

Abstract
Background:
According to the World Health Organization in 2009, hypertension is responsible for 13% of all deaths. Hypertension can increase the risk of stroke, coronary artery disease, dementia, heart disorder, kidney, and other chronic diseases. In this study, the prevalence and incidence of hypertension and knowledge and awareness of it among adults in Ahvaz are investigated.
Methods:
This cohort study was carried out on 688 participants in a study on the prevalence of metabolic syndrome investigated in adults in the city of Ahvaz in 2009. In 2014, participants were again recruited. Based on the standard method and disease history, blood pressure, height, and weight were measured, and a demographic information questionnaire was completed through interviews.
Results:
In this study, 688 individuals over 20 years of age participated with an average age of 42.7 ± 13.3 years, 300 men (43.6%), and 388 women (56.4%). Hypertension incidence was 65/1000 person-years which included 67.7 and 57.8/1000 person-years in men and women, respectively. The awareness of patients about hypertension was 51.2% in phase 2 (hypertension new cases).
Conclusions:
In this study conducted in Ahvaz, the incidence rate of hypertension was 65/1000 person-years, higher in men than women. Hypertension awareness was 50.5%, 45.1% in men, and 55.1% in women.
Keywords: Awareness, cohort studies, hypertension, incidence
Introduction
Hypertension has been known as a common cause of deaths and chronic diseases in most countries, especially Western countries.[1] More than 360 thousand deaths in 2013 in America were due to primary or secondary hypertension (about 1000 deaths daily).[2]
Hypertension is also one of the main causes of premature death worldwide, is associated with about 9.4 million deaths every year, and is still expanding. From among all the regions of the World Health Organization, Africa with 46% and America with 35% had the highest and lowest prevalence, respectively.[3] Hypertension constitutes about 13% of all deaths and is the strongest risk factor for hurting the individuals' healthy lifestyle.[4] It also increases the risk of stroke, coronary artery disease, heart and kidney failure, and other chronic diseases.[5,6,7]
Several studies have investigated the prevalence of hypertension around the world.[8,9] Furthermore, in Iran, some studies have been carried out which revealed that 22.2% of people over 15 years of age in Isfahan are suffering from hypertension.[10] Moreover, lipid and glucose study in 20–69 years old patients in Tehran showed that 22% are suffering from hypertension.[11] The prevalence of hypertension in rural populations is 18.4%[12] and in adults in the city of Ahvaz is 17.58%, 46.4% of them being aware of their hypertension condition.[13]
Few studies have been conducted on the incidence of hypertension. In previous studies, depending on age, gender, ethnicity and body size, the incidence of hypertension has been reported in the range of 3%–18%.[14] In a cohort study in Portugal with a median time of 3.8 years from 1999 to 2003, the incidence of hypertension was 47.3/1000 person-years.[15] Furthermore, in the study conducted in Kashan (Iran), (2013), the incidence of hypertension was 50/1000 adult person-years.[16] The aim of this study was to investigate the incidence and the level of awareness of hypertension, among people over 20 in Ahvaz in a 5-year cohort study from 2009 to 2014.
Methods
In this cohort study, participants were selected from individuals who participated in a cross-sectional study on the prevalence of metabolic syndrome in adults, which was carried out in Ahvaz in 2009.[17] Out of 24 health centers, six centers were selected by stratified random sampling. After obtaining written consent from the participant, they were invited to the centers with prior coordination. Blood pressure, height, and weight were measured and demographic information obtained through a questionnaire. Nine hundred and forty-four individuals participated in the baseline study, 166 of whom having been diagnosed with hypertension and 90 were unavailable or refused to continue, and finally, 688 people were reexamined 5 years later [Figure 1].
Figure 1.
