

Abstract
Because health systems are conceptualized as social systems, embedded in social contexts and shaped by human agency, values are a key factor in health system change. As such, health systems software—including values, norms, ideas and relationships—is considered a foundational focus of the field of health policy and systems research (HPSR). A substantive evidence-base exploring the influence of software factors on system functioning has developed but remains fragmented, with a lack of conceptual clarity and theoretical coherence. This is especially true for work on ‘social values’ within health systems—for which there is currently no substantive review available. This study reports on a systematic mixed-methods evidence mapping review on social values within HPSR. The study reaffirms the centrality of social values within HPSR and highlights significant evidence gaps. Research on social values in low- and middle-income country contexts is exceedingly rare (and mostly produced by authors in high-income countries), particularly within the limited body of empirical studies on the subject. In addition, few HPS researchers are drawing on available social science methodologies that would enable more in-depth empirical work on social values. This combination (over-representation of high-income country perspectives and little empirical work) suggests that the field of HPSR is at risk of developing theoretical foundations that are not supported by empirical evidence nor broadly generalizable. Strategies for future work on social values in HPSR are suggested, including: countering pervasive ideas about research hierarchies that prize positivist paradigms and systems hardware-focused studies as more rigorous and relevant to policy-makers; utilizing available social science theories and methodologies; conceptual development to build common framings of key concepts to guide future research, founded on quality empirical research from diverse contexts; and using empirical evidence to inform the development of operationalizable frameworks that will support rigorous future research on social values in health systems.
Keywords: Social values, health policy and systems research, evidence map
Key Messages
A focus on health systems software, including values, norms, interests, ideas and relationships, is widely considered foundational to health policy and systems research (HPSR).
The HPSR evidence-base on social values is substantive and spans a wide variety of areas of work within the field.
Problematically, there are significant gaps in the evidence-base with respect to low-income country contexts and rigorous empirical work focusing on values.
Strengthening the evidence-base will require channelling resources into low- and middle-income countries to enable locally lead production of evidence utilizing (often resource-intensive) social science methodologies. Continued conceptual and theoretical work is needed but should be based on empirical evidence from diverse contexts.
In addition to these concrete and tangible expressions of health systems, the ‘software’—by which we mean the ideas and interests, values and norms, and affinities and power that guide actions and underpin the relationships among system actors and elements—are also critical to overall health systems performance (Sheikh et al., 2011, p. 2).
Introduction
It has long been recognized that health systems are social systems in which values constitute a key determinant of system change (Donabedian, 1972; Lewis, 1977; Roemer, 1988). In the past, the understanding that health systems change is values-driven led many to question the utility of research on the organization and delivery of health services (Lewis, 1977) (see also Mechanic, 1978). If changes in the system are dependent on changes in social values, rather than by research-informed intervention, it was argued and then, while research may offer post hoc explanations for system change, it cannot generate improvement in the same way that clinical research improves the practice of medicine (Myers, 1973; Lewis, 1977; Roemer, 1988). Over the last 25 years, however, health policy and systems research (HPSR) has emerged as a distinct field of study, contributing to health systems development and improving health outcomes by providing a deeper understanding of the social structures and institutions through which health services are delivered (Remme et al., 2010; Yao et al., 2014; AHPSR, 2019). As the field of study develops, theory, empirical evidence and research methodologies are emerging that reveal the role of values in health system change and may begin to indicate strategies for effective intervention.
The term ‘values’ is sometimes used to denote individual preferences (Shams et al., 2016); however, within HPSR, and for the purposes of this paper, ‘values’ refers to the foundational normative beliefs underlying those preferences. In this sense, values, such as equity or autonomy, are abstract, or trans-situational, collective or cultural ideas ‘about what is deemed to be good or bad by a society’ (Giacomini et al., 2004, p. 20) that act as rationales for attitudes, motives and behaviours (Shams et al., 2016).
Because they are collectively or culturally generated and held, values are relatively stable and change resistant (Spates, 1983; Giacomini et al., 2004). For the same reason, while values can be held individually and shape individual behaviour, they are also socially constructed and are often considered as characteristics of organizations and institutions, cultures, communities and societies (Rokeach and Parker, 1970; Rokeach, 1974; Hofstede, 1985; Minkov and Hofstede, 2012). Dominant values will therefore vary from country to country (Roberts et al., 2003).
A values-orientation has been foundational to the field of HPSR throughout its emergence and remains strongly evident in HPSR today (Gilson, 2012a; Sheikh et al., 2011; 2014b). Because health systems are understood in HPSR to be social systems, shaped at all levels by human agency and embedded in social and political contexts (Gilson et al., 2011b), values are recognized as an important dimension of health systems and health system change and HPS researchers understand themselves to be producing ‘contextually relevant, values-driven research knowledge [for] people centred health systems’ (Sheikh et al., 2014b, p. ii4).
In addition, the field is shaped by a ‘systems thinking’ perspective and therefore frames the health system as a complex network of ‘hardware’ elements (structures, organizations and technologies) and ‘software’ elements (people, relationships, cultures and values) and emphasizes the interactions and interrelationships between these systems elements and between systems and their social and political contexts (Atun and Menabde, 2008; De Savigny and Adam, 2009; Sheikh et al., 2011; Gilson, 2012a).
Researchers in HPSR also pay close attention to the behaviours, norms, communications and relationship between actors and actor groups—acknowledged to be shaped by personal and shared values (Gilson and McIntyre, 2008; Marchal et al., 2016)—and to issues of equity, social justice, human rights and responsiveness to the needs and preferences of communities (Gostin and Powers, 2006; London et al., 2015; Gilson et al., 2017).
Sheikh et al. (2014a) argue that influencing real-world change through HPSR necessitates understanding health systems as social and political constructs, foregrounding human agency and values and paying particular attention to context. In doing so, HPS researchers are able to understand the influence of values and generate knowledge with the potential for real-world impact. HPSR can also, therefore, contribute to promoting certain values within heath systems by ‘exploring the societal relevance and purpose of systems and interventions’ (Sheikh et al., 2011, p. 4) and ‘generating new knowledge to advance particular health systems goals’ (Pratt et al., 2017, p. 891).
As a result of this values-orientation, discussion of values pervades the HPSR literature and evidence-base. Values are highlighted in theoretical frameworks (see more below), such as the popular Health System Dynamics Framework (HSDF) (van Olmen et al., 2012a), and commonly applied in conceptual tools and heuristic devices such as the hardware/software distinction referenced above (Sheikh et al., 2011).
Values are also used to make sense of health systems change. For example, values are said to explain global trends in health system financing—as in Walt and Gilson (1994), who argue that ‘severe economic constraints and shifts towards neo-liberal values…have led to cuts in public health services…increased charges for health care, and liberalization of the health sector to promote private sector development’ (p. 353). In fact, many theories of health policy change recognize that decision-makers are not entirely ‘rational’ actors and, therefore, decision-making requires trade-offs between competing values, interests and beliefs (AHPSR, 2004; Liverani et al., 2013; Langlois et al., 2018). Values are understood to shape policy-maker and public understandings of policy problems and the range of feasible or acceptable solutions to those problems (Gilson et al., 2011b), such as in the case of the formulation of policies to control the marketing of alcoholic beverages in South Africa, where various forms of evidence were accepted by different actors depending on their values and interests (Bertscher et al., 2018).
Values are also understood to shape collaboration between individuals in the health system and across health system dimensions through the establishment of trust, legitimacy, shared norms and ways of working (Bloom et al., 2008) and therefore affect whether and how policies are implemented (Gilson and Raphaely, 2008). Similarly, health system governance and management practices are acknowledged to be shaped by values (Fattore and Tediosi, 2013).
Perhaps to delineate between values understood as individual preferences and values understood as socially constructed, much of the HPSR work on values uses the concept of ‘social values’ (Shiffman, 2007; Clark and Weale, 2012; Kieslich, 2012; Koduah et al., 2018), or related ideas such ‘dominant values’ (Kehoe and Ponting, 2003; Exworthy, 2008; Abimbola et al., 2017), or ‘political values’ (Ham and Brommels, 1994; Kruk et al., 2010; Broqvist and Garpenby, 2015). For example, Clark and Weale (2012) note that health priority setting requires a combination of technical judgements and social value judgements. Similarly, Buse et al. (2012) note that for an idea to become a feasible policy solution, it must be consistent with dominant social values and Nord et al. (1995) critique the unthinking application of economic evaluation techniques on the basis that it imposes a set of values out of sync with those held by most members of society. From a socio-historical perspective, Cady (2016, p. 10) argues that ‘the mere existence of Canada’s publicly funded health system is an indication of deeply held social values’.
In addition to being shaped by values, health systems are understood to have a social value. That is, it is argued that health systems can build social cohesion, capture a sense of national identity, reinforce progressive conceptualizations of social justice, shape citizens’ understandings of their rights and entitlements or strengthen the relationships between citizens and the state (Gilson, 2003; Giacomini et al., 2004; Freedman et al., 2005; Kruk et al., 2010). For example, Gilson (2003, p. 1461) states, ‘rather than simply being shaped by the changing basis of societal values, a trusting and trusted health system can contribute to building wider social value and social order’.
However, despite these indicators of the ways in which social values shape health systems and are therefore central to understanding health systems change, the HPSR evidence-base on the role of social values in health systems is relatively weak. While there is much ‘values-talk’ in HPSR, there seems to be little research focusing on values in health systems. What evidence there is appears to be fragmented, with varied definitions and applications. For example, in publications by leading institutions such as the World Health Organization (WHO), the Alliance for Health Policy and Systems Research (AHPSR) and Health Systems Global (HSG), values are mentioned frequently but obliquely. The WHO’s (2015) report on people-centred health services mentions values only as a caveat to its five recommended strategic directions, noting that strategies will need to account for local values.
Some researchers have suggested that rigorous empirical or conceptual HPSR work focusing on values remains very limited. Littlejohns et al. (2012c) notes that the impact of social values on health policy decision-making remains unclear and is rarely recognized in a formal way. Similarly, Giacomini et al. (2004, p. 15) argue that ‘despite widespread recognition of the importance of values, decision makers and stakeholders in health policy appear to disagree fundamentally over what values essentially are’. Prior to the publication of Shams et al.’s (2016) concept mapping of values in health policy, no study had sought to systematically unpack definitions, conceptualizations and applications of values in any area of work within HPSR. While Shams et al. (2016) made a valuable contribution, it was restricted to one aspect of the health system, so did not remedy the fragmentation of the evidence-base. Furthermore, while the review systematically analysed the concept of values, data collection was not systematic and findings were restricted to the conceptualization of values. To date, no study has systematically mapped the evidence on social values in HPSR. This is striking given that HPSR is a values-driven field (HSG, 2018) and that, as HPSR is an emergent, interdisciplinary field, there is an acknowledged need to actively and consciously develop a common language through deliberation and consensus building around key concepts, theories and definitions (Sheikh et al., 2011; Hoffman et al., 2012). We therefore undertook a systematic mixed-methods evidence mapping the review of literature on social values within HPSR. The aim of this study was to describe the nature and distribution of HPSR theory and evidence on the topic, to identify gaps in the evidence-base and to suggest strategies to guide future research.
