

Abstract
Introduction
The Covid-19 pandemic triggered unprecedented nationwide regulations aimed primarily at slowing the spread of the virus. The objective of this study was to describe the effect of these regulations on the number and severity of trauma presentations to a regional emergency department in Kwa-Zulu Natal.
Methods
A retrospective cohort study of the triage register at Edendale Hospital Emergency Department was conducted, comparing all trauma presentations in the month of April 2020 with those from the preceding two years. The number of patients, mechanism of trauma and severity of illness were recorded and compared.
Results
A 47% reduction in the number of trauma cases was recorded for April 2020. The proportion of severe cases did not change. The categories showing a major decrease were motor vehicle accidents, pedestrian vehicle accidents, assault and gunshot wounds. The incidence of dog bite wounds and burns remained unchanged.
Conclusion
This study shows that the burden of trauma presenting to the emergency department was decreased in the month of April 2020 by the regulations implemented in response to the Covid-19 pandemic.
Keywords: Covid-19, Coronavirus, Trauma, Lockdown, Motor vehicle accidents, Interpersonal violence
African relevance
-
•
The study was conducted in a upper-middle income setting in Africa.
-
•
The results may be compared with other African settings where similar measures are implemented.
-
•
The reduction of trauma and interpersonal violence is an important agenda in multiple African areas.
Introduction
On the 27th March 2020 the South African government implemented a series of measures aimed at limiting the spread of the COVID-19 pandemic. These measures included restricting non-essential travel, prohibiting the sale of alcohol, closure of workplaces for non-essential services and restricting social gatherings.
These unique circumstances provided an opportunity to study the effect of these conditions on the burden of trauma presentations to a rural emergency department in Kwa-Zulu Natal, an area described as having a high trauma burden, particularly with regards to motor vehicle accidents, pedestrians injured by motor vehicles and interpersonal violence [1,2].
This study aims to describe the changes both in numbers and severity of trauma presentations to the emergency department at Edendale Hospital, Kwa-Zulu Natal during the time that the lockdown measures were applied.
These findings will serve as a record of this particular aspect of the pandemic, but they may also inform strategies for injury prevention in the area.
Methods
A retrospective cohort study was performed comparing the trauma presentations during the month of April 2020, during which the country was under level 5 lockdown regulations, with the month of April in the two preceding years, 2018 and 2019.
The setting was the emergency department at Edendale Hospital, a 900-bed regional hospital situated in a rural area on the outskirts of Pietermaritzburg, Kwa-Zulu Natal. The emergency department sees all trauma cases presenting to the hospital, including self-presentations, those brought by ambulance and referrals from clinics and district level facilities.
The study participants included all patients presenting to the emergency department with a traumatic mechanism as their chief complaint as captured by the triage register during the month of April 2018, 2019 and 2020. The triage register records a day by calendar date, from midnight at the beginning of the day to midnight again. The triage register was the only source of data used. No identifying details were recorded.
Permission to use the triage register data was obtained from the Edendale Hospital Research and Ethics Committee and approved as part of the BCA207/09 Class Approval by the UKZN BREC.
The data variables collected included the mechanism of trauma as well as the severity of illness, as defined by the South African Triage Score (SATS). The mechanisms were categorised by the most prevalent entries, including motor vehicle accident (MVA), pedestrian injured by motor vehicle (PVA), assault, gunshot wound, dog bite, burns and a category labelled “other”, which included various miscellaneous injury types. When one patient sustains multiple modes of trauma, e.g. burns and assault, it is at the discretion of the triage nurse to document the primary mode in the triage register, multiple modes are not routinely captured. The total number of patients presenting to the emergency department per month was also recorded, with the number of trauma patients compared to the total presentations being reflected as a percentage.
Data was captured in Microsoft® Excel (version 16, 2020) spreadsheets on a password protected laptop. Analysis was conducted in R (R Core Team, 2020) using the packages pastecs (Grosjean & Ibanez, 2018) for descriptive statistics, pgirmess (Giraudoux, 2018) for post-hoc tests and ggplot2 (Wickham, 2009), for figures.
The numbers of trauma cases are reflected as daily averages with standard deviations from the mean, with a box plot showing the extreme ranges, as often occur during public holidays.
For the various traumatic mechanisms defined, data are represented as categories with numerical totals. Kruskal-Wallis tests were used to determine the statistical significance of the variations observed. Injury severity was categorised as mild-moderate (yellow and green on the SATS) and severe (orange and red on the SATS). The proportion of severe cases was calculated for each month studied and these proportions were compared.
Results
A total of 2375 patients presented to the emergency department in April 2018. Of these, 1311 (55%) had trauma as their chief complaint. Two thousand six hundred and ninety five patients presented to the emergency department in April 2019. Of these, 1364 (51%) had trauma as their chief complaint. One thousand seven hundred and ninety eight patients presented to the emergency department in April 2020. Of these, 706 (39%) had trauma as their chief complaint. This represents a 47% reduction in the absolute number of trauma presentations in April 2020 compared to the average of the preceding two years.