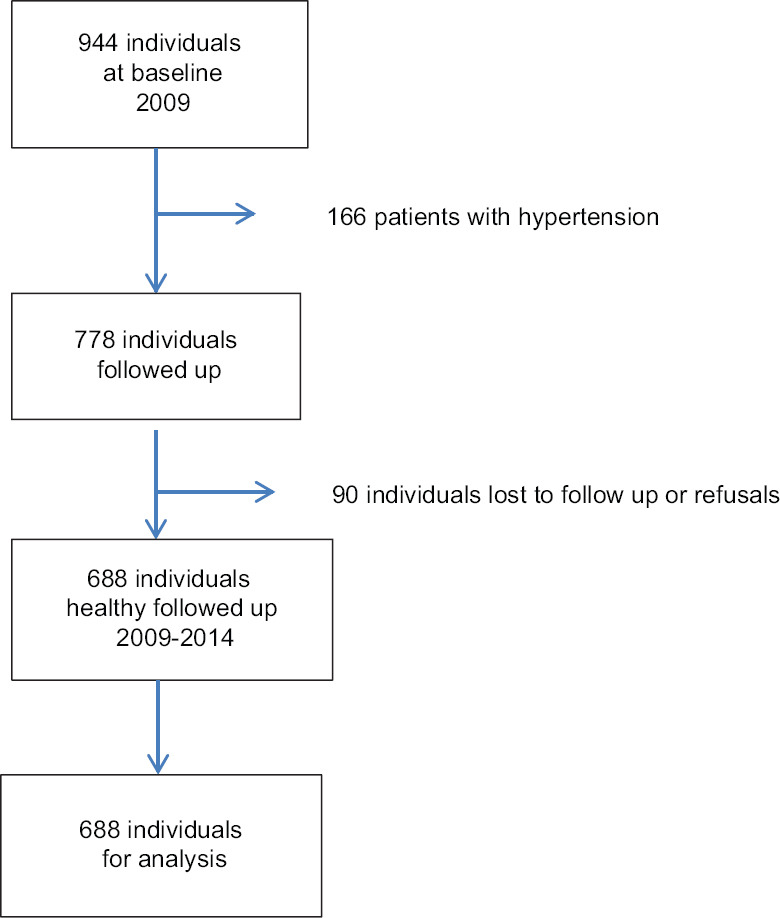
Flowchart illustrating the sample selection for the present analysis
Obesity was calculated based on body mass index (BMI) by dividing weight in kilograms to the square of height in meters. A BMI range of 25–29.99 was considered overweight, ≥30, obese and <25 normal
At least 15 min after rest, systolic blood pressure (SBP) and diastolic blood pressure (DBP) from the right arm (in suspended posture) were measured twice within 30 min in a seated position with Mercury manometers and putting Stethoscope under cuff. Mean twice measurement was recorded as the BP. To record BP Korotkoff sounds in phases one and five, preferably with the stethoscope bell was heard and blood pressure numbers in the first and fifth phases of Korotkoff recorded as systolic and DBP, respectively
According to the American diabetes association, hypertension is defined as (SBP ≥140/DBP ≥90 mmHg) or taking BP medication (on therapy)[18]
Family history of hypertension: hypertension in at least one first-degree relative
Waist circumference (WC) abnormal: WC ≥102 in men and WC ≥88 cm in women.
The collected data were entered into IBM SPSS statistical sowftwer (version 20, SPSS Inc., Chicago, IL, USA), and the data were analyzed using paired t-test, independent t-test, ANOVA, Chi-square, and logistic regression. P < 0.05 was considered statistically significant.
Results
A total of 688 healthy individuals over 20 years of age including 300 men (43.6%) and 388 women (56.4%) with an average age of 42.7 ± 13.3 years participated in this study. The cumulative incidence of hypertension was 26.8% that is equal to 65/1000 person-years (67.7 in men and 57.8 in women). The awareness in Phase 2 among adult patients in Ahvaz was 50.5% (male 45.1% and female 55.1%). Awareness of hypertension in the age groups of 20–39 was 35%, 40–59, 59%, and ≥60 years 76.1%, with increasing with age. 18.3% of people who reported having high blood pressure did not take medication.
A detailed comparison of systolic and diastolic, mean blood pressure, and incidence of hypertension are shown in Tables 1 and 2.
Table 1.
