

Abstract
Background
Life satisfaction is part of subjective well-being. Measurement of life satisfaction is undertaken using self-report measures. This study aimed to evaluate the structural validity, concurrent validity, and internal structure of the PROMIS® General Life Satisfaction Scale (GLSS) in a musculoskeletal pain cohort.
Method
Consecutive new patients attending the Victoria University Osteopathy Clinic (Melbourne, Australia) were invited to complete the GLSS prior to their initial consultation. Structural validity and internal structure were explored using confirmatory factor analysis and Mokken scale analysis. Concurrent validity was evaluated against a single-item measure of life satisfaction.
Results
The PROMIS® GLSS comprised a single factor and formed an acceptable Mokken scale in this population. No differential item functioning was observed. A large positive correlation (r = 0.70) was observed between the General Life Satisfaction scale and a single-item measure of life satisfaction.
Conclusions
The PROMIS® General Life Satisfaction scale demonstrated acceptable internal structure and structural validity in a musculoskeletal pain population. Additional research is required to explore concurrent validity and other measurement properties, however initial data suggests the measure could be a feasible screen of life satisfaction for Australian osteopathic patients.
Keywords: Item response theory, Reliability estimation, Patient report outcome measure, Internal consistency, Osteopathic medicine, Osteopathy
Background
Subjective well-being is a broad psychological construct with satisfaction with life (SWL) being one of the sub-constructs [1]. The latter relates to the subjective cognitions and judgments we make about our lives [2]. People form judgments of how satisfied they are based on their perception of emotional experience, with the number of positive experiences having a greater impact on higher ratings of SWL than negative emotions [3]. High levels of SWL are positively associated with a range of physical and mental health issues and health behaviours [4–8].
As SWL has previously been linked to mental and physical health status, measurement of life satisfaction may assist with patient management. Measuring life satisfaction is undertaken through self-report measures. There are a range of life satisfaction measures published in the literature with reported validity and reliability [2, 9]. The most commonly utilised of these measures is the Satisfaction with Life Scale (SWLS) [2]. From a measurement perspective, a number of SWL measures have been shown to comprise a single dimension or construct [10–12]. Measurement variance of the SWLS has also been evaluated. Emerson, Guhn and Gadermann [12] suggest that gender has little systematic influence on responses to the SWLS items however, age and culture may result in differing interpretations and subsequent responses. The most recently developed SWL measure is the PROMIS® Short Form v1.0 - General Life Satisfaction 5a scale (1Dec2017) (GLSS).
The Patient–Reported Outcome Measurement Information System (PROMIS®) (www.nihpromis.org) has been developed by the National Institute of Health (NIH) to develop, validate, and standardize an array of patient-reported outcome measures [13]. The PROMIS collection of measures encompasses physical, social and mental domains of health identified by the World Health Organisation (WHO). To our knowledge the GLSS has not been used to investigate the life satisfaction of patients seeking care for musculoskeletal complaints and to date, there is little published on its measurement properties. The purpose of this study was to evaluate the construct validity of the structure of the GLSS in this population, following the Consensus-based Standards for the Selection of Health Measurement Instruments (COSMIN) guidelines [14].
Methods
Participants
Patients presenting for their initial consultation at a student-led osteopathy clinic were invited to participate in the study. The clinic is located on the Victoria University campus in the Melbourne central business district, and is a clinical training environment for osteopathy students completing the final 2 years of their five-year program. All new patients were invited to complete a demographic and health information form prior to their consultation between January 1 and June 30, 2018. Consent to participate was taken as having completed the questionnaire and not indicating to ‘opt-out’ of the study. Responses from patients under the age of 18 were excluded.
Measures
Patients completed a personal and health information questionnaire. This questionnaire was designed to collect information about a range of health behaviours and current health status consistent with data collected in Australian population health surveys [15]. Patients were also invited to complete two measures of life satisfaction. First was a single life satisfaction question How satisfied are you with your life? rated on an anchored Likert-type scale from 0 (not at all satisfied) to 5 representing (extremely satisfied) [16]. Single item SWL measures have been shown to be both reliable [17] and valid [18]. The second measure was the GLSS comprising five items rated on a 7-point Likert-type scale from 1 (Strongly disagree) to 7 (strongly agree).
Data analysis
Each new patient form and questionnaire was screened and relevant data (additional demographics and clinical information) extracted from the clinical history by a single author (BV) then de-identified. Data from each form was entered into SPSS (IBM Corp, USA) [19] for analysis then exported to Microsoft Excel. The GLSS was scored using the Health Measures Scoring Service (https://www.assessmentcenter.net/ac_scoringservice) and results entered into Excel. The Scoring Service generates a T-score, the total score for the measure converted to a standardised score. A score of 50 is the mean T-score for the American general population for the GLSS [20].
