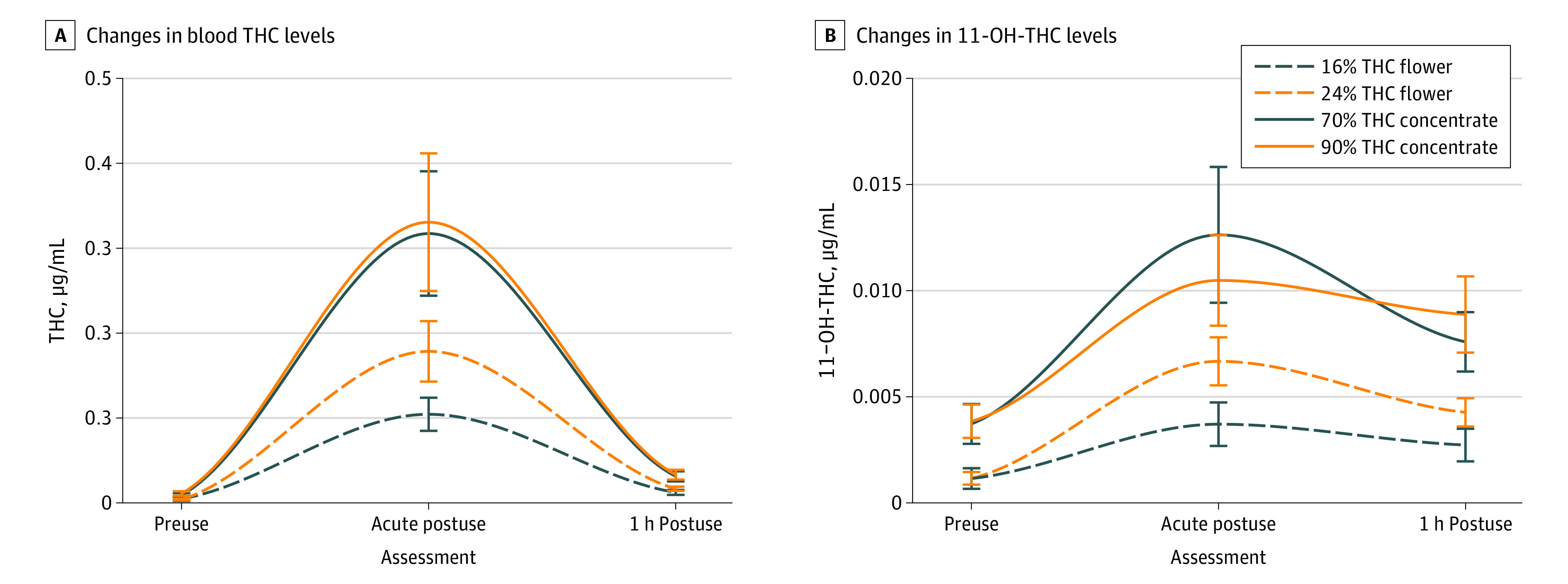
A, Changes in blood tetrahydrocannabinol (THC) (μg/mL [to convert to micromoles per liter, multiply by 3.18]) (A) and blood THC metabolite 11-Hydroxy-Δ9-THC (11-OH-THC) levels (μg/mL) (B) before cannabis use (preuse), immediately after cannabis use (acute postuse), and 1 hour postuse. A. Baseline median = 0.003; range = 0.0 to 0.05. B, Baseline median = 0.001; range = 0.0 to 0.03. For form, dashed lines indicate flower groups (16%, 24%) and solid lines indicate concentrate groups (70%, 90%). For potency, blue lines indicate lower potency within each form (16% flower, 70% concentrate) and orange lines indicate higher potency (24% flower, 90% concentrate). Across both forms of cannabis, THC and 11-OH-THC were acutely elevated after cannabis administration. The concentrates group had higher levels of the 2 cannabinoids across all assessments, as well as a stronger quadratic effect for THC (ie, a higher relative peak at the acute assessment).
