

This cross-sectional study examines the association of weight-adjusted doses of caffeine alone, a β-blocker alone, or a β-blocker and caffeine combination with surgical performance of vitreoretinal ophthalmology fellows during simulated vitreoretinal microsurgery.
Key Points
Question
Is there an association of weight-adjusted doses of caffeine alone, a β-blocker (propranolol) alone, or a β-blocker and caffeine combination with surgical performance by novice vitreoretinal surgeons?
Findings
In this cross-sectional study of 15 vitreoretinal surgical fellows, propranolol alone was associated with improved surgical performance compared with caffeine alone and the combination of caffeine and propranolol.
Meaning
The findings suggest that caffeine is negatively associated with surgical performance among novice vitreoretinal surgeons but that addition of propranolol is associated with improved performance.
Abstract
Importance
Vitreoretinal surgery can be technically challenging and is limited by physiologic characteristics of the surgeon. Factors that improve accuracy and precision of the vitreoretinal surgeon are invaluable to surgical performance.
Objectives
To establish weight-adjusted cutoffs for caffeine and β-blocker (propranolol) intake and to determine their interactions in association with the performance of novice vitreoretinal microsurgeons.
Design, Settings, and Participants
This single-blind cross-sectional study of 15 vitreoretinal surgeons who had less than 2 years of surgical experience was conducted from September 19, 2018, to September 25, 2019, at a dry-laboratory setting. Five simulations were performed daily for 2 days. On day 1, performance was assessed after sequential exposure to placebo, low-dose caffeine (2.5 mg/kg), high-dose caffeine (5.0 mg/kg), and high-dose propranolol (0.6 mg/kg). On day 2, performance was assessed after sequential exposure to placebo, low-dose propranolol (0.2 mg/kg), high-dose propranolol (0.6 mg/kg), and high-dose caffeine (5.0 mg/kg).
Interventions
Surgical simulation tasks were repeated 30 minutes after masked ingestion of placebo, caffeine, or propranolol pills during the 2 days.
Main Outcomes and Measures
An Eyesi surgical simulator was used to assess surgical performance, which included surgical score (range, 0 [worst] to 700 [best]), task completion time, intraocular trajectory, and tremor rate (range, 0 [worst] to 100 [best]). The nonparametric Friedman test followed by Dunn-Bonferroni post hoc test was applied for multiple comparisons.
Results
Of 15 vitreoretinal surgeons, 9 (60%) were male, with a mean (SD) age of 29.6 (1.4) years and mean (SD) body mass index (calculated as weight in kilograms divided by height in meters squared) of 23.15 (2.9). Compared with low-dose propranolol, low-dose caffeine was associated with a worse total surgical score (557.0 vs 617.0; difference, –53.0; 95% CI, –99.3 to –6.7; P = .009), a lower antitremor maneuver score (55.0 vs 75.0; difference, –12.0; 95% CI, –21.2 to –2.8; P = .009), longer intraocular trajectory (2298.6 vs 2080.7 mm; difference, 179.3 mm; 95% CI, 1.2-357.3 mm; P = .048), and increased task completion time (14.9 minutes vs 12.7 minutes; difference, 2.3 minutes; 95% CI, 0.8-3.8 minutes; P = .048). Postcaffeine treatment with propranolol was associated with performance improvement; however, surgical performance remained inferior compared with low-dose propranolol alone for total surgical score (570.0 vs 617.0; difference, –51.0; 95% CI, –77.6 to –24.4; P = .01), tremor-specific score (50.0 vs 75.0; difference, –16.0; 95% CI, –31.8 to –0.2; P = .03), and intraocular trajectory (2265.9 mm vs 2080.7 mm; difference, 166.8 mm; 95% CI, 64.1-269.6 mm; P = .03).
Conclusions and Relevance
The findings suggest that performance of novice vitreoretinal surgeons was worse after receiving low-dose caffeine alone but improved after receiving low-dose propranolol alone. Their performance after receiving propranolol alone was better than after the combination of propranolol and caffeine. These results may be helpful for novice vitreoretinal surgeons to improve microsurgical performance.
