

Abstract
Introduction
Testicular epidermal cysts in Klinefelter syndrome are very rare. We report a case of Klinefelter syndrome associated with a testicular epidermal cyst. To our knowledge, this is the first report showing successful spermatozoa retrieval from the affected testis.
Case presentation
A 25‐year‐old married man was referred to our hospital with right scrotal induration, which was in lower pole of the right testis. Testicular cancer tumor markers were normal; endocrinological findings indicated hypergonadotropic hypogonadism. Semen analyses revealed azoospermia. Preoperative chromosome test result: 47, XXY karyotype; ultrasonography report: 1.9‐cm internal heterogeneous echoic mass in the right testis (malignancy not discarded). Because the patient hoped for children, he underwent high orchiectomy with ipsilateral testicular sperm extraction (200 spermatozoa from normal testicular tissue) for future fertilization procedures. Tumor pathology was an epidermal cyst.
Conclusion
While performing orchiectomy for testicular tumors, sperm retrieval should be attempted from normal tissues in patients planning for children.
Keywords: epidermal cyst, epidermoid cyst, Klinefelter syndrome, testicular tumor
Abbreviation & Acronym
- TESE
testicular sperm extraction
Keynote message.
Testicular epidermal cysts in Klinefelter syndrome are very rare. If malignancy was not ruled out preoperatively, high orchiectomy should be conducted. When the patient hopes for children, simultaneous testicular sperm extraction from the normal testicular tissue on the ipsilateral side should be attempted.
Introduction
Klinefelter syndrome is the most common chromosomal disorder causing male infertility occurring in approximately one out of 500 men.1 Most cases present a non‐mosaic 47, XXY karyotype.2 Testicular epidermal cysts are rare tumors accounting for approximately 1% of all testicular tumors.3 We describe a case of Klinefelter syndrome and testicular epidermal cyst. To our knowledge, this is the seventh English literature report and the first one to show successful retrieval of spermatozoa from the affected testis.
Case presentation
A 25‐year‐old married Japanese man (height 188 cm, weight 76.1 kg, body mass index 21.5) was referred to our hospital with a painless, right scrotal induration in his right testis discovered 1 month previously with no other subjective symptoms or notable histories.
On physical examination, the pubic hair and penis had a normal aspect (Tanner's stage was 5 each), but the atrophic testes had volumes of 8 ml on the left side and 12 mL on the right side (with an induration in the lower pole).
Testicular cancer tumor markers were normal (human chorionic gonadotropin <0.1 mIU/mL; alpha‐fetoprotein 3.1 ng/mL; lactate dehydrogenase 132 U/L); endocrinological findings indicated hypergonadotropic hypogonadism (luteinizing hormone 21.3 mIU/mL, follicle‐stimulating hormone 58.0 mIU/mL, total testosterone 333 ng/dL). Two separate semen analyses revealed azoospermia.
Ultrasonography report showed a 1.9‐cm internal heterogeneous echoic mass with low echoic margin in the right testis. In the Doppler mode, blood flow presence inside the tumor was ambiguous, but a signal was seen at the periphery (Fig. 1).
Figure 1.

The ultrasonography showed a 1.9‐cm internal heterogeneous echoic mass with low echoic margin in the right testis (a). In the Doppler mode, the presence of blood flow inside the tumor was ambiguous, but a signal was seen at the periphery (b).
Malignancy was not ruled out; we planned to perform high orchiectomy. Because the patient hoped to have children, we decided to simultaneously perform a TESE from the normal testicular tissue.
In February 2018, the patient underwent a high orchiectomy with incision along the inguinal canal. Right spermatic cord was ligated and cut at the internal inguinal ring level. Immediately after orchiectomy, we sectioned the testis sagittally ex vivo. We observed a 1.5‐cm white tumor in the lower pole of the right testis and normal testicular tissue with atrophic seminiferous tubules in the upper half (Fig. 2). Approximately 200 motile and immotile spermatozoa were extracted and cryopreserved.
Figure 2.

A 1.5‐cm white tumor in the lower pole of the right testis (black arrow) and normal testicular tissue with atrophic seminiferous tubules in the upper half (white arrow).
Preoperative chromosomal testing results showed a 47, XXY karyotype in 20 of 20 cells.
Pathological finding of the tumor showed a cyst wall covered with keratinizing squamous epithelia (Fig. 3), without malignancy evidence, diagnosed as an epidermal cyst. The remaining testicular tissue of upper half showed atrophy of most seminiferous tubules hyalinized with Leydig cell hyperplasia. Only Sertoli cells (no germ cells) were apparent in the seminiferous tubules observed. Mean Johnsen's score count was 1.1. The patient's wife is planning to undergo oocyte retrieval and intracytoplasmic sperm injection in the future. TESE in the left testis can be scheduled if required.