Comparison of systolic and diastolic mean blood pressure in people without hypertension in baseline study between phases 1 and 2 in terms of demographic variables
| Variable | SBP | P | DBP | P | ||
|---|---|---|---|---|---|---|
| Phase 1 | Phase 2 | Phase 1 | Phase 2 | |||
| Sex | ||||||
| Male | 114±11 | 116.6±14.5 | 0.03 | 71.5±5 | 73.0±10 | 0.18 |
| Female | 110±11 | 114.6±16.2 | <0.001 | 67.7±10 | 69.4±15.2 | 0.11 |
| P | <0.001 | 0.02 | <0.001 | 0.004 | ||
| BMI | ||||||
| <25 | 111±11.1 | 112.9±13.3 | 0.12 | 67.9±10.7 | 68.6±13.2 | 0.07 |
| 25.29-29.99 | 112.6±11.1 | 116±15.7 | 0.012 | 70.6±9.6 | 72.6±15.2 | 0.16 |
| ≥30 | 112.6±11.5 | 118.6±16.9 | <0.001 | 69.9±10.1 | 73.5±16.8 | 0.68 |
| P | 0.29 | <0.001 | 0.046 | 0.002 | ||
| Age | ||||||
| 20-29 | 109.8±10.2 | 109.7±11.0 | 0.89 | 67.6±10.3 | 67.2±14.5 | 0.79 |
| 30-39 | 109.9±11.8 | 110.2±12.2 | 0.86 | 68.3±9.8 | 68.7±13.1 | 0.77 |
| 40-49 | 112.2±11.2 | 116.5±15.2 | 0.006 | 69.2±10.2 | 71.5±17.3 | 0.13 |
| 50-59 | 114.9±11.2 | 124.7±17.9 | <0.001 | 72±10.1 | 75.1±16.1 | 0.08 |
| 60-69 | 118.2±8.6 | 122.8±13.8 | 0.18 | 72.6±9.5 | 78.7±12.4 | 0.07 |
| ≥70 | 116.0±10.7 | 124.0±17.1 | 0.8 | 75±8.5 | 75.0±12.7 | 0.99 |
| P | <0.001 | <0.001 | 0.004 | 0.006 | ||
| Married | ||||||
| No | 112±9.1 | 108.6±10.5 | 0.049 | 69.5±8.5 | 67.6±13.7 | 0.34 |
| Yes | 112.1±11.5 | 116.6±15.7 | <0.001 | 69.5±10.4 | 71.5±15.6 | 0.012 |
| P | 0.98 | <0.001 | 0.97 | 0.036 | ||
| Ethnicity | ||||||
| Arab | 111.1±11.5 | 113.8±14.8 | 0.049 | 69±10.0 | 68.9±13.8 | 0.34 |
| Fars | 113.2±11.3 | 119.2±17.1 | <0.001 | 70.1±9.6 | 74.7±16.1 | 0.012 |
| P | 0.04 | <0.001 | 0.22 | <0.001 | ||
| Family history of hypertension | ||||||
| No | 112.3±10.7 | 115.0±15 | 0.004 | 69.5±10.1 | 70.8±15.8 | 0.17 |
| Yes | 111.6±12.4 | 117.5±15.9 | <0.001 | 69.2±10.5 | 72.6±14.1 | 0.008 |
| P | 0.46 | 0.022 | 0.10 | 0.06 | ||
| WC | ||||||
| Normal | 115.85±15.9 | 115.4±15.8 | 0.99 | 71.67±11.37 | 70.8±15.8 | 0.17 |
| Unmoral | 120.0±16.50 | 120.0±16.5 | 0.27 | 72.32±13.3 | 72.6±14.1 | 0.008 |
| P | 0.027 | 0.003 | 0.58 | 0.06 | ||
WC=Waist circumference, SBP=Systolic blood pressure, DBP=Diastolic blood pressure, BMI=Body mass index
Table 2.
