

Abstract
OBJECTIVES:
To determine if racial and ethnic subgroups of adolescents are at high risk for engagement in suicidal behaviors.
METHODS:
Using the nationally representative school-based Youth Risk Behavior Survey from the years 1991 to 2017, we conducted logistic regression analyses to examine trends by different racial and ethnic groups, with each suicide indicator serving as a dichotomous outcome. Participants included 198 540 high school students.
RESULTS:
Across all sex and race and ethnic groups, there were significant linear decreases in self-reported suicidal ideation and suicide plans from 1991 to 2017. Female adolescents (odds ratio [OR], 0.98; P < .001) had significant decreases in attempts over time. Black adolescents had positive linear trends for suicide attempts among both boys (OR, 1.04; P < .001) and girls (OR, 1.02; P = .003). Black adolescent boys (OR, 1.04; P = .048) had a significant linear increase in injury by attempt.
CONCLUSIONS:
The results suggest that, over time, black youth have experienced an increase in suicide attempts, which is troubling because attempts are the most prominent risk factor associated with suicide death. For black boys, a significant increase in injury by attempt occurred, which suggests that black boys may be engaging in increasingly lethal means when attempting suicide. Examining trends of suicidal thoughts and behaviors over time by sex and race and ethnicity allow us to determine where to focus prevention and intervention efforts. Future research should examine the underlying reasons for these changes observed in US high school students.
Suicide is the second leading cause of death in youth 12 to 18 years old, and in 2017, it accounted for >2200 deaths for this age group.1 Childhood maltreatment, mental health concerns (eg, depression), neurocognitive functioning deficits, and other risk factors have all been associated with suicide attempts, suicidal ideation, and suicide deaths.2–5 In recent studies, a racial disparity in suicide rates has been discovered. Black children, particularly black boys 5 to 11 years of age, have experienced an increase in the rate of suicide deaths; and in black children ages 5 to 12 years, the suicide rate was found to be 2 times higher compared with their white counterparts.6–8
A sex disparity in youth suicidal behavior has also been observed. Girls, compared with their male counterparts, are more likely to attempt suicide and have suicidal ideation, and boys are more likely to die by suicide.9 However, authors of recent studies have shown that the suicide rate in young girls is increasing, and the gap in suicide deaths between the sexes may be decreasing in youth ages 10 to 19 years.10–12
When examining suicide rates in youth ages 10 to 19 years, disparities are also present by race and sex.1 Non-Hispanic American Indian or Alaskan native (AI/AN) boys and girls (2017 rates = 26.22 per 100 000; 12.21 per 100 000, respectively) have the highest rate of suicide. These rates are followed by non-Hispanic white boys and girls (2017 rates = 13.19 per 100 000; 3.87 per 100 000, respectively), non-Hispanic black boys and girls (2017 rates = 7.33 per 100 000; 2.65 per 100 000, respectively), then Hispanic boys and girls (2017 rates = 7.24 per 100 000; 2.84 per 100 000, respectively). Non-Hispanic Asian American or Pacific Islander (PI) youth have the lowest suicide rate in the United States (boys = 6.74 per 100 000; girls = 3.63 per 100 000).1
The most robust risk factor associated with suicide death is a suicide attempt.9,10 A suicide attempt is a self-inflicted action or behavior with explicit or inferred intent to die.3,11–13 In 2017 in the United States, >111 000 youth 12 to 18 years old were seen in an emergency department for self-harm behavior.14 Yet, to our knowledge, racial and ethnic differences in youth suicidal ideation and suicide attempts have primarily been examined cross-sectionally, and longitudinal reports of these behaviors have been limited.15
The purpose of this study was to investigate racial and ethnic and sex differences in suicidal ideation and behavior over time in a nationally representative sample of high school students. Understanding if disparities are present in suicidal ideation and behavior and if changes have occurred over an extended period of time could inform prevention efforts and contribute to the development of new intervention programs that reduce the likelihood of suicide in this age group.
METHODS
Data and Participants
The Centers for Disease Control and Prevention (CDC) developed the Youth Risk Behavior Survey (YRBS) to monitor priority health-risk behaviors among youth in the United States.16 The national school-based YRBS is a cross-sectional survey conducted every 2 years since 1991. Each survey cycle uses a 3-stage cluster sampling design to produce a nationally representative sample of ninth- through 12th-grade students attending public and private schools in the 50 states and the District of Columbia. CDC investigators applied a weighting factor to adjust for nonresponse and the oversampling of black and Hispanic or Latino students. The Institutional Review Board at the CDC approved the protocol of national YRBS.16
Student participation in the survey is anonymous and voluntary through a self-administered computer-scannable questionnaire. A parent or legal guardian provides permission for youth to complete the survey. During 1991–2017, national YRBS sample sizes ranged from 10 904 to 16 410. School response rates ranged from 75% to 81%; student response rates ranged from 81% to 90%, and overall response rates for the surveys ranged from 60% to 71%. More details regarding sampling strategies and the psychometric properties of the YRBS questionnaire are reported elsewhere.17 The analytic sample in this study consisted of 198 540 adolescents (without missing values on sex and race and ethnicity) from the combined national YRBS data set from the years 1991 through 2017.
Measures
The YRBS asked 2 self-report questions about race and Hispanic heritage. Consistent with previous research,18 the 6 categories for race and ethnicity were non-Hispanic white, non-Hispanic black, non-Hispanic Asian or PI, Hispanic, American Indian/Alaska Native (AI/AN), and non-Hispanic multiple races. Native Hawaiian or other Pacific Islander is collapsed into Asian American or PI.