Introduction
Vitreoretinal surgery is one of the most technically challenging microsurgical procedures,1 derived in part from inherent human physiologic limits including tremor, precision, visual resolution, ability to sense microforces on underlying tissue, and fatigue. The level of surgical difficulty is also associated with innate properties of the target retinal tissues, which are delicate, transparent, nonregenerative, and critical to visual function.2,3,4
Virtual training simulators provide quantitative feedback on parameters of surgical precision, such as surgeon microtremor and accuracy of task completion, among other relevant measurements. Of importance, the use of the device allows better preparation for surgical performance and is associated with improvement in the individual skills required of novice surgeons.5,6 To be most useful, a simulator for vitreoretinal surgery requires a realistic retinal image and retinal tissue response to instrument manipulation.7,8 The ophthalmic surgical simulator Eyesi Surgical (VRmagic Holding AG) is a widely used virtual simulator for anterior segment and vitreoretinal surgical procedures.9,10
Consistent with the goal of improving microsurgical performance, the literature11,12 describes potential factors associated with surgical precision. Among these, all individuals have upper extremity physiologic oscillations that manifest as a fine tremor and may become more pronounced during stressful periods. Previous reports13,14 have described strategies to reduce physiologic oscillations and enhance manual dexterity, most of which can be categorized broadly into either postural considerations or pharmacologic interventions.13,14 Pharmacologic intervention with β-blockers (eg, propranolol and timolol)15,16 has been studied for its association with decreasing anxiety and hand tremor, thereby improving surgical precision. In contrast, an apparent correlation was reported between coffee consumption and impaired microsurgical performance by surgeons who identified as normally having a low-caffeine diet.17
The current study was designed to objectively analyze the individual performance of novice vitreoretinal surgeons exposed to various weight-adjusted doses of caffeine alone, propranolol alone, or a combination of caffeine and propranolol, 2 potentially opposing factors. The primary objective was to assess weight-based doses of propranolol and caffeine that would be associated with change of microsurgical skills during vitreoretinal surgery. The secondary outcome was to assess whether there was a potential role for the addition of propranolol to neutralize the caffeine effects in this setting.
Methods
Study Design and Participants
The Committee of Ethics of the Universidade Federal de São Paulo in Brazil approved this single-blind cross-sectional study, which was conducted according to the tenets of the Declaration of Helsinki.18 All participants provided written informed consent. No incentives or financial compensation were offered to participants to join the study. From September 19, 2018, to September 25, 2019, 15 vitreoretinal fellows from the Retinal Division of the Ophthalmology Department of the Universidade Federal de São Paulo with fewer than 2 years of surgical experience were enrolled. The exclusion criteria included daily caffeine consumption exceeding two 8-oz cups or systemic medical conditions (eg, asthma, cardiac or neurologic disease, or mental illness). Before entry into the research protocol, electrocardiography was performed for each surgeon and an oral dose of propranolol (0.6 mg/kg) was administered to test for adverse reactions.
Eyesi Surgical Simulator
The current study19 was conducted using the commercially available Eyesi software, version 3.4.2 (VRMagic Holding AG). The simulator combines training of basic skills with challenging surgical procedures in increasing levels of difficulty. The surgeon must meet a required performance level for each task to advance successfully to the next step. In this study, we established in advance that any score higher than 0 was sufficient for the operator to go to the next step. At the end of each training module, the Eyesi simulator presents a total score of 100 for each task together with a detailed performance summary.20,21,22,23
Simulated Surgical Protocol
The surgical skills were assessed during 2 nonsequential days. Blood pressure and heart rate were measured before and after each drug exposure followed by a scored simulated surgical performance analysis. The following fixed sequence of 7 tasks for posterior-segment surgery was repeated throughout the study: navigation exercise, antitremor maneuver, bimanual dumbbells touching, bimanual scissors task, posterior hyaloid detachment, epiretinal membrane peeling, and inner limiting membrane peeling. The antitremor maneuver was a task that was part of the simulation sequence that focused on quantifying tremor. Evaluation of the microsurgical technique occurred 30 to 60 minutes after ingestion of caffeine or propranolol to guarantee sufficient time for each intervention to reach a peak plasma drug concentration. The timing was in accordance with protocols of previously published and well-accepted work.17,24,25,26
To become familiar with the technology, all surgeons underwent a training period of at least 2 hours in the posterior-segment training module on the simulator. The training occurred on the day before the day of data collection. Surgeons were instructed to maintain their daily coffee consumption routine on the day of analysis because acute caffeine withdrawal may be associated with tremor in acclimated users.27 The research team administered placebo, caffeine, and propranolol pills, all of which were visually identical, making this a single-blinded experiment. The adjustment of the propranolol and caffeine doses based on weight were in accordance with a previously published study.24
Figure 1 summarizes the study flowchart for day 1 and day 2 of analysis. The main outcome measures evaluated for all 7 tasks were the total task score generated by the Eyesi platform, which ranges from 0 (worst) to 700 (best); the total time to task completion (minutes); and the total intraocular trajectory of the surgical tool tip, also called odometer (mm). The amount of hand tremor was assessed by the antitremor maneuver score ranging from 0 (worst) to 100 (best).
Figure 1. Study Flowchart of External Interventions.

Statistical Analysis
The sample size calculation was performed using PASS, version 14 (NCSS Statistical Software). A sample size of 14 was calculated to detect a 10-point difference in Eyesi mean score for each task after drug ingestion compared with placebo, with an SD of 14.5 points. The study was powered for 0.80 and P = .05. The data were analyzed by repeated measures analysis of variance with the Geisser-Greenhouse Corrected F.