Methods
Evidence mapping involves systematic synthesis, organization and interpretation of a broad range of literature or evidence, using rigorous and replicable data collection strategies (Hetrick et al., 2010; Bonell et al., 2011; Miake-Lye et al., 2016; Danan et al., 2017). The approach is commonly used to describe the extent and distribution of literature on a topic, identify gaps and indicate areas for future research but can also be used to describe the range of study designs and methodological approaches used, and the topical areas covered, giving readers a base-line understanding of a body of evidence (Bragge et al., 2011; Miake-Lye et al., 2016). As such, evidence mapping reviews do not seek to synthesize findings or establish the strength of evidence and, therefore, do not require the presentation of the results of included studies (Adam et al., 2018). ‘Mixed-methods review’ is a label given both to research that combines a review with another data collection approach, such as interviews (Grant and Booth, 2009) and to studies using review methodologies to collect both qualitative and quantitative evidence (Pace et al., 2012; Heyvaert et al., 2013). Here, we use the latter approach—employing systematic, transparent and reproducible data collection strategies (Heyvaert et al., 2013; Tricco et al., 2015) to explore and describe a range of qualitative and quantitative research on a complex subject (Pace et al., 2012).
As ‘social values’ is an abstract concept, used alternately with, and closely associated with related concepts, data collection and analysis were conducted iteratively, building the body of included literature in accordance with the researchers’ developing understanding of key ideas and perspectives (see Boell and Cecez-Kecmanovic, 2014; Greenhalgh and Shaw, 2017). Searches were conducted systematically, with records kept of all searches. In keeping with the aim of the study, the review was limited to published peer-reviewed content, including internally reviewed reports from key institutions. To be eligible for inclusion, a paper needed to include ‘social values’ or a related term.
The search was conducted in five phases. Using an iterative multi-pronged data collection strategy is common for evidence mapping studies (Hetrick et al., 2010; Randall and James, 2012; Bonell et al., 2013; Adam et al., 2018) and has been used previously in review studies of HPSR literature (MacQuilkan, 2016). In all five phases, searches were restricted to items in English, published within the last 20 years (roughly coinciding with the recognition of HPSR as a distinct field; Bennett et al., 2018), although in Phases 3–5, this time limit was not strictly applied. The searches did not set geographic limits, although HPSR generally has a field-based focus on low- and middle-income countries (LMICs).
The first phase of the search strategy consisted of a scoping review for work referring to ‘social values’ in health policy processes and health systems. During this scoping phase, Google and Google Scholar were used, as well as informal consultation with field experts in public health and health policy and systems at the University of Cape Town, the University of the Western Cape, and the Institute of Tropical Medicine in Antwerp, to identify relevant materials.
In the second phase, a systematic search strategy was developed for use in the PubMed, in consultation with a subject librarian, on the basis of the scoping review. Two search strings were developed, the first comprising ‘social values’ and variations thereof. The second string was designed to limit results to material taking a health systems perspective and included field terms such as ‘HPSR’ and topic terms such as ‘health system’, ‘policy’, and ‘planning’ (restricted to title or abstract)1 (see Table 1 for the full database search strategy). Due to the large number of results identified through the search, the ‘most relevant’ function was used to organize the results and the title and abstracts of the first 600 results were scanned, after which search results became less relevant. The reference and full text of ‘possibly relevant’ material were downloaded to EndNote.
Table 1.
Search strategy
| String 1: HPSR | MeSH terms | Health Policy OR Public Health Systems Research OR Health Planning | In: title/abstract |
| Free text | health system OR healthcare system OR health care system OR health systems OR healthcare systems OR health care systems OR health policy OR healthcare policy OR health care policy OR health policies OR healthcare policies OR health care policies | ||
| AND | |||
| String 2: social values | Free text | Social values OR community norms OR cultural beliefs OR cultural norms OR cultural values OR dominant values OR national character OR national culture OR national identity OR political values OR public values OR shared values OR social beliefs OR societal norms OR societal values OR society norms OR society values OR value orientations | In: text word |
The third phase consisted of a systematic search of the published outputs of 23 prominent HPSR authors.2 Authors were identified through a Scopus-based meta-analysis of the most commonly recurring authors in a search for ‘HPSR OR health policy and systems research’, as well as the formative scoping review, field expert consultation and database search. Most relevant publications for each author were then found through Google Scholar, through title and abstract screening.
In the fourth phase, a targeted search of key HPSR journal content was conducted (drawing from a selection of 11 journals identified by field experts). Each journal was searched using the ‘social values’ search string, and the title and abstract screening was conducted.
Finally, we searched the publications lists of key HPS institutions—including the AHPSR, WHO, HSG and the Collaboration for Health Policy and Systems Analysis in Africa (CHESAI) as identified by the field experts—by searching within each institutional database for the phrases in the ‘social values’ search string.
Materials from all five phases were gathered into an Endnote database for full-text review. After the removal of duplicates, full-texts were screened to ensure the paper fell within the bounds of HPSR. Although the boundaries of the HPSR field are notoriously ‘fuzzy’ (Gilson, 2012a; Hoffman et al., 2012), other studies have successfully reviewed concepts and topics within HPSR by ‘bounding’ their reviews (Pratt et al., 2017; De Allegri et al., 2018). This necessitates a certain level of subjectivity in selection of articles for inclusion. In this study, the following criteria served as guiding principles:3 addresses system-level issues (exclude purely programmatic or disease-focus, unless as a ‘tracer’ for systemic issues); utilizes a prominent HPSR framework; one or more of the papers’ authors list an institute or department focusing specifically on policy and systems as a primary affiliation; and published in a policy or systems-relevant journal (so already screened through editorial and peer review). For borderline cases, two additional criteria were considered: is the other work of any of the authors largely HPSR-focused?4 and does the reference list include a number of key HPSR texts? As a general rule, a stated focus on health systems (or issues such as policy, planning or health services) was not considered sufficient for the item to be categorized as HPSR—unless it also met one other criteria.
Information from each included paper was extracted into a data extraction sheet, including: author names, publication date, publication source (e.g. journal), country of first author affiliation, topic, whether values was a main topic, disciplinary foundation and the country of focus of the research. Data were also extracted on the suggested, demonstrated or assumed relationship between social values and the health system (synthesized into a simple relationship, but with key quotes also captured to retain the nuance of the author(s)’s phrasing).
Results
Full-text screening was conducted on 430 items, with 208 identified for inclusion and coding (Figure 1). The full data extraction sheet is provided as Supplementary material. A full list of reasons for exclusion is presented in Table 2. Of the 222 excluded items, 90 were categorized as ‘not HPSR’. Almost half of the papers excluded on this basis consider social values in relation to health care or health system reforms, indicating that moments of change are liable to spur values-based reflection among various health system stakeholders and observers. Taken as a whole, this body of works reaffirms the importance of values across a wide range of health, health care and health system issues.
Figure 1.

Flow diagram of study selection procedure and results
Table 2.
Exclusions
| Reason for exclusion | Number of papers |
|---|---|
| Not HPSR | 90 |
| Values not national/social | 41 |
| Insufficient information on values | 32 |
| Not national system focus (organizational/global) | 27 |
| Disciplinary or focused on research practice | 21 |
| No access to full text | 7 |
| Religion or theology | 4 |
The publication year of included papers spans 1994–2018, which coincides roughly with the formalization of HPSR as a field, as does the steady increase in distribution of papers over time. Figure 2 presents the number of included papers per year, shown against a rough estimation of the growth in HPSR publications in general. The comparator graph—‘social values’ (top)—is based on a search for ‘health policy and systems’ and ‘HPSR’ and variations, conducted in Scopus. The similarity across the two trend-lines underscores the centrality of a values-orientation to the field of HPSR.
Figure 2.

Number of papers per year
The terms used to denote social or population values are seen in Table 3, along with the number of papers using those terms. Attempts to offer a definition of ‘social values’ were exceedingly rare. Clark and Weale (2012, p. 294) define social values as ‘the moral or ethical values of a particular society’, while Stafinski et al. (2011, p. 208) conceptualize them as the ‘distributive preferences of the public’. Conversely, Giacomini et al. (2004) offer a broader understanding that includes ‘ideologies, interests, principles [and] goals’ (p. 16). The social values cited in the papers are seen in Box 1. The most commonly cited social values were equity and equality, solidarity, justice and fairness.
Table 3.
Terms used to denote ‘social values’
| Social/societal/society's values/value systems | 86 |
| Shared/community/communal/collective values/norms | 26 |
| Cultural/socio-cultural values/norms/beliefs | 25 |
| Social/societal norms | 18 |
| Public(‘s) values/attitudes/discourses | 18 |
| Political values/norms/culture/ideology | 15 |
| Dominant/predominant/popular/prevailing/common values | 14 |
| Ideology/worldview | 13 |
| Country/national/country X's values | 11 |
| Citizen/democratic values | 4 |
| Local values | 3 |
| National culture/identity | 3 |
| Values-orientation | 2 |
Box 1 Commonly cited values
Equity and equality, solidarity, justice and fairness, access, autonomy, accountability, choice, transparency, participation and representation, efficiency, universality and non-discrimination, respect, quality, effectiveness, trust and dignity
The relationship between health systems and social values
Across the included papers, connections are drawn between health systems and social values in various ways. We synthesized statements about the relationship between health systems and social values in terms of health system processes or functions and health system elements or dimensions. Relational statements were analysed in the same way whether presented as a finding of empirical research, or suggested or implied in an introduction or background section. The statements were synthesized into their constituent parts—usually a connection between a dimension or element of the health systems, and a particular function or process of the health system. For example, Mou (2013, p. 278) states that ‘collective values … are important in the politics around the public–private mix of health expenditure’ and Roberts et al. (2003) argue that, by connecting to symbols that relate to broad social values, health system actors can develop political strategies that gain them additional leverage in policy debates. In other words, these authors suggest a relationship between social values and health expenditure patterns, or between social values and policy development, rather than between social values and health systems as such.
Table 4 shows the number of (included) papers suggesting a relationship between a particular health system dimension or element and the particular health system function or procedure. As this is a synthesis analysis, dimensions and functions named in very few relational statements are not presented. The most commonly suggested relationships are those between social values and the behaviour or decision-making of healthcare workers and managers. For example, Watt et al. (2017, p. iv15) show how ‘implementation can be constrained by … social norms shaping the interaction between providers and populations’, while Berlan and Shiffman (2012) demonstrate that attempts to change implementer behaviour through information provision may have little impact because those behaviours are deeply ingrained through social norms. Many papers also draw out the relationships between social values and policy-maker decision processes—such as Shankardass et al.’s (2018, p. 5) suggestion that values ‘constitute the normative lens through which political elites … interpret and act upon social and political issues’ and Gilson et al.’s (2011a, p. 6) claim that the ‘outcomes pursued by public sector leaders are those judged as valuable by the public at large as well as by political stakeholders and policy makers’. A number of authors also identify a relationship between social values and the structure or framing of policies, such as Giacomini et al.’s (2004) demonstration that values can be used strategically in policy documents to declare values or demonstrate the prioritization of one value over a competing value.
Table 4.
