


Abstract
Scrape cellblock (SCB) is a novel technique to suggest possible primary site in fine-needle aspiration cytology (FNAC) smears from the liver, lung, and lymph nodes which are the common sites of metastasis of many primary tumors. Immunocytochemistry (ICC) on SCB averts the need of more invasive diagnostic procedures and gives a conclusive diagnosis. We present a series of four cases with unknown primary site, in which ICC was done on SCB to suggest possible primary site. Three of them were liver space-occupying lesions (SOL) and one from the periportal lymph node. In all four cases, wet-fixed smear for hematoxylin and eosin stain was prepared as routine procedure. FNAC was reported as metastatic adenocarcinoma in two and metastatic spindle cell neoplasm in one liver SOL. Periportal node was reported metastatic adenocarcinoma. Two hematoxylin and eosin-stained slides from each case with higher cellularity were used to scrape off the material to prepare SCB. ICC was put which gave conclusive diagnosis in all the cases. On ICC, two cases of metastatic carcinoma in the liver were diagnosed as metastatic neuroendocrine neoplasm from Gastrointestinal Tract and metastatic adenocarcinoma from the stomach. Spindle cell neoplasm of the liver was diagnosed as gastrointestinal stromal tumor from the stomach. Pancreatic head mass in metastatic periportal node was confirmed later by radiologic examination. SCB is a useful technique to make the best use of available material where reaspiration is difficult. ICC on SCB is of maximum utility to suggest possible primary sites in metastatic cases with unknown primary or where biopsy of the lesion is not possible.
Keywords: Immunocytochemistry, Scrape cellblock, Unknown primary
INTRODUCTION
Fine-needle aspiration cytology (FNAC) is the least invasive diagnostic method that aids in the immediate assessment and improves the patient’s outcomes. Cellblock preparation allows for additional ancillary studies such as immunocytochemical staining, FISH, and other molecular studies to be performed on cytology specimens. However, many a time, because of inadequate sampling or noncooperating patients, obtaining a cellblock is not possible. Furthermore, biopsy becomes challenging in some conditions because of inaccessible site or patient’s noncompliance. In such rare instances, FNAC smears are the only cellular sample available. Scrape cellblock (SCB) is a novel technique to arrive at a precise diagnosis from the minimum sample we have. The present article reports four such cases in which immunocytochemistry (ICC) was applied to SCB and a precise diagnosis was delivered that aided in further treatment of the patient.
MATERIALS AND METHODS
SCB is prepared by scraping off the material from already stained FNAC smears. Architecture, morphologic, and cellular details are well preserved if a block is prepared meticulously in experienced hands. In our cases, FNAC slides were made from the metastatic sites. They were stained with hematoxylin and eosin stain. After routine reporting, we selected two stained FNAC smears with high cellularity. Coverslips were removed by dipping the slides in xylene for 30 min. After destaining in 1% acid alcohol for few seconds, rehydration was done in various grades of decreasing concentration of alcohol for 20 min. We used a scalpel No. 22 to scrape off the material gently in a Petri dish. For maximum retrieval of the cellular material, slides were kept at 45° angle. The scraped off material was collected in the Petri dish and was transferred cautiously to a test tube. An equal amount of 1 ml plasma and thromboplastin was added to the material in the test tube and then was centrifuged. The clot formed thereafter was carefully transferred on the filter paper which was enclosed in the cassette and was then fixed in 10% neutral buffered formalin. It was further processed as routine tissue paraffin blocks. The slides obtained thereafter were subjected to hematoxylin and eosin staining, and a panel of immunomarkers was applied on them. We received informed consent from all the patients (or their guardians) before the study was performed.
CASE REPORTS AND RESULTS
Case 1
A 55-year-male presented with pain in the abdomen. On computed tomography (CT) scan, there was a mesenteric mass on the posterior wall of the stomach along with liver space-occupying lesions (SOL). The mesenteric mass was inaccessible for the evaluation, while FNAC of the liver SOL was done and reported as metastatic spindle cell neoplasm. SCB was made from liver FNAC smears, and a panel of ICC was applied. The spindle cells were immunopositive for CD34, Dog1, and CD117 [Figure 1]. Hence, the final diagnosis of malignant gastrointestinal stromal tumor was made, and the patient was subjected to the targeted therapy.