Statistical analysis was performed using Stata, version 12 (StataCorp LLC) and SPSS, version 20 (IBM Corp). The nonparametric Friedman test followed by the Dunn-Bonferroni post hoc test was applied for multiple comparisons. As a paired analysis, the differences in medians were calculated as the median of day 1 minus day 2 (median [day 1 – day 2]) and not the median of day 1 minus the median of day 2 (median [day 1] – median [day 2]). The values are expressed as the median and correspondent 95% CI. All statistical tests were 2-sided using a significance level set at P < .05.
Results
A total of 15 vitreoretinal fellows (9 [60%] men; mean [SD] age, 29.6 [1.4] years; mean [SD] body mass index, 23.15 [2.9] [calculated as weight in kilograms divided by height in meters squared]) with less than 2 years of surgical experience were recruited for the study. No surgeon was excluded, and no adverse effects were reported or observed for any surgeon. All surgeons were right handed. The mean (SD) baseline caffeine consumption reported was 1.27 (1.03) cups per day. There were no differences in demographic characteristics or daily caffeine intake. Systemic blood pressure and heart rate were measured before and after each external exposure, and the values were always equal or above 120/80 mm Hg for blood pressure and 60 beats/min for heart rate.
No differences in performance between the 2 days of testing were seen after the combined medication intake and placebo pill ingestion in the following parameters: Eyesi total score, tool intraocular trajectory, time to task completion, or amount of tremor (Figure 2). When treated with low-dose caffeine vs low-dose propranolol, surgeons had a lower total score (557.0 vs 617.0; difference, –53.0; 95% CI, –99.3 to –6.7; P = .009), a lower antitremor maneuver score (55.0 vs 75.0; difference, –12.0; 95% CI, –21.2 to –2.8; P = .009), longer intraocular trajectory (2298.6 vs 2080.7 mm; difference, 179.3 mm; 95% CI, 1.2-357.3 mm; P = .048), and increased task completion time (14.9 minutes vs 12.7 minutes; difference, 2.3 minutes; 95% CI, 0.8-3.8 minutes; P = .048). Median differences between days 1 and 2 with corresponding P values for Eyesi surgical-generated score (eTable 1 in the Supplement), tremor-specific task score (eTable 2 in the Supplement), intraocular trajectory (eTable 3 in the Supplement), and task completion time (eTable 4 in the Supplement) are recorded.
Figure 2. Results After External Exposure During the 2-Day Analysis.
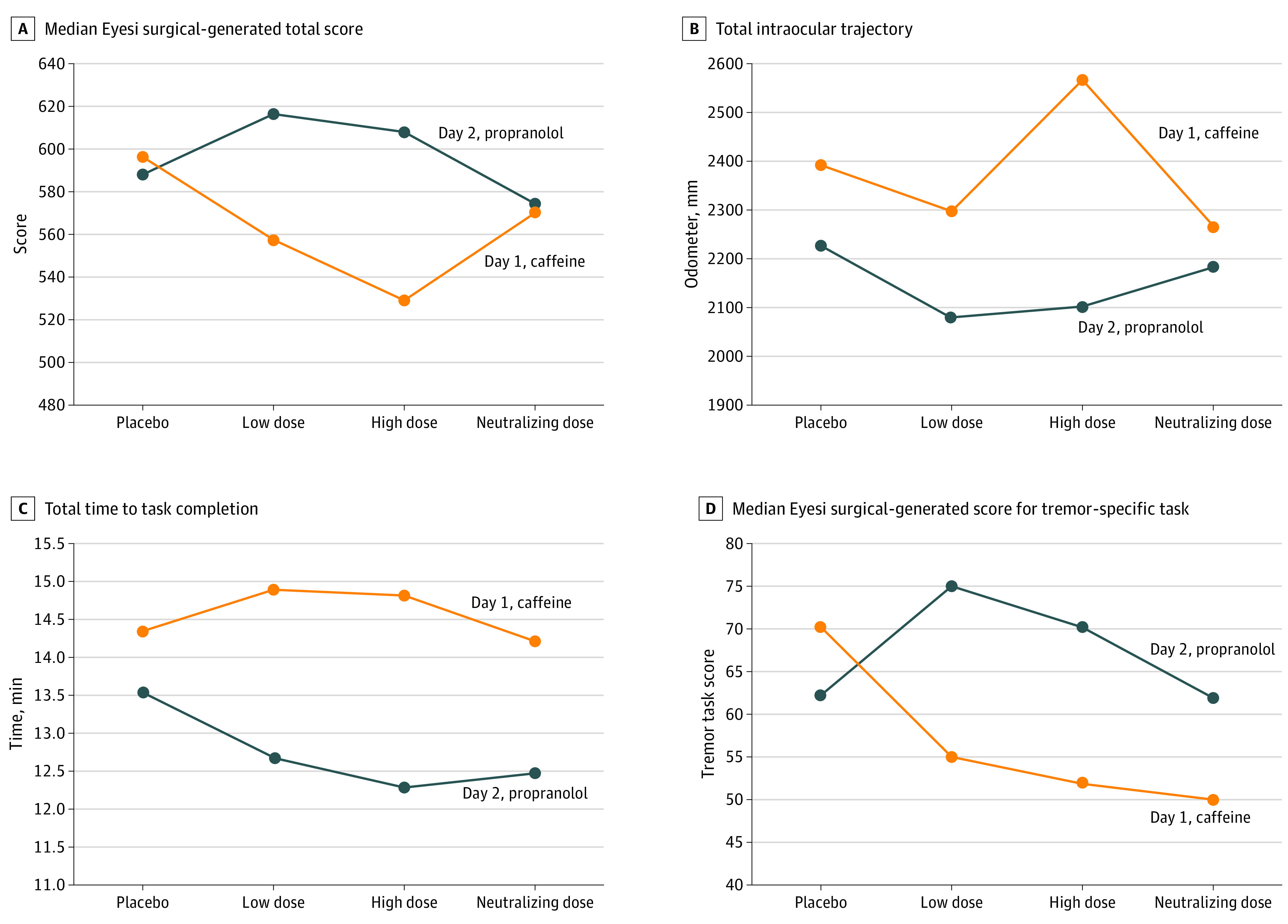
On day 1, the low dose of caffeine was 2.5 mg/kg, the high dose of caffeine was 5 mg/kg, and the neutralizing dose of propranolol was 0.6 mg/kg. On day 2, the low dose of propranolol was 0.2 mg/kg, the high dose of propranolol was 0.6 mg/kg, and the neutralizing dose of caffeine was 5 mg/kg.