Subjective Drug Effects
The ARCI-M was moderately correlated with the 3-item intoxication (r = 0.42) and POMS tension scales (r = 0.46). Other correlations among subjective measures were weakly significant (rs = 0.22-0.25). There was no correlation between the POMS tension and vigor scales (r = −0.10; P = .30). The predominant pattern of subjective intoxication and mood across assessments was quadratic, with all subjective measures peaking at short-term use and decreasing thereafter (Figure 2). Specific to mood, on average participants reported experiencing tension not at all to a little, vigor a little to moderately, and intoxication moderately to quite a bit. There was a significant main effect of the form of cannabis with tension and vigor, with the concentrates group reporting lower levels of tension and vigor. There were no associations with potency.
Figure 2. Subjective Drug Effects After Use of Cannabis by Cannabis Form and Potency During Acute Mobile Laboratory Session.

Changes in the Addiction Research Center Inventory (ARCI) marijuana scale (A), self-reported intoxication (average of feeling high, mentally stoned, and physically stoned) (B), self-reported tension (Profile of Mood States [POMS] tension subscale) (C), and self-reported positive mood (POMS vigor subscale) (D) before cannabis use (preuse), immediately after cannabis use (acute postuse), and 1-hour postuse. B, Baseline median, 0; range, 0 to 2. C, Baseline median, 0; range, 0 to 2. D, Baseline median, 1; range, 0 to 4. The ARCI assessed the endorsement rate of 12 subjective effects of cannabis (ie, range 0-1) (A). All scales had a range of 0 to 4 (B-D). For form, dashed lines indicate flower groups (16%, 24%) and solid lines indicate concentrate groups (70%, 90%). For potency, blue lines indicate lower potency within each form (16% flower, 70% concentrate) and orange lines indicate higher potency (24% flower, 90% concentrate). The effect of cannabis use assessed by all 4 measures peaked immediately after use and was generally sustained 1 hour postuse, indicated by significant effects of quadratic change. Additionally, the flower group reported higher levels of tension and vigor across all assessments, indicated by a main effect of form (flower vs concentrates). THC indicates tetrahydrocannabinol.
Neurobehavioral Performance
Cognition
There was a negative linear effect with delayed verbal recall errors, suggesting poorer performance after use compared with preuse (Figure 3). Conversely, there was a positive linear effect with inhibitory control and working memory, suggesting better performance after use, potentially because of practice effects46 (eFigure 1 in Supplement 2). There was a main effect of form with inhibitory control, for which the flower group performed better across all assessments. There were no short-term changes in inhibitory control after use and there was no association with potency.
Figure 3. Cognitive and Motor Function After Use of Cannabis by Cannabis Form and Potency During Acute Mobile Laboratory Session.

A, Number of verbal recall errors on the International Shopping List Task (A) and balance task performance with eyes closed (B) immediately before cannabis use (preuse), immediately after cannabis use (acute postuse), and 1 hour postuse. A, Baseline median = 0; range = 0 to 11. B, Baseline median = 0.6; range = 0.3 to 1.3. For form, dashed lines indicate flower groups (16%, 24%) and solid lines indicate concentrate groups (70%, 90%). For potency, blue lines indicate lower potency within each form (16% flower, 70% concentrate) and orange lines indicate higher potency (24% flower, 90% concentrate). The number of errors on the delayed verbal recall task increased in the flower and concentrate groups over time. There was a marginal effect suggesting that acute cannabis impairment was more pronounced in the flower group, which performed worse than the concentrates group on the delayed verbal recall task. During the eyes closed balance task, there was a quadratic effect of time with balance, with sway increasing acutely after use and then decreasing back to original levels 1 hour after use. There were no balance differences observed between the concentrate and flower groups. THC indicates tetrahydrocannabinol.
Balance
For the eyes open condition, the quadratic effect across time did not meet the a priori threshold for significance, but there was a trend showing impaired balance after cannabis use that normalized within an hour (eFigure 2 in Supplement 2). When the eyes were closed and the reliance on proprioception was greater, there was a significant quadratic effect of time with balance, with sway associated with a short-term increase postuse and a decrease back to preuse levels 1 hour after use (Figure 3). While performance was poorer overall in the eyes closed head back condition (eMethods in Supplement 2), there was no change from preuse to postuse. These findings did not differ by cannabis form or potency.