Most commonly identified relationships
| Health system dimension or element |
|||||||
|---|---|---|---|---|---|---|---|
| Health system | HCWs and managers | Policy | Policy-maker/ elite | Intervention/ programme/service | User | Citizen | |
| Health system process or function | |||||||
| Priority/agenda-setting | 29 | 6 | |||||
| Behaviour/decision-making | 36 | 35 | 14 | 3 | |||
| Success/effectiveness/implementation/function | 4 | 8 | 8 | ||||
| Change/reform | 23 | 5 | |||||
| Finance/funding/resource allocation | 23 | ||||||
| Management/governance | 2 | 1 | |||||
| Content/structure/framing | 20 | 30 | 9 | 2 | |||
| Perception/expectation | 2 | 1 | 8 | 4 | 10 | ||
| Goals/principles | 12 | 2 | 1 | 1 | 3 | ||
Note: The darker grey indicates relationships identified more than 10 times, the lighter grey indicates relationships identified between five and 10 times.
Many authors identify an effect of social values on the health system as a whole through processes such as priority-setting, reforms and restructurings, financing and goal-setting. For example, Agyepong et al. (2017, p. 59) state that values ‘shape the outcomes of health systems’ and Sabik and Lie (2008) demonstrate that, in Norway, procedures have been put in place to establish shared values to inform prioritization decisions and ensure that they are in line with society’s values and goals. Similarly, Kieslich (2012) points out that values rooted in political traditions influence the organizational form of health systems and Grundy (2015) argues that social values influence the direction of health system change and determine pathways for change towards universal health coverage. Claims like these underlie the common perception that values shape health systems.
The number of papers suggesting a relationship between social values and citizens’ expectations and perceptions in relation to health systems—such as Mirzoev and Kane (2017, p. 2) stating that public expectations are shaped by ‘socio-political societal views on health as a human right’—is noteworthy and may indicate that social values constitute a mechanism by which health systems can be responsive to citizens. In the same vein, Schlesinger (2002, p. 891) observes that as market-based ideologies become dominant in health policy, ‘these notions of fairness … become the primary way of judging equity’—suggesting a values-based relationship between citizens and the framing of health policies such that the social construction of policies drives changes in the public’s understand of what is fair and just in relation to health care. Similarly, Gilson (2003, p. 1458) states that social institutions, such as the health system, can ‘promote’ social values, stating, ‘social and political institutions embodying these norms [truthfulness, solidarity, fairness] promote affective trust in societies by committing and enforcing upon all those involved in them a specific set of values’. However, like many of the relationships presented in the table, these claims tend to be only briefly suggested or implied in the included papers and not fully justified or explained. This analysis suggests that while the influence of values is acknowledged across a diverse array of system dimensions and functions, mechanisms of influence are rarely explicitly stated or fully explored.
Topical foci and frameworks
We applied thematic analysis to identify the topics or areas of work in which reference to social values is most commonly made. The analysis resulted in the identification of 11 recurring topics across the included studies. The most common topic was ‘priority-setting’ (n = 38/208), which is indicative of widespread acknowledgement in HPSR that health systems are significantly shaped by resource-distribution decisions, which in turn are underpinned by social values. As Bennett and Chanfreau (2005, p. 541) note, ‘rationing mechanisms reflect several underlying ethical theories [that] should reflect societal values’. Other significant categories include health policy development, implementation or evaluation, health system analysis (including evaluation) and health system reform—collectively making up almost half of all papers. Table 5 shows the number of papers identified within each topic category.
Table 5.
Number of papers within each topic category
| Priority-setting (including cost-effectiveness analysis, health technology assessment, economic evaluation, rationing, resource allocation) | 43 |
| Health system analysis (including structure, evaluation, resilience, responsiveness, trust, complexity and context) | 36 |
| Policy analysis (including agenda-setting, process, development, evaluation) | 33 |
| Health system reform | 26 |
| Service delivery (including patient-provider relations, implementation, trust, provider behaviour, training and motivation) | 16 |
| Service delivery (including planning, management, accountability) | 14 |
| Public participation (including values and preferences, mechanisms) | 9 |
| Governance and leadership | 9 |
| Health finance (including contracting, funding mechanisms) | 9 |
| Knowledge translation (including research to policy) | 8 |
| Equity (including access to services) | 5 |
The frameworks and conceptual tools available to researchers can influence the type of research conducted and the extent to which that research incorporates particular ideas and concepts. We mapped the frameworks used in the included papers. The most commonly used framework is Sheikh et al.’s illustration of different perspectives of the subjects of inquiry within HPSR. This framework offers a conceptualization of policy decisions as an outcome of an interplay between health system hardware elements (such as human resources, finance) and health system software elements (including ideas, power and values and norms), within social and political contexts (Sheikh et al., 2011). The framework is cited in nine included papers,5 including, for example Fattore and Tediosi’s (2013) theoretical exploration of health systems governance, which argues that governance should be informed by, and align with, the values and principles that shape the system.
Clark and Weale (2012) present a conceptual framework for exploring the role social values play in health priority-setting that is cited in eight included papers.6 In one, Tantivess et al. (2012) apply the framework to understand the role of social values in the reform of Thailand’s Universal Health Coverage plan in 2009–10. The authors conclude that, despite efforts to make the decision-making process ‘transparent, participatory, systematic and evidence-based’, values such as welfarism, ethics and equity influenced prioritization decisions, particularly through deliberations among decision-makers (Tantivess et al., 2012, p. 338, 340). The Clark and Weale framework not only presents a defined list of social values but also offers a list of sites in which those values are likely to be seen within decision-making processes (Clark and Weale, 2012) and is thus readily operationalized by analysts.
Another noteworthy framework, Walt and Gilson’s (1994) Health Policy Analysis (HPA) Triangle, was presented as a response to a tendency in HPA to focus on the content of policies, at the neglect of factors such as actors, process and context and the interactions between them. While the framework does not explicitly list social values as a contextual factor, ‘it understands … policy processes to be contested, involving multiple actors, with different concerns, interests and values’ (Gilson et al., 2018, p. 12). The framework is employed in five included papers,7 including a prospective policy analysis of suicide prevention in Sri Lanka to develop feasible policy solutions that align with existing values and interests based on expert panel discussions by Pearson et al. (2010).
van Olmen et al.’s (2010) HSDF is noteworthy in that it considers the role of values in relation to the health systems as a whole (rather than one dimension or aspect of the system). However, the HSDF positions ‘values and principles’ externally to the health system elements, more distal than even ‘context’, and does not include any particular linkages between ‘values and principles’ to any other system elements. This framework informs three reviewed papers,8 including a conceptual study on attributes for health system performance assessment that finds the relationship with societal values to be a key attribute of such assessments (Tashobya et al., 2014). While the presence of such frameworks in the evidence-base reaffirms the centrality of social values to HPSR, this analysis also suggests that more easily operationalized frameworks might do more to facilitate rigorous empirical research on the topic (discussed further below).
Methodological approaches to social values research
To better understand the range of possible methodological approaches used in work on social values, we extracted data on the methods used in each paper—presented in Table 6.9 The papers were fairly evenly divided between empirical (n = 103/208) and non- or loosely empirical10 papers (n = 105/208). Within the 103 empirical papers, a wide range of methodological approaches were evident. Most (more than three quarters) were purely qualitative, with 12 quantitative studies and 13 mixed-methods studies identified. The qualitative studies mainly applied primary/field-based (e.g. process evaluations, ethnographies or action research) rather than secondary/desk-based approaches (e.g. document analysis, discursive methods and qualitative surveys). Review and synthesis and case study approaches were fairly ubiquitous across both the empirical and non-empirical studies.
Table 6.
Methodological approaches
| Method | Empirical | Not empirical | Total |
|---|---|---|---|
| Qualitative—field (interviews, process evaluation, public deliberation, focus-group discussions, participatory methods, observation) | 41 | 3 | 44 |
| Case study or descriptive piece | 29 | 15 | 44 |
| Review or evidence synthesis | 25 | 19 | 44 |
| Editorial, commentary, introduction | 0 | 25 | 25 |
| Reflection, perspective, opinion piece | 0 | 25 | 25 |
| Conceptual and theoretical, framework development or testing | 0 | 16 | 16 |
| Qualitative—desk based (document analysis, policy analysis, discourse analysis, qualitative survey) | 12 | 0 | 12 |
| Quantitative | 11 | 0 | 11 |
| Mixed methods | 10 | 0 | 10 |
| Protocol development or methodological piece | 0 | 5 | 5 |
Very few of the included papers report on studies seeking explicitly to investigate values (n = 48/2018). We found only 24 empirical papers explicitly focused on values in health systems,11 and only eight of these were about LMICs. A table summarizing the aims, methods and findings of these papers is available as Supplementary material. Most of the empirical values-focused papers are either assessments of the values of health policy stakeholders or analyses of values in policy documents or decision-making. The former set mostly uses data from surveys or questionnaires (using both qualitative and quantitative analysis approaches), interview or focus-group discussions, or literature or document review to collect data on the values of users and citizens, healthcare workers and civil servants, or policy and decision-makers. While most of the empirical values-focused work uses qualitative approaches, four of the papers in this set were quantitative. For example, in a study on social solidarity in South Africa, Harris et al. (2011) conducted interviews with 1330 civil servants in the health and education sectors and found that some cultural groups had more accepting attitudes towards cross-subsidization than others. The authors suggest that understanding how social relationships and cultural identities shape values is central to achieving values-oriented reform (Harris et al., 2011).
Similarly, in an empirical study aimed at developing a clearer conceptualization of trust in health systems, Abelson et al. (2009) use focus-group discussions and a public opinion telephone survey to better understand the values of Canadians in relation to the health system. The authors find that individuals value collaboration and alliances with health providers that build trust and note that this relationship can be extended to one between individuals and governments as health system actors (Abelson et al., 2009).
The papers exploring the role of values in decision-making processes mostly rely on data from document and literature reviews or interviews with decision-makers, or a combination thereof. For example, Giacomini et al. (2009) use a review of Canadian health policy documents to explore how ethics frameworks are used in Canadian policy documents. They find that, while there are many common values elements across policy documents, no two documents use the same framework and few documents attempt to justify the chosen values framework. Most of the papers in this category are applications of the Clark and Weale (2012) framework for social values in priority-setting (see below). These papers tend to combine interviews with document and literature reviews to gather data on the role of values in specific priority-setting decisions, which can then be analysed using the framework. For example, Tantivess et al. (2012) use document review to understand the role of social values in coverage decisions for Thailand’s Universal Health Coverage plan and triangulate their findings through personal communication with decision-makers and other key stakeholders.
A small number of the empirical values-focused papers seek to establish or describe a relationship between social values of stakeholders and health system outcomes or characteristics. These papers use survey data, case study approaches, interviews or a combination thereof to explore the health system impact of prevailing social values. For example, Landwehr and Klinnert (2015) explore the effect of value congruence between society and social institutions, and its effect on public acceptance of prioritization decisions and trust in the health system at large. The authors compare across the UK, Germany and France using survey data and document review. As a whole, the analysis of methodological approaches, particularly with regard to values-focused empirical studies, suggests that research on the topic is relatively labour and resource intensive, often combining methodological approaches spanning field-work, large-scale data collection through surveys and documentary analysis.