Incidence of hypertension in healthy people in baseline study and odds ratio in terms of demographic variables
| Cumulative incidence | OR 95% CI | |
|---|---|---|
| Sex | ||
| Male | 29 | 1 |
| Female | 25.3 | 1.15 (0.71-1.87) |
| P | 0.27 | |
| BMI | ||
| <25 | 18.1 | 1 |
| 25-29.99 | 25.7 | 1.4 (0.79-2.5) |
| ≥30 | 32.8 | 1.88 (1.01-3.5) |
| P | 0.013 | |
| Age | ||
| 20-29 | 1 | 13.2 |
| 30-39 | 9.8 | 0.49 (0.2-1.19) |
| 40-49 | 24.6 | 1.27 (0.59-2.76) |
| 50-59 | 44.1 | 3.1 (1.41-6.8) |
| 60-69 | 58.1 | 4.86 (1.78-13.2) |
| ≥70 | 32.6 | 5.25 (1.11-24.7) |
| P | <0.001 | |
| Married | ||
| No | 11.3 | 1 |
| Yes | 28.3 | 1.24 (0.48-3.23) |
| P | 0.013 | |
| Ethnicity | ||
| Arab | 18.9 | 1 |
| Fars | 32.7 | 1.75 (1.08-2.82) |
| P | <0.001 | |
| Family history of hypertension | ||
| No | 24 | 1 |
| Yes | 34.6 | 1.8 (1.8-2.9) |
| P | <0.001 | |
| Smoking | ||
| No | 27.3 | 1 |
| Yes | 24.4 | 0.69 (0.26-1.78) |
| P | <0.001 | |
| Diabetes mellitus | ||
| No | 22.7 | 1 |
| Yes | 47.7 | 2.23 (1.17-4.26) |
| P | <0.001 |
OR=Odds ratio, BMI=Body mass index, CI=Confidence interval
Discussion
This cohort study was carried out on people over 20 years of age in Ahvaz in Southwestern Iran in the 5-year period from 2009 to 2014. The cumulative incidence of hypertension was 26.8% (65/1000 person-years). The average SBP increased from 112.1 ± 11.2 to 115.6 ± 15.4 mmHg and DBP from 69.5 ± 10.1 to 71.1 ± 15.4 mm Hg in people without hypertension in baseline; this perceptible increase may be due to the participants' rising age, weight, or lifestyle change.
In phase 2, there was an increase in mean DBP In married individuals, the Fars ethnicity, and those with a family history of hypertension.
SBP also increased in both genders, overweight and obese individuals, ages 40–60 years old, Arab and Fars, with and without family history.
In baseline population, 46.4% of the patients were aware of their hypertension;[13] this awareness Increased to 50.5% in phase 2 among adult patients in Ahvaz without hypertension in baseline. The awareness results in different studies were as follows: Tehran (50%),[12] Saudi Arabia (44.7%),[9] India (33% in 2007 and 42.9% in 2010),[19] England (65%, 2006),[20] USA (81%, 2007–2010),[21] and Canada (83%, 2007–2009),[22] all of which are higher than Ahvaz. In phase 2, however, the awareness level in Ahvaz was more than that of Saudi Arabia and India, while lower than Iran (Tehran), England, USA, and Canada. This study shows the awareness of hypertension to be 43.8% in males and 53.3% in females in Ahvaz. Awareness of hypertension in this study increases with age, similar to the results of studies in Britain, The United States, and Canada.[23]
In participant with higher age 45 years in cohort study in the adult population of the city of Halle/Saale in eastern Germany, the awareness of hypertension was 69% in men and 80.9% women[24] that higher than in Ahvaz (male 45.1% and female 55.1%).
The prevalence of hypertension in adult who have reported their hypertension in Tehran (2011) was 5.27% (6.64% in women and 3. 83% of men) and the annual incidence was 6.87/1000 person-years (8.43 in women and 5.26 in men), which is much lower than results of nonself-report studies[25] due to lack of awareness.
The cumulative incidence of hypertension in Ahvaz was 26.8% (65/1000 person-years) which is considerably higher than that of Portugal (47.3/1000 person-years),[15] Canada (22.1/1000 person-years)[26] and India (23.6/1000 person-years)[19] but lower than Indian study (80.5/1000 person-years) (with 2 years follow-up),[27] and also lower than the Thai open university students study (the overall 4 years incidence of hypertension was 3.5%, also lower than Ahvaz).[28]
The incidence of hypertension in men and women in Ahvaz was 67.7and 57.8/1000 person-years respectively, which is similar to the results obtained in Canada (men 22.7 > 21.6 women per 1000 person-years), Portugal (men 52.7 > 43.4 women per 1000 person-years),[15] India men 93.1 > 70.9 women per 1000 person-years,[27] and the Thai study male 5.2% >2.1% female.[28]
There was a significant relationship between the incidence of hypertension and BMI, age, family history of hypertension, and ethnicity. In Thai Open University students study hypertension was associated with age, higher BMI, and comorbidities.[28] Furthermore, the risk of hypertension in >50 age group was at least three times higher than 20–29 age groups. A study in the city of Kerala in India showed that the risk of hypertension in people over 35 years of age was four times higher than people below 35.[19] In another India study, the risk for developing hypertension was associated with age, low socioeconomic status, current alcohol use, being overweight, prehypertension, and dysglycemia. Awareness of hypertension in women is more than men.
