

To the Editor: Syphilis is a sexually transmitted disease caused by Treponema pallidum (T. pallidum). Secondary syphilitic lesions usually occur within 3 months after the initial exposure to T. pallidum. The most frequent skin manifestations of secondary syphilis are macular and papular eruptions. However, other uncommon lesions, such as nodular, pustular, arcuate, and psoriasis-like lesions, have been occasionally reported.[1,2] Annular syphilitic lesions are relatively rare and usually present as multiple lesions scattered over the body or are limited to local skin such as genital.[1,3] Herein, we report a solitary annular lesion of secondary syphilis on the face.
A 33-year-old man presented with an annular plaque on his left jaw that appeared 4 weeks ago and had centrifugally expanded. The lesion was non-pruritic and painless. Physical examination revealed a solitary well-demarcated annular plaque with slightly raised, infiltrated ridges with fine scaling and a diameter of 5.5 cm on the patient's left jaw [Figure 1A]. There were no other skin lesions, but lymphadenopathy was observed in his left sub-maxillary region. A surgical biopsy revealed superficial and deep perivascular and hair follicles were infiltrated with numerous plasma cells, lymphocytes and eosinophils, as well as acanthosis and orthokeratosis with poly-morphonuclear neutrophils exudate in the epidermis [Figure 1B and 1C]. An immunohistochemical analysis with an anti-T. pallidum antibody showed the presence of numerous spirochetes in the epidermis [Figure 1D]. Further serum examinations showed a positive T. pallidum particle assay, and a toluidine red unheated serum test revealed a titer of 1:64. The hepatitis and anti-human immunodeficiency virus antibody serology tests were both negative. Upon further inquiry, the patient admitted that he had several episodes of unprotected extramarital sex 8 weeks prior to the skin eruptions. The diagnosis of secondary syphilis was confirmed. The patient was treated with benzathine penicillin G, 2.4 million units by intramuscular injection once a week for three consecutive weeks. His skin lesions disappeared 4 weeks after the end of treatment. The patient is still being followed up.
Figure 1.
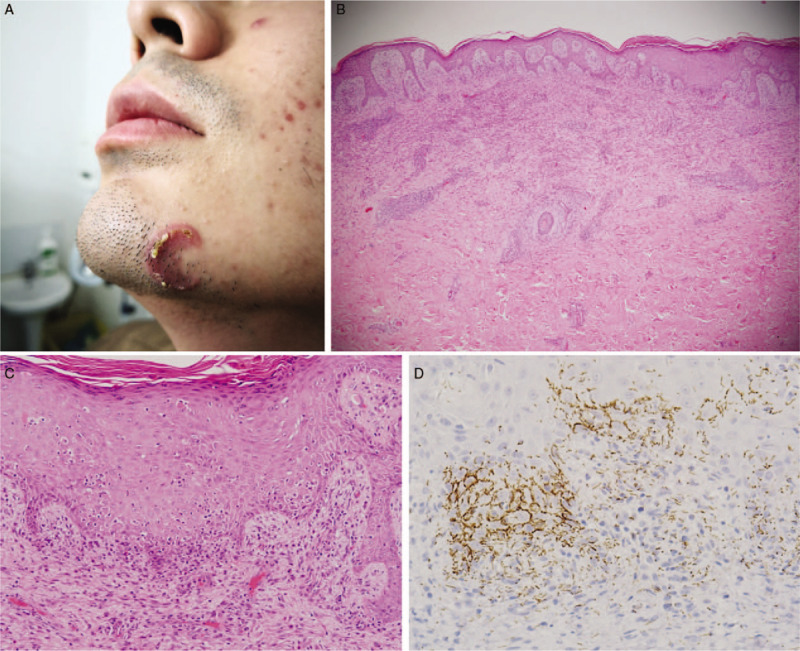
(A) A solitary annular plaque on the patient's left jaw. (B, C) Section of biopsy showing superficial and deep perivascular inflammatory infiltration with numerous plasma cells, lymphocytes and eosinophils, as well as acanthosis and orthokeratosis with poly-morphonuclear neutrophils exudate in the epidermis (hematoxylin-eosin staining, original magnification ×40, ×200, respectively). (D) Immunohistochemical staining showing numerous spirochetes in the epidermis (original magnification ×400).
Because the patient's skin lesion was located only on his face, clinical differential diagnoses including granuloma annulare, tinea faciei, plaque psoriasis, and sub-acute cutaneous lupus erythematosus were possible. It is difficult to distinguish these diseases simply by the morphological characteristics of the lesion. Histopathology can be helpful for diagnosis in cases with atypical manifestations. Previous studies have revealed that interstitial inflammation, plasma cells, endothelial swelling, irregular acanthosis, and elongated rete ridges were the most common histologic changes of secondary syphilis.[4,5] Particularly, as reported in some studies, the presence of plasma cells ranging from 74% to 86.4% raises the possibility of secondary syphilis.[4,5] Additionally, immunohistochemistry directed at T. pallidum is a more sensitive and specific method than the traditional silver stain for detecting spirochetes in formalin-fixed, paraffin-embedded tissue of secondary syphilis.[4] In conclusion, secondary syphilis continues to be a diagnostic challenge for clinicians owing to its protean cutaneous presentations. When confronted with rare skin lesions, especially among sexually active young adults, clinicians should consider syphilis as a differential diagnosis.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understand that his names and initials will not be published and due efforts will be made to conceal his identity, but anonymity cannot be guaranteed.
Conflicts of interest
None.
Footnotes
How to cite this article: Wu J, Chen H, Long FQ. A solitary annular plaque on the jaw: atypical presentation of secondary syphilis. Chin Med J 2020;133:1383–1384. doi: 10.1097/CM9.0000000000000807
References
- 1.Balagula Y, Mattei PL, Wisco OJ, Erdag G, Chien AL. The great imitator revisited: the spectrum of atypical cutaneous manifestations of secondary syphilis. Int J Dermatol 2014; 53:1434–1441. doi: 10.1111/ijd.12518. [DOI] [PubMed] [Google Scholar]
- 2.Li F, Wang T, Wang L. Secondary syphilis primarily presenting with multiple nodules on the scalp: case report and published work review. J Dermatol 2017; 44:1401–1403. doi: 10.1111/1346-8138.13965. [DOI] [PubMed] [Google Scholar]
- 3.Knöpfel N, Del Pozo LJ, Díaz I. Solitary annular plaque on the scrotum. Am J Dermatopathol 2016; 38:930–931. doi: 10.1097/DAD.0000000000000389. [DOI] [PubMed] [Google Scholar]
- 4.Flamm A, Parikh K, Xie Q, Kwon EJ, Elston DM. Histologic features of secondary syphilis: a multicenter retrospective review. J Am Acad Dermatol 2015; 73:1025–1030. doi: 10.1016/j.jaad.2015.08.062. [DOI] [PubMed] [Google Scholar]
- 5.Liu XK, Li J. Histologic features of secondary syphilis. Dermatology 2019; 19:1–6. doi: 10.1159/000502641. [DOI] [PubMed] [Google Scholar]