

Dear Editors,
With the spread of the COVID‐19 (coronavirus 2019) pandemic paralysing the world, governments have adopted control measures ranging from social distancing and self‐quarantine to total lockdowns depending on the severity of the outbreak. Such physical distancing also implies that providers must be prepared for disruption from this pandemic mode of health care for the next 18 months. 1 Unsurprisingly, a major at‐risk population are patients with chronic wounds as they often suffer from several underlying comorbidities, such as diabetes, cardiovascular and cerebrovascular diseases, hypertension, and respiratory diseases, which, in addition to old age and traumatic injuries, intensify susceptibility to COVID‐19. 2 In fact, untreated chronic ulcerations can even be an entry door for secondary infections, further debilitating patients. 3 With chronic wounds already occupying a major part of the health system, complete cessation of professional wound care during restricted health care visit may exacerbate these chronic wounds into acute wounds with irreversible systemic damage that may result in severe complications, or even mortality. Hence, chronic non‐healing wounds, which already require specialised care, must be aggressively attended to by a multidisciplinary wound care team.
Out of the need to protect both medical workers and patients, hospital visits for non‐urgent conditions are largely prohibited or restricted. In cities or countries where outbreak severity is still minimal, wound patients may even voluntarily refuse clinic visits for fear of being quarantined or exposed to the coronavirus. Fortunately, telecommunication facilitates interaction that replaces face‐to‐face contact so as to prevent the spread of this highly communicable disease. For instance, a study has showed that regular wound care helps to decrease diabetes‐related ER visits, hospitalisation, length‐of‐stay, and amputations. 1 Through efficient and effective application of tele‐health strategies, health care providers can bypass infection risks while enabling the continuation of care for chronic wounds.
After the outbreak of COVID‐19, an institution‐wide protocol has been established at Kaohsiung Medical University Hospital (KMUH) for the management of chronic wounds through remote wound care. All patients received optimal care without sequelae. The central concept behind this management algorithm has been described as a direct‐to‐consumer forward triage that allows patients to be efficiently screened with the advantages of being both patient‐centred and protective of patients, clinicians, and the community from exposure. 4 This management strategy of remote control, patient education, and home care has been successful in maintaining regular care of chronic wounds outside of the hospital; the importance of which has been highlighted in the inevitability of wound assessment and treatment (eg, dressing changes). 5
The proposed virtual algorithm for chronic wound care in KMUH could be applied to all patients who previously undergo follow‐up at the outpatient clinic at our hospital (Figure 1). After the COVID‐19 outbreak, doctor‐patient wireless communication through the telephone, email, WeChat, WhatsApp, and Line messenger apps are conducted by the medical team 7 days a week. Patients are reminded that they can also contact the medical team 24 hours per day with their concerns. Wound specialists, including physicians and registered nurses, can perform wound assessment through questions in text message format or phone calls, as well as photos and videos, to determine whether the lesions are stable, improving, or deteriorating. Questions can be asked regarding the presence of any foul odour or local heat. Clinical photos and videos sent by the patients provide visual clues for evaluation such as the presence of any erythema, exudation, ulceration, pustule formation, and so on. In the same light, should patients have any doubt in the execution of simple wound dressing, the medical team can respond with a virtually personalised tutorial video with step‐by‐step explanation or a video call for real‐time instruction for correction or adjustment in the procedures if mistakes are identified. 6
FIGURE 1.