Conclusions
The incidence of hypertension was reported 65/1000 person-years and with higher rate in men compared to women in Ahvaz. The level of awareness was 50.5% among adult patients without hypertension in baseline, with awareness in women greater than men. Awareness of hypertension in Ahvaz increases with age.
Financial support and sponsorship
Nill.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Perkovic V, Huxley R, Wu Y, Prabhakaran D, Macmahon S. The burden of blood pressure related disease: Analysis of worldwide data. Lancet. 2005;365:217. doi: 10.1161/HYPERTENSIONAHA.107.095497. [DOI] [PubMed] [Google Scholar]
- 2.Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, et al. Heart disease and stroke-2015 Update: A report from the American Heart Association. Circulation. 2015;131:e29–322. doi: 10.1161/CIR.0000000000000152. [DOI] [PubMed] [Google Scholar]
- 3.World Health Organization. Global Health Observatory (GHO) Data 2013 World Health Organization-Global Health Risks, Mortality and Burden of Disease Attributable to Selected Major Risks. Geneva (Swaziland): The Organization; 2009. pp. 1–62. [Google Scholar]
- 4.MacMahon S, Peto R, Cutler J, Collins R, Sorlie P, Neaton J, et al. Blood pressure, stroke, and coronary heart disease. Part 1, prolonged differences in blood pressure: Prospective observational studies corrected for the regression dilution bias. Lancet. 1990;335:765–74. doi: 10.1016/0140-6736(90)90878-9. [DOI] [PubMed] [Google Scholar]
- 5.Jafar TH, Stark PC, Schmid CH, Landa M, Maschio G, de Jong PE, et al. Progression of chronic kidney disease: The role of blood pressure control, proteinuria, and angiotensin-converting enzyme inhibition: A patient-level meta-analysis. Ann Intern Med. 2003;139:244–52. doi: 10.7326/0003-4819-139-4-200308190-00006. [DOI] [PubMed] [Google Scholar]
- 6.Tozawa M, Iseki K, Iseki C, Kinjo K, Ikemiya Y, Takishita S, et al. Blood pressure predicts risk of developing end-stage renal disease in men and women. Hypertension. 2003;41:1341–5. doi: 10.1161/01.HYP.0000069699.92349.8C. [DOI] [PubMed] [Google Scholar]
- 7.Frieden TR. CentersCenters for Disease control and prevention (CDC) Health, States Table No 53. USA: US Government Printing Office; 2015. [Google Scholar]
- 8.Saeed AA, Al-Hamdan NA, Bahnassy AA, Abdalla AM, Abbas MA, Abuzaid LZ, et al. Prevalence, awareness, treatment, and control of hypertension among Saudi adult population: A National survey. Int J Hypertens. 2011;2011:174135. doi: 10.4061/2011/174135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Nutuli ST, Malmela E, Alberts M, Choma S, Dikotope S. Prevalence and Associated Risk Factors of Hypertension Amongst Adults in a Rural Community of Limpopo Province South Africa. [Last accessed on 2020 Apr 27]. Available from: http://wwwphcfmorg . [DOI] [PMC free article] [PubMed]
- 10.Meraci M, Feizi A, Nejad MB. Investigating the prevalence of high blood pressure, Type 2 diabetes mellitus and related risk factors according to a large general study in Isfahan-using multivariate logistic regression model. Health System Res. 2012;8:193–203. [Google Scholar]
- 11.Azizi F, Ghanbarian A, Madjid M, Rahmani M. Distribution of blood pressure and prevalence of hypertension in Tehran adult population: Tehran lipid and glucose study (TLGS), 1999-2000. J Hum Hypertens. 2002;16:305–12. doi: 10.1038/sj.jhh.1001399. [DOI] [PubMed] [Google Scholar]
- 12.Chaman R, Yunesian M, Hajimohamadi A, Gholami Taramsari M. Investigating hypertension prevalence and some of its influential factors in an ethnically variant rural sample. J Knowl Health. 2008;3:39–42. [Google Scholar]
- 13.Yazdanpanah L, Shahbazian H, Shahbazian H, Latifi SM. Prevalence, awareness and risk factors of hypertension in southwest of Iran. J Renal Inj Prev. 2015;4:51–6. doi: 10.12861/jrip.2015.11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hajjar I, Kotchen JM, Kotchen TA. Hypertension: Trends in prevalence, incidence, and control. Annu Rev Public Health. 2006;27:465–90. doi: 10.1146/annurev.publhealth.27.021405.102132. [DOI] [PubMed] [Google Scholar]