The R program [21] was used to perform the analyses. Data missing completely at random (MCAR) were imputed using the twoway function in the TestDataImputation [22] package prior to analysis. Descriptive statistics were generated for demographic variables using the psych package [23]. Multiple statistical approaches were used to evaluate the measurement properties of the GLSS: confirmatory factor analysis (CFA), reliability estimations, Mokken scale analysis and differential item function. Concurrent validity of the GLSS was evaluated by way of a correlation coefficient (Pearson’s r) with the single-item life satisfaction question.
Confirmatory factor analysis has been performed together with Mokken scaling in numerous studies [24–28]. Authors suggest the combination of these two approaches (classical test theory and modern test theory respectively) may provide complimentary measurement property data [24, 28] (for example dimensionality [25, 29]) and provide data that allows for comparison with other research [24, 30]. Boothroyd, Dagnan and Muncer [31] also suggest that “Mokken analysis can be used in a confirmatory way to check whether a proposed scale is acceptable” (p. 533). In the case of the current work the additional benefit of utilising both data analysis strategies was to provide measurement data in a population where the questionnaire has not been utilised.
Confirmatory factor analysis
Confirmatory factor analysis (CFA) was performed using the lavaan package [32]. Given the GLSS data are ordinal, the robust weighted least squares (WLSMV) estimation method was used [33]. Multiple CFA fit statistics were generated given the varied measurement properties of each fit statistic [34, 35] and the recommended cut values are described in Table 3.
Table 3.
Confirmatory factor analysis statistics PROMIS General Life Satisfaction 5a
| Statistic | Recommended value | Model |
|---|---|---|
| χ2 | NA | 33.77 |
| χ2 p-value | > 0.05 | < 0.01 |
| df | NA | 5 |
| χ2/df | < or = 2 | 6.75 |
| Comparative fit index (CFI) | > or = 0.9 | 0.998 |
| Tucker-Lewis index (TLI) | > or = 0.9 | 0.997 |
| Root mean square residual (SRMR) | As close to 0 as possible | 0.034 |
| Root mean square error of approximation (RMSEA) | < or = 0.08 |
0.118 (CI 0.083–0.158) |
Reliability estimations
Internal structure of the GLSS was also evaluated using McDonald’s omega total and hierarchal [36, 37], in addition to the ordinal Cronbach’s alpha [38] statistic. Confidence intervals (95%) were calculated for the omega total and alpha statistics. McDonald’s omega hierarchal values over 0.5 provide additional support for a total score calculation [39].
Mokken scale analysis
Mokken scaling analysis (MSA) is a non-parametric item response theory (IRT) statistical approach with scale construction for polytomous items based on four assumptions: the scale measures a single latent construct (unidimensionality); higher levels of the latent construct correspond with higher values selected for individual items (monotonicity); responses to one item should not be systematically influenced by responses to another item (local dependence) [40]; and, non-overlapping item characteristic curves (non-intersection) [41]. A Mokken scale is constructed when these assumptions are met.
The Mokken scale analysis was performed using the mokken package [42] and the following steps describe the analysis:
Evaluate items that may form Mokken scales using the automated item search function (aisp) [43]. Initial cut-off was set at 0.3 then retested at 0.5 increments until the scales could not be explained.
Calculation of the scalability coefficient(s) for all items creating a scale (H), the individual items (Hi), and item pairs (Hij). Interpreted as < 0.3 = ‘weak’, 0.4–0.5 = ‘moderate’, > 0.5 = ‘strong’.
Local dependence was evaluated with the conditional association procedure [44]. For locally dependent items, the item with the lower Hi value was removed and the data set reanalysed.
Graphical and numerical approaches were used to evaluate monotonicity to ensure that each item demonstrated item response functions that monotonically increased.
Invariant item ordering (HT) was then evaluated with values < 0.3 suggesting the items could not be meaningfully ordered, 0–3-0.4 the items may be meaningfully ordered, items of between 0.4–0.5 demonstrating moderate ordering, and items with HT greater than 0.5 demonstrating strong item ordering [45].
Once a scale had been finalised, Mokken’s rho was evaluated as a reliability estimation with a value over 0.7 being acceptable [46].