A large number of papers (160/208) do not focus specifically on values but nonetheless mention values in the introduction or background sections—as foundational or contextual knowledge—or as knowledge necessary to interpreting, understanding or explaining the findings. This suggests that, in many cases, it is necessary to incorporate an understanding of social values and their role in health systems in the interpretation of evidence on other topics. For example, Walker and Gilson (2004) use questionnaires and in-depth interviews to investigate how South African nurses in urban Community Health Centres experience the implementation of the free care policy. The study reveals that values influence nurses’ experiences of, and responses to, policies and the authors conclude that, to make sense of nurses’ practices, it is necessary to understand them as social actors within social, historical and professional contexts (Walker and Gilson, 2004).
The non-empirical and ‘loosely empirical’ papers reviewed included perspectives and opinion pieces; editorials and commentaries; non-systematic reviews, conceptual and theoretical discussions and framework development pieces; descriptive pieces; and methodological guidelines and protocols. As with the empirical papers, about a quarter (n = 24/105) were explicitly focused on values, a third of which were ‘loosely empirical’. For example, Saltman and Bergman (2005) use policy documents, social observations and personal experience to explore how Sweden’s social and political context ensures that two core Swedish values (jamlikhet/equality and trygghet/security) influence national health policy-makers, resulting in system-wide resilience to outside pressures for change. The authors argue that ‘core social values tied to national culture play an essential role in defining both the structure of existing health sector institutions and the range of feasible policy options with which to modify these institutions’ (Saltman and Bergman, 2005, p. 255).
Another example is a book review by Reinhardt (2003), in which he argues that Canada’s deep-rooted social values, reflected in their national health system, underlie the country’s historical opposition to external cultural influences. However, he also cautions that changes in the structure of health systems have the capacity to undermine national values (Reinhardt, 2003). The analysis of methodological approaches suggests that the relative lack of empirical values-focused research, particularly in LMICs, may reflect the resource-intensive nature of the types of methodologies commonly used in this type of work.
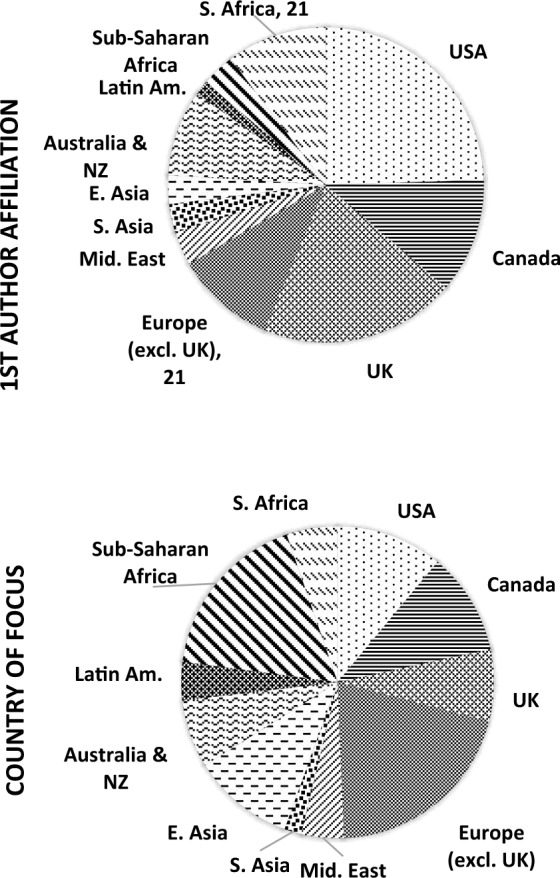
Geographic distribution—country of focus and first author affiliation
The politics of where and how HPSR knowledge is produced has been a growing concern within the field in recent years (Bennett et al., 2018; Gilson et al., 2018; George et al., 2019). To better understand the geographic distribution of the HPSR evidence-base on social values, we mapped the country of focus for each article by geographic region (Figure 3). This reveals a significant proportion of the research focuses on Canada, the USA and the UK, which together account for nearly a third of all research on social values in health systems. With 11 included papers, South Africa is noteworthy as the only middle- or lower-income country in which a relatively significant body of research has emerged.
Figure 3.
Geographic mapping by region
This uneven distribution is more acute when the evidence-base is analysed according to the institutional affiliation of the first author of each study as a proxy for the geographic origin of the paper. Authors from Canada, the UK and the USA represent more than half of all the first authors, and less than a quarter of all papers had first authors based in Africa (excluding South Africa), Asia and the Middle East. Once again, South Africa is comparatively well represented (n = 21/208 papers). When classified according to World Bank income classifications (World Bank, 2019) rather than regional groupings, similar trends emerge, with most included papers focusing on HICs, and only five and eight papers produced by authors at institutions in low-income and lower–middle-income countries, respectively (Figure 4).
Figure 4.

Geographic mapping by income group
A quarter of the included papers did not focus on any specific country, region or income bracket. These articles are largely non-empirical pieces or global reviews and tend to make general claims about the nature of health systems that may be interpreted by readers as universally applicable. Almost all of these papers were written by authors based in high-income (n = 44/208) or upper–middle-income countries (n = 7/208).
This analysis classifies papers according to the institutional affiliation of the first author only, so may not accurately represent the geographic distribution of all the authors contributing to the evidence-base. To account for this, we also conducted an analysis of the most commonly recurring authors, irrespective of authorship position. Figure 5 gives the number of empirical and other papers contributed by each author (excluding those with only one or two contributions). Many well-renowned HPSR authors are shown to have made a substantial contribution to the evidence-base, reaffirming the importance of social values to health systems research. Unsurprisingly, however, most of these authors are from high- or upper–middle-income countries. Only three of the authors contributing three or more papers to the evidence-base are affiliated with institutions in low- or lower–middle-income countries.
Figure 5.

Number of papers per author
The geographic mapping suggests that paying attention to social values in relation to health systems is fairly ubiquitous—with research identified across all geographic regions—but unevenly distributed. In addition, much of the research on this topic is led by out-of-country actors.
Discussion
This study reviews the HPSR evidence on social values in health systems. While data collection was conducted systematically, the iterative, multi-phase search approach may have inadvertently missed some relevant literature. In addition, the designation of particular papers as either HPSR or not is necessarily subjective and, although steps were taken to ensure this was done according to predetermined criteria, other researchers may have interpreted the criteria differently. Finally, the purpose of an evidence mapping review is to provide a broad assessment of the ‘state of evidence’ on a particular topic. The purposively broad review therefore has limits in terms of depth of analysis—for example we do not compare or assess particular findings from empirical papers or assess the ‘best’ health systems intervention involving the manipulation of social values.
Despite these limitations, the study reveals significant geographic, methodological and conceptual gaps in the literature and suggests that these gaps have significant consequences for the development of this field of study.
Geographic gaps: the importance of context-specific and embedded research
The geographic mapping reveals significant gaps in the evidence-base with respect to research focusing on Eastern Europe, Latin America, South Asia and the Middle East (with respect to evidence published in English). This geographic distribution indicates a failure to adequately explore the important role that social values play in the development and strengthening of health systems in these regions, and LMICs generally. This is problematic for a number of reasons.
First, evidence of the role values play in health systems is likely more valuable and necessary for LMICs. While all health systems are inherently relational (Bevan and Robinson, 2005; Freedman et al., 2005; Bloom et al., 2008; Gilson, 2012b), there is evidence to suggest that relational factors such as values might matter more in LMICs and fragile and conflict affects states where formal mechanisms and systems hardware may be weaker (Palmer and Mills, 2003; Batley and Mcloughlin, 2010). In addition, values-based health systems could play an important role in strengthening social and political institutions in these contexts. Evidence for the relationship between strong health systems and the development of just, democratic and cohesive societies is growing (Freedman, 2005; Mackintosh and Koivusalo, 2005; London et al., 2015; WHO, 2016). For example, Kruk et al. (2010) draw on literature conceptualizing health systems as social and political institutions to develop a logic model for the contribution of the health system to social cohesion, state-building, solidarity and public trust in the state. Similarly, McIntyre et al. (2006) have demonstrated that the commercialized nature of the South African health system has undermined government’s efforts to institute reforms that would contribute to social development and social cohesion. This suggests that more inequitable, less cohesive societies have that much more to gain from evidence-based efforts in health systems strengthening that acknowledge the central role of values and relational factors.
Second, context-specific knowledge is essential. While social values are a central dimension of any health system, both the nature of the values themselves and the extent of their influence will vary between contexts. For example, Ridde (2008) argues that policy actors in Burkina Faso tend to prioritize efficiency over equity in the implementation of public health policies, largely because inequity has not been seen as a public policy issue in that context. In Thailand, Teerawattananon and Russell (2008, p. S58) found that decision-makers felt that the public would simply not accept priority-setting decisions based on economic evaluation if ‘the societal values of equity or justice were not incorporated into decision-making’. Similarly, while libertarian values of choice and freedom underlie the USA’s market-based health financing system (Schlesinger, 2002; Roberts et al., 2003; Ruger, 2008), in neighbouring Canada the universality of the health system is a point of national pride (Redden, 1999; Axworthy and Spiegel, 2002; Giacomini et al., 2004; Daw et al., 2014). This suggests that dominant values may differ between settings and, therefore, affect health system change in different ways. For this reason, as with most HPSR, findings about the way values operate in one context may not be directly generalizable and gaps in the evidence-base can only be filled with context-specific research (Bennett et al., 2011; Gilson, 2012a).
Relatedly, given the well-established importance of a deep understanding of contextual realities and local value systems to conducting rigorous HPSR (Sheikh et al., 2014a; George et al., 2015; Edwards et al., 2017; Hasnida et al., 2017), the mal-distribution of literature may also point towards a failure to adequately harness the existing capacity of LMIC researchers with deep tacit knowledge of their local contexts (Hasnida et al., 2017). This tacit knowledge is all the more valuable in under-researched contexts, for which there is likely very limited secondary data capturing contextual complexities.
The limited evidence on social values in LMICs is often produced by researchers based outside of the country they are researching. We identified a significant over-representation of authors from high-income countries in this regard, with a large proportion of the evidence-base being produced by authors in Canada, the USA and the UK. This dominance is widely acknowledged as troubling within HPSR—a research field that ‘should be driven by understanding of local contexts’ (Bennett et al., 2011, p. 1), with the specific aim of contributing to health systems strengthening in LMICs (Adam et al., 2011; Hasnida et al., 2017)—reflecting global power imbalances in knowledge production (Bloom and Standing, 2008; Gilson and Raphaely, 2008; Yao et al., 2014; Hasnida et al., 2017).
While out-of-country researchers can, and regularly do, produce relevant and rigorous health systems evidence within LMICs, such evidence may be less likely to directly impact policy-making in those contexts. Evidence shows that embedded researchers are both more likely to have in-depth and nuanced knowledge of the system and the political and cultural context, and to be able to ‘see’ what is tacit or un-spoken (Franzen et al., 2017; Olivier et al., 2017a,b)—as values often are.
Furthermore, research is more likely to be taken up by decision-makers and practitioners when produced by actors embedded in, or with existing relationships within, the country (AHPSR, 2018; Cheetham et al., 2018; Ghaffar et al., 2017; Hasnida et al., 2017). As such, work conducted by researchers who are not embedded in the context may be less relevant and have a more limited effect on health systems strengthening. Recognition of this has spurred growing interest in embedded research approaches in HPSR—in which researchers position themselves as part of the health system and build trust-based relationships with policy-makers and implementers over time, to ensure that research questions are informed by real-world evidence needs, and to open communication channels for the feedback of findings that inform practice (George et al., 2019; AHPSR, 2017; Olivier et al., 2017b). In addition to the large body of work produced by out-of-country researchers, only one included study reported using an embedded research approach (Gilson et al., 2017).
