

Abstract
The COVID-19 pandemic has presented a formidable challenge to care continuity for community mental health clients with serious mental illness and for providers who have had to quickly pivot the modes of delivering critical services. Despite these challenges, many of the changes implemented during the pandemic can and should be maintained. These include offering a spectrum of options for remote and in-person care, greater integration of behavioral and physical healthcare, prevention of viral exposure, increased collaborative decision-making related to long-acting injectable and clozapine use, modifying safety plans and psychiatric advance directives to include new technologies and broader support systems, leveraging natural supports, and integration of digital health interventions. This paper represents the authors’ collaborative attempt to both reflect the changes to clinical practice we have observed in CMHCs across the US during this pandemic and to suggest how these changes can align with best practices identified in the empirical literature.
Keywords: COVID-19 pandemic, Serious mental illness, Community mental health, Behavioral health treatment delivery, e-Mental health
Introduction
The current coronavirus disease 2019 (COVID-19) pandemic has required dramatic transformation of the delivery of outpatient mental health services for individuals with serious mental illness (SMI) in the US. Federal and state guidelines limit face-to-face contact and specifically request that health facilities limit in-person contact. This transformation in care delivery has tremendous public health implications, as individuals who receive care through the public mental health system are particularly vulnerable during public health crises (Druss 2020). Multiple factors contribute to increased risk of infection and poorer outcomes in this population, including disparities in access to healthcare, and increased risk of contracting COVID-19 due to social inequalities (e.g., increased rates of poverty leading to residential instability and food security, high unemployment rates), higher rates of medical conditions, and unhealthy behaviors (e.g., Chowkwanyun and Reed 2020). Moreover, the risk of poorer mental health outcomes is further exacerbated by the pandemic, and this must also be recognized as a public health priority (Williams and Cooper 2020). Since there is currently no vaccine or specific treatment for COVID-19, current health efforts focus on providing prevention and screening, ensuring access to appropriately intensive services for those with the most severe symptoms, and maintaining continuity of treatment for other chronic conditions (Adalja et al. 2020).
The pandemic presents a serious threat to the continuity of treatment for SMI. It is critical for community mental health centers (CMHCs) to develop plans to ensure that they can maintain essential services and adequate supplies of psychotropic medications. This paper aims to provide community mental health providers who are working with clients with SMI with practical recommendations for optimizing the continuity of care in the context of rapidly evolving mandates and recommendations for healthcare providers.
Transformation of Care in the COVID-19 Era
Clients with SMI who are served by CMHC outpatient and outreach teams may have chronically elevated risk of severe functional impairments, emergency department visits, psychiatric hospitalizations, harm behaviors, arrest and incarceration, food and water insecurity, and homelessness. During a public health crisis, these risk factors must be considered along with the individual’s risk of COVID-19 infection to determine how to best meet an individual’s treatment needs. Medical and psychiatric risks and benefits for every individual client should be weighed by the clinical team, with input from the medical director as needed, to decide if there is an urgent or essential need that necessitates in-person care and, if so, what modifications to care delivery are necessary. In addition, natural supports, warm lines, and pandemic-compatible psychiatric advance directives should become the standard of care in the peri- and post-COVID era.
Utilizing a Continuum of Modes of Service Delivery
Clinics should consider a spectrum of service delivery options that are responsive to clients’ needs and preferences for care as well as their psychiatric and medical risk status (see Fig. 1). These care delivery options are not mutually exclusive. Indeed, using a variety of care delivery methods in combination may support frequent contact without increasing the risk of client or staff exposure to the virus. The spectrum includes in-person care in the community with appropriate preventative measures; clinic-based care in a larger room that allows physical distancing; clinic-based telehealth, in which the client is accommodated in a private clinic office for a telepsychiatry session with their provider; clinic-based care in a standard office in a manner consistent with local public health guidelines; and telehealth encounters with clients at home or in the community. Clinic-delivered care can also be extended by coaching family members, establishing linkages to warm lines, and supplemental forms of e-mental health (for a review of e-mental health literature, see Lal and Adair 2014). Each of these options are reviewed below, followed by delineation of key considerations for care delivered in-person and by telehealth.
Fig. 1.