Differential item function
Differential item function (DIF) is used to explore whether a factor (i.e. age, gender) influences responses to an item or items on a measure in either a systematic (uniform) or non-systematic (non-uniform) manner [47]. Lack of DIF is a requirement to establish measurement invariance [47]. Age, gender, birthplace and stage of presenting complaint were the factors explored in the current work. Analysis of DIF was undertaken in the lordif package [48] using the likelihood ratio chi-square test and an alpha value of p < 0.01.
Results
Six hundred and thirty-two (N = 632) patients attended the clinic during the data collection period. Two hundred and twelve (n = 212, 33.5%) did not provide data or declined to participate, with nine (1.8%) additional patients excluded as they were under 18 years of age. No data was collected on non-participants. Data from 411 (65%) were available for analysis. Age, gender and clinical characteristics for the sample are in Table 1. Descriptive statistics for the GLSS are presented in Table 2. The single-item life satisfaction question mean was 3.92 (±0.83) and a median of 4 [IQR 4–4].
Table 1.
Demographic data for patients participating in the study
| Gender | |
| Male | 164 (39.9%) |
| Female | 247 (60.1%) |
| Age | |
| Mean (±SD) years | 33.47 (±13.2) |
| Range | 18–80 years |
| Median | 29 years |
| Stage | |
| Acute | 183 (44.5%) |
| Chronic | 227 (55.2%) |
| Region of presenting complaint | |
| Spine & pelvis | 238 (57.9%) |
| Upper extremity | 61 (14.8%) |
| Lower extremity | 98 (23.8%) |
Note: percentages that do not add to 100% represent missing data
Table 2.
Descriptive statistics and correlation for the PROMIS General Life Satisfaction 5a scale items and total score
| PROMIS item | Mean (SD) | Median [IQR] | Range | SWL correlation [95%CI] | Betaa | SE | p-value |
|---|---|---|---|---|---|---|---|
| PA045m. In most ways, my life is close to perfect | 4.92 (1.47) | 5 [4–6] | 1–7 | 0.64 [0.58, 0.69] | 0.81 | 0.02 | < 0.01 |
| PA046. If I could live my life over, I would change almost nothing | 4.90 (1.63) | 5 [4–6] | 1–7 | 0.53 [0.46, 0.60] | 0.93 | 0.01 | < 0.01 |
| PA047. I am satisfied with my life | 5.68 (1.22) | 6 [5–6] | 1–7 | 0.69 [0.63, 0.74] | 0.93 | 0.01 | < 0.01 |
| PA048. So far I have gotten the important things I want in life | 5.52 (1.30) | 6 [5–6] | 1–7 | 0.58 [0.51, 0.67] | 0.76 | 0.02 | < 0.01 |
| PA049m. My life situation is excellent | 5.53 (1.18) | 6 [5–6] | 1–7 | 0.65 [0.59, 0.70] | 0.85 | 0.01 | < 0.01 |
| Total score | 26.57 (5.82) | 28 [24–30] | 5–35 | 0.70 [0.65, 0.74] | |||
| T-score | 54.32 (8.90) | 55.20 [49.27–58.30] | 23.0–73.4 | 0.70 [0.65, 0.74] |
SWL single item satisfaction with life score, astandardised estimate, SE standard error
Confirmatory factor analysis fit statistics for the one factor model are presented in Table 3 and item statistics presented in Table 2. These results suggest a fit of the data to a one-factor model representing the latent construct of life satisfaction.
Results of the MSA suggest the GLSS forms a strong Mokken scale in the current population, with acceptable Hi coefficients, no monotonicity violation (Fig. 1) and low accuracy of item ordering (Table 4). Reliability estimations were also acceptable (Table 4). The results provide support for the GLSS being a unidimensional measure in this population. The sample size prevented further MSA to examine the internal structure of the GLSS for demographic variables such as gender. These were subsequently evaluated using a differential item function analysis. Variables were dichotomised for the DIF analysis: age (< 30 years/30 years or older), gender (male/female), stage (acute/chronic), and born in Australia (yes/no).
Fig. 1.