Propranolol administered after caffeine was associated with enhanced overall hand dexterity. However, this improvement remained inferior to that observed with low-dose propranolol alone for total surgical score (570.0 vs 617.0; difference, –51.0; 95% CI, –77.6 to –24.4; P = .01), tremor-specific score (50.0 vs 75.0; difference, –16.0; 95% CI, –31.8 to –0.2; P = .03), and pathway inside the eye (2265.9 vs 2080.7 mm; difference, 166.8 mm; 95% CI, 64.1 mm to 269.6 mm; P = .03). After exposure to the final neutralizing agent, there were no differences between day 1 and day 2 in the generated surgical score, total time to task completion, and intraocular trajectory.
Discussion
The results of our prospective cross-sectional study showed that overall the combined ingestion of caffeine and propranolol was associated with surgeons achieving their own placebo-level performance. These data also suggest that preoperative ingestion of caffeine by a novice surgeon can neutralize to a large extent the deleterious association with hand dexterity by receiving a 0.6 mg/kg dose of propranolol. However, receiving propranolol after caffeine was not associated with improved overall hand dexterity compared with propranolol alone. The current results provide supporting evidence for avoiding even low-dose caffeine in the hours before performing surgical procedures by nonhabitual caffeine users to maintain overall performance capability.
Arnold et al28 obtained similar results when studying hand movement, amplified by a handheld laser pointer, among ophthalmology trainees after their ingestion of fixed low-dose caffeine (200 mg), 12.5 mg of timolol (another β-blocker), a combination of caffeine and timolol, or placebo. The authors described increased hand steadiness after consumption of timolol combined with caffeine compared with caffeine alone.
Similarly, Jacobson et al24 analyzed nonphysician, caffeine-naive women by recording the error time and frequency in static and dynamic delicate manual tasks. The experiments occurred 30 to 60 minutes after caffeine ingestion, a time of the peak plasma caffeine concentrations. The authors24 found differences in the hand steadiness error time and tracing error time and frequency for the 5-mg/kg dose of caffeine but not for the 2.5-mg/kg dose or placebo. Changes occurred with both the 5.0-mg/kg and 2.5-mg/kg doses for only the hand steadiness error frequency. The authors24 concluded that both low- and high-dose caffeine were negatively associated with selected performance skills. The low dose of caffeine established in that study (2.5 mg/kg) and in the current study represents approximately a 25-mL cup of espresso29 or an 8-oz cup of drip or percolated coffee30,31 for a person weighing 70 kg. Regarding very low doses of caffeine, Mürbe et al32 found no change in the tremor amplitude after consumption of 50 mg of caffeine.
The terms low dose and high dose in the current protocol simply standardized the amount of weight-adjusted caffeine and propranolol intake because high and low doses of these medications are different in the treatment of other diseases. The dose of propranolol for a person weighing 70 kg that is used to treat benign essential tremor ranges from 1.7 mg/kg to 3.4 mg/kg,33 whereas it ranges from 0.8 mg/kg to 9.1 mg/kg for systemic hypertension.34 Therefore, high-dose propranolol in this protocol of 0.6 mg/kg would be considered low dose in other clinical disease settings.