The average daily numbers of trauma presentations are reflected in Fig. 1 below. Of note, the maximum numbers reflected by the “whiskers” of the plot occurred on the Saturday of the Easter weekend in 2018 and 2019. This surge in numbers was also significantly reduced in 2020.
Fig. 1.
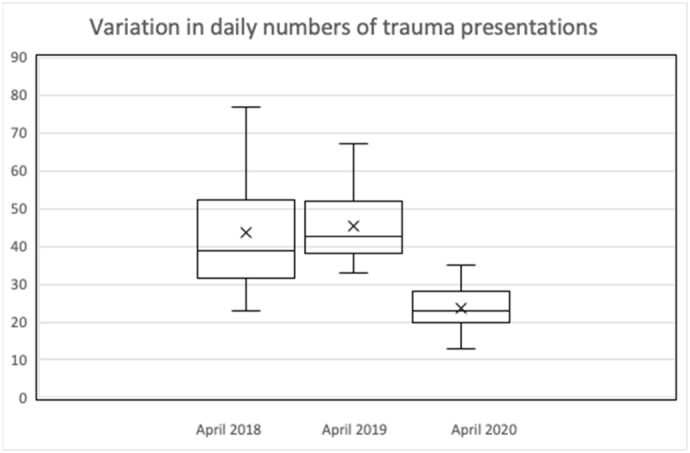
Boxplots showing the daily numbers of trauma presentations.
The severity of injuries is reflected in Table 1. The proportion of cases that were severe (orange and red triage scores by SATS) remained similar over the time periods studied.
Table 1.
Injury severity is divided into mild-moderate (SATS green and yellow) and severe (SATS orange and red).
| Injury severity as determined by triage score | |||
|---|---|---|---|
| April 2018 | April 2019 | April 2020 | |
| Mild-moderate | 1234 | 1300 | 671 |
| Severe | 77 | 64 | 35 |
| % severe | 5,87 | 4,69 | 4,96 |
The reductions in numbers in the categories MVA, PVA, Assault, and Gunshot wound, when comparing April 2018 and April 2019 to April 2020, were statistically significant (p < 0,05, Kruskal-Wallis test). The change in the categories Dog bite and Burns was not statistically significant for April 2020. The last category, Other, comprised of various injury types not included in the above categories, also showed a statistically significant decrease, with 550 cases in April 2018, 609 cases in April 2019 and 366 cases in April 2020 (p < 0,05). Examples of the types of entry in this category include “fall”, “laceration”, “bee sting” or “painful arm”.
Discussion
The level 5 lockdown measures implemented during April 2020 had a major impact on the number of trauma presentations (Fig. 2) to the emergency department, reducing the numbers by 47%. This reduction has anecdotally been described in several countries, although the data are not available at the time of writing this article. A 25% reduction in general Accident and Emergency presentations in England in the week following the implementation of their national lockdown was noted by Thornton [3]. Jenkins et al. reported a 23% reduction in the number of orthopaedic surgeries performed for trauma at his hospital in Glasgow in the week following the implementation of the lockdown measures [4].
Fig. 2.

The major categories of trauma studied over the three months.
If patients were avoiding hospital presentations due to fear or public health messages, we would expect that the proportion of mild-moderate injury severity would decrease in comparison to those with more severe injuries. The severity of presentation in our cohort did not differ significantly from previous years, suggesting that this difference in the number of trauma presentations should not be attributed to a reduction in health seeking behaviour alone.
It is important to note that at the time of data capture there were still no confirmed cases of Covid-19 at Edendale Hospital, despite testing according to the NICD criteria taking place. Thus, while the virus may have had psychological impacts on the community, there was not yet a significant burden of illness to explain these results.
The most significant reductions were seen in the categories MVA, PVA, assault and gunshot wounds. There was no significant difference to the incidence of dog bites and burns presenting to the hospital. Parkinson et al. described the high incidence of motor vehicle accidents and pedestrian vehicle accidents presenting to Edendale Hospital in 2013 [2]. They also commented on the self-reported high-risk behaviours at the time of accident in their series. These behaviours included speeding, alcohol consumption, overloading of vehicles and failure to wear seatbelts [2].
Our study did not document the presence of these high-risk behaviours, but the lockdown measures should have caused a reduction in the number of vehicles on the road, a decrease in alcohol consumption prior to driving and less overloading of vehicles. A more detailed study would be needed to determine the causation of each accident, but the reduction in numbers seen in our study suggests that the high number of motor vehicle accidents in this area can be reduced by the implementation of specific strategic measures. These may include increased police surveillance for drivers under the influence of alcohol or awareness campaigns about the risks of drinking and driving.