The findings from this review mirror broader trend in HSPR. Despite the acknowledged need for HPSR about and from LMICs, the bulk of evidence currently tends to be produced in, and focused on, developed country contexts (Gilson and Raphaely, 2008; Adam et al., 2011; Bennett et al., 2011; Erasmus et al., 2014; Hasnida et al., 2017). Furthermore, the limited capacity for HPSR in LMIC contexts—the effect of structural and systemic barriers—results in an unfortunately high proportion of LMIC-focused HPSR being conducted by out-of-country researchers (Adam et al., 2018). This status quo is particularly problematic given the need for a thick understanding of local contexts in HPSR (Gilson and Raphaely, 2008; Gilson et al., 2011b; Gilson, 2012a) and is all the more concerning with regard to the study of social values, which arguably demands a deep understanding of local social and norms and cultural dynamics.
Methodological gaps: the need for more empirical research and the potential of methods rooted in social sciences
There are also significant gaps in the evidence based with respect to the range of methodological approaches employed in research on social values. First, as discussed above, a large proportion of the evidence-base is not empirical and only a fifth of the empirical studies are asking research questions about values in health systems. Furthermore, we only identified seven empirical papers focusing on social values in LMICs. These findings mirror that of Gilson and Raphaely (2008), who reviewed work analysing health policy processes and found that fewer than half of the included studies were empirical studies focused on LMICs.
The almost even split between empirical and non-empirical work on the topic is concerning because, while rigorous conceptual or theoretical work is important and should not be under-valued (Bennett et al., 2011; Sheikh et al., 2011; Gilson, 2012a; Edwards et al., 2017), this theory must be informed by empirical literature from a broad range of contexts and, as noted above, theory developed on the basis of empirical work from a limited range of contexts is unlikely to be widely relevant. The paucity of empirical, values-focused research on LMIC settings indicates a risk that the growth of the theoretical evidence-base out-strips the empirical work from LMICs, resulting in a body of theoretical literature that is not sufficiently reflective of LMIC realities.
Similarly, the shortage of embedded approaches and in-country perspectives shaping the literature, which forms the foundation for conceptual development and discourse-building, risks the development of theory that fails to reflect local realities (Edwards et al., 2017). As almost all of papers of purportedly general relevance (i.e. without a particular country of focus) were first-authored by researchers in high-income countries, there is a potential for ‘conceptual capture’—promulgating a particular perspective that may not adequately reflect the realities of LMIC settings (Giacomini et al., 2009; Shams et al., 2016). Producing empirical HPSR evidence on the role of values in health systems through context-specific research in under-researched settings is necessary to strengthen the evidence-base and inform representative theory.
The large number of non-empirical and loosely empirical papers making reference to social values suggests that commentary and reflective-type publication formats allow HPSR authors to explore underlying assumptions or beliefs about values that would require a significant burden of proof if they were presented in empirical papers. Interestingly, of the authors contributing the most papers to the evidence-base, almost a quarter of those contributing three or more papers do so entirely through non-empirical or loosely empirical papers, suggesting, perhaps, that these ideas inform the author’s thinking, but nonetheless are not considered appropriate subjects for empirical research.
However, the limited number of empirical papers focusing explicitly on values is also likely a reflection of the relatively resource intensive nature of this work. Most of the empirical, values-focused papers utilize large-scale survey data in combination with interviews with healthcare workers or decision-makers, and/or review of policy documents, decision-making records or academic literature. These are relatively labour- and capacity-intensive research approaches that may well necessitate both a significant number of researchers on the team and substantial funding to support them. Furthermore, in some contexts, relevant survey data may not be available and availability of documentary records from decision-making processes is dependent on the extent to which these processes are transparent. In these settings, empirical research on values would require additional resources to conduct surveys and interview decision-makers—and may well be impossible.
There is also a paucity of work drawing on social science methodologies. This is somewhat surprising given that a fundamental feature of HPSR is that it draws on a wide variety of concepts and methods from social sciences to explore complexity (Gilson et al., 2011b; Sheikh et al., 2014a), precisely because these approaches can help researchers tackle complex topics where multiple interpretations are possible (Gilson et al., 2011b; Topp et al., 2018), such as the relationship between social values and health systems. In addition, there is existing work on health systems and social values within the social sciences that is largely ignored in this evidence-base. For example, there is a body of work in medical anthropology that uses ethnography to understand how health systems influence citizens’ understandings of their rights and entitlements in relations to the state (see for example, Abadía‐Barrero, 2016; Dao and Mulligan, 2016; Prince, 2017).
This gap is likely a reflection of the well-established ‘disciplinary capture’ in the field of HPSR (Sheikh et al., 2011). While HPSR is characterized as a necessarily trans-disciplinary field (Sheikh et al., 2014a; Bennett et al., 2018), many authors have commented on the persistent schism between positivist research with generalizable results and relativist research in which context specificity is key (Remme et al., 2010; Gilson et al., 2011b; Gilson, 2012a; Hoffman et al., 2012). As a result of a growing need, largely funder-driven, to easily appraise the ‘quality’ of qualitative work (and therefore its readiness to directly inform policy) through assessments of ‘sampling, coding, validity, reliability and generalizability’ (Torrance, 2017, p. 75), there is a tendency in the field to valorize research reflecting positivist knowledge paradigms and forms of qualitative social science research that are more readily quantifiable (Sheikh et al., 2011; Topp et al., 2018). In addition, it has been suggested that, in some settings, particularly LMICs, there is a limited capacity to undertake rigorous qualitative research (Lewin and Glenton, 2018). This is acknowledged to result in the under-utilization of social science methodologies, and attendant knowledge paradigms, limiting the capacity of the field to conduct rigorous research on software factors (Gilson et al., 2011b; Sheikh et al., 2011; Gilson, 2012a). Purposeful efforts to counter these forces, and actively draw on methodologies from the social sciences, may be necessary in developing the empirical evidence-base on the topic.
Conceptual gaps: definitional clarity and the need for conceptual frameworks and theory
A lack of definitional and conceptual clarity is apparent. As noted, very few included papers offered a definition or explanation of ‘social values’ and no common definition was used across any of the papers. In addition, the definitions and explanations that are presented vary considerably. While a fixed, universal definition of the term is perhaps neither necessary nor desirable—because hasty concretization of a term risks ‘constraining the … natural development of the field’ (Sheikh et al., 2011, p. 5)—given scope of the evidence-base, and the fact that values have been considered central to HPSR since its inception, it is surprising that no consensus framings have emerged.
In addition to definitional issues, there is a general lack of specificity in the evidence-base with regard to the mechanisms or pathways through which values impact health system change. In the synthesis of statements about the relationship between health systems and social values, a large proportion of the relational statements drew a connection between some element or function, and the health system as a whole. Such statements do not specify any particular dimension of the health system and, therefore, make it difficult to identify the causal mechanism at play.
Similarly, the prominent conceptual frameworks identified rarely indicate how analysts can or should identify the influence of values. The Clark and Weale Framework for priority-setting (2012) is the exception, as it not only presents a defined and concise list of social values but also offers a comprehensive framework for analysis of those values—comprising a list of sites in which those values are likely to be seen within decision-making processes. In other words, the framework tells the researcher how it should be applied in analysis. The Clark and Weale framework seems to have given rise to a significant number of studies employing similar methodologies across a range or contexts, and therefore producing comparable results.
The other three dominant frameworks, however, seem to be used (within the body of included literature, at least) more conceptually—often combined with other frameworks and conceptual tools to inform or justify a particular understanding of health systems. In the case of the HPA Triangle framework, this is somewhat surprising, given that the framework does offer an approach to analysis. However, both the HPA triangle (Walt and Gilson, 1994) and the hardware/software distinction (Sheikh et al., 2011) constitute heuristic devices encouraging analysts to consider the effect of values and other software factors on the behaviour of health policy actors but do not indicate where analysts should look. By positioning values as external to the rest of the health system, the HSD framework (van Olmen et al., 2010) indicates the importance of values but does not indicate where this effect might be seen, nor suggest mechanisms or pathways of influence. By offering a common conceptual tool to organize research and analysis, frameworks can enable more rigorous research on particular topics (Gilson, 2012a). It seems, however, that the frameworks evident in the HPSR literature on social values achieve this only to a limited extent.
While the value of conceptual frameworks for making sense of complexity cannot be overstated, this review suggests that the operationalization of the existing frameworks might encourage or enable further empirical work on the relationship between social values and health systems and that the lack of such a framework presents a significant gap in the literature. One strategy for expanding the empirical evidence-base on the topic, therefore, may be to develop the available conceptual frameworks to be more readily operationalized.
The importance of values in HPSR
Despite significant gaps in the HPSR evidence-base on social values, the substantive body of evidence reveals the myriad of ways in which social values shape health systems and affirms that values are seen as central to understanding health system change across a broad range of HPSR literature—in keeping with broader literature described in the introduction (Gilson, 2012a; Sheikh et al., 2011; 2014a). The scale of the evidence-base—seen in the relatively large number of papers referring to social values—as well as the scope of included papers (with reference to social values made across a diversity of areas of work), confirms that social values are a key concept within HPSR.
As suggested in the introduction, values were found to be used as explanations for health system change with respect to governance, implementation, interpersonal relationships between system actors, policy decision-making and health system change and reform. However, we also identified a significant body of work on the role of values in priority-setting and a number of papers on financing, planning and management, public participation and knowledge translation. The particular prominence of values in work on priority-setting, health systems analysis, health systems reform and policy analysis indicates that, in these areas of work, the explicit consideration of values is becoming normalized, and perhaps expected, as an indicator of a thorough analysis.
In addition, the centrality of social values to understanding and conceptualizing health systems functioning, posited by key HPSR authors (Sheikh et al., 2011; Gilson, 2012a), is confirmed by the match between the growth of HPSR literature on social values and HPSR literature more generally. Finally, the large proportion of papers that are not specifically focused on social values, but nonetheless use social values either as foundational or background knowledge, or in the discussion and conclusion, confirms the foundational role play in the field—indicating that reference to social values is often necessary background or contextual information for demonstrating the substantive relevance of an HPSR research question, describing the context in which the systems or policy problem exists, or interpreting the relevance of the study findings—even when values are not the subject being researched.
Simultaneously, theory and evidence are emerging on the nature of the relationship between citizens and the health system—evident in papers making causal claims about the influence of health system on social values. This literature suggests that, in strengthening health systems through research paying close attention to ‘ideas, interests, values, norms and relationships’, we can harness the power of health systems to build more equitable societies (Sheikh et al., 2014a, p. 2).
Strengthening the HPSR evidence-base on social values
To this end, the review points to a number of strategies for strengthening the HPSR evidence-base on social values. As a research community, HPS researchers, funders and guiding institutions must strive to harness the capacity of researchers in low-income and under-researched settings to strengthen the evidence-base of empirical work on social values conducted by in-country or embedded researchers with deep contextual knowledge of those settings.