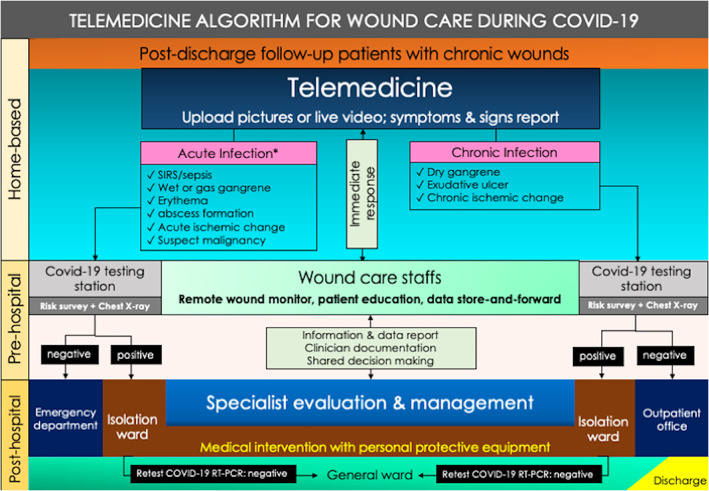
Algorithm for chronic wound management during COVID‐19
If signs and symptoms of acute infection are detected in a new patient or in a patient under follow‐up, further medical intervention is warranted. First of all, the patients receive testing for COVID‐19 at the hospital testing station, which includes an initial risk survey consisting of a chest radiograph and history of travel, occupation, contact, and cluster as outlined by the Taiwanese Center of Disease Control to rule out any potential carrier of COVID‐19. When infection is suspected, a reverse transcription polymerase chain reaction testing for COVID‐19 from nasopharyngeal swabs and chest‐computed tomography are arranged. If tested positive for coronavirus, the patient enters isolation under standard COVID‐19 treatment. If the result is negative, the patient proceeds to the emergency department and wound care is provided by the consulted plastic surgeon. Whereas if a new patient presents with chronic infected wounds associated with dry gangrene, chronic ischemic change, or exudative ulcer, the patient must also undergo risk survey and chest radiograph screening at the COVID‐19 testing station. If tested positive, the patient enters isolation care for coronavirus. If negative, the patient can then be treated through appointment at the Outpatient Wound Care Office. Throughout every contact with suspected or confirmed patients, it is crucial that every member of the Wound Care Unit must be dressed in personal protective equipment until the patients are cleared of infection and isolation status.
In conclusion, the complex nature of chronic wounds during COVID‐19 calls for a unique management that can only be implemented through a redesigned multidisciplinary approach. This comprehensive algorithm for chronic wound care via telemedicine assistance during the setting of COVID‐19 or any pandemic could safeguard the safety and health for both patients and medical providers, as the exposure risks of COVID‐19 are reduced to a minimum at all phases of care.
CONFLICT OF INTEREST
The authors declare no conflicts of interest.
REFERENCES
- 1. Rogers LC, Armstrong DG, Capotorto J, Fife CE, Garcia JR, Gelly H, Gurtner GC, Lavery LA, Marston W, Neville R, Nusgart M, Ravitz K, Woelfel S. Wound center without walls: the new model of providing care during the COVID‐19 pandemic. Wounds. 2020. WNDS20200420‐1. (Online ahead of print.) [PMC free article] [PubMed]
- 2. Wang R, Peng Y, Jiang Y, Gu J. Managing chronic wounds during novel coronavirus pneumonia outbreak. Burns Trauma. 2020;8:tkaa016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Serra R, Grande R, Butrico L, Rossi A, Settimio UF, Caroleo B, Amato B, Gallelli L, de Franciscis S. Chronic wound infections: the role of Pseudomonas aeruginosa and Staphylococcus aureus . Expert Rev Anti Infect Ther. 2015;13(5):605‐613. [DOI] [PubMed] [Google Scholar]
- 4. Hollander JE, Carr BG. Virtually perfect? Telemedicine for COVID‐19. N Engl J Med. 2020;382:1679‐1681. [DOI] [PubMed] [Google Scholar]
- 5. Queen D, Harding K. COVID‐19 a short‐term challenge, telewound a lifetime change. Int Wound J. 2020;17(3):529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Zagaria O, Ruggiero A, Cinelli E, Marasca C, Monfrecola A, Fabbrocini G. Chronic cutaneous ulcers management in dermatologic department during COVID‐19 era. Int Wound J. 2020. doi: 10.1111/iwj.13385. (Online ahead of print). [DOI] [PMC free article] [PubMed] [Google Scholar]