

Once upon a time…
… a novel coronavirus was described in China. The new year 2020 had just arrived full of hope and promise. Portugal was preparing to defend its European Football Champion title. And China was far far away.
Suddenly, something changed. The virus had a name, as did the disease it caused. The cases were spreading fast and arrived in Europe. Now, the threat was real. Portugal was panicking with suspected cases and the scientific community was warning of a lack of preparedness.
And it arrived indeed on March 2nd.
Then what?
Epidemiologists began to develop mathematical models to predict the epidemic, describing different scenarios.1 The predicted peak in the number of cases in Portugal could be as high as 2.5 million.1
As the days went by, journalists and television commentators were becoming “experts” in epidemiology. Recommendations from health authorities were extensively publicized in the media.
Anticipating the worst-case scenario and keeping an eye on other European countries, the state of emergency was officially declared in Portugal on March 18th. And, in the name of public health, individual freedom was suspended.
Contingency plans were adopted across the National Health Service and the rule was clear: only emergencies allowed!2
The number of cases began to rise. And the testing capacity was struggling to meet the high demand. Investigators advised that scaling up testing could be cost-saving, since early isolation would lead to prevention of new infections and fewer hospitalizations.3
Scientific knowledge was evolving…
… but a lot of uncertainties remained… COVID-19 had too many faces4 and asymptomatic carriers were an unsolved mystery.4
Clinical evidence kept growing, and recommendations for intensive care approach to COVID-19 patients were published.5 Safety of health-care professionals was a major concern, especially regarding aerosol-generating procedures. Non-invasive ventilation and high-flow nasal cannula oxygen therapy were a controversial subject. A literature search found a window of opportunity for those strategies in some non-severe patients.6
About all the potential COVID-19 therapies, was there something missing? Potential benefits from a drug widely used in asthmatic patients – Montelukast – were proposed and are being submitted to investigation in a clinical trial.
What's coming next?
Coming to a point where the curve of new infection cases is progressively declining (Fig. 1 ), it is time to look forward.
Fig. 1.
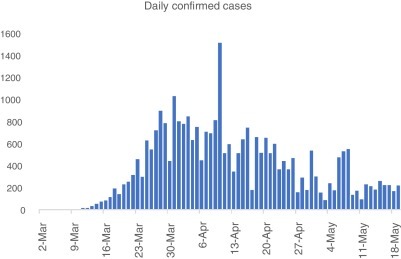
Daily confirmed cases of SARS-CoV-2 infection in Portugal (from 2nd March until 19th May).
The persistence of the virus in the community increases the risk of new mutations. Until now, 436 genomes were analyzed in Portugal.7 350 mutations were already identified, with a mean number of mutations by genome of 8. These results are compatible with the mutation rate predicted for SARS-CoV-2 – about 2 mutations/genome/month.
A lot of concerns arise, but with the arrival of spring and summer in the Northern hemisphere, encouraging data are coming in as well.
While waiting for a vaccine, it is important to talk about herd immunity. It's currently believed that herd immunity to SARS-CoV-2 infection requires 60–70% of immune individuals. However, individual variation in biological susceptibility and exposure (heterogeneity of populations) needs to be considered, as it accelerates the acquisition of immunity in populations – this can reduce the herd immunity threshold to 10–20%.8
COVID-19 has dominated our minds over the previous months. But what was left behind?
Many health activities were neglected and an excess mortality was described, 3–5 fold higher than can be explained by the official COVID-19 deaths.9 And this is probably just the tip of the iceberg.
This story ends with the words of a pulmonologist: we must learn how to evolve in the wake of these new Coronaviruses, the nCoVs, to make a sustained and responsible change in our behaviour and attitudes. New citizens, new mankind: 2020-nMan.10
After it all ends, let's just hope to live happily ever after.
For this storytelling, a literature search on Portuguese publications on COVID-19 was performed. Up to May 19th, 43 articles were retrieved, 11 of them not peer-reviewed and distributed by preprint server – medRxiv. Among the studies already published, 11 were in Portuguese journals and 21 in international journals. The mean impact factor was 3.044.
References
- 1.Pais R.J., Taveira N. Predicting the evolution and control of the COVID-19 pandemic in Portugal. F1000Research. 2020;9:283. doi: 10.12688/f1000esearch.23401.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Drummond M. Sleep labs, lung function tests and COVID-19 pandemic – only emergencies allowed! Pulmonology. 2020 doi: 10.1016/j.pulmoe.2020.04.002. S2531-0437(20)30089-1 [published online ahead of print, 27.04.20] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sousa-Pinto B., Almeida Fonseca J., Costa-Pereira A., Rocha Gonçalves F.N. Is scaling-up COVID-19 testing cost-saving? medRxiv. 2020 doi: 10.1101/2020.03.22.20041137. [DOI] [Google Scholar]
- 4.Ferreira-Santos D., Maranhão P., Monteiro-Soares M. Identifying baseline clinical features of people with COVID-19. medRxiv. 2020 doi: 10.1101/2020.05.13.20100271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mendes J.J., Mergulhão P., Froes F., Paiva J.A., Gouveia J. Recommendations from the Sociedade Portuguesa de Cuidados Intensivos and Infection & Sepsis Group for intensive care approach to COVID-19. Rev Bras Ter Intensiva. 2020;32:2–10. doi: 10.5935/0103-507x.20200002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Winck J.C., Ambrosino N. COVID-19 pandemic and non invasive respiratory management: every Goliath needs a David. An evidence based evaluation of problems. Pulmonology. 2020 doi: 10.1016/j.pulmoe.2020.04.013. S2531-0437(20)30093-3 [published online ahead of print, 27.04.20] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.INSA. Diversidade genética do novo coronavírus SARS-CoV-2 (COVID-19) em Portugal. Ponto de situação 2020.05.12. Available from: https://insaflu.insa.pt/covid19/relatorios/INSA_SARS_CoV_2_DIVERSIDADE_GENETICA_relatorio_situacao_2020-05-12.pdf [accessed 19.05.20].
- 8.Gomes M.G.M., Corder R.M., King J.G., Langwig K.E., Souto-Maior C., Carneiro J. Individual variation in susceptibility or exposure to SARS-CoV-2 lowers the herd immunity threshold. medRxiv. 2020 doi: 10.1101/2020.04.27.20081893. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Nogueira P.J., Nobre M.A., Nicola P.J., Furtado C., Vaz Carneiro A. Excess mortality estimation during the COVID-19 pandemic: preliminary data from Portugal. Acta Med Port. 2020;33:376–383. doi: 10.20344/amp.13928. [DOI] [PubMed] [Google Scholar]
- 10.Froes F. And now for something completely different: from 2019-nCoV and COVID-19 to 2020-nMan. Pulmonology. 2020;26:114–115. doi: 10.1016/j.pulmoe.2020.02.010. [DOI] [PMC free article] [PubMed] [Google Scholar]