

The world is facing challenging times. Coronavirus disease 2019 (COVID-19) is a global pandemic, and severe cases overwhelm medical centers around the world. Societies struggle to prevent the spread of the disease and effectively treat a rapidly rising number of patients while not neglecting other health and societal priorities.
This public health crisis has dramatically altered the delivery of preventive cardiology care and healthy lifestyle implementation. In the context of a changing landscape filled with immediate challenges, health interventions that provide long-term benefit may seem counterintuitive and be marginalized. However, continued efforts geared toward preventing cardiovascular disease (CVD) should not be discounted. Although COVID-19 is the most impending health emergency in most countries, CVD remains the leading cause of death around the world, accounting for 17.8 million deaths in 2017, and diabetes mellitus and obesity have also become pandemic.1 It is crucial to ensure that even during these trying times, our CVD-prevention efforts remain a top health, social, and policy priority.
We are learning that current social distancing restrictions may need to be extended for months, and renowned infectious disease experts believe that coronavirus outbreaks will become seasonal,2 meaning that long periods of staying at and working from home may become cyclic until effective vaccines become available. These phenomena, together with their implications for cardiovascular health, will require innovative efforts to adapt current CVD prevention approaches. Of note, COVID-19–related complications and death are more frequent among individuals with established CVD,3 and primary and secondary cardiovascular prevention efforts have direct implications for reducing the burden of current and future outbreaks.
One of the key implications of the current crisis in terms of CVD prevention is the fact that social distancing, staying at home, and telecommuting reduce exercise and mobility options, markedly decreasing levels of physical activity.4 Among the hundreds of millions who are required to stay at home, most activities are sedentary and screen time is skyrocketing. Recommendations by health authorities should include aggressive promotion of physical activity for the entire family, adherence to a healthy diet, and reduction of caloric intake to avoid weight gain. Despite physical distance, there are now opportunities to engage with others virtually for social support while doing exercise, such as group fitness classes, treadmill runs, and stationary cycling that can be connected online. Some governances still allow for exercising outdoors if safe social distancing is maintained. Mobile health devices, fitness-promoting games, and activity trackers can also be leveraged to promote activity. Also, with many smokers staying at home and having a hard time buying or using tobacco products, the momentum is optimal for widespread tobacco cessation counseling. The same is true for vaping.
Health technology was already becoming central to cardiology, but this novel context will boost further implementation. This is enhanced by expanded coverage of telemedicine for current and new patients by the Centers for Medicare and Medicaid Services, including audio-only visits that significantly widen its reach.5 Preventive cardiology visits are particularly well-suited for telemedicine because they rely heavily on clinical history, review of laboratory and imaging studies, and ambulatory blood pressure monitoring, with less of a need for physical examination. Telemedicine and remote monitoring will make it easier to frequently reach patients to optimize risk factor control, titrate medications, assess diets and physical activity levels, and integrate reminders to meet daily goals, among other capabilities.
Given their higher risk of complications, secondary prevention cardiovascular patients are at the center of social distancing measures, and their cardiologists need to ensure effective communication channels. An emphasis will have to be placed on adhering to cardiovascular medications, rehabilitation activities, and healthy lifestyles while isolated. Patients should also be advised to maintain adequate supplies of their chronic medications and instructed on how to refill prescriptions, potentially using mail-order pharmacies in the context of lockdowns and quarantines that impede ready access. Patients should invest in a home blood pressure monitor and a scale. They should be trained to self-evaluate and recognize concerning symptoms, monitor their vital signs and weight, report any abnormalities, and adjust medications. Overall, this new scenario will represent an invaluable opportunity to enhance patient empowerment and ownership in cardiovascular prevention, with less reliance on clinician authority.
Besides health implications, the economic effect of the COVID-19 pandemic will be enormous and preventive cardiologists will need to adapt to a landscape of potential economic recession, with some patients facing financial hardship. Care of these patients will need to be particularly sensitive to minimize financial toxicity through medication choices and an emphasis on inexpensive lifestyle changes. Coaching patients for stress management should also be integrated into routine preventive cardiology care.