In addition, HPS researchers should consciously strive to meet the trans-disciplinary aspirations of the field and actively draw on social science methodologies in their work. However, it must be recognized that many of the methodologies that allow researchers to conduct high-quality empirical work on values may well be particularly resource intensive, requiring longer study timelines and large-scale data collection efforts. Such resource and data intensive research is likely more challenging in LMICs, where not only is funding more constrained, but also decision-making processes more opaque, and less likely to be captured in publicly available documents.
Conceptual tools that are easily operationalized and relevant across distinct areas of work within HPSR are necessary to building consensus framings and common language and will likely facilitate and encourage empirical research. However, researchers doing conceptual and theoretical work must strive to ensure that their work is founded on quality empirical research from diverse contexts and adequately represents the complex realities of LMICs. As the theoretical and empirical evidence-base grows, this knowledge should be used to inform the development of operationalizable frameworks that will support rigorous future research on the subject.
Strengthening the evidence-base will also require countering the still pervasive ideas about research hierarchies that valorize research centralizing health system hardware and reflecting positivist knowledge paradigms as more rigorous and of higher substantive relevance. Research needs not have a direct policy influence to be valuable, and rigorous social science conducted from a relativist perspective can indirectly bring about system change or provide crucial conceptual tools that shape policy-makers’ assumptions and contribute to health systems strengthening.
Conclusion
In 1977, a study of health systems research and innovations published in The New England Journal of Medicine concluded that ‘there is little reason to expect such research to produce major alterations in the system, since these alterations are linked to changes in the values and expectations of society’ (Lewis, 1977, p. 423). Since then, however, HPSR has emerged as a trans-disciplinary field of study with capacity to understand health systems as complex people-centred systems and to produce evidence on values that contributes to stronger, more just health systems and societies.
To realize this potential of values-focused research; however, it is necessary to strengthen the body of evidence on values in health systems. This will require overcoming the systemic barriers within the field that result in imbalances in knowledge production between high-income and LMIC countries, seeking specifically to enable further empirical and conceptual work in low-income, under-researched contexts. Promoting empirical research on values in LMICs that can be used to inform representative and rigorous theory on the subject of values in health systems is also key and will lay the foundation for the development of consensus framings, and operationalizable frameworks to support future work. In addition, it will be necessary to recognize the deep contextual knowledge of embedded researchers as a significant intangible asset in research endeavours and invest in embedded research projects that take a longitudinal perspective and draw on social science methodologies. This also entails actively countering pervasive ideas about research hierarchies that prize systems hardware-focused studies using positivist methodologies as more substantively relevant or rigorous. As this review has shown, values play a central role in health system change and, a better understanding of this role will enable HPS researchers and practitioners to more effectively harness the power of values for progressive health system change.
Supplementary Material
Acknowledgements
This study was supported by the Alliance for Health Policy and Systems Research (World Health Organization) Health Policy Analysis Fellowship, the University of Cape Town Health Policy and Systems Division, the National Research Foundation of South Africa and the University of Cape Town. The authors would like to acknowledge colleagues at the University of Cape Town (South Africa), the University of the Western Cape (South Africa) and the Institute of Tropical Medicine (Belgium) for their assistance in the data collection phase of this study.
Ethical approval. No ethical clearance was required for this research. However, the broader research project, of which this paper forms a part, has been granted ethical clearance but the University of Cape Town, Faculty of Health Sciences, Human Research Ethics Committee (HREC REF:848/2019).
Footnotes
To keep the scope of the search manageable, and sufficiently sensitive to identify material on social values in relation to health policy and systems, a decision was made to restrict the first search string to title or abstract. This approach successfully excluded material that may mention health policy or systems, but that is primarily clinical, epidemiological or economic.
Twenty-three key authors in the field: A Ghaffar, L Gilson, B Pratt, S Bennett, F El-Jardali, S Theobold, A George, A Mills, T Mirzoev, N Tran, I A Agyepong, M Bigdeli, B Marchal, D H Peters, B Uzochukwu, T Adam, G Boom, K Daniels, U Lehman, S Molyneux, SAbimbola, K Sheikh and A A Hyder.
Many but not all the included papers met the initial four criteria. A few of included items met only two of these criteria.
This is an additional criterion because, for the most part, inclusion was decided on a case-by-case basis—i.e. a paper from a particular author might be excluded even if other work by that author was included.
Abimbola et al. (2017), Agyepong et al. (2017), Fattore and Tediosi (2013), Gilson et al. (2017), Langlois et al. (2018) and Sheikh et al. (2014a,b).
Ahn et al. (2012), Keren and Littlejohns (2012), Landwehr and Klinnert (2015), Littlejohns et al. (2012a,b,c), Mostafavi et al. (2016), Russell et al. (2014), Tantivess et al. (2012) and Whitty and Littlejohns (2015).
Buse et al. (2009), Gilson (2012a,b), Grundy (2015), Koduah et al. (2018) and Pearson et al. (2010).
These data were captured as presented by the author in the abstracts or method section of the paper. For many papers, more than one method was used. As such, the totals in this table exceed the total number of papers included in the review.
These were categorised as either non-empirical or loosely empirical to capture the distinction between opinion pieces, editorials or commentaries and articles in which methods and findings are not explicitly laid out, but which are nonetheless presented as based on common knowledge, existing evidence or personal experience.
It must be noted that categorising a study as ‘about’ values is subjective—a study may have sought to explore values through a particular lens and the title, and therefore the focus on values may not be reflected in the title or keywords, or made explicit in the methods. For this reason, papers were categorised as ‘about’ values, only if this was made explicit in the title, abstract or methods.
Supplementary Data
Supplementary data are available at Health Policy and Planning online.
References
- Abadía‐Barrero CE. 2016. Neoliberal justice and the transformation of the moral: the privatization of the right to health care in Colombia. Medical Anthropology Quarterly 30: 62–79. [DOI] [PubMed] [Google Scholar]
- Abelson J, Miller FA, Giacomini M.. 2009. What does it mean to trust a health system? Health Policy 91: 63–70. [DOI] [PubMed] [Google Scholar]
- Abimbola S, Negin J, Martiniuk AL, Jan S.. 2017. Institutional analysis of health system governance. Health Policy and Planning 32: 1337–44. [DOI] [PubMed] [Google Scholar]
- Adam GP, Di M, Cu-Uvin S. et al. 2018. Strategies for improving the lives of US women aged 40 and above living with HIV/AIDS: an evidence map. Systematic Reviews 7: 25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Adam T, Ahmad S, Bigdeli M, Ghaffar A, Røttingen J-A.. 2011. Trends in health policy and systems research over the past decade: still too little capacity in low-income countries. PLoS One 6: e27263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Agyepong IA, Kwamie A, Frimpong E. et al. 2017. Spanning maternal, newborn and child health (MNCH) and health systems research boundaries: conducive and limiting health systems factors to improving MNCH outcomes in West Africa. Health Research Policy and Systems 15: 54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ahn J, Kim G, Suh HS, Lee SM.. 2012. Social values and healthcare priority setting in Korea. Journal of Health Organization and Management 26: 343–50. [DOI] [PubMed] [Google Scholar]
- AHPSR. 2004. Strengthening Health Systems: The Role and Promise of Policy and Systems Research. Geneva, Switzerland: Alliance for Health Policy and Systems Research.
- AHPSR. 2017. Embedded Health Policy and Systems Research: Within the System, for the System, Used by the System. Geneva, Switzerland: Alliance for Health Policy and Systems Research.
- AHPSR. 2018. Embedded Health Policy and Systems Research: Within the System, for the System, Used by the System. Geneva, Switzerland: Alliance for Health Policy and Systems Research.
- AHPSR. 2019. What Is Health Policy and Systems Research (HPSR)? Geneva, Switzerland: World Health Organization. [Google Scholar]
- Atun R, Menabde N.. 2008. Health systems and systems thinking In: Coker R, Atun R, McKee M (eds). Health Systems and the Challenge of Communicable Diseases: Experiences from Europe and Latin America. Berkshire, UK: Open University Press, McGraw-Hill Education, 121–40. [Google Scholar]
- Axworthy L, Spiegel J.. 2002. Retaining Canada’s health care system as a global public good. CMAJ 167: 365–6. [PMC free article] [PubMed] [Google Scholar]
- Batley R, Mcloughlin C.. 2010. Engagement with non-state service providers in fragile states: reconciling state-building and service delivery. Development Policy Review 28: 131–54. [Google Scholar]
- Bennett S, Agyepong IA, Sheikh K. et al. 2011. Building the field of health policy and systems research: an agenda for action. PLoS Medicine 8: e1001081. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bennett S, Chanfreau C.. 2005. Approaches to rationing antiretroviral treatment: ethical and equity implications. Bulletin of the World Health Organization 83: 541–7. [PMC free article] [PubMed] [Google Scholar]
- Bennett S, Frenk J, Mills A.. 2018. The evolution of the field of Health Policy and Systems Research and outstanding challenges. Health Research Policy and Systems 16: 43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berlan D, Shiffman J.. 2012. Holding health providers in developing countries accountable to consumers: a synthesis of relevant scholarship. Health Policy and Planning 27: 271–80. [DOI] [PubMed] [Google Scholar]
- Bertscher A, London L, Orgill M.. 2018. Unpacking policy formulation and industry influence: the case of the draft control of marketing of alcoholic beverages bill in South Africa. Health Policy and Planning 33: 786–800. [DOI] [PubMed] [Google Scholar]
- Bevan G, Robinson R.. 2005. The interplay between economic and political logics: path dependency in health care in England. Journal of Health Politics, Policy and Law 30: 53–78. [DOI] [PubMed] [Google Scholar]
- Bloom G, Standing H.. 2008. Future health systems: why future? Why now? Social Science & Medicine (1982) 66: 2067–75. [DOI] [PubMed] [Google Scholar]
- Bloom G, Standing H, Lloyd R.. 2008. Markets, information asymmetry and health care: towards new social contracts. Social Science & Medicine (1982) 66: 2076–87. [DOI] [PubMed] [Google Scholar]
- Boell SK, Cecez-Kecmanovic D. 2014. A hermeneutic approach for conducting literature reviews and literature searches. Communications of the Association for Information Systems, 34: 257–86. [Google Scholar]
- Bonell C, Harden A, Wells H. et al. 2011. Protocol for a systematic review of the effects of schools and school-environment interventions on health: evidence mapping and syntheses. BMC Public Health 11: 453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bonell C, Jamal F, Harden A. et al. 2013. Systematic review of the effects of schools and school environment interventions on health: evidence mapping and synthesis. Public Health Research 1: 1–320. [PubMed] [Google Scholar]
- Bragge P, Clavisi O, Turner T. et al. 2011. The global evidence mapping initiative: scoping research in broad topic areas. BMC Medical Research Methodology 11: 92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Broqvist M, Garpenby P.. 2015. It takes a giraffe to see the big picture—citizens’ view on decision makers in health care rationing. Social Science & Medicine (1982) 128: 301–8. [DOI] [PubMed] [Google Scholar]
- Buse K, Dickinson C, Gilson L, Murray SF.. 2009. How can the analysis of power and process in policy-making improve health outcomes? The Official Journal of the International Hospital Federation 45: 14. [PubMed] [Google Scholar]
- Buse K, Mays N, Walt G.. 2012. Making Health Policy. UK: McGraw-Hill Education. [Google Scholar]
- Cady P. 2016. A system of system lenses for leadership decision-making. Healthcare Management Forum 29: 8–11. [DOI] [PubMed] [Google Scholar]
- Cheetham M, Wiseman A, Khazaeli B. et al. 2018. Embedded research: a promising way to create evidence-informed impact in public health? Journal of Public Health (Oxford, England) 40: i64–i70. [DOI] [PubMed] [Google Scholar]
- Clark S, Weale A.. 2012. Social values in health priority setting: a conceptual framework. Journal of Health Organization and Management 26: 293–316. [DOI] [PubMed] [Google Scholar]
- Danan ER, Krebs EE, Ensrud K. et al. 2017. An evidence map of the women veterans’ health research literature (2008–2015). Journal of General Internal Medicine 32: 1359–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dao A, Mulligan J.. 2016. Toward an anthropology of insurance and health reform: an introduction to the special issue. Medical Anthropology Quarterly 30: 5–17. [DOI] [PubMed] [Google Scholar]
- Daw JR, Morgan SG, Collins PA, Abelson J.. 2014. Framing incremental expansions to public health insurance systems: the case of Canadian pharmacare. Journal of Health Politics, Policy and Law 39: 295–330. [DOI] [PubMed] [Google Scholar]
- De Allegri M, Sieleunou I, Abiiro G, Ridde V.. 2018. How far is mixed methods research in the field of health policy and systems in Africa? A scoping review. Health Policy and Planning 33: 445–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Savigny D, Adam T.. 2009. Systems Thinking for Health Systems Strengthening. World Health Organization, Geneva. [Google Scholar]
- Donabedian A. 1972. Models for organizing the delivery of personal health services and criteria for evaluating them. The Milbank Memorial Fund Quarterly 50: 103–54. [Google Scholar]
- Edwards A, Whyle E, Grieve A, Lee C, Rajpuria C.. 2017. Expanding the Boundaries of HPSR: A Southern Perspective. Essay awarded 1st place in 2017 Alliance for Health Policy and Systems Research competition.
