

1. Letter to the editor
A 59-year-old woman with grade 2 obesity and a history of iodinated contrast media allergy, but without any other known comorbidity, was admitted to the Strasbourg University Hospital for severe dyspnea with a four-day history of fatigue, myalgia and a fever of up to 41 °C. When paramedics arrived at her home, the patient was in respiratory distress. Oxygen saturation was at 85% under 15 L/min of nasal oxygen, which required an immediate orotracheal intubation on-site.
Upon admission to the intensive care unit, oxygen saturation was 95% under FiO2 100%. Breath sounds were bilateral with bronchial rales. Laboratory tests revealed a slight neutrophilia (8.13 g/L), lymphopenia (0.73 g/L), a high biological inflammatory syndrome (C-reactive protein [CRP]: 114 mg/L). Prothrombin and activated partial thromboplastin times were normal. Liver function tests revealed a mild cytolysis (twice normal). The chest radiography showed bilateral diffuse ground-glass opacities that were consistent with a COVID-19 infection (Fig. 1A). A nasopharyngeal swab, using RT-PCR, tested positive for the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
Fig. 1.
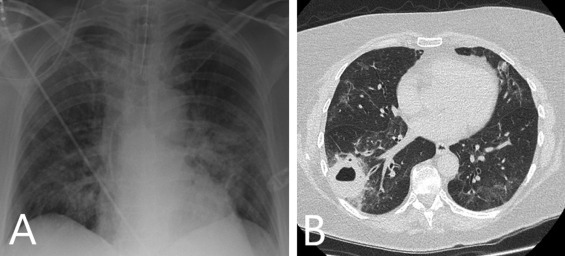
A. Chest radiography showing bilateral diffuse ground-glass opacities, which are consistent with a COVID-19 infection, four days after symptom onset. B. Axial chest CT, one month after symptom onset, revealing one pulmonary abscess in the right lower lobe, which is associated with sub-pleural bilateral ground-glass opacities that are consistent with partially resolved moderate-to-severe COVID-19 pneumonia.
Initial management consisted of treatment with lopinavir/ritonavir, combined with probabilistic intravenous amoxicillin-clavulanic acid and spiramycin for 5 days, with curative low-molecular weight heparin.
On day 7, two days after stopping antiviral and antibiotic treatments, the patient's respiratory condition deteriorated. A ventilator-associated pneumonia was suspected, despite negative results on all bacteriological respiratory samples and blood cultures. A nasopharyngeal swab and tracheal aspiration still revealed positive RT-PCR results for SARS-CoV-2. The patient then began 7-day probabilistic treatment with piperacillin-tazobactam and linezolid. Her respiratory status improved gradually, which enabled extubation on day 13.
On day 14, a nasopharyngeal swab and expectorations, using RT-PCR, tested negative for SARS-CoV-2.
On day 15, the patient was transferred to the pneumology department for further care and treatment. She had fully recovered rapidly, including the withdrawal of oxygen therapy, despite the persistence of bibasilar rales, without any other respiratory symptoms or fever. CRP decreased to 9.3 mg/L. Over the following days, chest radiography follow-up demonstrated a partial regression of the ground-glass opacities that were initially observed. Furthermore, diabetes mellitus was diagnosed during hospitalization (fasting glycemia 1.43 g/L [normal range, 0.74–1.06], glycated hemoglobin 6.7%).
Between days 8 and 25 of hospitalization, three specific serologies for SARS-CoV-2 were performed, all of which strongly demonstrated positive IgM and IgG levels (BIOSYNEX COVID-19 BSS rapid test, Strasbourg, France). The symptoms’ onset had occurred more than 10 days before the first serology, which can explain these results.
After day 24, the patient was discharged from hospital. But the day after, she experienced intermittent fever (peak temperature of 39.5 °C) and complained of a dry cough and abundant purulent sputum production (“vomica”) with halitosis. Her CRP rose to 219 mg/L. Chest radiography revealed the presence of diffuse bilateral ground-glass opacities and a rounded opacity surmounting the right diaphragm. A chest computed tomography (CT) scan revealed one pulmonary abscess (43 mm inner diameter) in the right lower lobe. This was associated with subpleural ground-glass opacities with basal and peripheral predominance and linear alveolar condensations, consistent with partially resolved moderate-to-severe COVID-19 pneumonia (involving approximately 50% of pulmonary parenchyma) (Fig. 1B). One RT-PCR test for SARS-CoV-2 on a nasopharyngeal swab returned weakly positive, but the next control samples remained negative.