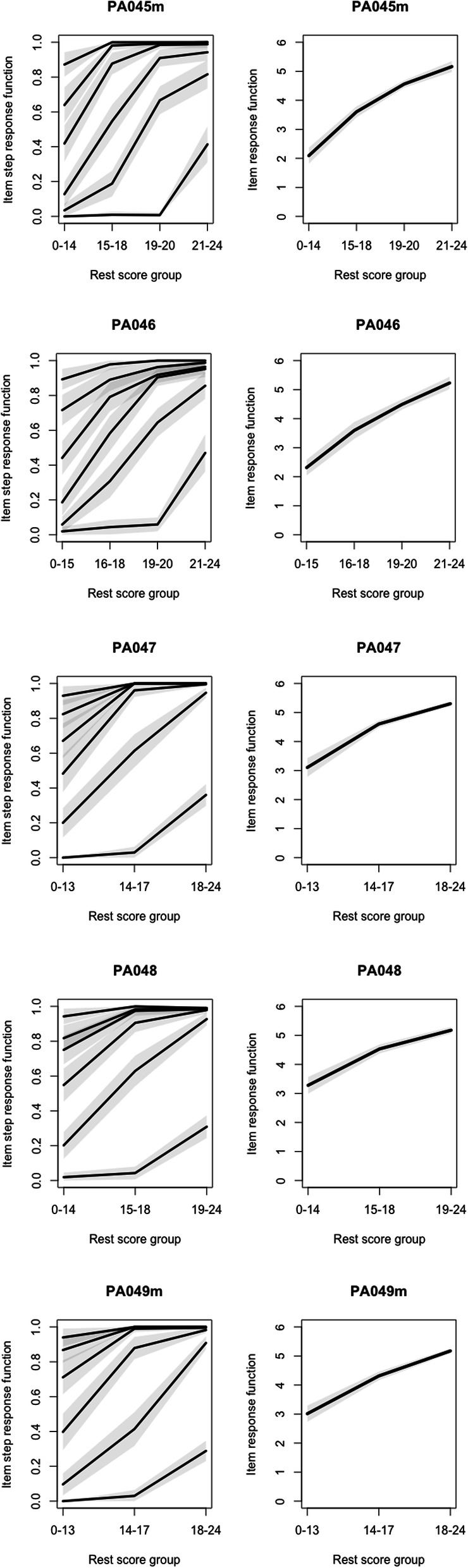
Graphical evaluation of PROMIS General Life Satisfaction 5a scale items
Table 4.
Mokken scaling coefficients and reliability estimations for each of the PROMIS General Life Satisfaction 5a items and scale
| Coefficient H | 0.700 (±0.031) |
| Item coefficients (Hi) | |
| In most ways, my life is close to perfect (PA045m) | 0.657 (±0.042) |
| If I could live my life over, I would change almost nothing (PA046) | 0.747 (±0.028) |
| I am satisfied with my life (PA047) | 0.748 (±0.031) |
| So far I have gotten the important things I want in life (PA048) | 0.633 (±0.038) |
| My life situation is excellent (PA049m) | 0.728 (±0.028) |
| Invariant item ordering (HT) | 0.37 |
| Mokken’s rho | 0.91 |
| Cronbach’s alpha (ordinal) | 0.91 [95%CI 0.90–0.93] |
| McDonald’s omega total (ordinal) | 0.91 [95%CI 0.90–0.93] |
| McDonald’s omega hierarchical (ordinal) | 0.91 |
Pearson’s r coefficient for the correlation between the GLSS T-score and single-item SWL measure was 0.70 (95%CI 0.65, 0.74]) suggesting a large correlation between the scores for each measure. Correlations between the individual items and the single-item SWL score were moderate to high (Table 2).
Discussion
The current study explored the construct validity of the PROMIS® General Life Satisfaction scale in a musculoskeletal pain population and identified the measure demonstrated acceptable measurement properties in this cohort. A further aim evaluated the concurrent validity of a single item life satisfaction question and the PROMIS General Life Satisfaction scale. The mean T-score was 54.32 (+/− 8.90) suggesting the average life satisfaction across the cohort is consistent with American general population data (the comparator when using PROMIS scales) [49]. At the time of writing, there was no Australian data using this measure, therefore it is not possible to draw comparisons. The PROMIS scales are anchored with a mean of 50, therefore the current population displays a slightly higher level of life satisfaction than the American general population.
Classical test theory (CTT), in this case CFA, was used to evaluate the construct validity of the GLSS. A number of CFA fit statistics support the presence of a single factor representing the latent construct of SWL, including the CFI, TLI and SRMR. These relative fit statistics are less affected by sample size compared to the chi-square test [50]. The other fit statistics were less positive in their support of the single factor. The chi-square test was statistically significant, meaning we accept that the one factor model fits perfectly. However, statistical significance may be due to the chi-square test being suited to more complex models compared with the one-factor model in the current work [50, 51]. Kenny [51] also suggests chi-square will always be statistically significantly with sample sizes greater than 400. The RMSEA value also suggests the one-factor model may not be ‘close-fitting’ however this is likely due to the calculation of this statistic relying on the degrees of freedom (df) and the aforementioned chi-square. Small df values result in greater sampling error and a resultant high RMSEA value [51]. Ordinal Cronbach’s alpha and McDonald’s omega reliability estimations also support the single factor. These results are consistent with other SWL research suggesting that many life satisfaction measures evaluate a single latent construct [10–12]. The current study is also the first to provide confirmatory factor analysis and reliability estimation data for the GLSS and offers a useful comparator for future research.