- Erasmus E, Orgill M, Schneider H, Gilson L.. 2014. Mapping the existing body of health policy implementation research in lower income settings: what is covered and what are the gaps? Health Policy and Planning 29: iii35–iii50. [DOI] [PubMed] [Google Scholar]
- Exworthy M. 2008. Policy to tackle the social determinants of health: using conceptual models to understand the policy process. Health Policy and Planning 23: 318–27. [DOI] [PubMed] [Google Scholar]
- Fattore G, Tediosi F.. 2013. The importance of values in shaping how health systems governance and management can support universal health coverage. Value in Health 16: S19–S23. [DOI] [PubMed] [Google Scholar]
- Franzen SR, Chandler C, Lang T.. 2017. Health research capacity development in low and middle income countries: reality or rhetoric? A systematic meta-narrative review of the qualitative literature. BMJ Open 7: e012332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Freedman LP. 2005. Achieving the MDGs: health systems as core social institutions. Development 48: 19–24. [Google Scholar]
- Freedman LP, Waldman Rj, de Pinho H., Wirth Me. 2005. Who’s Got the Power? Transforming Health Systems for Women and Children. London: Task Force on Child Health and Maternal Health. [DOI] [PubMed] [Google Scholar]
- George A, Olivier J, Glandon D, Kapilashrami A, Gilson L.. 2019. Health systems for all in the SDG era: key reflections based on the Liverpool statement for the fifth global symposium on health systems research. Health Policy and Planning 34: ii135–ii138. [DOI] [PubMed] [Google Scholar]
- George A, Scott K, Garimella S. et al. 2015. Anchoring contextual analysis in health policy and systems research: a narrative review of contextual factors influencing health committees in low and middle income countries. Social Science & Medicine 133: 159–67. [DOI] [PubMed] [Google Scholar]
- Ghaffar A, Langlois EV, Rasanathan K. et al. 2017. Strengthening health systems through embedded research. Bulletin of the World Health Organization 95: 87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Giacomini M, Hurley J, Gold I, Smith P, Abelson J.. 2004. The policy analysis of ‘values talk’: lessons from Canadian health reform. Health Policy (Amsterdam, Netherlands) 67: 15–24. [DOI] [PubMed] [Google Scholar]
- Giacomini M, Kenny N, DeJean D.. 2009. Ethics frameworks in Canadian health policies: foundation, scaffolding, or window dressing? Health Policy 89: 58–71. [DOI] [PubMed] [Google Scholar]
- Gilson L. 2003. Trust and the development of health care as a social institution. Social Science & Medicine (1982) 56: 1453–1468. [DOI] [PubMed] [Google Scholar]
- Gilson L. 2012. a. Health Policy and Systems Research: A Methodology Reader. Geneva: Alliance for Health Policy and Systems Research, WHO. [Google Scholar]
- Gilson L. 2012. b. Health systems and institutions In: Smith RD, Hanson K (eds). Health Systems in Low- and Middle-Income Countries: An Economic and Policy Perspective. Oxford: Oxford University Press, 21–48. [Google Scholar]
- Gilson L, Daire J, Patharath A, English R.. 2011. a. Leadership and governance within the South African health system. South African Health Review, 2011: 69–80. [Google Scholar]
- Gilson L, Hanson K, Sheikh K. et al. 2011. b. Building the field of health policy and systems research: social science matters. PLoS Medicine 8: e1001079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gilson L, Lehmann U, Schneider H.. 2017. Practicing governance towards equity in health systems: LMIC perspectives and experience. International Journal for Equity in Health 16:171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gilson L, McIntyre D.. 2008. The interface between research and policy: experience from South Africa. Social Science & Medicine (1982) 67: 748–759. [DOI] [PubMed] [Google Scholar]
- Gilson L, Orgill M, Shroff ZC.. 2018. A Health Policy Analysis Reader: The Politics of Policy Change in Low- and Middle-Income Countries. Geneva: World Health Organization. [Google Scholar]
- Gilson L, Raphaely N.. 2008. The terrain of health policy analysis in low and middle income countries: a review of published literature 1994–2007. Health Policy and Planning 23: 294–307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gostin LO, Powers M.. 2006. What does social justice require for the public’s health? Public health ethics and policy imperatives. Health Affairs 25: 1053–1060. [DOI] [PubMed] [Google Scholar]
- Grant MJ, Booth A.. 2009. A typology of reviews: an analysis of 14 review types and associated methodologies. Health Information and Libraries Journal 26: 91–108. [DOI] [PubMed] [Google Scholar]
- Greenhalgh T, Shaw S.. 2017. Understanding heart failure; explaining telehealth–a hermeneutic systematic review. BMC Cardiovascular Disorders 17: 156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grundy J. 2015. Health Systems and Social Transition in Asia. Victoria, Australia: Deakin University. [Google Scholar]
- Ham C, Brommels M.. 1994. Health care reform in the Netherlands, Sweden, and the United Kingdom. Health. Health Affairs (Project Hope) 13: 106–119. [DOI] [PubMed] [Google Scholar]
- Harris B, Nxumalo N, Ataguba JE. et al. 2011. Social solidarity and civil servants’ willingness for financial cross-subsidization in South Africa: implications for health financing reform. Journal of Public Health Policy 32: S162–S183. [DOI] [PubMed] [Google Scholar]
- Hasnida A, Borst RA, Johnson AM. et al. 2017. Making health systems research work: time to shift funding to locally-led research in the South. The Lancet. Global Health 5: e22–e24. [DOI] [PubMed] [Google Scholar]
- Hetrick SE, Parker AG, Callahan P, Purcell R.. 2010. Evidence mapping: illustrating an emerging methodology to improve evidence‐based practice in youth mental health. Journal of Evaluation in Clinical Practice 16: 1025–1030. [DOI] [PubMed] [Google Scholar]
- Heyvaert M, Maes B, Onghena P.. 2013. Mixed methods research synthesis: definition, framework, and potential. Quality & Quantity 47: 659–676. [Google Scholar]
- Hoffman SJ, Røttingen J-A, Bennett S. et al. 2012. Background Paper on Conceptual Issues Related to Health Systems Research to Inform a WHO Global Strategy on Health Systems Research. Geneva, Switzerland: World Health Organization.
- Hofstede G. 1985. The interaction between national and organizational value systems. Journal of Management Studies 22: 347–357. [Google Scholar]
- HSG. 2018. Liverpool Statement for the Fifth Global Symposium on Health Systems Research. Health Systems Global. [Google Scholar]
- Kehoe SM, Ponting JR.. 2003. Value importance and value congruence as determinants of trust in health policy actors. Social Science & Medicine (1982) 57: 1065–1075. [DOI] [PubMed] [Google Scholar]
- Keren R, Littlejohns P.. 2012. Consideration of social values in the establishment of accountable care organizations in the USA. Journal of Health Organization and Management 26: 384–9. [DOI] [PubMed] [Google Scholar]
- Kieslich K. 2012. Social values and health priority setting in Germany. Journal of Health Organization and Management 26: 374–83. [DOI] [PubMed] [Google Scholar]
- Koduah A, Agyepong IA, van Dijk H.. 2018. Towards an explanatory framework for national level maternal health policy agenda item evolution in Ghana: an embedded case study. Health Research Policy and Systems 16: 76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kruk ME, Freedman LP, Anglin GA, Waldman RJ.. 2010. Rebuilding health systems to improve health and promote statebuilding in post-conflict countries: a theoretical framework and research agenda. Social Science & Medicine 70: 89–97. [DOI] [PubMed] [Google Scholar]
- Landwehr C, Klinnert D.. 2015. Value congruence in health care priority setting: social values, institutions and decisions in three countries. Health Economics, Policy, and Law 10: 113–32. [DOI] [PubMed] [Google Scholar]
- Langlois ÉV, Daniels K., Akl Ea. 2018. Evidence Synthesis for Health Policy and Systems: A Methods Guide. Geneva: World Health Organization. [PubMed] [Google Scholar]
- Lewin S, Glenton C.. 2018. Are we entering a new era for qualitative research? Using qualitative evidence to support guidance and guideline development by the World Health Organization. International Journal for Equity in Health 17: 126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewis CE. 1977. Health-services research and innovations in health-care delivery: does research make a difference? The New England Journal of Medicine 297: 423–427. [DOI] [PubMed] [Google Scholar]
- Littlejohns P, Sharma T, Jeong K.. 2012. a. Social values and health priority setting in England: “values” based decision making. Journal of Health Organization and Management 26: 363–73. [DOI] [PubMed] [Google Scholar]
- Littlejohns P, Weale A, Chalkidou K, Faden R, Teerawattananon Y.. 2012. b. Social values and health policy: a new international research programme. Journal of Health Organization and Management 26: 285–92. [DOI] [PubMed] [Google Scholar]
- Littlejohns P, Yeung K, Clark S, Weale A.. 2012. c. A proposal for a new social values research program and policy network. Journal of Health Organization and Management 26: 407–21. [DOI] [PubMed] [Google Scholar]
- Liverani M, Hawkins B, Parkhurst JO.. 2013. Political and institutional influences on the use of evidence in public health policy. A systematic review. PLoS One 8: e77404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- London L, Himonga C, Fick N, Stuttaford M.. 2015. Social solidarity and the right to health: essential elements for people-centred health systems. Health Policy and Planning 30: 938–945. [DOI] [PubMed] [Google Scholar]
- Mackintosh M, Koivusalo M.. 2005. Health systems and commercialization: in search of good sense Commercialization of Health Care. Springer, 3–21. [Google Scholar]
- MacQuilkan KE. 2016. The representation and practice of interdisciplinarity in Health Policy and Systems Research: a systematic review. School of Public Health University of Cape Town, Cape Town.