Discussion
Using an observational design with random assignment to a potency condition, this study is the first to our knowledge to address the association of naturalistic administration of legal market cannabis flower and concentrates with subjective intoxication and mood, cognition, and balance in regular cannabis users. Compared with cannabis flower users, cannabis concentrate users had higher plasma levels of THC and its active metabolite 11-OH-THC in the short term and overall (across all assessments). However, despite this higher THC exposure, concentrate users did not show greater short-term subjective, cognitive, or balance impairment.
Compared with previous studies, THC blood levels after legal market flower use were broadly higher than previous reports using lower potency forms, which typically fall between 0.05 to 0.12 μg/mL.21 Concentrate users showed strikingly higher levels of THC cannabinoids across all assessments compared with previous reports. Notably, there was no within-form association of THC potency with blood levels, suggesting that within the flower and concentrate groups users may be self-titrating to achieve similar levels of THC exposure as the THC potency of their cannabis increases.20,21,22
Given the marked differences in THC blood levels between concentrate and flower users, it is interesting that the self-reported levels of intoxication were not significantly different. The observation that the concentrate users achieved much higher THC blood levels (a mean [SD] of 0.32 [0.43] μg/mL) but the same intoxication level as the flower users (who had a mean [SD] of 0.14 [0.16] μg/mL) requires explanation. It is possible that the concentrate users have much greater tolerance to the effects of THC. This is consistent with data suggesting that tolerance to the psychoactive effects of cannabis is common with repeated exposure and in regular users.47,48 Another possibility is that cannabinoid receptors may become saturated with THC (a cannabinoid receptor 1 partial agonist) at higher levels, beyond which there is a diminishing effect of additional THC.49 A third possibility is that there may be individual differences among users in terms of metabolism or sensitivity to cannabis that might be associated with genetics or other preexisting biological differences.50,51 Future research is needed to test these potential mechanisms.
In general, across most cognitive measures, acute performance changes following cannabis use were minimal. In 1 exception, delayed verbal recall performance was impaired after use, which is consistent with prior work demonstrating reliable cannabis-associated impairment in this memory domain.26
A unique aspect of this study is the inclusion of a measure of the short-term association of cannabis with balance, as little research has explored the neuromotor effects of cannabis.52,53,54,55 Immediately postuse, individuals in both groups demonstrated a modest performance decrement on a moderately challenging balance task (quiet standing with no vision), and these short-term changes appeared to recover within an hour. The degree of balance impairment (approximately 11% increase in sway with eyes closed from preuse to postuse) found is consistent with prior balance effects of moderate alcohol (eg, 0.05%-0.10% blood alcohol concentration56) and lower-potency THC administration in regular users.57 These results provide evidence that balance impairment could be a useful marker of recent cannabis use, even in regular users of highly potent products who show tolerance to short-term cannabis use in other domains. Similar to the use of a field sobriety test to measure short-term alcohol intoxication, such a marker could be useful for identifying potentially impaired drivers.57
Limitations
Despite its strengths (eg, naturalistic design, inclusion of random assignment to multiple THC potency groups, and concentrate and flower cannabis users), ethical limitations preclude the random assignment of participants to the concentrate or flower user conditions. Thus, there are pre-existing differences between these 2 groups that may partially account for our findings. We also lack a placebo control, as such products do not exist in the current legal market. Further, federal cannabis regulations restricted our ability to control dosing and other aspects of drug administration, such as participant masking to product potency. There are many complex interactions between cannabinoid strength and ratio, characteristics of the individual users (eg, modality of use, expectancies, and smoking topography), and the natural environment that were not explicitly tested or accounted for in the present investigation and are important directions for future work.
Conclusions
In this study, delayed recall memory and balance impairment were associated with short-term cannabis use even in regular users, and concentrate users demonstrated similar or lower levels of subjective drug intoxication and short-term impairment compared with users of lower-potency flower forms of cannabis. However, THC exposure was much higher in concentrate users, prompting concern about long-term clinical and neurobehavioral implications of concentrate use.