Figure 1:
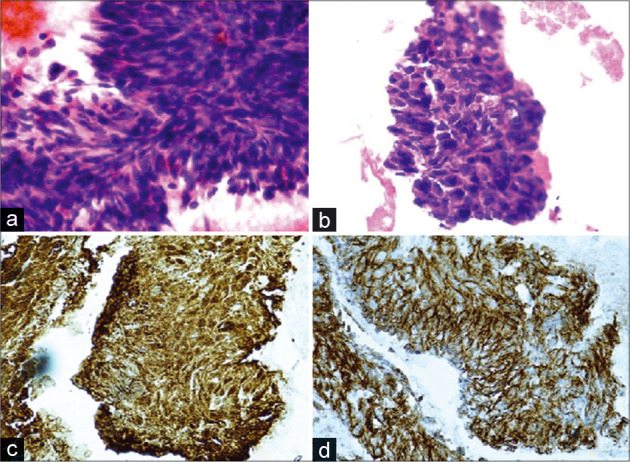
(a) Cellular material on the conventional smears, (b) scrape cellblock, (c) CD34 immunohistochemical, and (d) DOG 1 immunohistochemical (Case 1).
Case 2
A 52-year-female presented with pain in the abdomen. Radiologically, there was a liver SOL suggesting metastasis with unknown primary. FNAC from liver SOL was reported as metastatic neuroendocrine carcinoma. ICC on SCB was applied that was immunopositive for CDX2, Neuron Specific Enolase NSE, and synaptophysin [Figure 2]. Hence, the patient was further evaluated, and the final primary site was confirmed as the stomach. Surgical treatment was offered to the patient with subsequent chemothearapy.
Figure 2:
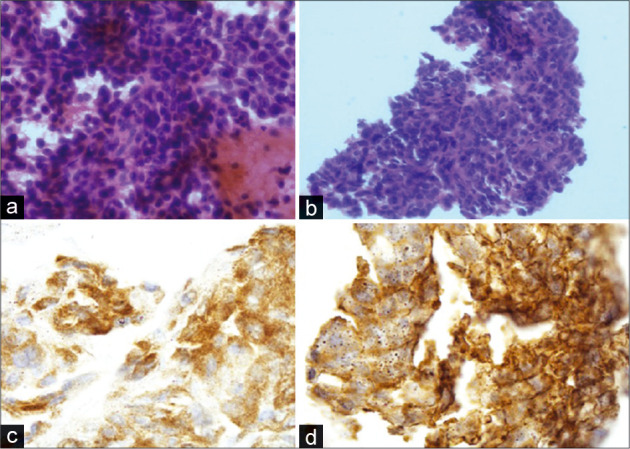
(a) Conventional smear (H&E), (b) scrape cellblock (H&E), (c) synaptophysin IHC and (d) NSE IHC (Case 2).
Case 3
A 43-year-male presented with pain in the abdomen and jaundice. On CT, there was periportal lymphadenopathy and a small mass at the head of the pancreas. FNAC from the lymph node was suggestive of metastatic neoplasm, while FNAC from the pancreatic mass was inconclusive. The patient’s general condition did not allow for repeat FNAC or other invasive techniques. CK20 and CA19.9 [Figure 3] immunopositivity on SCB proved it to be of pancreatic origin. As pancreatic neoplasm has a dismal outcome, it is utmost required having prompt treatment.
Figure 3:
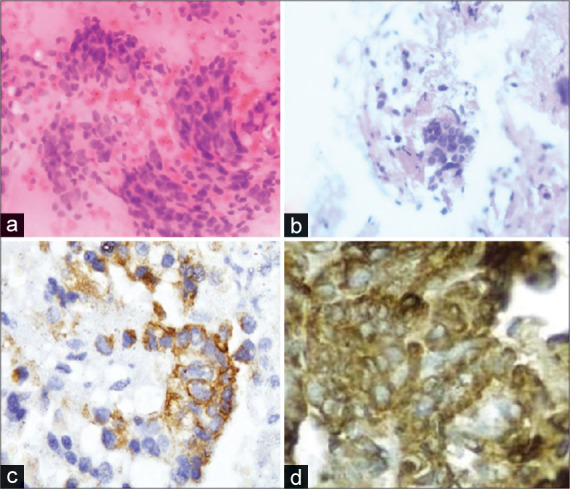
(a) Conventional smear (H&E), (b) scrape cellblock (H&E), (c) CK20 IHC and (d) CA 19.9 IHC (Case 3).
Case 4
A 50-year-male patient was admitted with pain in the abdomen. On evaluation, he was found to have multiple liver lesions suggesting liver metastasis of unknown primary. Routine FNAC was reported as metastatic adenocarcinoma.