Mokken scale analysis (MTT) was utilised to evaluate the internal structure and dimensionality of the GLSS. This non-parametric item response theory approach suggests that the GLSS is unidimensional, with acceptable scale measurement properties. The unidimensional nature of the scale is further supported by the high McDonald’s omega hierarchal value [39, 52], with the coefficient suggesting that 91% of the variance of the GLSS T-Score is due to the general factor – life satisfaction. The other MSA results support the GLSS as meeting the requirements of the Mokken scale [53]. The ability to order the GLSS items (invariant item ordering), that is, the order of the items consistently reflects an increasing level of life satisfaction, does not appear possible. This suggests that some patients may report high levels of satisfaction with an item whereas for other items they will report it as low, even if their overall life satisfaction T-score is the same.
This work also provides additional evidence for the GLSS with respect to differential item function. Age and culture have been shown to influence responses to life satisfaction measures [10–12]. The current work did not identify DIF for age, gender, being born in Australia nor the stage of the presenting complaint. Lack of DIF for age may be a reflection of the younger population in the current work, and this study provides support for the notion that gender does not systematically influence SWL item responses. That said, typically only one of the groups in the DIF analysis reached the 200 per group sample size suggested by Scott, Fayers, Aaronson, Bottomley, de Graeff, Groenvold, Gundy, Koller, Petersen and Sprangers [54] to achieve approximately 80% power. Further, we chose not to explore DIF for region of complaint as Bonferroni-adjusted p-values would likely require more than 500 responses in each complaint group [54] which is prohibitive in the current work.
A large positive correlation was observed between the single-item SWL question and the GLSS scores supporting the criterion validity of the measures. These two measures exhibit a shared variance of approximately 50% suggesting significant overlap in construct measurement. Similar shared variances have been described in studies exploring the Satisfaction with Life Scale and single item SWL measures [18, 55]. Although single item measures are widely used in large scale studies, Diamantopoulos, Sarstedt, Fuchs, Wilczynski and Kaiser [56] suggest that they only be used in small scale studies (less than 50 participants) and that multi-item measures will perform more appropriately where larger samples are used. This work by Diamantopoulos, Sarstedt, Fuchs, Wilczynski and Kaiser [56] was based on simulation data so further work in real populations is required. Our work highlights the need for additional work on the concurrent validity of the GLSS, particularly with other multi-item life satisfaction measures.
There are several limitations in the current work. The study used a consecutive sampling design. As such non-response, acquiescence and social desirability biases [57] may influence responses to the GLSS. Non-response was an issue as one-third of patients presenting during the study did not complete the measure. This may have been a result of all participants attending as new patients, with other data being collected on the same health demographics form. Using the GLSS in isolation for returning patients or with only a small number of other measures may have resulted in a higher response rate. The study was undertaken in a student-led clinical teaching environment and the patient cohort may not be reflective of those who present for musculoskeletal care in other manual therapy clinical environments in Australia.
Conclusion
The present study has provided evidence to support the internal structure and dimensionality of the GLSS in a population seeking musculoskeletal care. The study also provided some evidence to support the use of a single-item SWL question, although this question may not capture the breadth of the construct. The GLSS demonstrates elements of construct and criterion validity that support its utility as a measure of life satisfaction in Australian musculoskeletal care populations. Further research is now required to evaluate other aspects of reliability, validity and responsiveness of the GLSS and also evaluate the measure in other Australian clinical populations.
Acknowledgements
Not applicable.
Authors’ contributions
BV, JM and KF were responsible for the design of the study. All authors developed the Introduction. BV undertook the data analysis. All authors contributed to the development of the discussion. All authors approved the final version of the manuscript.
Funding
Not applicable.
Availability of data and materials
The datasets generated during and/or analysed during the current study are available in the figshare repository, 10.26188/5e97cb9a362e7.