- 15.Pereira M, Lunet N, Paulo C, Severo M, Azevedo A, Barros H. Incidence of hypertension in a prospective cohort study of adult from Porto, Portugal. BMC Cardiovasc Disord. 2012;12:114. doi: 10.1186/1471-2261-12-114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Adib-Hajbaghery M, Lotfi MS, Rezaee-Shahsavarloo Z, Sadat Mousavi M. The incidence of hypertension and the follow-up rate in a sample of population over 30 years old in Kashan 2013. J Caring Sci. 2014;3:211–9. doi: 10.5681/jcs.2014.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Shahbazian H, Latifi SM, Jalali MT, Shahbazian H, Amani R, Nikhoo A, et al. Metabolic syndrome and its correlated factors in an urban population in South West of Iran. J Diabetes Metab Disord. 2013;12:11. doi: 10.1186/2251-6581-12-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Standards of Medical Care in Diabetes-2013. [Last accessed on 2020 Apr 27];Diabetes Care. 2013 36:511–66. Available from: http://wwwmayocliniccom . [Google Scholar]
- 19.Sathish T, Kannan S, Sarma PS, Razum O, Thankappan KR. Incidence of hypertension and its risk factors in rural Kerala, India: A community-based cohort study? Public Health. 2012;126:25–32. doi: 10.1016/j.puhe.2011.11.002. doi: 10.1016/j.puhe.2011.11.002. Epub 2011 Nov 30. [DOI] [PubMed] [Google Scholar]
- 20.Craig R, Mindell J, editors. Health Survey for England 2006. London, UK: The Information Centre; 2008. [Google Scholar]
- 21.CDC National Health and Nutrition Examination Survey Data. Hyattsville, MD: US Department of Health and Human Services, CDC; 2010. [Last accessed on 2020 Apr 27]. Available from: http://wwwcdcgov/nchs/nhanes/about_nhaneshtm . [Google Scholar]
- 22.The Canadian Health Measures Survey: Rationale Background and Overview. [Last accessed on 2020 Apr 27]. Available from: http://wwwstatcangcca/pub/82–003-s/82–003-s2007000-enghtm . [PubMed]
- 23.Joffres M, Falaschetti E, Gillespie C, Robitaille C, Loustalot F, Poulter N, et al. Hypertension prevalence, awareness, treatment and control in national surveys from England, the USA and Canada, and correlation with stroke and ischaemic heart disease mortality: A cross-sectional study. BMJ Open. 2013;3:e003423. doi: 10.1136/bmjopen-2013-003423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Lacruz ME, Kluttig A, Hartwig S, Löer M, Tiller D, Greiser KH, et al. Prevalence and incidence of hypertension in the general adult population: Results of the CARLA-cohort study. Medicine (Baltimore) 2015;94:e952. doi: 10.1097/MD.0000000000000952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Cheraghin B, Asadi-Lari M, Mansournia MA. Prevalence and associated factors of self-reported hypertension among Tehran adults in 2011: A population-based study (Urban HEART-2) Med J Islamic Republ Iran (MJIRI) 2014;28:105. [PMC free article] [PubMed] [Google Scholar]
- 26.American Diabetes Association. Standards of Medical Care in Diabetes-2013. Diabetes Care. 2013;36(Suppl 1):S11–S66. doi: 10.2337/dc13-S011. Published online 2012 Dec 10. doi: 10.2337/dc13-S011. PMCID: PMC3537269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Prabhakaran D, Jeemon P, Ghosh S, Shivashankar R, Ajay VS, Kendal D, et al. Prevalence and incidence of hypertension: Results from a representative cohort of over 16,000 adults in three cities of South Asia. Indian Heart J. 2017;69:434–41. doi: 10.1016/j.ihj.2017.05.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Thawornchaisit P, de Looze F, Reid CM, Seubsman SA, Sleigh AC. Health risk factors and the incidence of hypertension: 4-year prospective findings from a national cohort of 60 569 Thai Open University students? BMJ Open. 2013;3:e002826. doi: 10.1136/bmjopen-2013-002826. doi:10.1136/ bmjopen-2013-002826. [DOI] [PMC free article] [PubMed] [Google Scholar]