Four questions assessed suicidal thoughts and behaviors: (1) “During the past 12 months, did you ever seriously consider attempting suicide?” (suicide ideation), (2) “During the past 12 months, did you make a plan about how you would attempt suicide?” (suicide plan), (3) “During the past 12 months, how many times did you actually attempt suicide?” (suicide attempts; any response ≥1 was considered a “yes” response), and (4) “Did any attempt result in an injury, poisoning, or overdose that had to be treated by a doctor or nurse?” (injury by attempt). Response options were dichotomized into “yes” or “no.” These questions demonstrated substantial reliability in previous studies.19
Statistical Analysis
Logistic regression analyses were used to assess trends by different sex and racial and ethnic groups, with each of the 4 suicidal behavior questions serving as dichotomous outcomes. Survey year was treated as a continuous variable and was used to examine the linear trend. Quadratic terms over and above the standardized linear terms of survey year were used to examine the quadratic trend of responses. Secular trends in the prevalence of suicidal ideation, suicide plan, suicide attempts, and injury by attempt were examined by using multivariate logistic regression models that included linear time variables and then both linear and nonlinear (quadratic) time variables while controlling for the grade levels. Student grade levels were controlled to limit the effects of age. Trends that include significant quadratic and linear components demonstrated nonlinear variation in addition to an overall increase or decrease over time. Regression odds ratios (ORs), as well as 95% confidence intervals (CIs), were reported. Statistical significance was set to P < .05 with Wald χ2 tests using design-adjusted coefficient variance-covariance matrices. Statistical significance was set at 2-sided α = .05. Trends analyses were conducted by using “SURVERYLOGISTIC” process in SAS software version 9.4 (SAS Institute, Inc, Cary, NC) to adjust for the complex sampling design. The national YRBS data are weighted to the sample size. Thus, there is no need for additional adjustments to the weights.20 Both linear and nonlinear (quadratic) time variables were estimated while controlling for grade levels to explore nonlinear trends of suicidal behaviors across time, which was also suggested by previous literature.21 Linear trend is depicted with a straight line, whereas a quadratic trend is depicted with a curve with 1 bend. A significant quadratic trend indicates a nonlinear change in the data over time. Trends with both significant quadratic and linear components reveal nonlinear variation in addition to an overall increase or decrease over time. According to the missing data analysis, missing patterns were assumed as not missing at random. Hence, missing values were handled by using the Taylor series variance estimation with the “NOMCAR” option in the “SURVERYLOGISTIC” process.
RESULTS
The sample sizes by sex and race and ethnicity are shown in Table 1. Of the 198 540 adolescents in the sample, there were slightly more boys than girls (51% boys; 49% girls), and the average age for both groups was ~16 years (male mean age: 16.11 years; female mean age: 16.02 years). Figure 1 portrays changes in the distribution of suicidal behaviors by survey year and race and ethnicity. From 1991 to 2017, the weighted overall prevalence rates of suicidal ideation, plan, attempt, and injury by attempt were 18.8%, 14.7%, 7.9%, and 2.5%, respectively. ORs for the linear trends of suicidal thoughts and behaviors by sex and race and ethnicity groups are shown in Tables 2 and 3, respectively. Across all sex and racial and ethnic groups (except non-Hispanic multiple-race group), significant linear decreases were present in self-reported suicidal ideation and suicide plan. Among AI/AN adolescents, there was a noticeable increase in suicidal behaviors during 1995 and 1997.
TABLE 1.
Unweighted Sample Sizes and Weighted Percentages for Adolescents by Race and Ethnicity and Sex: YRBS 1999–2017
| All Groups, n (%) | White, n (%) | Black, n (%) | Hispanic, n (%) | Asian American or PI, n (%) | AI/AN, n (%) | Non-Hispanic Multiple Race, n (%) | |
|---|---|---|---|---|---|---|---|
| Female | 100 600 (49) | 41 527 (48) | 23 334 (51) | 27 750 (49) | 4034 (47) | 1006 (45) | 2949 (54) |
| Male | 97 940 (51) | 42 175 (52) | 20 946 (49) | 26 804 (51) | 4244 (53) | 1251 (55) | 2520 (46) |
| Total | 198 540 (100) | 83 702 (100) | 44 280 (100) | 54 554 (100) | 8278 (100) | 2257 (100) | 5469 (100) |
FIGURE 1.