Ethics approval and consent to participate
Ethics approval was provided by the Victoria University Human Research Ethics Committee (HRE15–005). Consent to participate was implied by the return of a completed questionnaire(s).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Diener E, Heintzelman SJ, Kushlev K, Tay L, Wirtz D, Lutes LD, Oishi S. Findings all psychologists should know from the new science on subjective well-being. Can Psychol Rev. 2017;58:87–104. [Google Scholar]
- 2.Diener E, Emmons RA, Larsen RJ, Griffin S. Satisfaction with life scale. J Pers Assess. 1985;49:71–75. doi: 10.1207/s15327752jpa4901_13. [DOI] [PubMed] [Google Scholar]
- 3.Diener E, Kuppens P, Realo A. The role of positive and negative emotions in life satisfaction judgment across nations. J Pers Soc Psychol. 2008;95:66–75. doi: 10.1037/0022-3514.95.1.66. [DOI] [PubMed] [Google Scholar]
- 4.Boehm JK, Peterson C, Kivimaki M, Kubzansky L. A prospective study of positive psychological well-being and coronary heart disease. Health Psychol. 2011;30:259–267. doi: 10.1037/a0023124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.St. John PD, Mackenze C, Menec V. Does life satisfaction predict five-year mortality in community-living older adults? Aging Ment Health. 2015;19:363–370. doi: 10.1080/13607863.2014.938602. [DOI] [PubMed] [Google Scholar]
- 6.Ruiz-Párraga GT, López-Martínez A. The contribution of posttraumatic stress symptoms to chronic pain adjustment. Health Psychol. 2014;33:958–967. doi: 10.1037/hea0000040. [DOI] [PubMed] [Google Scholar]
- 7.Grant N, Wardle J, Steptoe A. The relationship between life satisfaction and health behavior: a cross-cultural analysis of young adults. Int J Behav Med. 2009;16:259–268. doi: 10.1007/s12529-009-9032-x. [DOI] [PubMed] [Google Scholar]
- 8.Baumann M, Tchicaya A, Lorentz N, Le Bihan E. Life satisfaction and longitudinal changes in physical activity, diabetes and obesity among patients with cardiovascular diseases. BMC Public Health. 2017;17:925. doi: 10.1186/s12889-017-4925-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lucas RE, Diener E, Eunkook MS. Discriminant validity of well-being measures. J Pers Soc Psychol. 1996;71:616–628. doi: 10.1037//0022-3514.71.3.616. [DOI] [PubMed] [Google Scholar]
- 10.Pavot W, Diener E. Review of the satisfaction with life scale. In: Diener E, editor. Assessing well-being. Netherlands: Springer; 2009. pp. 101–117. [Google Scholar]
- 11.Gilman R, Huebner ES. Review of life satisfaction measures for adolescents. Behav Chang. 2000;17:178–195. [Google Scholar]
- 12.Emerson SD, Guhn M, Gadermann AM. Measurement invariance of the satisfaction with life scale: reviewing three decades of research. Qual Life Res. 2017;26:2251–2264. doi: 10.1007/s11136-017-1552-2. [DOI] [PubMed] [Google Scholar]
- 13.Cella D, Yount S, Rothrock N, Gershon R, Cook K, Reeve B, Ader D, Fries JF, Bruce B, Rose M, et al. The patient-reported outcomes measurement information system (PROMIS): progress of an NIH roadmap cooperative group during its first two years. Med Care. 2007;45:S3–S11. doi: 10.1097/01.mlr.0000258615.42478.55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Consensus-based standards for the selection of health measurement instruments. COSMIN taxonomy of measurement properties. 2010. https://www.cosmin.nl/tools/cosmin-taxonomy-measurement-properties/. Accessed 20 Aug 2019.
- 15.Australian Bureau of Statistics. National health survey: first results, 2014–15. Canberra, Australia; 2017. http://www.abs.gov.au/ausstats/abs@.nsf/Lookup/by%20Subject/4364.0.55.001~2014-15~Main%20Features~Self-assessed%20health%20status~6.
- 16.Mulcahy JC. Meaningful daily activity and chronic pain. Melbourne: Victoria University; 2011. [Google Scholar]
- 17.Lucas RE, Donnellan BM. Estimating the reliability of single-item life satisfaction measures: results from four national panel studies. Soc Indic Res. 2012;105:323–331. doi: 10.1007/s11205-011-9783-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Cheung F, Lucas RE. Assessing the validity of single-item life satisfaction measures: results from three large samples. Qual Life Res. 2014;23:2809–2818. doi: 10.1007/s11136-014-0726-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Vaughan B, Mulcahy J, Fitzgerald K. Data from PROMIS general life satisfaction scale. Fighshare. 2020. doi: 10.26188/5e97cb9a362e7. [DOI] [PMC free article] [PubMed]
- 20.HealthMeasures. PROMIS® reference populations. 2019. http://www.healthmeasures.net/score-and-interpret/interpret-scores/promis/reference-populations. Accessed 12 Oct 2019.