Propranolol is widely used to treat tremor-related diseases, systemic hypertension, heart rhythm disorders, and other heart or circulatory conditions. The most common adverse effects are nausea, diarrhea, bradycardia, hypotension, paresthesia, lightheadedness, and lethargy.35 However, because propranolol-related adverse effects are dose dependent, at low doses, most of these effects are mild and transient.36 No adverse effects associated with propranolol were reported among the participants in this study, which is likely because of the low dose of the medication used.
Our finding that propranolol use was associated with improved surgical performance and decreased surgical tremor can be explained by β-blocker pharmacologic characteristics. β-Blockers bind competitively to heart and smooth muscle β-receptors, thereby diminishing the sympathetically mediated cardiovascular effects of stress, peripheral muscle tremor, and central anxiety. Left untreated, these sympathetic responses may jeopardize performance when a complex task is being performed.37 It is important to emphasize that β-blockers may be unsuitable for surgeons with underlying asthma, cardiac conduction disorders, diabetes, and peripheral vascular disease.38
Although there was no difference between low-dose exposure of propranolol or caffeine and baseline Eyesi-generated surgical score, there was a progressive dose-dependent difference in scores between the 2 days. Our results agree with those of Pointdujour et al,13 who reported that administration of a fixed amount of propranolol (10 mg) or caffeine (200 mg) was not associated with the Eyesi score compared with the baseline performance among physicians who were more experienced than an ophthalmology resident.
The cumulative trajectory length of the instrument tip inside the eye was shorter after receiving low-dose propranolol compared with receiving low-dose caffeine (suggesting conservation of movement associated with use of propranolol). Receiving low-dose propranolol was also associated with shortened time to task completion compared with low-dose caffeine. Foster et al39 reported a potential confounding effect (ie, increase in time of surgeon’s reaction time after receiving 40 mg of oxprenolol, a different class of β-blocker) but no association with accuracy or tremor.
We found that the doses of caffeine and propranolol associated with modification of surgical microtremor were similar to those associated with changes in intraocular trajectory and total time for task completion (low-dose propranolol vs low-dose caffeine). In contrast, Lubahn et al40 did not find a beneficial association between hand tremor and a fixed dose of timolol 12.5 mg. However, Elman et al41 reinforced the hypothesis of the beneficial association with high-dose propranolol and reported a subjective decrease in tremor and anxiety by ophthalmology residents, but the group could not demonstrate improved surgical outcome.
In contrast to our study results, Humayun et al15 reported a mean decrease in hand tremor associated with oral propranolol at a fixed low dose (10 mg) compared with baseline performance. However, there were fundamental differences in the methods between the studies. Their study15 did not adjust the medication dose according to the participant’s weight; both men and women were included. Their study results15 focused on measuring static hand steadiness by asking surgeons to hold an endoillumination probe at a preset target location, whereas in our protocol, tremor was quantified during a dynamic surgical task. In accordance with our study, their study results15 confirmed no difference in performance between low-dose caffeine and placebo.
The associations of high-dose propranolol and high-dose caffeine were neutralized by exposure to the high dose of the combined drug (caffeine and propranolol); on completion of the final protocol step, the performance was the same on days 1 and 2, which suggests the difference in performance was associated with the prescribed external exposure.
Despite the knowledge that caffeine is associated with decreased surgical performance and increased hand tremor,11 its negative association with microsurgery appears to be partially attenuated by tolerance. Caffeine-naive individuals have a more pronounced decrease in dexterity compared with those who are regular coffee drinkers.15,42 Caffeinated beverages are widely consumed by surgeons and residents sometimes because of their long working hours and consequent fatigue.43 Therefore, to avoid bias, we recommended that all study participants maintain their regular daily caffeine intake routine.
In addition, the requirement for 2 hours of previous nonconsecutive surgical training with the Eyesi surgical simulator in the posterior-segment module was adopted by this protocol to avoid bias. Urso-Baiarda et al17 reported that the results of a crossover study that investigated the adverse effect of low-dose caffeine intake by novice microsurgeons was affected by a learning curve. Their protocol allocated participants to receive either placebo in the morning and caffeine in the afternoon or the reverse treatment. Receiving caffeine followed by placebo was associated with improved microsurgical skills from the morning to the afternoon, whereas the reverse treatment was associated with no improvement.
Strengths and Limitations
A strength of this research is that the physiologic association with vitreoretinal surgical performance is described in the context of a balanced interaction between caffeine and β-blockers. The current study has some limitations. First, when performing a multifactorial comparison on the same day of analysis, a higher dose of propranolol was associated with progressive score improvement, a reduction in the total time to task completion, a shorter trajectory inside the eye, and reduced tremor. An opposite phenomenon occurred after exposure to progressively higher caffeine doses. The significance of these findings might require an increase in the sample size, even though the current study was adequately powered to detect the external exposure association among vitreoretinal fellows. Second, our results were restricted to novice surgeons; future studies are required to assess whether the findings translate to more experienced vitreoretinal surgeons. Third, although Eyesi is the only simulator model for ophthalmologic training that has undergone comprehensive investigation, no published evidence supports the transfer of skills from the simulator to the operating room, to our knowledge.44 Consequently, there is still insufficient evidence to support propranolol intake by novice surgeons before performing surgical procedures, and further investigations are required to confirm the association between the performance changes demonstrated in this study and clinically significant differences in surgical outcomes.