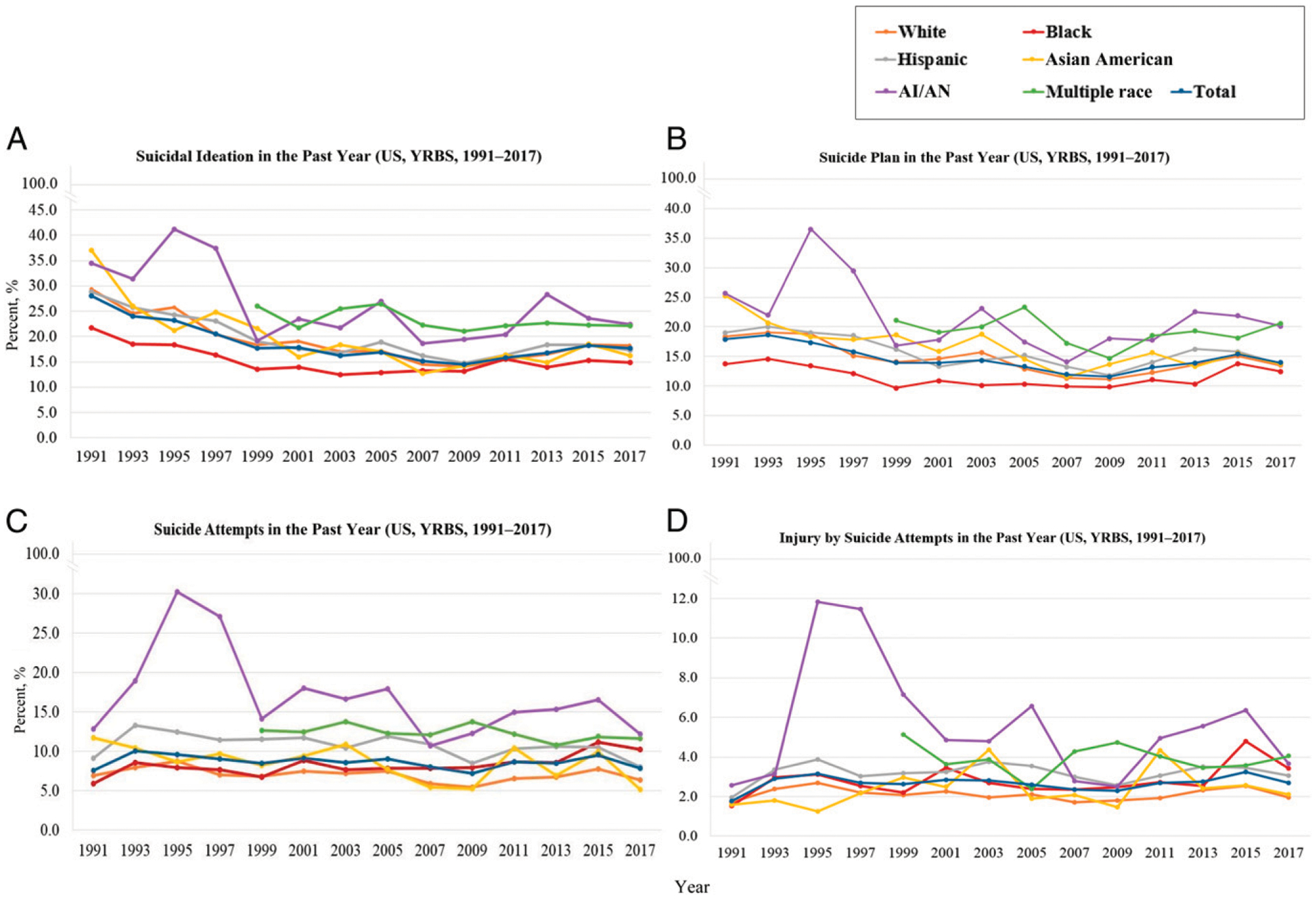
Suicidal thoughts and behaviors trends by race and ethnicity: YRBS 1991–2017. Both the linear trend and quadratic trend had a P value <.05. Additionally, multiracial data were not collected before 1999. A, Suicidal ideation in the past year (US, YRBS, 1991–2017); B, Suicidal plan in the past year (US, YRBS, 1991–2017); C, Suicidal attempts in the past year (US, YRBS, 1991–2017); D, Injury by suicide attempts in the past year (US, YRBS, 1991–2017).
TABLE 2.
Linear Trend for Suicidal Thoughts and Behaviors by Sex Groups From 1991 to 2017
| Suicidal Behaviors | Sex | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Female | Male | ||||||||
| OR | 95% CI | P | OR | 95% CI | P | OR | 95% CI | P | |
| Suicidal ideation | 0.96 | 0.95–0.96 | <.001 | 0.96 | 0.95–0.96 | <.001 | 0.96 | 0.95–0.96 | <.001 |
| Suicide plan | 0.97 | 0.96–0.98 | <.001 | 0.98 | 0.97–0.98 | <.001 | 0.97 | 0.97–0.98 | <.001 |
| Suicide attempt | 0.98 | 0.98–0.99 | <.001 | 1.01 | 1.00–1.02 | .30 | 0.99 | 0.98–1.00 | .008 |
| Injury by attempt | 1.00 | 0.99–1.01 | .81 | 1.01 | 0.99–1.02 | .31 | 1.00 | 0.99–1.02 | .47 |
All analyses adjusted for grade levels.
TABLE 3.
Linear Trend for Suicidal Thoughts and Behaviors by Race and Ethnicity Groups From 1991 to 2017
| Suicidal Behaviors | Race and Ethnicity | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| White | Black | Hispanic | Asian American or PI | AI/AN | Non-Hispanic Multiple Race | |||||||||||||
| OR | 95% CI | P | OR | 95% CI | P | OR | 95% CI | P | OR | 95% CI | P | OR | 95% CI | P | OR | 95% CI | P | |
| Suicidal ideation | 0.95 | 0.94–0.96 | <.001 | 0.97 | 0.96–0.98 | <.001 | 0.95 | 0.94–0.96 | <.001 | 0.94 | 0.92–0.95 | <.001 | 0.95 | 0.92–0.97 | <.001 | 0.98 | 0.96–1.00 | .090 |
| Suicide plan | 0.97 | 0.96–0.97 | <.001 | 0.98 | 0.97–0.99 | <.001 | 0.97 | 0.96–0.98 | <.001 | 0.95 | 0.95–0.97 | <.001 | 0.97 | 0.94–0.99 | .017 | 0.99 | 0.97–1.02 | .564 |
| Suicide attempt | 0.99 | 0.98–1.00 | .003 | 1.02 | 1.01–1.04 | <.001 | 0.98 | 0.97–0.99 | <.001 | 0.96 | 0.94–0.99 | .005 | 0.95 | 0.92–0.99 | .005 | 0.99 | 0.96–1.02 | .389 |
| Injury by attempt | 1.00 | 0.98–1.01 | .58 | 1.02 | 1.00–1.04 | .06 | 1.00 | 0.99–1.02 | .79 | 1.02 | 0.99–1.06 | .23 | 0.98 | 0.92–1.04 | .463 | 0.99 | 0.94–1.04 | .602 |
All analyses adjusted for grade levels.