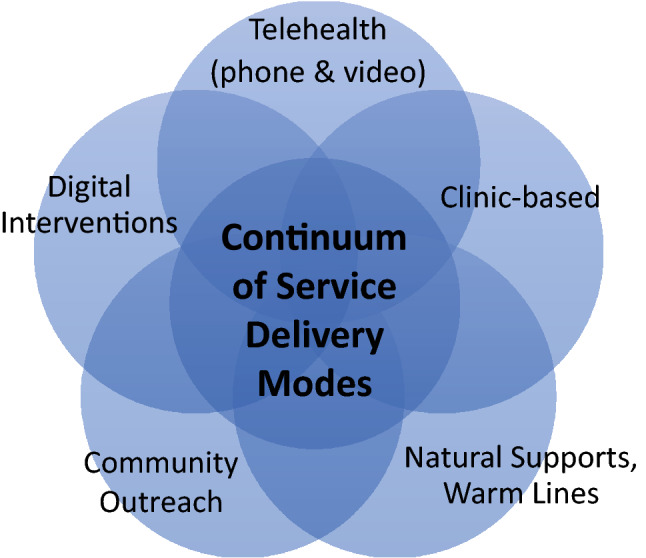
Continuum of service delivery modes for CMHC clients
While most CMHCs may be able to shift to telehealth practices for many clients, a significant group of clients will continue to need in-person services to help meet basic needs or because they lack access to the required technology or data plans required to engage in telehealth. But telehealth can be adapted to address technologic or psychosocial barriers. For instance, the client can present to clinic for a telehealth session in a private office, thereby minimizing close contact with clinic staff. Clients who present with cognitive disorganization or paranoia related to technology or surveillance may be amenable to telephone encounters, which represent an efficient, familiar alternative for clients, and hold greater pragmatic appeal to CMHCs in states that can now receive equitable compensation for certain types of telephone encounters (e.g., Washington State Emergency Order No. 20-02, 2020). Telephone encounters have limitations that impact clinical care, though, as they may limit clinical observation, therapeutic engagement, assessment, and interventions, further reinforcing the need to diversify therapeutic contacts.
In the short term during the pandemic, providers may need to temporarily shift from skills teaching and other rehabilitation efforts to direct assistance with basic needs. To this end, providers may need to coordinate with the client, natural supports, representative payees, faith communities, and social service organizations to locate resources, prepare care packages, and even prepare and drop off warm meals. Providers doing outreach visits should avoid entering homes, especially if it is a closed space or when others are in the residence and control over physical distancing is less certain. Outreach teams should meet outside the residence in well-ventilated areas, to visually assess how the person is doing, present as a familiar and comforting supportive social visit, model and reinforce behaviors, deliver medications, and provide an in-person demonstration of how to use smartphones or other devices to engage in e-mental health. With all in-person encounters, providers need to be familiar with and adhere to local public health infection control guidelines on personal protective equipment (PPE) and physical distancing.
Leveraging All Available Supports
In addition to a multimodal plan service delivery, care should also leverage all available members of the clinic staff, natural supports, and ancillary services, in an “all hands on deck” fashion. Administrative staff such as receptionists can make welfare phone calls to check on clients, or may be able to provide learning sessions to clients to prepare them for telehealth sessions. Peer specialists can continue to play a key role in supporting person-centered wellness management and coping skills, coaching and consultation to promote self-efficacy and self-advocacy, and problem-solving client needs. Peer specialists and case managers may be helpful in facilitating access to virtual spiritual, peer-based, recreational, and other communities to help clients connect with others. Therapists may replace or augment full clinical sessions in the short-term with telephone sessions intended to coach the client in the acquisition, strengthening, and rehearsal of specific behavioral skills in order to avert a behavioral crisis.
Natural Supports as Extensions of the Clinical Team
Families and caregivers may be in a position to support their loved one experiencing a mental illness, and are available more hours in a given day or week than the treatment team, especially if living with their loved one. Now, more than ever, providers need to enlist families as partners in care delivery. Providers can augment services by directing some of their efforts to natural supports, such as, skills they teach directly to individual clients. As a team, providers can work with both clients and families to plan for structuring their day, especially with leisure activities and opportunities for social connectedness while physical distancing. While this places demands on families, it may prove to be an important avenue for supplementing shorter clinical sessions, particularly with clients who are not engaging in video or phone sessions. Families can be further supported with cloud-based shared folders or other resources that contain educational and training materials (e.g., manuals, clinical tips sheets for family members) to supplement direct care. Additionally, many community mental health systems offer support from trained family specialists who have lived experiences with a loved one with mental illness who may be available to families during this time.