Figure 3.
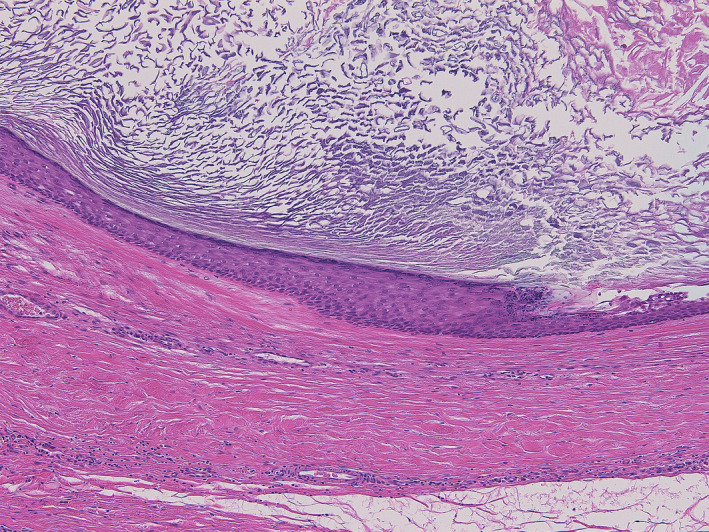
The pathological finding of the tumor showed a cyst wall covered with keratinizing squamous epithelia.
Discussion
Klinefelter syndrome is associated with an increased risk of malignant diseases including testicular germ cell tumor due to inherent endocrinological abnormalities of the hypergonadotropic hypogonadism.
Association with malignancies is often explained by testicular dysgenesis syndrome hypothesis,4 genetic defects and polymorphisms and environmental factors including endocrine disrupters lead to disturbances of Sertoli and peritubular cell functions with decreased Leydig cell function, resulting in impaired germ cells and tumors.
Testicular tumors are often discovered during male infertility screenings; azoospermia associated with Klinefelter syndrome may be found during testicular tumor screening.
Suspected malignancy led to a semi‐urgent operation; we did not wait for chromosome test result before operating. Intraoperative rapid pathological diagnosis was an option to preserve the testis in absence of malignancy; the malignancy could not be completely ruled out and azoospermia due to Klinefelter syndrome was strongly suspected. Therefore, we planned sperm retrieval from normal seminiferous tubules right after the orchiectomy. Given the possibility of finding spermatogenesis in the contralateral left testis, this procedure was not exactly “onco‐TESE”;5 it was similar and achieved spermatozoa preservation. The main purpose was to remove the testicular tumor (semi‐urgent case); we did not attempt TESE in the contralateral testis.
Testicular epidermal cysts account for approximately 1% of all testicular tumors.3 Most of them occur in men between 10 and 40 years, presenting as painless testicular induration found incidentally. Ultrasonography demonstrates an avascular, mostly lamellated heterogeneous internal echotexture, with hypoechoic and hyperchoic concentric rings (onion‐ring or target appearance). Histologically, five Price criteria can be used for the diagnosis: (i) cyst located within the testis parenchyma; (ii) cyst lumen filled with keratinized debris; (iii) cyst wall comprising fibrous tissue with complete or incomplete squamous epithelial inner lining; (iv) lacking teratomatous elements or adrenal structures (sebaceous glands or hair follicles) within the cyst wall or testicular parenchyma; and (v) no scar in the remaining testicular parenchyma.6
We found seven cases of testicular epidermal cyst associated with Klinefelter syndrome7, 8, 9, 10, 11 (Table 1). Patients’ age ranged from 6 to 38 years; the chief complaint was infertility in three cases8, 11 and scrotal induration in the other three.9, 10 In all cases, Klinefelter syndrome karyotypes were non‐mosaic (47, XXY); patients underwent orchiectomy treatments.
Table 1.