- 21.R Core Team . R: A language and environment for statistical computing. 2019. [Google Scholar]
- 22.Dai S, Wang X, Svetina D. TestDataImputation: missing item responses imputation for test and assessment data. Version 1.1. 2019. [Google Scholar]
- 23.Revelle W. psych: Procedures for personality and psychological research. Version 1.9.7. 2019. [Google Scholar]
- 24.Nader IW, Tran US, Baranyai P, Voracek M. Investigating dimensionality of Eskin's attitudes toward suicide scale with Mokken scaling and confirmatory factor analysis. Arch Suicide Res. 2012;16:226–237. doi: 10.1080/13811118.2012.695271. [DOI] [PubMed] [Google Scholar]
- 25.Emons WHM, Sijtsma K, Pedersen SS. Dimensionality of the hospital anxiety and depression scale (HADS) in cardiac patients: comparison of Mokken scale analysis and factor analysis. Assessment. 2012;19:337–353. doi: 10.1177/1073191110384951. [DOI] [PubMed] [Google Scholar]
- 26.Lee C-P, Chou Y-H, Liu C-Y, Hung C-I. Dimensionality of the Chinese hospital anxiety depression scale in psychiatric outpatients: Mokken scale and factor analyses. Int J Psychiatry Clin Pract. 2017;21:283–291. doi: 10.1080/13651501.2017.1311350. [DOI] [PubMed] [Google Scholar]
- 27.Abberger B, Haschke A, Krense C, Wirtz M, Bengel J, Baumeister H. The calibrated, unidimensional anxiety item bank for cardiovascular patients provided the basis for anxiety assessment in cardiovascular rehabilitation patients. J Clin Epidemiol. 2013;66:919–927. doi: 10.1016/j.jclinepi.2012.08.009. [DOI] [PubMed] [Google Scholar]
- 28.Lee C-P, Fu T-S, Liu C-Y, Hung C-I. Psychometric evaluation of the Oswestry disability index in patients with chronic low back pain: factor and Mokken analyses. Health Qual Life Outcomes. 2017;15:192. doi: 10.1186/s12955-017-0768-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Nielsen MG, Ørnbøl E, Vestergaard M, Bech P, Larsen FB, Lasgaard M, Christensen KS. The construct validity of the perceived stress scale. J Psychosom Res. 2016;84:22–30. doi: 10.1016/j.jpsychores.2016.03.009. [DOI] [PubMed] [Google Scholar]
- 30.Friedrich O, Sipötz J, Benzer W, Kunschitz E, Höfer S. The dimensional structure of the MacNew health related quality of life questionnaire: a Mokken scale analysis. J Psychosom Res. 2015;79:43–48. doi: 10.1016/j.jpsychores.2015.04.007. [DOI] [PubMed] [Google Scholar]
- 31.Boothroyd L, Dagnan D, Muncer S. PHQ-9: one factor or two? Psychiatry Res. 2019;271:532–534. doi: 10.1016/j.psychres.2018.12.048. [DOI] [PubMed] [Google Scholar]
- 32.Rosseel Y. Lavaan: an R package for structural equation modeling. J Stat Softw. 2012;48:1–36. [Google Scholar]
- 33.Muthén B, Du Toit SH, Spisic D. Robust inference using weighted least squares and quadratic estimating equations in latent variable modeling with categorical and continuous outcomes. Psychometrika. 1997;75:1–45. [Google Scholar]
- 34.DiStefano C, Hess B. Using confirmatory factor analysis for construct validation: an empirical review. J Psychoeduc Assess. 2005;23:225–241. [Google Scholar]
- 35.Jackson DL, Gillaspy JA, Jr, Purc-Stephenson R. Reporting practices in confirmatory factor analysis: an overview and some recommendations. Psychol Methods. 2009;14:6. doi: 10.1037/a0014694. [DOI] [PubMed] [Google Scholar]
- 36.Revelle W, Zinbarg RE. Coefficients alpha, beta, omega, and the glb: comments on Sijtsma. Psychometrika. 2009;74:145–154. [Google Scholar]
- 37.Dunn TJ, Baguley T, Brunsden V. From alpha to omega: a practical solution to the pervasive problem of internal consistency estimation. Br J Psychol. 2014;105:399–412. doi: 10.1111/bjop.12046. [DOI] [PubMed] [Google Scholar]
- 38.Zumbo BD, Gadermann AM, Zeisser C. Ordinal versions of coefficients alpha and theta for Likert rating scales. J Mod Appl Stat Methods. 2007;6:4. [Google Scholar]
- 39.Revelle W. Hierarchical cluster analysis and the internal structure of tests. Multivar Behav Res. 1979;14:57–74. doi: 10.1207/s15327906mbr1401_4. [DOI] [PubMed] [Google Scholar]