Trial protocol
eMethods. Supplemental methods
eResults. Results of the tests of potency assignment within forms of cannabis (flower and concentrate)
eTable 1. Results of the tests of potency-by-change over time interactions for flower users
eTable 2. Results of the tests of potency-by-change over time interactions for concentrate users
eFigure 1. Cognitive performance after use of cannabis by cannabis form and potency during acute modile lab session
eFigure 2. Balance function after use of cannabis by cannabis form and potency during acute mobile lab session
References
- 1.Vergara D, Bidwell LC, Gaudino R, et al. Compromised external validity: federally produced cannabis does not reflect legal markets. Sci Rep. 2017;7(March):46528. doi: 10.1038/srep46528 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Orens A, Light M, Lewandowski B, Rowberry J, Saloga C 2017 market update. Accessed August 20, 2018. https://www.colorado.gov/pacific/sites/default/files/MED%20Demand%20and%20Market%20%20Study%20%20082018.pdf
- 3.Stogner JM, Miller BL. Assessing the dangers of “dabbing”: mere marijuana or harmful new trend? Pediatrics. 2015;136(1):1-3. doi: 10.1542/peds.2015-0454 [DOI] [PubMed] [Google Scholar]
- 4.Daniulaityte R, Lamy FR, Barratt M, et al. Characterizing marijuana concentrate users: a web-based survey. Drug Alcohol Depend. 2017;178:399-407. doi: 10.1016/j.drugalcdep.2017.05.034 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Raber JC, Elzinga S, Kaplan C. Understanding dabs: contamination concerns of cannabis concentrates and cannabinoid transfer during the act of dabbing. J Toxicol Sci. 2015;40(6):797-803. doi: 10.2131/jts.40.797 [DOI] [PubMed] [Google Scholar]
- 6.Cinnamon Bidwell L, YorkWilliams SL, Mueller RL, Bryan AD, Hutchison KE. Exploring cannabis concentrates on the legal market: User profiles, product strength, and health-related outcomes. Addict Behav Rep. 2018;8:102-106. doi: 10.1016/j.abrep.2018.08.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Volkow ND, Baler RD, Compton WM, Weiss SRB. Adverse health effects of marijuana use. N Engl J Med. 2014;370(23):2219-2227. doi: 10.1056/NEJMra1402309 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Heishman SJ, Huestis MA, Henningfield JE, Cone EJ. Acute and residual effects of marijuana: profiles of plasma THC levels, physiological, subjective, and performance measures. Pharmacol Biochem Behav. 1990;37(3):561-565. doi: 10.1016/0091-3057(90)90028-G [DOI] [PubMed] [Google Scholar]
- 9.Chait LD, Zacny JP. Reinforcing and subjective effects of oral delta 9-THC and smoked marijuana in humans. Psychopharmacology (Berl). 1992;107(2-3):255-262. doi: 10.1007/BF02245145 [DOI] [PubMed] [Google Scholar]
- 10.Chait LD, Evans SM, Grant KA, Kamien JB, Johanson CE, Schuster CR. Discriminative stimulus and subjective effects of smoked marijuana in humans. Psychopharmacology (Berl). 1988;94(2):206-212. doi: 10.1007/BF00176846 [DOI] [PubMed] [Google Scholar]
- 11.Martin-Santos R, Crippa JA, Batalla A, et al. Acute effects of a single, oral dose of d9-tetrahydrocannabinol (THC) and cannabidiol (CBD) administration in healthy volunteers. Curr Pharm Des. 2012;18(32):4966-4979. doi: 10.2174/138161212802884780 [DOI] [PubMed] [Google Scholar]
- 12.Hunault CC, Böcker KBE, Stellato RK, Kenemans JL, de Vries I, Meulenbelt J. Acute subjective effects after smoking joints containing up to 69 mg Δ9-tetrahydrocannabinol in recreational users: a randomized, crossover clinical trial. Psychopharmacology (Berl). 2014;231(24):4723-4733. doi: 10.1007/s00213-014-3630-2 [DOI] [PubMed] [Google Scholar]
- 13.Hart CL, van Gorp W, Haney M, Foltin RW, Fischman MW. Effects of acute smoked marijuana on complex cognitive performance. Neuropsychopharmacology. 2001;25(5):757-765. doi: 10.1016/S0893-133X(01)00273-1 [DOI] [PubMed] [Google Scholar]