Warm Lines
For those who are not connected to family or other natural supports, providers will need to help identify and extend other natural supports available to the client. As long as physical distancing is necessary, virtual connections and online communities are even more key. Unlike hotlines or crisis lines, which are designed to be responsive to individuals in the throes of a psychiatric emergency, warm lines are designed to be a comforting option for people experiencing distress and seeking emotional support. The COVID-19 pandemic has led to the expansion of the availability of warm lines, many hosted by peer support organizations. A national crisis text service, Crisis Text Line, provides free confidential text message service for people in crisis (users can text HOME to 741741 to be connected to a crisis counselor). Some states have developed their own emotional support text lines, such as Call4Calm, a free-of-charge texting service made available by the Illinois Department of Human Services’ Mental Health Division to English and Spanish-speaking residents (Halstead 2020). Providers may wish to curate these resources, help input phone numbers into clients’ cell phones, and post them to agency websites or social media.
Establishing a COVID-Compatible Psychiatric Advance Directive
Providers should work with clients to update safety plans, and help clients to establish or update a psychiatric advance directive that includes contingency planning related to pandemics. Advance directives delineate an individual’s wishes in the event that they are unable to express their wishes for health care and treatments. Under federal law, facilities receiving CMS reimbursements are required to use advance directives, including for behavioral health conditions. The American Psychiatric Association’s SMI Adviser program (www.smiadviser.org) has released a digital version of a psychiatric advance directive, called My Mental Health Crisis Plan (SMI Advisor 2020) that meets the legal requirement for all 50 states and allows for tailoring to where the individual resides. Companion guidance documents to facilitate collaboration with both natural supports and providers to develop and execute the psychiatric advance directive are in development. As hospitals and crisis centers may be differentially impacted by the COVID-19 pandemic, individuals should factor in treatment setting to their advance directives. It is important to inform the client that it may not be possible to accommodate some aspects of their advance directive, given that circumstances and resources are quite fluid during this time. Providers should help to problem-solve around these contingencies in order to best ensure maximal application of the individual’s wishes within their psychiatric advance directive.
Telehealth in Community Mental Health Settings
The virtues of virtual care have been well-documented, as has its underutilization in public behavioral health (Schmeida et al. 2007; Simmons et al. 2005). Institutional and policy barriers to broad dissemination of telepsychiatry and digital health interventions (Saeed et al. 2012) are now being surmounted in response to emergent need. Federal policy shifts have also signaled widespread recognition that the flexible use of digital health technologies may be required to maintain uninterrupted mental health services during the COVID-19 crisis. For instance, the Office for Civil Rights (OCR) has announced that it would waive penalties embedded in the Health Insurance Portability and Accountability Act (HIPAA) against health care providers who serve their clients using “everyday communications technologies,” (Department of Health and Human Services 2020) although we are sensitive to the dialectic between reducing barriers to care and protecting patient rights (Hall and McGraw 2014).
Evidence suggests that the use of telepsychiatry (both via telephone and videoconferencing) is both feasible and acceptable for individuals with SMI, and may improve client outcomes (Baker et al. 2018; Kasckow et al. 2014). That said, research on telepsychiatry practice has typically involved rigorous implementation planning, support, and evaluation. In contrast, the urgent need to provide telehealth services quickly has resulted in clinical sites across the US scrambling to adopt new technology, workflows, job aids, and training for their providers who are simultaneously addressing emergent clinical needs. Clients may not have access to the hardware, software, or data plans required for telepsychiatry. Both staff and service users may require several learning sessions to become proficient enough for independent use. Key targets for assessment and management using telehealth modalities are discussed in the next section. Telepsychiatry practice guidelines are beyond the scope of this article, but can be accessed online (https://www.psychiatry.org/psychiatrists/practice/telepsychiatry/toolkit/practice-guidelines).