- 40.Stochl J, Jones PB, Croudace TJ. Mokken scale analysis of mental health and well-being questionnaire item responses: a non-parametric IRT method in empirical research for applied health researchers. BMC Med Res Methodol. 2012;12:1–16. doi: 10.1186/1471-2288-12-74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Vaughan B, Grace S. A Mokken scale analysis of the peer physical examination questionnaire. Chiro Man Thera. 2018;26:6. doi: 10.1186/s12998-018-0176-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Van der Ark LA. New developments in Mokken scale analysis in R. J Stat Softw. 2012;48:1–27. [Google Scholar]
- 43.Sitjtsma K, Van der Ark LA. A tutorial on how to do a Mokken scale analysis on your test and questionnaire data. Br J Math Stat Psychol. 2017;70:137–158. doi: 10.1111/bmsp.12078. [DOI] [PubMed] [Google Scholar]
- 44.Straat JH, Van der Ark LA, Sitjtsma K. Using conditional association to identify locally independent item sets. Methodology. 2016;12:117–123. [Google Scholar]
- 45.Ligtvoet R, Van der Ark LA, te Marvelde JM, Sijtsma K. Investigating an invariant item ordering for polytomously scored items. Educ Psychol Meas. 2010;70:578–595. [Google Scholar]
- 46.Sitjtsma K, Molenaar IW. Reliability of test scores in nonparametric item response theory. Psychometrika. 1987;52:79–97. [Google Scholar]
- 47.Hagquist C, Andrich D. Recent advances in analysis of differential item functioning in health research using the Rasch model. Health Qual Life Outcomes. 2017;15:181. doi: 10.1186/s12955-017-0755-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Choi SW, Gibbons LE, Crane PK. Lordif: an R package for detecting differential item functioning using iterative hybrid ordinal logistic regression/item response theory and Monte Carlo simulations. J Stat Softw. 2011;39:1. doi: 10.18637/jss.v039.i08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Siahpush M, Spittal M, Singh GK. Happiness and life satisfaction prospectively predict self-rated health, physical health, and the presence of limiting, long-term health conditions. Am J Health Promot. 2008;23:18–26. doi: 10.4278/ajhp.061023137. [DOI] [PubMed] [Google Scholar]
- 50.Sun J. Assessing goodness of fit in confirmatory factor analysis. Meas Eval Couns Dev. 2005;37:240–256. [Google Scholar]
- 51.Kenny D. Measuring model fit. 2015. [Google Scholar]
- 52.Reise SP. The rediscovery of bifactor measurement models. Multivar Behav Res. 2012;47:667–696. doi: 10.1080/00273171.2012.715555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Wind SA. An instructional module on Mokken scale analysis. Educ Measure. 2018;36:50–66. [Google Scholar]
- 54.Scott NW, Fayers PM, Aaronson NK, Bottomley A, de Graeff A, Groenvold M, Gundy C, Koller M, Petersen MA, Sprangers MAG. A simulation study provided sample size guidance for differential item functioning (DIF) studies using short scales. J Clin Epidemiol. 2009;62:288–295. doi: 10.1016/j.jclinepi.2008.06.003. [DOI] [PubMed] [Google Scholar]
- 55.Jovanović V. The validity of the satisfaction with life scale in adolescents and a comparison with single-item life satisfaction measures: a preliminary study. Qual Life Res. 2016;25:3173–3180. doi: 10.1007/s11136-016-1331-5. [DOI] [PubMed] [Google Scholar]
- 56.Diamantopoulos A, Sarstedt M, Fuchs C, Wilczynski P, Kaiser S. Guidelines for choosing between multi-item and single-item scales for construct measurement: a predictive validity perspective. J Acad Mark Sci. 2012;40:434–449. [Google Scholar]
- 57.Sedgwick P. Bias in observational study designs: cross sectional studies. Br Med J. 2015;350:h1286. doi: 10.1136/bmj.h1286. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets generated during and/or analysed during the current study are available in the figshare repository, 10.26188/5e97cb9a362e7.