For suicide attempts, however, there was a statistically significant annual decline of suicide attempts among adolescent girls (OR, 0.98; 95% CI, 0.98–0.99; P < .001), whereas no significant trend was observed for boys (see Table 2). Results for trends of suicide attempts across race and ethnicity indicated adolescents who identified as white, Hispanic, Asian American or PI, and AI/AN had a significant linear decrease; however, black adolescents had a significantly linear increase in self-reported suicide attempts (OR, 1.02; 95% CI, 1.01–1.04; P < .001). Linear trends for injury by attempt were nonsignificant among adolescents from both sex groups and all races and ethnicities. There were no significant trends across any suicidal outcomes among individuals in the non-Hispanic multiple-race group.
Subgroup differences were observed after stratifying by sex and race and ethnicity (Tables 4, 5, and 6). There were significant linear decreases in suicidal ideation and suicide plan across the years among all adolescent subgroups, except for nonsignificant trends found for black girls and AI/AN boys for suicide plan only, as well as AI/AN girls, non-Hispanic multiple-race boys and girls for suicidal ideation and plan. Additionally, there were significant quadratic trends in suicidal ideation and suicide plan among adolescents who were white girls and boys, black girls and boys, Hispanic girls and boys, and Asian American girls and boys (suicidal ideation only), suggesting a nonlinear relationship with a downward but concave-up trend over time among these groups (P < .001).
TABLE 4.
Linear and Quadratic Trends for Suicidal Thoughts and Behaviors by Race and Ethnicity Among Female Adolescents, 1991–2017
| Suicidal Behaviors | White | Black | Hispanic | Asian American or PI | AI/AN | Non-Hispanic Multiple Race | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% Cl | P | OR | 95% Cl | P | OR | 95% Cl | P | OR | 95% Cl | P | OR | 95% Cl | P | OR | 95% Cl | P | |
| Suicidal ideation | ||||||||||||||||||
| Linear | 0.95 | 0.95–0.96 | <.001 | 0.98 | 0.97–0.99 | <.001 | 0.95 | 0.95–0.96 | <.001 | 0.92 | 0.90–0.95 | <.001 | 1.00 | 0.96–1.05 | .90 | 0.99 | 0.95–1.02 | .41 |
| Quadratic | 1.01 | 1.01–1.01 | <.001 | 1.01 | 1.01–1.02 | <.001 | 1.01 | 1.01–1.01 | <.001 | 1.01 | 1.01–1.02 | <.001 | 1.02 | 1.01–1.03 | .00 | 1.01 | 1.00–1.02 | .07 |
| Suicide plan | ||||||||||||||||||
| Linear | 0.97 | 0.96–0.97 | <.001 | 0.99 | 0.98–1.00 | .09 | 0.96 | 0.95–0.97 | <.001 | 0.95 | 0.93–0.97 | <.001 | 1.01 | 0.97–1.05 | .71 | 0.98 | 0.94–1.02 | .23 |
| Quadratic | 1.01 | 1.01–1.01 | <.001 | 1.01 | 1.01–1.01 | <.001 | 1.01 | 1.01–1.01 | <.001 | 1.01 | 1.00–1.01 | .08 | 1.02 | 1.01–1.03 | .00 | 1.02 | 1.01–1.03 | .00 |
| Suicide attempt | ||||||||||||||||||
| Linear | 0.98 | 0.97–0.99 | <.001 | 1.02 | 1.01–1.03 | .00 | 0.97 | 0.96–0.98 | <.001 | 0.95 | 0.92–0.98 | .00 | 0.96 | 0.90–1.02 | .17 | 0.99 | 0.95–1.04 | .64 |
| Quadratic | 1.00 | 1.00–1.01 | .049 | 1.01 | 1.00–1.01 | .01 | 1.00 | 0.99–1.00 | .048 | 1.01 | 1.00–1.02 | .07 | 1.00 | 0.99–1.02 | .73 | 1.01 | 0.99–1.02 | .32 |
| Injury by attempt | ||||||||||||||||||
| Linear | 1.00 | 0.98–1.02 | .88 | 1.02 | 1.00–1.04 | .12 | 1.00 | 0.98–1.01 | .70 | 1.00 | 0.96–1.06 | .89 | 1.04 | 0.94–1.15 | .43 | 0.97 | 0.90–1.04 | .35 |
| Quadratic | 1.01 | 1.00–1.01 | .01 | 1.01 | 1.00–1.02 | .00 | 1.00 | 0.99–1.00 | .61 | 1.00 | 0.99–1.02 | .70 | 1.01 | 0.99–1.03 | .41 | 1.02 | 1.00–1.05 | .08 |
All analyses adjusted for grade levels.
TABLE 5.