Key Targets for Assessment and Treatment During Telehealth Visits
Mental health providers will need to make the most of potentially limited time for assessment and treatment, as clients with psychosis may not be able to tolerate long sessions via phone or video call. Providers should aim to increase the frequency (and perhaps reduce the duration) of their client encounters (e.g., transition from one weekly 30-min session to twice weekly 15-min sessions). More frequent visits may provide greater opportunities for assessment of dynamic factors associated with increased risk of functional impairment, victimization, substance use, self-harm, violence, and change in housing or employment status. In addition, increased contact with members of the clinical team also provides more social contact during this period of physical distancing. Communication and building trust over the phone are particularly challenging with clients with significant thought disorganization and paranoia, and providers will need to skillfully interweave engagement, assessment, and intervention strategies. Providers may find it particularly difficult to assess and engage clients who are newly enrolled in services effectively via telehealth. A complete initial assessment and building a therapeutic relationship can be difficult over the phone. New clients may benefit most from at least an initial in-person visit to allow a more thorough intake assessment and diagnostic interview including physical observation and exam, as indicated. Telemedicine using videoconferencing is the second-best option for new clients, with telephone encounters being used as a stop gap. Notably, telehealth offers opportunities for environmental and interpersonal assessments that are not afforded during clinic visits, and these data may help to advance clients’ functional recoveries. Several targets for assessment and treatment should be prioritized for both new and existing clients, including safety assessment and management, psychological and pharmacotherapeutic strategies to manage psychiatric symptoms and co-occurring substance use disorders, assessment and management of physical health, and augmenting care by enlisting natural supports and employing asynchronous digital health interventions.
Safety Assessment
Comprehensive and effective community-based mental health treatment is essential to limit emergency room visits and inpatient psychiatric hospitalizations that increase risk of COVID-19 exposure and further overload the health care system. Along with clinic administrators, the medical director, and/or the risk management team, providers should weigh the risks and benefits of seeing a client who is at elevated risk of potentially lethal self-injurious behavior or violence toward others in-person versus via telehealth. Clients who are less familiar to the clinical team, for whom historical and clinical risk factors are particularly high, or who are newly expressing behavioral intent to harm self or others should be prioritized for in-person care with appropriate measures to reduce risk of infection (PPE, physical distancing, etc.). As hospital beds may be even more difficult to access and some traditional clinic-based services will be reduced, administrators may need to re-deploy some outpatient clinical staff to outreach and crisis response teams to enhance capacity for both proactive and reactive contact with clients in-need, with appropriate precautions for both clients and staff.
At the start of all telehealth and telephonic encounters, it is critical for the provider to obtain and document the client’s phone number and current location. The phone number is important for technological troubleshooting, (client cannot access videoconference, or gets disconnected). An exact address from which they are calling is important to provide enough detail to direct emergency services to the client’s location if necessary for a welfare check. It is imperative that safety plans are created and updated to ensure that all aspects of the plans are compatible with the restrictions in place in clients’ immediate environments. If the client already has a safety plan, efforts should be made to ensure that the client has easy access to the plan in multiple modalities and that all aspects of the plan are feasible. Depending on the nature of suicidal or homicidal ideation, distress tolerance will be most helpful to engage the client in down-regulation until the acute crisis remits. The My3 App (www.my3app.org) adapts an evidence-based strategy for safety planning to a print or mobile application (Stanley and Brown 2012). It is critically important for providers to identify triggers to suicidal urges; teach the client to look for affective, cognitive, or physiologic cues; and help the client to plan new responses when early warning signs emerge. Ideally, natural supports—particularly those who live with the client—will contribute to identifying early warning signs and assist with adherence to the safety plan, if the client agrees to their participation.
Key Psychotherapeutic Strategies
Excessive worry, anxious avoidance, and insomnia are prevalent to high degrees in individuals suffering from mood and psychotic symptoms, represent putative causal factors for psychosis, and are each treatable intervention targets (Freeman et al. 2019). In addition, poor self-regard—consisting of negative self-beliefs and low self-efficacy—are known correlates of both depression and psychosis (Freeman 2016; Sowislo and Orth 2013). These important targets of in-person cognitive behavioral treatments of mood and psychotic disorders can also be addressed via remote care. During times of stress and uncertainty, clients may lapse into former, maladaptive habits. As providers and clients become more proficient in the use of telehealth, their intervention strategies more closely approximate in-person care (e.g., resuming Prolonged Exposure for PTSD; Morland et al. 2020). In the interim, the priority during the public health crisis is to manage lapses in an effort to prevent relapse, acute decompensation, and risk behaviors.