CDX2 and CK20 immunopositivity on SCB suggested it to be of gastric origin [Figure 4].
Figure 4:
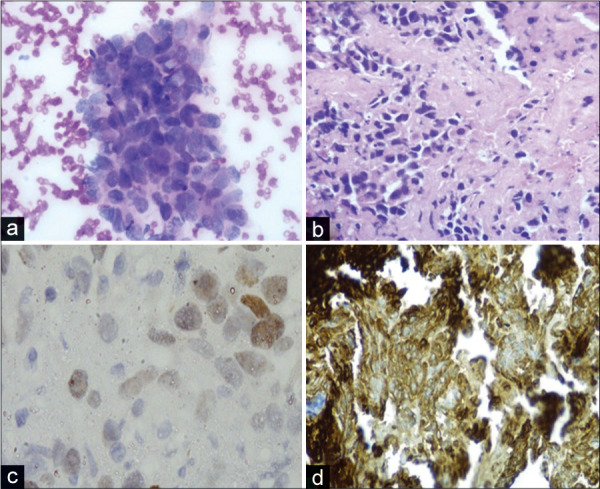
(a) Conventional smear (H&E), (b) scrape cellblock (H&E), (c) CDX2 IHC and (d) CK20 IHC (Case 4).
DISCUSSION
Cellblock has now been widely accepted as an adjuvant technique to the conventional smears, especially in fluid cytology, as it provides high cellularity, better architectural patterns, morphological details, and additional yield for malignant cells.[1] FNAC has diagnostic limitations and requires immunomarkers to suggest possible primary site, especially in poorly/undifferentiated neoplasm. Kulkarni et al. in 2000 suggested the use of SCB technique when there is an inconclusive diagnosis on FNAC due to poor spreading and presence of thick tissue fragments despite aspiration of adequate material and when repeat aspiration is not possible.[2] Zhu et al. at Harborview Medical Center, Seattle, Washington, used a scraped slide technique that transferred smear material on Papanicolaou-stained slides into paraffin-embedded cellblocks.[3] They applied ICC on paraffin block. This technique has been utilized by many cytopathologists and has resulted in increased diagnostic yield. We found this technique to have its maximum utility in the cases presented with metastasis of unknown primary. Published literature describes an approximate of 3%–5% of malignancies that present with metastasis of unknown origin.[4] In such cases, the origin of the tumor is hidden in spite of extensive radiological and pathological assessment. Hence, further ancillary techniques are required to arrive at a conclusion. ICC is an essential adjunct to cytomorphology and is easily available at various laboratories. This particular approach, that is, ICC on SCB, helps in increasing the diagnostic accuracy with the minimum cytology material available with us. Bhatia et al.[5] compared cytomorphology preservation and immunohistochemistry results between conventional cellblocks (CCB) and cytoscrape cell blocks (SCB). The study demonstrated a good morphological, architechtural, and nuclear preservation in all SCB samples. Regarding immunostaining quality, the results have shown better and clear intensity of staining with little background in cellblock cases.[6] In our study, the pattern of ICC staining was in good corroboration with the control slides.
Further, cellblock preparation by the Thromboplastin Plasma (TP-CB) method is a well-established method of obtaining a cellblock. It has a number of advantages over other techniques of cellblock preparation. Being simple, cost-effective, and reproducible, this method can be easily adopted by various laboratories. Moreover, other cellblock techniques, such as agarose gel embedding technique, are more cumbersome to perform both technically and financially. TP-CB provides a high cellularity; thus, more amount of cellular material can be harvested from the scrapped off material.[7] Furthermore, the cellular elements obtained are well preserved and concentrated in a small area, thus making its evaluation more convenient.[8]
SCB has achieved advantages over FNAC and conventional cellblock preparation. It eliminates the diagnostic limitations of FNAC, as it averts the need of the invasive diagnostic procedure. SCB is best useful when FNAC is inconclusive due to the poor spreading and tissue fragments when reaspiration is not possible and in special circumstances when a biopsy is difficult or not possible.
CONCLUSION
While the world is advancing over lesser invasive and more diagnostic methods, SCB is a novel technique to make the best use of available material when reaspiration or biopsy is difficult or not possible. SCB obviates diagnostic limitations of FNAC and unpredictable cell content problem of conventional cellblock. However, it is important to understand the critical limitations of this method because of potential compromisation of immunoreactivity pattern as a result of exposure to multiple non-formalin fixatives and reagents during processing for cell-block making.[9,10]. ICC on SCB prevents the need to repeat the procedure in rare selected cases especially in inaccessible lesions.