Conclusions
This study suggests that young vitreoretinal surgeons who ingest caffeine before performing a surgical procedure may benefit from receiving a partially neutralizing dose of propranolol. However, the expected beneficial association of caffeine and propranolol combination may be no greater than the surgeon’s baseline performance. Moreover, receiving propranolol without caffeine may be associated with enhanced microsurgical performance by novice vitreoretinal surgeons. In this study, surgical performance after receiving caffeine and propranolol combination was inferior compared with receiving low-dose propranolol alone. These data may provide guidance regarding the association of receiving propranolol alone and the neutralization potential of receiving the propranolol and caffeine combination by novice microsurgeons who wish to improve their surgical performance.
eTable 1. Median Differences Between Days 1 and 2 With Corresponding P-value for the Eyesi Surgical-Generated Score
eTable 2. Median Differences Between Days 1 and 2 With the Corresponding P-value for the Eyesi Tremor-Specific Task Score
eTable 3. Median Difference Between Days 1 and 2 With the Corresponding P-value for the Intraocular Trajectory (Odometer)
eTable 4. Median Difference Between Days 1 and 2 With the Corresponding P-value for the Total Time for Task Completion
REFERENCES
- 1.Roizenblatt M, Edwards TL, Gehlbach PL. Robot-assisted vitreoretinal surgery: current perspectives. Robot Surg. 2018;5:1-11. doi: 10.2147/RSRR.S122301 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Vander Poorten E, Esteveny L, Gijbels A, et al. Use case for European robotics in ophthalmologic micro-surgery. In: Proceedings of the Fifth Joint Workshop on New Technologies for Computer/Robot Assisted Surgery; 2015:10-12. [Google Scholar]
- 3.He X, van Geirt V, Gehlbach P, Taylor R, Iordachita I. IRIS: integrated robotic intraocular snake. IEEE Int Conf Robot Autom. 2015;2015:1764-1769. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ida Y, Sugita N, Ueta T, Tamaki Y, Tanimoto K, Mitsuishi M. Microsurgical robotic system for vitreoretinal surgery. Int J Comput Assist Radiol Surg. 2012;7(1):27-34. doi: 10.1007/s11548-011-0602-4 [DOI] [PubMed] [Google Scholar]
- 5.Thomsen ASS, Bach-Holm D, Kjærbo H, et al. . Operating room performance improves after proficiency-based virtual reality cataract surgery training. Ophthalmology. 2017;124(4):524-531. doi: 10.1016/j.ophtha.2016.11.015 [DOI] [PubMed] [Google Scholar]
- 6.McCannel CA, Reed DC, Goldman DR. Ophthalmic surgery simulator training improves resident performance of capsulorhexis in the operating room. Ophthalmology. 2013;120(12):2456-2461. doi: 10.1016/j.ophtha.2013.05.003 [DOI] [PubMed] [Google Scholar]
- 7.Mukai N, Harada M, Muroi K, Miyamoto Y, Uratani A, Yano T. Development of a PC-based real-time surgical simulator. Syst Comput Jpn. 2002;33(7):11-20. doi: 10.1002/scj.10076 [DOI] [Google Scholar]
- 8.Hunter IW, Jones LA, Sagar MA, Lafontaine SR, Hunter PJ. Ophthalmic microsurgical robot and associated virtual environment. Comput Biol Med. 1995;25(2):173-182. doi: 10.1016/0010-4825(94)00042-O [DOI] [PubMed] [Google Scholar]
- 9.Deuchler S, Wagner C, Singh P, et al. . Clinical efficacy of simulated vitreoretinal surgery to prepare surgeons for the upcoming intervention in the operating room. PLoS One. 2016;11(3):e0150690. doi: 10.1371/journal.pone.0150690 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Selvander M, Asman P. Cataract surgeons outperform medical students in Eyesi virtual reality cataract surgery: evidence for construct validity. Acta Ophthalmol. 2013;91(5):469-474. doi: 10.1111/j.1755-3768.2012.02440.x [DOI] [PubMed] [Google Scholar]
- 11.Fargen KM, Turner RD, Spiotta AM. Factors that affect physiologic tremor and dexterity during surgery: a primer for neurosurgeons. World Neurosurg. 2016;86:384-389. doi: 10.1016/j.wneu.2015.10.098 [DOI] [PubMed] [Google Scholar]