Linear and Quadratic Trends for Suicidal Thoughts and Behaviors by Race and Ethnicity Among Male Adolescents, 1991–2017
| Suicidal Behaviors | White | Black | Hispanic | Asian American or PI | AIAN | Non-Hispanic Multiple Race | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% Cl | P | OR | 95% Cl | P | OR | 95% Cl | P | OR | 95% Cl | P | OR | 95% Cl | P | OR | 95% Cl | P | |
| Suicidal ideation | ||||||||||||||||||
| Linear | 0.96 | 0.95–0.96 | <.001 | 0.96 | 0.95–0.97 | <.001 | 0.96 | 0.95–0.97 | <.001 | 0.95 | 0.93–0.97 | <.001 | 0.94 | 0.89–0.99 | .01 | 0.96 | 0.92–1.01 | .10 |
| Quadratic | 1.01 | 1.01–1.01 | <.001 | 1.01 | 1.00–1.01 | <.001 | 1.01 | 1.01–1.01 | <.001 | 1.01 | 1.01–1.02 | .00 | 1.01 | 1.00–1.02 | .09 | 0.99 | 0.98–1.01 | .29 |
| Suicide plan | ||||||||||||||||||
| Linear | 0.97 | 0.96–0.98 | <.001 | 0.98 | 0.97–1.00 | .01 | 0.98 | 0.97–0.99 | <.001 | 0.97 | 0.94–0.99 | .00 | 0.97 | 0.93–1.02 | .23 | 0.97 | 0.93–1.02 | .25 |
| Quadratic | 1.00 | 1.00–1.01 | .06 | 1.01 | 1.00–1.01 | .00 | 1.00 | 1.00–1.01 | .02 | 1.01 | 1.00–1.01 | .17 | 1.00 | 0.99–1.02 | .56 | 0.99 | 0.98–1.01 | .46 |
| Suicide attempt | ||||||||||||||||||
| Linear | 1.00 | 0.98–1.01 | .76 | 1.04 | 1.02–1.07 | <.001 | 0.99 | 0.98–1.01 | .35 | 0.98 | 0.95–1.02 | .42 | 0.96 | 0.90–1.02 | .18 | 1.00 | 0.94–1.06 | .96 |
| Quadratic | 1.00 | 0.99–1.00 | .16 | 1.00 | 0.99–1.00 | .38 | 1.00 | 1.00–1.00 | .67 | 0.99 | 0.98–1.01 | .34 | 1.00 | 0.99–1.02 | .70 | 0.98 | 0.96–1.00 | .04 |
| Injury by attempt | ||||||||||||||||||
| Linear | 0.98 | 0.96–1.01 | .26 | 1.04 | 1.00–1.08 | .048 | 1.01 | 0.99–1.04 | .40 | 1.08 | 0.99–1.16 | .08 | 0.89 | 0.78–1.02 | .09 | 0.99 | 0.90–1.09 | .82 |
| Quadratic | 0.99 | 0.99–1.00 | .01 | 0.99 | 0.98–1.00 | .08 | 1.00 | 0.99–1.00 | .13 | 0.97 | 0.95–0.99 | .01 | 0.99 | 0.96–1.01 | .31 | 0.98 | 0.95–1.02 | .30 |
All analyses adjusted for grade levels.
TABLE 6.
Summary of Linear and Quadratic Trends for Suicidal Thoughts and Behaviors by Interactions of Race and Ethnicity and Sex Groups From 1991 to 2017
| Suicidal Behaviors | White Girl | White Boy | Black Girl | Black Boy | Hispanic Girl | Hispanic Boy | Asian American or PI Girl | Asian American or PI Boy | AI/AN Girl | AI/AN Boy | Non-Hispanic Multiple Race Girl | Non-Hispanic Multiple Race Boy |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Suicidal ideation | ↓(L,Q) | ↓(L,Q) | ↓(L,Q) | ↓(L,Q) | ↓(L,Q) | ↓(L,Q) | ↓(L,Q) | ↓(L,Q) | NS | ↓(L) | NS | NS |
| Suicide plan | ↓(L,Q) | ↓(L) | NS | ↓(L,Q) | ↓(L,Q) | ↓(L,Q) | ↓(L) | ↓(L) | NS | NS | NS | NS |
| Suicide attempt | ↓(L) | NS | ↑(L,Q) | ↑(L) | ↓(L,Q) | NS | ↓(L) | NS | NS | NS | NS | NS |
| Injury by attempt | NS | NS | NS | ↑(L) | NS | NS | NS | NS | NS | NS | NS | NS |
Both the linear trend (L) and quadratic trend (Q) had a P value <.05. Up arrows indicate increasing trends; down arrows indicate decreasing trends. NS, nonsignificant.
When examining trends for self-reported suicide attempts, girls that classified as white, Hispanic, and Asian American or PI had a significant linear decrease (see Table 4). Also, marginally significant quadratic trends in suicide attempts were observed among white girls (OR, 1.00; 95% CI, 1.00–1.01; P = .049) and Hispanic girls (OR, 1.00; 95% CI, 0.99–1.00; P = .048), suggesting accelerations in the decreasing rates of attempting suicide over time among these 2 groups. Boys in these racial and ethnic groups, together with AI/AN and non-Hispanic multiple-race boys, had nonsignificant changes in suicide attempts (see Table 5).
However, among black adolescents, there were significant and positive linear trends found for suicide attempts among both girls (OR, 1.02; 95% CI, 1.01–1.03; P = .003) and boys (OR, 1.04; 95% CI, 1.02–1.07; P < .001). The quadratic trend examining the rate of suicide attempts among black girls was also significant (Table 4), indicating an acceleration in the increasing rate of self-reported suicide attempts in this group (OR, 1.01; 95% CI, 1.00–1.01; P = .01). For injury by attempt (Table 5), there was a significant linear increase for black boys (OR, 1.04; 95% CI, 1.00–1.08; P = .048).
DISCUSSION
Nationally representative data from 1991 to 2017 reflect findings of concern regarding US high schoolers’ engagement in suicidal behaviors. Our findings reveal that over that span of time, almost 1 in 5 adolescents are thinking about suicide (18.8%), and >1 in 10 has a suicide plan (14.7%). Despite increased attention given to the creation of campaigns to reduce youth suicide in the United States over the last decade,22–24 these findings suggest that continued concern and attention regarding suicidal behaviors among high school–aged youth is warranted, although more recent data and attention have been given to younger US youth.6,8
Our findings also indicate 2 distinct trends regarding suicidal thoughts and behaviors. First, the rates for suicidal ideation and suicide plans have been trending downward across all sex and racial and ethnic groups. This is an important finding because suicidal ideation and suicide plan are key risk factors to engagement in suicidal behaviors (eg, suicide attempt).25 The findings, however, are not as heartening regarding suicide attempts and injury by attempt, particularly for specific sex and racial and ethnic groups. Black adolescents experienced an increase in rates for suicide attempts, and a significant increase was reported for black adolescent boys concerning the rates of injury caused by suicide attempts. Adolescent girls from all racial and ethnic groups experienced a significant downward trend in suicide attempts (white, Hispanic, and Asian American or PI); however, for black adolescent girls, there was a significant increase.