- Marchal B, Van Belle S, Hoerée T, De Brouwere V, Kegels G.. 2016. Complexity in Health: Consequences for Research & Evaluation, Management and Decision Making. Antwerp, Belgium: Institute of Tropical Health. [Google Scholar]
- McIntyre D, Gilson L, Wadee H, Thiede M, Okarafor O.. 2006. Commercialisation and extreme inequality in health: the policy challenges in South Africa. Journal of International Development 18: 435–446. [Google Scholar]
- Mechanic D. 1978. Prospects and problems in health services research. The Milbank Memorial Fund Quarterly. Health and Society 56: 127–139. [PubMed] [Google Scholar]
- Miake-Lye IM, Hempel S, Shanman R, Shekelle PG.. 2016. What is an evidence map? A systematic review of published evidence maps and their definitions, methods, and products. Systematic Reviews 5: 28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Minkov M, Hofstede G.. 2012. Is national culture a meaningful concept?: Cultural values delineate homogeneous national clusters of in-country regions. Cross-Cultural Research 46: 133–159. [Google Scholar]
- Mirzoev T, Kane S.. 2017. What is health systems responsiveness? Review of existing knowledge and proposed conceptual framework. BMJ Global Health 2: e000486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mostafavi H, Rashidian A, Arab M, Mahdavi MR, Ashtarian K.. 2016. Health priority setting in Iran: evaluating against the social values framework. Global Journal of Health Science 8: 53834. [DOI] [PubMed] [Google Scholar]
- Mou H. 2013. The political economy of the public–private mix in heath expenditure: an empirical review of thirteen OECD countries. Health Policy 113: 270–283. [DOI] [PubMed] [Google Scholar]
- Myers BA. 1973. Health services research and health policy: interactions. Medical Care 11: 352–358. [DOI] [PubMed] [Google Scholar]
- Nord E, Richardson J, Street A, Kuhse H, Singer P.. 1995. Who cares about cost? Does economic analysis impose or reflect social values? Health Policy (Amsterdam, Netherlands) 34: 79–94. [DOI] [PubMed] [Google Scholar]
- Olivier J, Scott V, Molosiwa D, Gilson L.. 2017. a. Embedded systems approaches to health policy and systems research In: De Savigny D, Blanchet K, Adam T (eds). Applied Systems Thinking for Health Systems Research: A Methodological Handbook. London, England: McGraw-Hill Education. [Google Scholar]
- Olivier J, Whyle E, Gilson L.. 2017. b. Embedded Health Policy and Systems Research: A Rapid Scoping Review. Geneva: Alliance for Health Policy and Systems Research, World Health Organisation.
- Pace R, Pluye P, Bartlett G. et al. 2012. Testing the reliability and efficiency of the pilot Mixed Methods Appraisal Tool (MMAT) for systematic mixed studies review. International Journal of Nursing Studies 49: 47–53. [DOI] [PubMed] [Google Scholar]
- Palmer N, Mills A.. 2003. Classical versus relational approaches to understanding controls on a contract with independent GPs in South Africa. Health Economics 12: 1005–1020. [DOI] [PubMed] [Google Scholar]
- Pearson M, Zwi AB, Buckley NA.. 2010. Prospective policy analysis: how an epistemic community informed policymaking on intentional self poisoning in Sri Lanka. Health Research Policy and Systems 8: 19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pratt B, Paul A, Hyder AA, Ali J.. 2017. Ethics of health policy and systems research: a scoping review of the literature. Health Policy and Planning 32: 890–910. [DOI] [PubMed] [Google Scholar]
- Prince R. 2017. Universal Health Coverage in the Global South: new models of healthcare and their implications for citizenship, solidarity, and the public good. Michael 2: 153–72.
- Randall NP, James KL.. 2012. The effectiveness of integrated farm management, organic farming and agri-environment schemes for conserving biodiversity in temperate Europe—a systematic map. Environmental Evidence 1: 4. [Google Scholar]
- Redden CJ. 1999. Rationing care in the community: engaging citizens in health care decision making. Journal of Health Politics, Policy and Law 24: 1363–89. [DOI] [PubMed] [Google Scholar]
- Reinhardt UE. 2003. Resisting US Social Ethics. Review of First Do No Harm by Terence Sullivan and Patricia Baranek. Health Affairs, Project HOPE-The People-to-People Health Foundation, Inc.
- Remme JH, Adam T, Becerra-Posada F. et al. 2010. Defining research to improve health systems. PLoS Medicine 7: e1001000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ridde V. 2008. Equity and health policy in Africa: using concept mapping in Moore (Burkina Faso). BMC Health Services Research 8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roberts M, Hsiao W, Berman P, Reich M.. 2003. Getting Health Reform Right: A Guide to Improving Performance and Equity. Oxford, UK: Oxford University Press. [Google Scholar]
- Roemer MI. 1988. Health system research and health system strategies in the United States. Health Systems Research in Action 12: 111–126. [Google Scholar]
- Rokeach M. 1974. Change and stability in American value systems, 1968–1971. Public Opinion Quarterly 38: 222–238. [Google Scholar]
- Rokeach M, Parker S.. 1970. Values as social indicators of poverty and race relations in America. The Annals of the American Academy of Political and Social Science 388: 97–111. [Google Scholar]
- Ruger JP. 2008. Ethics in American health 1: ethical approaches to health policy. American Journal of Public Health 98: 1751–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Russell J, Swinglehurst D, Greenhalgh T.. 2014. ‘ Cosmetic boob jobs’ or evidence-based breast surgery: an interpretive policy analysis of the rationing of ‘low value’ treatments in the English National Health Service. BMC Health Services Research 14: 413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sabik LM, Lie RK.. 2008. Priority setting in health care: lessons from the experiences of eight countries. International Journal for Equity in Health 7: 4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saltman RB, Bergman S-E.. 2005. Renovating the commons: Swedish health care reforms in perspective. Journal of Health Politics, Policy and Law 30: 253–276. [DOI] [PubMed] [Google Scholar]
- Schlesinger M. 2002. On values and democratic policy making: the deceptively fragile consensus around market-oriented medical care. Journal of Health Politics, Policy and Law 27: 889–925. [DOI] [PubMed] [Google Scholar]
- Shams L, Sari AA, Yazdani S.. 2016. Values in health policy—a concept analysis. International Journal of Health Policy and Management 5: 623–630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shankardass K, Muntaner C, Kokkinen L. et al. 2018. The implementation of health in all policies initiatives: a systems framework for government action. Health Research Policy and Systems 16: 26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sheikh K, George A, Gilson L.. 2014. a. People-centred science: strengthening the practice of health policy and systems research. Health Research Policy and Systems 12: 19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sheikh K, Gilson L, Agyepong IA. et al. 2011. Building the field of health policy and systems research: framing the questions. PLoS Medicine 8: e1001073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sheikh K, Ranson MK, Gilson L.. 2014. b. Explorations on people centredness in health systems. Health Policy and Planning 29: ii1–ii5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shiffman J. 2007. Generating political priority for maternal mortality reduction in 5 developing countries. American Journal of Public Health 97: 796–803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spates JL. 1983. The sociology of values. Annual Review of Sociology 9: 27–49. [Google Scholar]
- Stafinski T, Menon D, Marshall D, Caulfield T.. 2011. Societal values in the allocation of healthcare resources. The Patient: Patient-Centered Outcomes Research 4: 207–225. [DOI] [PubMed] [Google Scholar]
- Tantivess S, Pérez Velasco R, Yothasamut J. et al. 2012. Efficiency or equity: value judgments in coverage decisions in Thailand. Journal of Health Organization and Management 26: 331–342. [DOI] [PubMed] [Google Scholar]
- Tashobya CK, da Silveira VC, Ssengooba F. et al. 2014. Health systems performance assessment in low-income countries: learning from international experiences. Globalization and Health 10: 5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Teerawattananon Y, Russell S.. 2008. A difficult balancing act: policy actors’ perspectives on using economic evaluation to inform health-care coverage decisions under the Universal Health Insurance Coverage scheme in Thailand. Value in Health 11: S52–S60. [DOI] [PubMed] [Google Scholar]
- Topp SM, Scott K, Ruano AL, Daniels K.. 2018. Showcasing the Contribution of Social Sciences to Health Policy and Systems Research. International Journal for Equity in Health 17: 145 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Torrance H. 2017. Be careful what you wish for: data entanglements in qualitative research, policy, and neoliberal governance. In: Denzin NK, Giardina MD (eds). In: Qualitative Inquiry in Neoliberal Times. New York: Routledge, 81–92. [Google Scholar]
- Tricco AC, Antony J, Zarin W. et al. 2015. A scoping review of rapid review methods. BMC Medicine 13: 224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Olmen J, Criel B, Bhojani U. et al. 2012. a. The Health System Dynamics Framework: the introduction of an analytical model for health system analysis and its application to two case-studies. Health, Culture and Society 2: 1–21. [Google Scholar]
- van Olmen J, Criel B, Van Damme W. et al. 2010. Analysing Health Systems to Make Them Stronger. Antwerp, Belgium: ITGPress. [Google Scholar]
- van Olmen J, Marchal B, Van Damme W, Kegels G, Hill PS.. 2012. b. Health systems frameworks in their political context: framing divergent agendas. BMC Public Health 12: 774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walker L, Gilson L.. 2004. ‘ We are bitter but we are satisfied’: nurses as street-level bureaucrats in South Africa. Social Science & Medicine 59: 1251–61. [DOI] [PubMed] [Google Scholar]
- Walt G, Gilson L.. 1994. Reforming the health sector in developing countries: the central role of policy analysis. Health Policy and Planning 9: 353–370. [DOI] [PubMed] [Google Scholar]
- Watt N, Sigfrid L, Legido-Quigley H. et al. 2017. Health systems facilitators and barriers to the integration of HIV and chronic disease services: a systematic review. Health Policy and Planning 32: iv13–iv26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whitty JA, Littlejohns P.. 2015. Social values and health priority setting in Australia: an analysis applied to the context of health technology assessment. Health Policy (Amsterdam, Netherlands) 119: 127–36. [DOI] [PubMed] [Google Scholar]
- WHO. 2015. People-Centred and Integrated Health Services: An Overview of the Evidence: Interim Report. Geneva, Switzerland: World Health Organization. [Google Scholar]
- WHO. 2016. Framework on Integrated People-Centred Health Services: Report by the Secretariat. Geneva, Switzerland: World Health Organization. [Google Scholar]
- World Bank. 2019. World Bank Country and Lending Groups. The World Bank. [Google Scholar]
- Yao Q, Chen K, Yao L. et al. 2014. Scientometric trends and knowledge maps of global health systems research. Health Research Policy and Systems 12: 26. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.