- 12.Roizenblatt M, Grupenmacher AT, Belfort R Jr, Maia M, Gehlbach PL. Robot-assisted tremor control for performance enhancement of retinal microsurgeons. Br J Ophthalmol. 2019;103(8):1195-1200. doi: 10.1136/bjophthalmol-2018-313318 [DOI] [PubMed] [Google Scholar]
- 13.Pointdujour R, Ahmad H, Liu M, Smith E, Lazzaro D. B-Blockade affects simulator scores. Ophthalmology. 2011;118(9):1893-1893.e3. doi: 10.1016/j.ophtha.2011.04.019 [DOI] [PubMed] [Google Scholar]
- 14.Mehta S, Hubbard GB III. Avoiding neck strain in vitreoretinal surgery: an ergonomic approach to indirect ophthalmoscopy and laser photocoagulation. Retina. 2013;33(2):439-441. doi: 10.1097/IAE.0b013e318276cbca [DOI] [PubMed] [Google Scholar]
- 15.Humayun MU, Rader RS, Pieramici DJ, Awh CC, de Juan E Jr. Quantitative measurement of the effects of caffeine and propranolol on surgeon hand tremor. Arch Ophthalmol. 1997;115(3):371-374. doi: 10.1001/archopht.1997.01100150373010 [DOI] [PubMed] [Google Scholar]
- 16.Ayometzi CC, Lopez AG, Sosa AB, Castillejos AR. Quantitative evaluation of the effect of oral propranolol and sublingual timolol on hand tremor and its effect on surgical performance: using the EYESi surgical simulator. Invest Ophthalmol Vis Sci. 2012;53(14):6632. [Google Scholar]
- 17.Urso-Baiarda F, Shurey S, Grobbelaar AO. Effect of caffeine on microsurgical technical performance. Microsurgery. 2007;27(2):84-87. doi: 10.1002/micr.20311 [DOI] [PubMed] [Google Scholar]
- 18.World Medical Association World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191-2194. doi: 10.1001/jama.2013.281053 [DOI] [PubMed] [Google Scholar]
- 19.Mahr MA, Hodge DO. Construct validity of anterior segment anti-tremor and forceps surgical simulator training modules: attending versus resident surgeon performance. J Cataract Refract Surg. 2008;34(6):980-985. doi: 10.1016/j.jcrs.2008.02.015 [DOI] [PubMed] [Google Scholar]
- 20.Saleh GM, Theodoraki K, Gillan S, et al. . The development of a virtual reality training programme for ophthalmology: repeatability and reproducibility (part of the International Forum for Ophthalmic Simulation Studies). Eye (Lond). 2013;27(11):1269-1274. doi: 10.1038/eye.2013.166 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Webster R, Sassani J, Shenk R, et al. . Simulating the continuous curvilinear capsulorhexis procedure during cataract surgery on the EYESI system. Stud Health Technol Inform. 2005;111:592-595. [PubMed] [Google Scholar]
- 22.Le TDB, Adatia FA, Lam W-C. Virtual reality ophthalmic surgical simulation as a feasible training and assessment tool: results of a multicentre study. Can J Ophthalmol. 2011;46(1):56-60. doi: 10.3129/i10-051 [DOI] [PubMed] [Google Scholar]
- 23.Solverson DJ, Mazzoli RA, Raymond WR, et al. . Virtual reality simulation in acquiring and differentiating basic ophthalmic microsurgical skills. Simul Healthc. 2009;4(2):98-103. doi: 10.1097/SIH.0b013e318195419e [DOI] [PubMed] [Google Scholar]
- 24.Jacobson BH, Winter-Roberts K, Gemmell HA. Influence of caffeine on selected manual manipulation skills. Percept Mot Skills. 1991;72(3, pt 2):1175-1181. doi: 10.2466/pms.1991.72.3c.1175 [DOI] [PubMed] [Google Scholar]
- 25.Mort JR, Kruse HR. Timing of blood pressure measurement related to caffeine consumption. Ann Pharmacother. 2008;42(1):105-110. doi: 10.1345/aph.1K337 [DOI] [PubMed] [Google Scholar]
- 26.Mansur AP, Avakian SD, Paula RS, Donzella H, Santos SR, Ramires JA. Pharmacokinetics and pharmacodynamics of propranolol in hypertensive patients after sublingual administration: systemic availability. Braz J Med Biol Res. 1998;31(5):691-696. doi: 10.1590/S0100-879X1998000500014 [DOI] [PubMed] [Google Scholar]
- 27.Juliano LM, Griffiths RR. A critical review of caffeine withdrawal: empirical validation of symptoms and signs, incidence, severity, and associated features. Psychopharmacology (Berl). 2004;176(1):1-29. doi: 10.1007/s00213-004-2000-x [DOI] [PubMed] [Google Scholar]
- 28.Arnold RW, Springer DT, Engel WK, Helveston EM. The effect of wrist rest, caffeine, and oral timolol on the hand steadiness of ophthalmologists. Ann Ophthalmol. 1993;25(7):250-253. [PubMed] [Google Scholar]