From a research standpoint, enhanced incorporation of telemedicine and other technologies will generate very granular monitoring and patient trajectory data. Evaluation of the benefits of increased self-care and close e-health follow-up approaches will be key areas of cardiovascular outcomes research in the coming years. The same will be true for research on patient- and context-level determinants associated with adverse cardiovascular outcomes during lockdowns and on opportunities to improve these. Some patients will flourish, and others will decompensate. This pandemic will further enrich our understanding of the many factors that drive cardiovascular health, disease, and outcomes under various circumstances.
Despite the challenges that CVD prevention already faces in this unprecedented context, we believe there are good reasons for hope. As with all crises, novel opportunities and innovation arise (Figure). The overflow of COVID-19 health-related information has likely increased the general public’s awareness of the importance of CVD and its risk factors as powerful predictors of outcomes for both communicable and noncommunicable diseases. The COVID-19 pandemic has demonstrated the extraordinary actions that our societies can take when it comes to tackling urgent crises; in the coming years, we will need to use similar determination, resilience, and innovation to tackle the pandemics of obesity and diabetes mellitus, which will also overwhelm health systems and economies if we do not act promptly. Marked advances in telemedicine in the post–COVID-19 era will provide an opportunity to enhance the care of primary and secondary prevention patients, with implications not only for CVD outcomes but also for reducing the burden of complications and deaths in current and future viral outbreaks.
Figure.
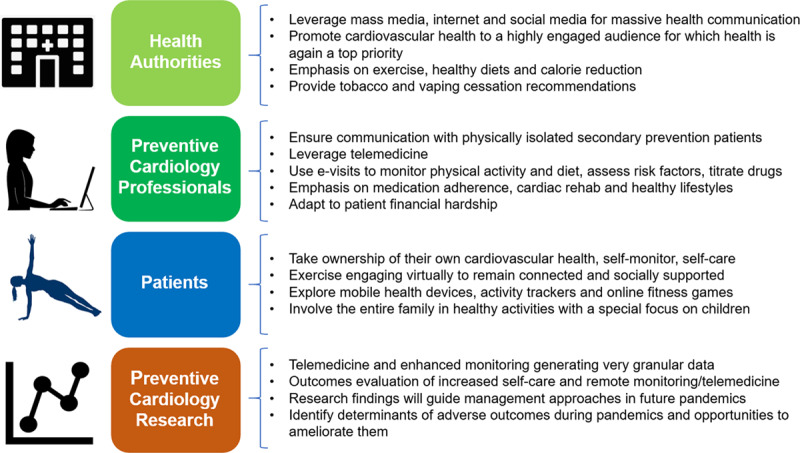
Novel opportunities and related roles for primary and secondary cardiovascular disease prevention during a coronavirus pandemic.
Disclosures
None.
Footnotes
The opinions expressed in this article are not necessarily those of the editors or of the American Heart Association.
References
- 1.Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Delling FN, et al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics–2020 update: a report from the American Heart Association. Circulation. 2020;141:e139–e596. doi: 10.1161/CIR.0000000000000757. doi: 10.1161/CIR.0000000000000757. [DOI] [PubMed] [Google Scholar]
- 2.Fauci AS, Lane HC, Redfield RR. Covid-19—navigating the uncharted. N Engl J Med. 2020;382:1268–1269. doi: 10.1056/NEJMe2002387. doi: 10.1056/NEJMe2002387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Yang J, Zheng Y, Gou X, Pu K, Chen Z, Guo Q, Ji R, Wang H, Wang Y, Zhou Y. Prevalence of comorbidities in the novel Wuhan coronavirus (COVID-19) infection: a systematic review and meta-analysis [published online March 12, 2020]. Int J Infect Dis. doi: 10.1016/j.ijid.2020.03.017. doi: 10.1016/j.ijid.2020.03.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Fitbit. The impact of coronavirus on global activity. Fitbit News. https://blog.fitbit.com/covid-19-global-activity/. Published March 23,2020. Accessed April 1, 2020. [Google Scholar]
- 5.Centers for Medicare and Medicaid Services. Additional background: sweeping regulatory changes to help U.S. healthcare system address COVID-19 patient surge. CMS.gov Newsroom. https://www.cms.gov/newsroom/fact-sheets/additional-backgroundsweeping-regulatory-changes-help-us-healthcare-system-address-covid-19-patient. Published March 30,2020. Accessed April 1, 2020.