All bacteriological cultures (expectorations, hemocultures), aspergillus serology, and antigenemia that were performed were negative. Maxillary sinuses and dental radiographies performed to investigate an extra-thoracic infectious cause were normal. A specific clinical evaluation found a mild dysphagia, which was probably secondary to the intubation.
Finally, the patient fully recovered after a 14 days-intravenous treatment with piperacillin-tazobactam and levofloxacin, followed with at home-treatment with amoxicillin-clavulanic acid and levofloxacin for seven more days (Fig. 2 ).
Fig. 2.
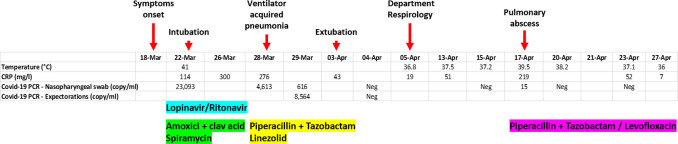
Patient's characteristics and results during hospitalization.
Clinical follow-up at one-month post-discharge revealed no symptoms and chest radiography was normalized.
Several studies and clinical observations have put forth the potential association between COVID-19 and high thrombotic risk [1]. The main thrombotic manifestations described until now include pulmonary embolism, acute coronary syndrome, and stroke. In our case, we did not perform a V/Q lung scintigraphy, believing that it would be hard to differentiate a pulmonary abscess from a pulmonary infarction, also regarding the presence of the bilateral diffuse COVID-19-related lung opacities. A lower limb venous doppler revealed no abnormalities. Low-molecular-weight heparin was initially prescribed at therapeutic dose within the 14 first days of hospitalization, then prescribed at preventive dose for the rest of the hospitalization stay. Although a pulmonary infarction could not be eliminated because of the patient's allergic comorbidities, a pulmonary abscess following a COVID-19 pneumonia remained our main diagnostic hypothesis.
Since the beginning of the COVID-19 epidemic was first described in China [2], bacterial and fungal superinfections after COVID-19 pneumonia have been described on multiple occasions [3], [4]. However, to our knowledge, this is the first case of a post-COVID-19 infection pulmonary abscess. In this case, several causes can explain the constitution mechanism of the abscess, including intubation-secondary vocal-cord dysfunction, which can be quite common. Strasbourg is in a part of France that has had an extremely high number of cases of COVID-19, since the epidemic started in late December. Our personal experience in the Strasbourg University Hospital suggests that many severe COVID-19 pneumonias are followed by bacterial superinfections, including ventilator-associated pneumonia. Whether these complications are a direct consequence of a specific COVID-19-related toxicity remains unknown.
What is remarkable here is that this complication occurred more than one month after symptom onset, and after the patient had initially fully recovered. She was treated with several empiric antibiotics and lopinavir/ritonavir (Fig. 2). This case confirms the need to be vigilant for late infectious complications after COVID-19 pneumonia, even after initial patient recovery. Otherwise, respiratory long-term sequelae of COVID-19, such as potential post-ARDS fibrotic abnormalities are unknown. We believe that patients that present with a severe form of COVID-19 pneumonia would benefit from a well-defined and specific follow-up after hospital discharge, including early clinical examination, chest CT, and pulmonary-function tests.
Disclosure of interest
The authors declare that they have no competing interest.
References
- 1.Bikdeli B., Madhavan M.V., Jimenez D., et al. COVID-19 and thrombotic or thromboembolic disease: implications for prevention, Antithrombotic Therapy, and Follow-Up: JACC State-of-the-Art Review. J Am Coll Cardiol. 2020;75:2950–2973. doi: 10.1016/j.jacc.2020.04.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Zhu N., Zhang D., Wang W., Li X., Yang B., Song J., et al. for the China Novel Coronavirus Investigating and Research Team A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020;382:727–773. doi: 10.1056/NEJMoa2001017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Duployez C., Le Guern R., Tinez C., et al. Panton-valentine leukocidin-secreting staphylococcus aureus pneumonia complicating COVID-19 [published online ahead of print, 2020 Apr 16] Emerg Infect Dis. 2020;26 doi: 10.3201/eid2608.201413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Blaize M., Mayaux J., Nabet C., et al. Fatal invasive aspergillosis and coronavirus disease in an immunocompetent patient [published online ahead of print, 2020 Apr 28] Emerg Infect Dis. 2020;26 doi: 10.3201/eid2607.201603. [DOI] [PMC free article] [PubMed] [Google Scholar]