Findings regarding the rising rates of suicide attempts in black youth may be related to the documented disparities in mental health treatment26–28 and common social etiologic factors disproportionately experienced by black youth.29–31 Authors of epidemiological studies, since 1990, affirm lower mental health treatment among black adolescents compared with their white counterparts.26,32–34 Lower rates of treatment could be attributed to black adolescents not wanting to be judged as weak and refusing to acknowledge mental illness symptoms.35,36 Another explanation could be that black adolescents view mental health treatment with skepticism because of mistrust of providers causing them to prefer to address mental health symptoms with family and peer networks.37 This could lead to unmanaged and unmonitored mental health concerns that escalate to self-harm behaviors. Finally, social etiologic factors disproportionately experienced by black adolescents include racial discrimination,30,31 adverse childhood experiences (eg, abuse and neglect),29 and poverty,38,39 all of which have been positively associated with suicidal behaviors in this group.
The significant increase found for black boys for injury by attempt could be explained by the documented change of suicide method in adolescents.40–43 For example, during this study period, rates of suicide by firearms decreased from 60% to 22%, whereas rates of suicide by hanging and/or suffocation increased from 20% to 60%.44 Unfortunately, hanging and/or suffocation is the leading method of suicide in youth.45–47 It is highly lethal, and items related to hanging and/or suffocation are more accessible than a firearm.47,48 Our findings regarding injury by attempt suggest black boys may be engaging in more lethal methods of suicide, which ultimately lead to the need for medical care.
AI/AN adolescents saw a notable spike in suicidal behaviors between the years 1995 and 1997, which might be associated with an uptick in substance use rates observed among AI/AN adolescents during that same period.49 Namely, between 1995 and 1997, AI/AN adolescents saw increases in marijuana, methamphetamine, inhalant, cocaine, and cigarette use.50 Elsewhere, substance use has been strongly associated with increased rates of suicidal behaviors among AI/AN youth during that period,49,51,52 suggesting a strong possible connection between the increase in substance use and rising suicidal behavior rates for AI/AN adolescents.
Further research is necessary to understand the rise in suicide among older black adolescents. It is critical to develop and test the efficacy of treatment or prevention interventions on a larger scale that have been shown to reduce suicide risk among older black adolescents.15 Preventive interventions within the black community should invest in key protective factors that help reduce stigma related to mental illness and increase help-seeking behaviors.53,54 Research specifically designed to examine treatments in clinical and nonclinical settings that ameliorate the symptoms or signs of suicidal behaviors among black adolescents should be considered. Primary care settings, where well visits are most likely to occur for adolescents,41–43 can play a critical role in screening efforts to identify black adolescents who might be at risk for engagement in suicidal behaviors.44
This study has several limitations. One important limitation is that the YRBS data are cross-sectional. Therefore, we cannot determine the causality and directionality of the associations found. Second, the results only applied to youth who attend school based on the YRBS sampling design. Thus, they are not representative of all adolescents in this age group. Nationwide, ~5.8% of individuals drop out of high school, among which Hispanic (9.1%) and black (7.0%) students have higher rates than their white (4.5%) and Asian American (2.0%) counterparts.55 Third, the measurements of suicidal thoughts and behaviors are self-reported. Despite the survey questions demonstrating good test-retest reliability,19 there is potential for some level of under- or overreporting bias.
CONCLUSIONS
When examining youth suicidal behavior, white youth have historically had higher rates of suicide attempts and deaths by suicide compared with their black counterparts; however, this study provides some evidence to the contrary. The results suggest that, over time, black youth have experienced an increase in suicide attempts, which is the most prominent risk factor associated with suicide deaths, and for black boys, a significant increase in injury by attempt, which suggests black boys may be engaging in more lethal means when attempting suicide. Examining trends in suicidal ideation and behaviors over time by sex and race and ethnicity allows us to determine where to focus prevention and intervention efforts. Future research should be used to examine the underlying reasons for these observed changes.
WHAT’S KNOWN ON THIS SUBJECT:
Suicide is the second leading cause of death among adolescents. Racial and ethnic disparities have been discovered in suicide deaths. Racial and ethnic differences in trends of youth suicidal ideation, plans, and suicide attempts, however, remain understudied.
WHAT THIS STUDY ADDS:
This study uncovered racial and ethnic differences in trends of suicidal behaviors. Suicide ideation and suicidal plans decreased among US adolescents between 1991 and 2017. Subgroup findings indicate suicide attempts increased only among black adolescents.
FUNDING:
No external funding.
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
ABBREVIATIONS
- AI/AN
American Indian and Alaskan native
- CDC
Centers for Disease Control and Prevention
- CI
confidence interval
- OR
oddsratio
- PI
Pacific Islander
- YRBS
Youth Risk Behavior Survey
Footnotes
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
COMPANION PAPER: A companion to this article can be found online at www.pediatrics.org/cgi/doi/10.1542/peds.2019-1912.