Providers who are new to clients should rely heavily on befriending and engagement strategies before attempting to systematically intervene. Even among existing clients, befriending and engagement strategies should be the fallback if the client becomes more reluctant to discuss delusions and hallucinations (Kingdon and Turkington 2005) after transitioning to telehealth. While symptom management strategies should be tailored to individuals’ needs, preferences, and their ability to learn and practice new skills using e-mental health, all clients are likely to benefit from efforts to broaden their repertoire of distress tolerance skills for distressing beliefs and hallucinations, anxiety management strategies such as paced breathing, and behavioral activation, each of which are amenable to delivery in brief sessions (Wright et al. 2010) to help manage distressing emotions. Skills practice can be enhanced through virtual communities, websites, and—as detailed below—mobile health applications. As a transdiagnostic and translational model, CBT interventions for a variety of presenting problems can be delivered through telepsychiatry (McLay et al. 2020). CBT and DBT skills training can help clients sustain gains and experience relief from emergent symptoms (Matsumoto et al. 2018; Stubbings et al. 2013). Telehealth may also be beneficial in understanding and addressing environmental contributors to symptoms, reducing no shows, and even improving engagement. Although less studied, psychotherapy groups can also be offered through teletherapy (Backhaus et al. 2012), and some resources are available to support practitioners as they transition groups to videoconference (e.g., https://mhttcnetwork.org/).
Addressing Substance Urges and Use
Special attention should be given to individuals with substance use disorders, whether or not they were actively using substances prior to the pandemic. Individuals with a history of substance use are at elevated risk of relapse, and urges to use should be normalized, monitored, and addressed with appropriate environmental, motivational, behavioral, cognitive, and—if applicable—pharmacologic interventions. Individuals who are currently engaging in substance use may be particularly vulnerable to complications from COVID-19 due to disproportionate rates of homelessness and incarceration compared to those without substance use, drug seeking behaviors that put them in close contact with others, and also effects of certain drugs on the lungs and respiratory system. In addition, practitioners must be mindful of the elevated risk of withdrawal syndromes related to sudden disruptions in the drug supply chain or inability to access medication-assisted treatment (MAT). Symptoms of withdrawal syndromes vary based on the substance, but can include increased anxiety and agitation, tremors, nausea, difficulty sleeping, increased psychotic and mood symptoms, and increased suicidal ideation. The provider should alert the client to these effects of discontinuation and promote harm reduction practices to balance safe discontinuation and consumption of substances. Harm reduction approaches for clients with co-occurring substance use and psychiatric disorders during the COVID-19 crisis should include maintaining frequent contacts across remote modalities (videocalls, phone, and texting, as available), generous use of befriending and normalization strategies, education on safer options for drug administration and drug administration sites, as well as a review of available MAT options. In addition, providers can help clients develop strategies to promote safer social interactions that are acceptable to the client. Emotion regulation strategies and distress tolerance skills that focus on activating the parasympathetic nervous system should be the main focus for these clients. Among clients with cognitive impairment and/or disorganization, preference is given to depth over breadth to enhance overlearning. Providers should coach the client to independently administer one or two skills that are effective in reducing subjective units of anxiety (0–100%), rather than teaching a variety of these skills. Clients should also identify a natural support they can access for skills coaching if a member of the CMHC’s clinical team is not available for phone coaching, and that individual should be conferenced into remote clinical encounters whenever possible.
Medical Management
Community mental health providers are often the primary point of contact with the health care system for their clients with SMI and represent the first responders to the COVID-19 pandemic for many of these individuals. Medical management during this time should target prevention strategies for COVID-19 infection, management of physical health conditions in partnership with primary care and public health, support of smoking reduction or cessation, medication management, and lab monitoring.