- 14.Schacht JP, Selling RE, Hutchison KE. Intermediate cannabis dependence phenotypes and the FAAH C385A variant: an exploratory analysis. Psychopharmacology (Berl). 2009;203(3):511-517. doi: 10.1007/s00213-008-1397-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Cooper ZD, Haney M. Cannabis reinforcement and dependence: role of the cannabinoid CB1 receptor. Addict Biol. 2008;13(2):188-195. doi: 10.1111/j.1369-1600.2007.00095.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Metrik J, Kahler CW, Reynolds B, et al. Balanced placebo design with marijuana: pharmacological and expectancy effects on impulsivity and risk taking. Psychopharmacology (Berl). 2012;223(4):489-499. doi: 10.1007/s00213-012-2740-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Metrik J, Rohsenow DJ, Monti PM, et al. Effectiveness of a marijuana expectancy manipulation: Piloting the balanced-placebo design for marijuana. Exp Clin Psychopharmacol. 2009;17(4):217-225. doi: 10.1037/a0016502 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Heishman SJ, Stitzer ML, Yingling JE. Effects of tetrahydrocannabinol content on marijuana smoking behavior, subjective reports, and performance. Pharmacol Biochem Behav. 1989;34(1):173-179. doi: 10.1016/0091-3057(89)90369-9 [DOI] [PubMed] [Google Scholar]
- 19.Cappell H, Pliner P. Regulation of the self-administration of marihuana by psychological and pharmacological variables. Psychopharmacologia. 1974;40(1):65-76. doi: 10.1007/BF00429448 [DOI] [PubMed] [Google Scholar]
- 20.Ramesh D, Haney M, Cooper ZD. Marijuana’s dose-dependent effects in daily marijuana smokers. Exp Clin Psychopharmacol. 2013;21(4):287-293. doi: 10.1037/a0033661 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Cooper ZD, Haney M. Comparison of subjective, pharmacokinetic, and physiological effects of marijuana smoked as joints and blunts. Drug Alcohol Depend. 2009;103(3):107-113. doi: 10.1016/j.drugalcdep.2009.01.023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hartman RL, Brown TL, Milavetz G, et al. Controlled cannabis vaporizer administration: blood and plasma cannabinoids with and without alcohol. Clin Chem. 2015;61(6):850-869. doi: 10.1373/clinchem.2015.238287 [DOI] [PubMed] [Google Scholar]
- 23.Huestis MA, Henningfield JE, Cone EJ. Blood cannabinoids. I. absorption of THC and formation of 11-OH-THC and THCCOOH during and after smoking marijuana. J Anal Toxicol. 1992;16(5):276-282. doi: 10.1093/jat/16.5.276 [DOI] [PubMed] [Google Scholar]
- 24.Karila L, Roux P, Rolland B, et al. Acute and long-term effects of cannabis use: a review. Accessed January 24, 2019. https://www.ingentaconnect.com/content/ben/cpd/2014/00000020/00000025/art00014 [DOI] [PubMed]
- 25.Volkow ND, Swanson JM, Evins AE, et al. Effects of cannabis use on human behavior, including cognition, motivation, and psychosis: a review. JAMA Psychiatry. 2016;73(3):292-297. doi: 10.1001/jamapsychiatry.2015.3278 [DOI] [PubMed] [Google Scholar]
- 26.Broyd SJ, van Hell HH, Beale C, Yücel M, Solowij N. Acute and chronic effects of cannabinoids on human cognition—a systematic review. Biol Psychiatry. 2016;79(7):557-567. doi: 10.1016/j.biopsych.2015.12.002 [DOI] [PubMed] [Google Scholar]
- 27.Crean RD, Crane NA, Mason BJ. An evidence based review of acute and long-term effects of cannabis use on executive cognitive functions. J Addict Med. 2011;5(1):1-8. doi: 10.1097/ADM.0b013e31820c23fa [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Crane NA, Schuster RM, Fusar-Poli P, Gonzalez R. Effects of cannabis on neurocognitive functioning: recent advances, neurodevelopmental influences, and sex differences. Neuropsychol Rev. 2013;23(2):117-137. doi: 10.1007/s11065-012-9222-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Ranganathan M, D’Souza DC. The acute effects of cannabinoids on memory in humans: a review. Psychopharmacology (Berl). 2006;188(4):425-444. doi: 10.1007/s00213-006-0508-y [DOI] [PubMed] [Google Scholar]