REFERENCES
- 1.Centers for Disease Control and Prevention. WISQARS. Leading causes of death reports, 1981 – 2017 Available at: https://webappa.cdc.gov/sasweb/ncipc/leadcause.html. Accessed July 11, 2019
- 2.Cash SJ, Bridge JA. Epidemiology of youth suicide and suicidal behavior. Curr Opin Pediatr. 2009;21(5):613–619 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Cha CB, Franz PJ, M Guzmán E, et al. Annual Research Review: suicide among youth - epidemiology, (potential) etiology, and treatment. J Child Psychol Psychiatry. 2018;59(4):460–482 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bridge JA, McBee-Strayer SM, Cannon EA, et al. Impaired decision making in adolescent suicide attempters. J Am Acad Child Adolesc Psychiatry. 2012; 51(4):394–403 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sheftall AH, Davidson DJ, McBee-Strayer SM, et al. Decision-making in adolescents with suicidal ideation: a case-control study. Psychiatry Res. 2015;228(3):928–931 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bridge JA, Asti L, Horowitz LM, et al. Suicide trends among elementary school-aged children in the United States from 1993 to 2012. JAMA Pediatr. 2015;169(7):673–677 [DOI] [PubMed] [Google Scholar]
- 7.Bridge JA, Horowitz LM, Fontanella CA, et al. Age-related racial disparity in suicide rates among US youths from 2001 through 2015. JAMA Pediatr. 2018; 172(7):697–699 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Sheftall AH, Asti L, Horowitz LM, et al. Suicide in elementary school-aged children and early adolescents. Pediatrics. 2016;138(4):e20160436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Borges G, Nock MK, Haro Abad JM, et al. Twelve-month prevalence of and risk factors for suicide attempts in the World Health Organization World Mental Health Surveys. J Clin Psychiatry. 2010; 71(12):1617–1628 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Glenn CR, Nock MK. Improving the short-term prediction of suicidal behavior. Am J Prev Med. 2014;47(3 suppl 2):S176–S180 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.O’Carroll PW, Berman AL, Maris RW, et al. Beyond the Tower of Babel: a nomenclature for suicidology. Suicide Life Threat Behav. 1996;26(3):237–252 [PubMed] [Google Scholar]
- 12.Silverman MM, Berman AL, Sanddal ND, O’carroll PW, Joiner TE. Rebuilding the tower of Babel: a revised nomenclature for the study of suicide and suicidal behaviors. Part 1: background, rationale, and methodology. Suicide Life Threat Behav. 2007;37(3):248–263 [DOI] [PubMed] [Google Scholar]
- 13.Silverman MM, Berman AL, Sanddal ND, O’carroll PW, Joiner TE. Rebuilding the tower of Babel: a revised nomenclature for the study of suicide and suicidal behaviors. Part 2: suicide-related ideations, communications, and behaviors. Suicide Life Threat Behav. 2007;37(3):264–277 [DOI] [PubMed] [Google Scholar]
- 14.Centers for Disease Control and Prevention. WISQARS. Nonfatal injury reports, 2000 – 2017 Available at: https://webappa.cdc.gov/sasweb/ncipc/nfirates.html. Accessed September 16, 2019
- 15.Joe S, Scott ML, Banks A. What works for adolescent black males at risk of suicide: a review. Res Soc Work Pract. 2018;28(3):340–345 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Centers for Disease Control and Prevention. Youth Risk Behavior Surveillance System (YRBSS). 2018. Available at: https://www.cdc.gov/healthyyouth/data/yrbs/index.htm. Accessed January 1, 2019
- 17.Brener ND, Kann L, Shanklin S, et al. ; Centers for Disease Control and Prevention (CDC). Methodology of the youth risk behavior surveillance system–2013. MMWR Recomm Rep. 2013;62(RR):1–20 [PubMed] [Google Scholar]
- 18.Silverman JG, Raj A, Mucci LA, Hathaway JE. Dating violence against adolescent girls and associated substance use, unhealthy weight control, sexual risk behavior, pregnancy, and suicidality. JAMA. 2001;286(5):572–579 [DOI] [PubMed] [Google Scholar]
- 19.Brener ND, Kann L, McManus T, et al. Reliability of the 1999 youth risk behavior survey questionnaire. J Adolesc Health. 2002;31(4):336–342 [DOI] [PubMed] [Google Scholar]
- 20.Centers for Disease Control and Prevention. Combining YRBS Data Across Years and Sites. Washington, DC: US Department of Health and Human Services; 2018 [Google Scholar]
- 21.Lowry R, Crosby AE, Brener ND, Kann L. Suicidal thoughts and attempts among U.S. high school students: trends and associated health-risk behaviors, 1991–2011. J Adolesc Health. 2014;54(1): 100–108 [DOI] [PubMed] [Google Scholar]
- 22.Olfson M, Marcus SC, Bridge JA. Focusing suicide prevention on periods of high risk. JAMA. 2014;311(11): 1107–1108 [DOI] [PubMed] [Google Scholar]
- 23.Pirkis J, Rossetto A, Nicholas A, et al. Suicide prevention media campaigns: a systematic literature review. Health Commun. 2019;34(4):402–414 [DOI] [PubMed] [Google Scholar]
- 24.Torok M, Calear A, Shand F, Christensen H. A systematic review of mass media campaigns for suicide prevention: understanding their efficacy and the mechanisms needed for successful behavioral and literacy change. Suicide Life Threat Behav. 2017;47(6):672–687 [DOI] [PubMed] [Google Scholar]
- 25.Bridge JA, Goldstein TR, Brent DA. Adolescent suicide and suicidal behavior. J Child Psychol Psychiatry. 2006;47(3–4):372–394 [DOI] [PubMed] [Google Scholar]
- 26.Wu P, Hoven CW, Bird HR, et al. Depressive and disruptive disorders and mental health service utilization in children and adolescents. J Am Acad Child Adolesc Psychiatry. 1999;38(9): 1081–1090–1092 [DOI] [PubMed] [Google Scholar]
- 27.US Department of Health and Human Services. Mental Health: Culture, Race, and Ethnicity-A Supplement to Mental Health: A Report of the Surgeon General. Rockville, MD: US Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services; 2001 [Google Scholar]