The reduction in interpersonal violence, including assault and gunshot wounds, also requires further investigation. Norman et al. reported that interpersonal violence is the second ranked cause of loss of Disability Adjusted Life Years (DALYs) in South Africa [5]. The underlying factors, including alcohol abuse, intimate partner violence, child abuse and various societal factors are described by Seedat et al., who also discuss strategies for the prevention of violence [6]. Although not the primary goal of the lockdown measures implemented in South Africa, the reduction in the incidence of interpersonal violence is clearly one of the positive results. This should provide motivation and encouragement to policy makers looking to sustain this reduction in interpersonal violence by showing that it is possible to reduce these numbers, while acknowledging that the measures in place to cause this reduction were severe. It is also not clear how sustained this reduction would have been should the level 5 lockdown have been implemented for a longer period of time.
Patients presenting with dog bites and burns continued unchanged, suggesting that the lockdown measures did not affect the incidence of these types of trauma.
A potential source of confounding is the nature of the triage register, which lists a single primary complaint only. Hence, a patient complaining primarily of a sore arm may well have been assaulted, causing this pain. This primary complaint (sore arm) would then be captured in the Other category rather than under Assault. This would lead to underreporting of the specified categories, such as Assault in this example.
The major limitation of this study is that, because several measures were implemented at the same time, we are unable to separate which of the measures had the most significant effect. While a reduction in the number of vehicles on the road may lead to a decrease in the incidence of road traffic accidents, a restriction in the sale of alcohol may also have contributed significantly to this statistic. Likewise, the reduction in the incidence of assault is likely to have been affected by alcohol restrictions, but this would also have been impacted by the restriction of public gatherings. The only clear conclusion that we can draw is that when these conditions are applied together there is a significant reduction in the burden of trauma. As the lockdown measures are eased there may be different combinations of circumstances that would allow the impact of specific conditions to be more clearly defined.
The results of this study should be compared with similar data from other settings to determine generalisability. Hardcastle et al. noted that even within Kwa-Zulu Natal there are regional differences in the incidence and type of trauma [7]. Whether the reductions in trauma incidence due to the lockdown measures was observed in other areas of South Africa would be of great interest and may further inform local trauma and public health services of the unique aspects of their population.
Conclusion
The implementation of the level 5 lockdown measures in response to the Covid-19 pandemic caused a 47% reduction in the number of patients presenting to Edendale Hospital Emergency Department with trauma. The major reductions were in the presentations of motor vehicle accidents, pedestrian vehicle accidents, assault and gunshot wounds. These results can be compared with other South African settings, and potentially with other phases of the lockdown, to determine potential injury prevention targets and strategies. They will also serve as a reminder of the unique and life-changing situation our country once faced.
Dissemination of results
The results of this study were shared with the clinicians at the study site through an informal presentation.
Authors' contribution
Authors contributed as follows to the conception or design of the work; the acquisition, analysis, or interpretation of data for the work; and drafting the work or revising it critically for important intellectual content: DM contributed 40%, ND contributed 30% AdP, NK and MR contributed 10% each. All authors approved the version to be published and agreed to be accountable for all aspects of the work.
Declaration of competing interest
The authors declared no conflicts of interest.
References
- 1.Moodley N.B., Clarke D.L. Current trauma patterns in Pietermaritzburg. South African J Surg. 2015;53:3–4. [PubMed] [Google Scholar]
- 2.Parkinson F., Kent S., Aldous C., Oosthuizen G., Clarke D. Road traffic crashes in South Africa: the burden of injury to a regional trauma centre. South African Med J. 2013;103(11):850–852. doi: 10.7196/samj.6914. [DOI] [PubMed] [Google Scholar]
- 3.Thornton J. Covid-19: A&E visits in England fall by 25% in week after lockdown. BMJ [Internet] 2020;369(April) doi: 10.1136/bmj.m1401. Available from. [DOI] [PubMed] [Google Scholar]
- 4.Jenkins P. The early effect of COVID-19 on trauma and elective orthopaedic surgery. Br Orthop Assoc. 2020 https://www.boa.ac.uk/policy-engagement/journal-of-trauma-orthopaedics/journal-of-trauma-orthopaedics-and-coronavirus/the-early-effect-of-covid-19-on-trauma-and-elect.html Internet. (April). Available from. [Google Scholar]
- 5.Norman R., Bradshaw D., Schneider M., Joubert J., Groenewald P., Lewin S. A comparative risk assessment for South Africa in 2000. South African Med J [Internet] 2007;97(8):637–641. http://www.samj.org.za/index.php/samj/article/view/654/151 Available from. [PubMed] [Google Scholar]
- 6.Seedat M., Van Niekerk A., Jewkes R., Suffla S., Ratele K. Violence and injuries in South Africa: prioritising an agenda for prevention. Lancet. 2009;374(9694):1011–1022. doi: 10.1016/S0140-6736(09)60948-X. [DOI] [PubMed] [Google Scholar]
- 7.Hardcastle T.C., Samuels C., Muckart D.J. An assessment of the hospital disease burden and the facilities for the in-hospital care of trauma in KwaZulu-Natal, South Africa. World J Surg. 2013;37(7):1550–1561. doi: 10.1007/s00268-012-1889-1. [DOI] [PubMed] [Google Scholar]