- 30.Lundqvist T. Cognitive consequences of cannabis use: comparison with abuse of stimulants and heroin with regard to attention, memory and executive functions. Pharmacol Biochem Behav. 2005;81(2):319-330. doi: 10.1016/j.pbb.2005.02.017 [DOI] [PubMed] [Google Scholar]
- 31.Ramaekers JG, Kauert G, van Ruitenbeek P, Theunissen EL, Schneider E, Moeller MR. High-potency marijuana impairs executive function and inhibitory motor control. Neuropsychopharmacology. 2006;31(10):2296-2303. doi: 10.1038/sj.npp.1301068 [DOI] [PubMed] [Google Scholar]
- 32.Stella N. Chronic THC intake modifies fundamental cerebellar functions. J Clin Invest. 2013;123(8):3208-3210. doi: 10.1172/JCI70226 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Pillay SS, Rogowska J, Kanayama G, et al. Cannabis and motor function: fMRI changes following 28 days of discontinuation. Exp Clin Psychopharmacol. 2008;16(1):22-32. doi: 10.1037/1064-1297.16.1.22 [DOI] [PubMed] [Google Scholar]
- 34.Klawitter J, Sempio C, Mörlein S, et al. An atmospheric pressure chemical ionization MS/MS assay using online extraction for the analysis of 11 cannabinoids and metabolites in human plasma and urine. Ther Drug Monit. 2017;39(5):556-564. doi: 10.1097/FTD.0000000000000427 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Huestis MA, Sampson AH, Holicky BJ, Henningfield JE, Cone EJ. Characterization of the absorption phase of marijuana smoking. Clin Pharmacol Ther. 1992;52(1):31-41. doi: 10.1038/clpt.1992.100 [DOI] [PubMed] [Google Scholar]
- 36.Haertzen CA, Hickey JE Addiction Research Center Inventory (ARCI): measurement of euphoria and other drug effects. Accessed January 1, 2016. https://link.springer.com/chapter/10.1007%2F978-1-4612-4812-5_24
- 37.Zuardi AW, Shirakawa I, Finkelfarb E, Karniol IG. Action of cannabidiol on the anxiety and other effects produced by δ 9-THC in normal subjects. Psychopharmacology (Berl). 1982;76(3):245-250. doi: 10.1007/BF00432554 [DOI] [PubMed] [Google Scholar]
- 38.Bidwell LC, Mueller R, YorkWilliams SL, Hagerty S, Bryan AD, Hutchison KE. A novel observational method for assessing acute responses to cannabis: preliminary validation using legal market strains. Cannabis Cannabinoid Res. 2018;3(1):35-44. doi: 10.1089/can.2017.0038 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Shacham S. A shortened version of the profile of mood states. J Pers Assess. 1983;47(3):305-306. doi: 10.1207/s15327752jpa4703_14 [DOI] [PubMed] [Google Scholar]
- 40.Metrik J, Kahler CW, McGeary JE, Monti PM, Rohsenow DJ. Acute effects of marijuana smoking on negative and positive affect. J Cogn Psychother. 2011;25(1):31-46. doi: 10.1891/0889-8391.25.1.31 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Hindocha C, Freeman TP, Xia JX, Shaban NDC, Curran HV. Acute memory and psychotomimetic effects of cannabis and tobacco both ‘joint’ and individually: a placebo-controlled trial. Psychol Med. 2017;47(15):2708-2719. doi: 10.1017/S0033291717001222 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Panee J, Gerschenson M, Chang L. Associations between microbiota, mitochondrial function, and cognition in chronic marijuana users. J Neuroimmune Pharmacol. 2018;13(1):113-122. doi: 10.1007/s11481-017-9767-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Petker T, Owens MM, Amlung MT, Oshri A, Sweet LH, MacKillop J. Cannabis involvement and neuropsychological performance: findings from the Human Connectome Project. J Psychiatry Neurosci. 2019;44(6):414-422. doi: 10.1503/jpn.180115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Thompson TAC, Wilson PH, Snyder PJ, et al. Sensitivity and test-retest reliability of the international shopping list test in assessing verbal learning and memory in mild Alzheimer’s disease. Arch Clin Neuropsychol. 2011;26(5):412-424. doi: 10.1093/arclin/acr039 [DOI] [PubMed] [Google Scholar]