Characteristics of seven patients with Klinefelter syndrome and epidermal cyst
| Patient | Authors | Age | Chief complaint | Side | Treatment | Size | Karyotype |
|---|---|---|---|---|---|---|---|
| 1 | Goldstein et al. | 19 | Cryptorchidism | Left | Orchiectomy | 2.5 | 47, XXY |
| 2 | Sasagawa et al. | 30 | Infertility | Right | Orchiectomy | 3.0 | 47, XXY |
| 3 | Sasagawa et al. | 29 | Infertility | Right | Orchiectomy | – | 47, XXY |
| 4 | Baniel et al. | 17 | Scrotal induration | Right | Orchiectomy | 1.8 | 47, XXY |
| 5 | Kurzrock et al. | 6 | Scrotal induration | Bilateral | Orchiectomy | 1.0 | 47, XXY |
| 6 | Yoshida et al. | 38 | Infertility | Right | Orchiectomy | 4.0 | 47, XXY |
| 7 | Takeshima et al. | 25 | Scrotal induration | Right | Orchiectomy | 1.5 | 47, XXY |
Reports on epydermoid cysts have shown that one‐fifth of cases underwent cyst enucleation preserving the testis, while the rest underwent orchiectomy because malignancy including immature teratoma was not discarded,12 as in this case. This is the first study reporting successful spermatozoa retrieval with simultaneous orchiectomy in a patient with testicular epidermal cyst and Klinefelter syndrome. Sperm retrieval rate in Klinefelter syndrome is approximately 65%,13, 14 but may be lower in single testis post orchiectomy cases. Serum testosterone level decreases after TESE in such cases. Likely as in onco‐TESE cases, sperm should be retrieved from normal testicular tissue in the cancerous testis along with orchiectomy.
Conclusion
We described a case of Klinefelter syndrome with successful TESE along with orchiectomy for an ipsilateral testicular tumor. Sperm retrieval from normal testicular tissue in cancerous testes is possible for patients hoping to have children.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgment
We thank Enago (https://www.enago.jp) for their English language editing.
References
- 1. Nielsen J, Wohlert M. Sex chromosome abnormalities found among 34,910 newborn children: results from a 13‐year incidence study in Arhus, Denmark. Birth Defects Orig. Artic. Ser. 1990; 26: 209–23. [PubMed] [Google Scholar]
- 2. Lanfranco F, Kamischke A, Zitzmann M, Nieschlag E. Klinefelter's syndrome. Lancet 2004; 364: 273–83. [DOI] [PubMed] [Google Scholar]
- 3. Shah KH, Maxted WC, Chun B. Epidermoid cysts of the testis: a report of three cases and an analysis of 141 cases from the world literature. Cancer 1981; 47: 577–82. [DOI] [PubMed] [Google Scholar]
- 4. Sonne SB, Kristensen DM, Novotny GW et al Testicular dysgenesis syndrome and the origin of carcinoma in situ testis. Int. J. Androl. 2008; 31: 275–87. [DOI] [PubMed] [Google Scholar]
- 5. Schrader M, Muller M, Sofikitis N, Straub B, Krause H, Miller K. “Onco‐tese”: testicular sperm extraction in azoospermic cancer patients before chemotherapy‐new guidelines? Urology 2003; 61: 421–5. [DOI] [PubMed] [Google Scholar]
- 6. Price EB Jr. Epidermoid cysts of the testis: a clinical and pathologic analysis of 69 cases from the testicular tumor registry. J. Urol. 1969; 102: 708–13. [DOI] [PubMed] [Google Scholar]
- 7. Goldstein AM, Mendez R, Vargas A, Terry R. Epidermoid cysts of testis. Urology 1980; 15: 186–9. [DOI] [PubMed] [Google Scholar]
- 8. Sasagawa I, Nakada T, Kazama T, Sakamoto M, Satomi S, Katayama T. Epidermoid cyst of the testis in Klinefelter's syndrome. Urol. Int. 1987; 42: 398–400. [DOI] [PubMed] [Google Scholar]
- 9. Baniel J, Perez JM, Foster RS. Benign testicular tumor associated with Klinefelter's syndrome. J. Urol. 1994; 151: 157–8. [DOI] [PubMed] [Google Scholar]
- 10. Kurzrock EA, Tunuguntla HS, Busby JE, Gandour‐Edwards R, Goldman LA. Klinefelter's syndrome and precocious puberty: a harbinger for tumor. Urology 2002; 60: 514. [DOI] [PubMed] [Google Scholar]
- 11. Yoshida T, Takao T, Tsujimura A, Tomita H, Aozasa K, Okuyama A. Testicular epidermoid cyst in Klinefelter's syndrome. Int. J. Urol. 2006; 13: 478–80. [DOI] [PubMed] [Google Scholar]
- 12. Malek RS, Rosen JS, Farrow GM. Epidermoid cyst of the testis: a critical analysis. Br. J. Urol. 1986; 58: 55–9. [DOI] [PubMed] [Google Scholar]
- 13. Ramasamy R, Ricci JA, Palermo GD, Gosden LV, Rosenwaks Z, Schlegel PN. Successful fertility treatment for Klinefelter's syndrome. J. Urol. 2009; 182: 1108–13. [DOI] [PubMed] [Google Scholar]
- 14. Dabaja AA, Schlegel PN. Microdissection testicular sperm extraction: an update. Asian J. Androl. 2013; 15: 35–9. [DOI] [PMC free article] [PubMed] [Google Scholar]