Footnotes
How to cite this article: Mathur A, Sharma A, Sharma M, Maurya A, Yadav A, Sethi N. Immunocytochemistry on scrape cellblock: An aid in the diagnosis of metastatic neoplasm with unknown primary: A series of four cases. CytoJournal 2020;17:9.
COMPETING INTERESTS STATEMENT BY ALL AUTHORS
The authors have declared that no competing interests exist.
AUTHORSHIP STATEMENT BY ALL AUTHORS
The study was designed, directed and supervised by Dr Anjali Sharma. Resource management and data collection was done by Dr Arpita Mathur (Corresponding author). Dr Neha Sethi helped in formatting the manuscript, Mr Mudit Sharma provided the technical assistance. Dr Anamika Yadav and Dr Abhishek Maurya also contributed in manuscript prepararion and data collection.
ETHICS STATEMENT BY ALL AUTHORS
All procedures performed in the study were in accordance with the ethical standards of the institution. Informed consent was taken from all the patients involved in the study.
LIST OF ABBREVIATIONS (In alphabetic order)
ICC – Immunocytochemistry,
IHC – Immunohistochemistry,
SCB – Scrape cell block,
TP-CB – Thromboplastin Plasma Cell-Block technique.
EDITORIAL/PEER-REVIEW STATEMENT
To ensure the integrity and highest quality of CytoJournal publications, the review process of this manuscript was conducted under a double-blind model (the authors are blinded for reviewers and vice versa) through automatic online system.
References
- 1.Udasimath, Shivakumar, Arakeri, Surekha, Karigoudar, Mahesh, Yelikar, Balasaheb The Role of the Cell Block Method in the Diagnosis of Malignant Ascitic Fluid Effusions. Journal of Clinical and diagnostic Research. 2012 Sep;6(Suppl)(7):1280–1283. (2012) [Google Scholar]
- 2.Kulkarni MB, Prabhudesai NM, Desai SB, Borges AM. Scrape cell-block technique for fine needle aspiration cytology smears. Cytopathology. 2000;11:179–84. doi: 10.1046/j.1365-2303.2000.00249.x. [DOI] [PubMed] [Google Scholar]
- 3.Zhu LC, Feng Q, Grieco VS. The Use of Endoscopic Ultrasound-Guided Fine Needle Aspiration (EUS-FNA) in Cytopathology Diagnosis. 2013. [DOI]
- 4.Pavlidis N, Khaled H, Gaafar R. A mini review on cancer of unknown primary site: A clinical puzzle for the oncologists. J Adv Res. 2015;6:375–82. doi: 10.1016/j.jare.2014.11.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bhatia P, Dey P, Uppal R, Shifa R, Srinivasan R, Nijhawan R, et al. Cell blocks from scraping of cytology smear: Comparison with conventional cell block. Acta Cytol. 2008;52:329–33. doi: 10.1159/000325516. [DOI] [PubMed] [Google Scholar]
- 6.Choi YI, Jakhongir M, Choi SJ, Kim L, Park IS, Han JY, et al. High-quality cell block preparation from scraping of conventional cytology slide: A technical report on a modified cytoscrape cell block technique. Malays J Pathol. 2016;38:295–304. [PubMed] [Google Scholar]
- 7.Kulkarni MB, Desai SB, Ajit D, Chinoy RF. Utility of the thromboplastin-plasma cell-block technique for fine-needle aspiration and serous effusions. Diagn Cytopathol. 2009;37:86–90. doi: 10.1002/dc.20963. [DOI] [PubMed] [Google Scholar]
- 8.Karnauchow PN, Bonin RE. “Cell-block” technique for fine needle aspiration biopsy. J Clin Pathol. 1982;35:688. doi: 10.1136/jcp.35.6.688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Shidham VB. CellBlockistry: Chemistry and art of cell-block making a detailed review of various historical options with recent advances (Review) CytoJournal. 2019;16:12. doi: 10.4103/cytojournal.cytojournal_20_19. Available from: http://www.cytojournal.com/temp/CytoJournal16112-3882578_104705.pdf [Last accessed on 2019 Jun 28] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Shidham VB. CellBlockistry: Science of cell-block making as ancillary cytopathology component in the era of minimally invasive techniques with increasing role of molecular pathology (invited short communication) Clin Surg. 2019;4:2510. Available from: http://www.clinicsinsurgery.com/pdfs_folder/cis-v4-id2510.pdf. [Google Scholar]