- 45.Weintraub S, Dikmen SS, Heaton RK, et al. Cognition assessment using the NIH Toolbox. Neurology. 2013;80(11)(suppl 3):S54-S64. doi: 10.1212/WNL.0b013e3182872ded [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Weintraub S, Dikmen SS, Heaton RK, et al. The cognition battery of the NIH toolbox for assessment of neurological and behavioral function: validation in an adult sample. J Int Neuropsychol Soc. 2014;20(6):567-578. doi: 10.1017/S1355617714000320 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Bosker WM, Kuypers KPC, Theunissen EL, et al. Medicinal Δ(9)–tetrahydrocannabinol (dronabinol) impairs on-the-road driving performance of occasional and heavy cannabis users but is not detected in standard field sobriety tests. Addiction. 2012;107(10):1837-1844. doi: 10.1111/j.1360-0443.2012.03928.x [DOI] [PubMed] [Google Scholar]
- 48.Hirvonen J, Goodwin RS, Li C-T, et al. Reversible and regionally selective downregulation of brain cannabinoid CB1 receptors in chronic daily cannabis smokers. Mol Psychiatry. 2012;17(6):642-649. doi: 10.1038/mp.2011.82 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Yao B, Mackie K. Endocannabinoid receptor pharmacology. Curr Top Behav Neurosci. 2009;1:37-63. doi: 10.1007/978-3-540-88955-7_2 [DOI] [PubMed] [Google Scholar]
- 50.Flanagan JM, Gerber AL, Cadet JL, Beutler E, Sipe JC. The fatty acid amide hydrolase 385 A/A (P129T) variant: haplotype analysis of an ancient missense mutation and validation of risk for drug addiction. Hum Genet. 2006;120(4):581-588. doi: 10.1007/s00439-006-0250-x [DOI] [PubMed] [Google Scholar]
- 51.Cravatt BF, Giang DK, Mayfield SP, Boger DL, Lerner RA, Gilula NB. Molecular characterization of an enzyme that degrades neuromodulatory fatty-acid amides. Nature. 1996;384(6604):83-87. doi: 10.1038/384083a0 [DOI] [PubMed] [Google Scholar]
- 52.Huestegge L, Radach R, Kunert HJ. Long-term effects of cannabis on oculomotor function in humans. J Psychopharmacol. 2009;23(6):714-722. doi: 10.1177/0269881108091601 [DOI] [PubMed] [Google Scholar]
- 53.Zuurman L, Roy C, Schoemaker RC, et al. Effect of intrapulmonary tetrahydrocannabinol administration in humans. J Psychopharmacol. 2008;22(7):707-716. doi: 10.1177/0269881108089581 [DOI] [PubMed] [Google Scholar]
- 54.Klumpers LE, Beumer TL, van Hasselt JGC, et al. Novel Δ(9)–tetrahydrocannabinol formulation Namisol® has beneficial pharmacokinetics and promising pharmacodynamic effects. Br J Clin Pharmacol. 2012;74(1):42-53. doi: 10.1111/j.1365-2125.2012.04164.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Greenberg HS, Werness SAS, Pugh JE, Andrus RO, Anderson DJ, Domino EF. Short-term effects of smoking marijuana on balance in patients with multiple sclerosis and normal volunteers. Clin Pharmacol Ther. 1994;55(3):324-328. doi: 10.1038/clpt.1994.33 [DOI] [PubMed] [Google Scholar]
- 56.Hafstrom A, Patel M, Modig F, Magnusson M, Fransson PA. Acute alcohol intoxication impairs segmental body alignment in upright standing. J Vestib Res. 2014;24(4):297-304. doi: 10.3233/VES-140513 [DOI] [PubMed] [Google Scholar]
- 57.Liguori A, Gatto CP, Jarrett DB. Separate and combined effects of marijuana and alcohol on mood, equilibrium and simulated driving. Psychopharmacology (Berl). 2002;163(3-4):399-405. doi: 10.1007/s00213-002-1124-0 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Trial protocol
eMethods. Supplemental methods
eResults. Results of the tests of potency assignment within forms of cannabis (flower and concentrate)
eTable 1. Results of the tests of potency-by-change over time interactions for flower users
eTable 2. Results of the tests of potency-by-change over time interactions for concentrate users
eFigure 1. Cognitive performance after use of cannabis by cannabis form and potency during acute modile lab session
eFigure 2. Balance function after use of cannabis by cannabis form and potency during acute mobile lab session