- 28.Costello EJ, Mustillo S, Erkanli A, Keeler G, Angold A. Prevalence and development of psychiatric disorders in childhood and adolescence. Arch Gen Psychiatry. 2003;60(8):837–844 [DOI] [PubMed] [Google Scholar]
- 29.Hunt TKA, Slack KS, Berger LM. Adverse childhood experiences and behavioral problems in middle childhood. Child Abuse Negl. 2017;67:391–402 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Lanier Y, Sommers MS, Fletcher J, Sutton MY, Roberts DD. Examining racial discrimination frequency, racial discrimination stress, and psychological well-being among black early adolescents. J Black Psychol. 2017;43(3):219–229 [Google Scholar]
- 31.Tobler AL, Maldonado-Molina MM, Staras SA, et al. Perceived racial/ethnic discrimination, problem behaviors, and mental health among minority urban youth. Ethn Health. 2013;18(4):337–349 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Garrison CZ, Jackson KL, Marsteller F, McKeown R, Addy C. A longitudinal study of depressive symptomatology in young adolescents. J Am Acad Child Adolesc Psychiatry. 1990;29(4):581–585 [DOI] [PubMed] [Google Scholar]
- 33.Roberts RE, Roberts CR, Chen YR. Ethnocultural differences in prevalence of adolescent depression. Am J Community Psychol. 1997;25(1): 95–110 [DOI] [PubMed] [Google Scholar]
- 34.Merikangas KR, He JP, Burstein M, et al. Service utilization for lifetime mental disorders in U.S. adolescents: results of the National Comorbidity Survey-Adolescent Supplement (NCS-A). J Am Acad Child Adolesc Psychiatry. 2011; 50(1):32–45 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Lindsey MA, Korr WS, Broitman M, et al. Help-seeking behaviors and depression among African American adolescent boys. Soc Work. 2006;51(1):49–58 [DOI] [PubMed] [Google Scholar]
- 36.Weist MD, Freedman AH, Paskewitz DA, Proescher EJ, Flaherty LT. Urban youth under stress: empirical identification of protective factors. J Youth Adolesc. 1995;24(6):705 [Google Scholar]
- 37.Lindsey MA, Joe S, Nebbitt V. Family matters: the role of mental health stigma and social support on depressive symptoms and subsequent help seeking among African American boys. J Black Psychol. 2010;36(4): 458–482 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Kubrin CE, Wadsworth T, DiPietro S. Deindustrialization, disadvantage and suicide among young black males. Soc Forces. 2006;84(3):1559–1579 [Google Scholar]
- 39.Joe S Explaining changes in the patterns of black suicide in the United States from 1981 to 2002: an age, cohort, and period analysis. J Black Psychol. 2006;32(3):262–284 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Baker SP, Hu G, Wilcox HC, Baker TD. Increase in suicide by hanging/suffocation in the U.S., 2000–2010. Am J Prev Med. 2013;44(2):146–149 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Shaw D, Fernandes JR, Rao C. Suicide in children and adolescents: a 10-year retrospective review. Am J Forensic Med Pathol. 2005;26(4):309–315 [DOI] [PubMed] [Google Scholar]
- 42.Centers for Disease Control and Prevention (CDC). Suicide among black youths--United States, 1980–1995. MMWR Morb Mortal Wkly Rep. 1998;47(10): 193–196 [PubMed] [Google Scholar]
- 43.Holland KM, Vivolo-Kantor AM, Logan JE, Leemis RW. Antecedents of suicide among youth aged 11–15: a multistate mixed methods analysis. J Youth Adolesc. 2017;46(7):1598–1610 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Cheung AH, Dewa CS. Current trends in youth suicide and firearms regulations. Can J Public Health. 2005;96(2):131–135 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Curtin SC, Warner M, Hedegaard H. Increase in suicide in the United States, 1999–2014. NCHS Data Brief. 2016;(241): 1–8 [PubMed] [Google Scholar]
- 46.Curtin SC, Heron M, Miniño AM, Warner M. Recent increases in injury mortality among children and adolescents aged 10–19 years in the United States: 1999–2016. Natl Vital Stat Rep. 2018;67(4): 1–16 [PubMed] [Google Scholar]
- 47.Ruch DA, Sheftall AH, Schlagbaum P, et al. Trends in suicide among youth aged 10 to 19 years in the United States, 1975 to 2016 [published correction appears in JAMA Netw Open. 2019;2(6):e197687]. JAMA Netw Open. 2019;2(5):e193886. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Kõlves K, McDonough M, Crompton D, de Leo D. Choice of a suicide method: trends and characteristics. Psychiatry Res. 2018;260:67–74 [DOI] [PubMed] [Google Scholar]
- 49.Borowsky IW, Resnick MD, Ireland M, Blum RW. Suicide attempts among American Indian and Alaska Native youth: risk and protective factors. Arch Pediatr Adolesc Med. 1999;153(6): 573–580 [DOI] [PubMed] [Google Scholar]
- 50.Beauvais F, Jumper-Thurman P, Burnside M. The changing patterns of drug use among American Indian students over the past 30 years. Am Indian Alsk Native Ment Health Res. 2008;15(2):15–24 [DOI] [PubMed] [Google Scholar]
- 51.Shaughnessy L, Doshi SR, Jones SE. Attempted suicide and associated health risk behaviors among Native American high school students. J Sch Health. 2004;74(5):177–182 [DOI] [PubMed] [Google Scholar]
- 52.Gone JP, Trimble JE. American Indian and Alaska Native mental health: diverse perspectives on enduring disparities. Annu Rev Clin Psychol. 2012; 8(1):131–160 [DOI] [PubMed] [Google Scholar]
- 53.Greening L, Stoppelbein L. Religiosity, attributional style, and social support as psychosocial buffers for African American and white adolescents’ perceived risk for suicide. Suicide Life Threat Behav. 2002;32(4):404–417 [DOI] [PubMed] [Google Scholar]
- 54.Marion MS, Range LM. African American college women’s suicide buffers. Suicide Life Threat Behav. 2003;33(1): 33–43 [DOI] [PubMed] [Google Scholar]
- 55.US Department of Education National Center for Education Statistics. Trends in high school dropout and completion rates in the United States. 2019. Available at: https://nces.ed.gov/programs/dropout/ind_03.asp. Accessed March 21, 2019