- 29.Caprioli G, Cortese M, Maggi F, et al. . Quantification of caffeine, trigonelline and nicotinic acid in espresso coffee: the influence of espresso machines and coffee cultivars. Int J Food Sci Nutr. 2014;65(4):465-469. doi: 10.3109/09637486.2013.873890 [DOI] [PubMed] [Google Scholar]
- 30.Lieberman HR. The effects of ginseng, ephedrine, and caffeine on cognitive performance, mood and energy. Nutr Rev. 2001;59(4):91-102. doi: 10.1111/j.1753-4887.2001.tb06995.x [DOI] [PubMed] [Google Scholar]
- 31.Glicksman JT, Curhan SG, Curhan GC. A prospective study of caffeine intake and risk of incident tinnitus. Am J Med. 2014;127(8):739-743. doi: 10.1016/j.amjmed.2014.02.033 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Mürbe D, Hüttenbrink K-B, Zahnert T, et al. . Tremor in otosurgery: influence of physical strain on hand steadiness. Otol Neurotol. 2001;22(5):672-677. doi: 10.1097/00129492-200109000-00019 [DOI] [PubMed] [Google Scholar]
- 33.Haubenberger D, Hallett M. Essential tremor. N Engl J Med. 2018;378(19):1802-1810. doi: 10.1056/NEJMcp1707928 [DOI] [PubMed] [Google Scholar]
- 34.Wong GWK, Wright JM. Blood pressure lowering efficacy of nonselective β-blockers for primary hypertension. Cochrane Database Syst Rev. 2014;(2):CD007452. doi: 10.1002/14651858.CD007452.pub2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Hanu-Cernat LM, Rehman K-u, Sittampalam G, Whear NM. Propranolol—an aid to microvascular surgery. Br J Oral Maxillofac Surg. 2008;46(2):171-172. doi: 10.1016/j.bjoms.2007.07.210 [DOI] [PubMed] [Google Scholar]
- 36.Schadt CR, Duffis EI, Charles PD. Pharmacological treatment of disabling tremor. Expert Opin Pharmacother. 2005;6(3):419-428. doi: 10.1517/14656566.6.3.419 [DOI] [PubMed] [Google Scholar]
- 37.James IM, Griffith DN, Pearson RM, Newbury P. Effect of oxprenolol on stage-fright in musicians. Lancet. 1977;2(8045):952-954. doi: 10.1016/S0140-6736(77)90890-X [DOI] [PubMed] [Google Scholar]
- 38.Prichard BN. Risk-benefits of antihypertensive drugs–β-blockers. Clin Exp Pharmacol Physiol. 1988;15(3):203-213. doi: 10.1111/j.1440-1681.1988.tb01063.x [DOI] [PubMed] [Google Scholar]
- 39.Foster GE, Makin C, Evans DF, Hardcastle JD. Dose β-blockade affect surgical performance? a double blind trial of oxprenolol. Br J Surg. 1980;67(9):609-612. doi: 10.1002/bjs.1800670902 [DOI] [PubMed] [Google Scholar]
- 40.Lubahn JD, Dickson BG, Cooney TE. Effect of timolol vs a postural orthotic on hand tremor during microsurgery. Microsurgery. 2002;22(6):273-276. doi: 10.1002/micr.10049 [DOI] [PubMed] [Google Scholar]
- 41.Elman MJ, Sugar J, Fiscella R, et al. . The effect of propranolol versus placebo on resident surgical performance. Trans Am Ophthalmol Soc. 1998;96:283-291. [PMC free article] [PubMed] [Google Scholar]
- 42.Jacobson BH, Thurman-Lacey SR. Effect of caffeine on motor performance by caffeine-naive and -familiar subjects. Percept Mot Skills. 1992;74(1):151-157. doi: 10.2466/pms.1992.74.1.151 [DOI] [PubMed] [Google Scholar]
- 43.Quintana LM. How to be a neurosurgeon with good hands. World Neurosurg. 2016;89:686-688. doi: 10.1016/j.wneu.2015.11.005 [DOI] [PubMed] [Google Scholar]
- 44.Lee R, Raison N, Lau WY, et al. . A systematic review of simulation-based training tools for technical and non-technical skills in ophthalmology. Eye (Lond). Published online March 13, 2020. doi: 10.1038/s41433-020-0832-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eTable 1. Median Differences Between Days 1 and 2 With Corresponding P-value for the Eyesi Surgical-Generated Score
eTable 2. Median Differences Between Days 1 and 2 With the Corresponding P-value for the Eyesi Tremor-Specific Task Score
eTable 3. Median Difference Between Days 1 and 2 With the Corresponding P-value for the Intraocular Trajectory (Odometer)
eTable 4. Median Difference Between Days 1 and 2 With the Corresponding P-value for the Total Time for Task Completion