Reducing COVID-19 Risk
Mental health providers need to be able to recognize the signs and symptoms of COVID-19 illness, educate clients about basic strategies to recognize symptoms, and translate public health recommendations in ways that are comprehensible and implementable by clients. Client-facing materials developed for general populations may need to be tailored to address limited health literacy (Farrell et al. 2020) and promote more harm reduction strategies to mitigate viral exposure. Providers can help clients problem-solve logistical barriers to reducing risks of infection, in some cases choosing among several options that are all associated with some risk. Many social services and settings on which clients rely (e.g., clubhouses, food pantries, shelters) may be temporarily unavailable or present an unacceptable level of risk of infection. Treatment plans that include clinic or pharmacy visits should specifically include strategies to reduce risk of COVID-19 infection. Risk mitigation strategies may be more challenging for some clients to implement due to cognitive challenges, interfering symptoms, and/or lack of skills on how to use or access key resources. As such, teams will need to translate CDC guidelines into more concrete behavior examples and use various means to model such behaviors visually. These may include demonstrating recommended hand washing techniques; personalized strategies for length of handwashing; use of disinfectant within the home, especially when living with others; specific guidance on how to navigate the environment if leaving the residence, such as understanding what more than six feet spatially looks like; application and removal of face masks; and modifying how one interacts with neighbors. Such teaching may occur in-person while standing outside of the residence, or could be reviewed through videoconference if telehealth is possible.
Coordination with Primary Care and Public Health
The mental health team should be aware of each client’s PCP or help them establish care. It is important to coordinate with primary care, communicate about new respiratory symptoms, and advocate for evaluation and COVID-19 testing as indicated. Clients with respiratory symptoms should be advised to call PCP or ER ahead rather than just showing up. In addition, coordinating with PCP and specialists may be needed to ensure ongoing treatment of chronic medical conditions in the midst of increased system strain and/or office closures, particularly for conditions that are correlated with a more severe coronavirus illness course (Hu et al. 2020). Clients without housing, phones, or computers will face particular challenges getting their medical care needs met. Behavioral health providers making outreach visits can be trained to assess vital signs. In some cases, funds have been allocated for purchasing communication hardware and/or data plans for clients in need. County and state public health departments are a resource for guidance on PPE recommendations in different settings, access to COVID testing, and may have quarantine sites for those who are homeless or do not have sufficient space to isolate. Public health departments should be contacted when clients are positive for COVID, particularly if the client may have trouble following isolation guidelines secondary to impaired insight or judgment. Public health may elect to conduct contact tracing and consider clients interactions at a mental health center, housing unit, or shelter.
Support of Smoking Cessation
Smoking increases both the risk of contracting COVID-19 and the severity of illness. Because the coronavirus targets the lungs, there is an increased urgency to quit smoking or vaping, or at least reduce use. This is an excellent time for mental health providers to focus on clients’ efforts to quit. Multiple medications are both effective in promoting smoking cessation among people with psychosis, and safe to use (not associated with increased risk of adverse neuropsychiatric side effects). In large clinical trials, varenicline appears to be the most effective medication to support smoking cessation among people with psychosis, but bupropion and nicotine replacement are also effective (Anthenelli et al. 2016). Combination nicotine therapy should also be considered, as this may increase the likelihood of success (Stead et al. 2012). The clinical team should be apprised when pharmacotherapeutic interventions for smoking cessation are initiated, as mood and suicidal ideation should be monitored. Clients should be advised that support is available through phone and texting services from 1-800-QUIT-NOW (1-800-784-8669), a free national phone service that routes the caller to the state line associated with caller’s area code, and resources are also available from the American Lung Association, 1-800-LUNG-USA (1-800-586-4872), and the National Cancer Institute (877-44U-QUIT (877-448-7848). In addition, there are a multitude of online resources to connect people to support groups and recommendations, including a government-sponsored website with information in English and Spanish for adults and teenagers who smoke (Smokefree: Home) and a site from the American Lung Association, with a variety of tools to help quit both smoking and vaping (Freedom From Smoking). Apps may be particularly useful at this time. MyQuit Coach offers different approaches to quitting smoking and community support. Smoke Free provides 20 different techniques to quitting smoking, plus options and graphs to track cravings.
Medication Management
Virtual medication management visits should also be considered, as in-person visits pose a health risk not only to clients and providers, but also to elderly or medically-compromised individuals who live with clients or accompany them to clinic visits. There are unique challenges for telepsychiatry medication management visits for the treatment of psychosis and, to the extent possible, these should include video assessment. First, the evaluation of most medication side effects—including akathisia, Parkinsonism, dystonic reactions, and tardive dyskinesia—is limited to self-report in telephone encounters. Metabolic self-monitoring should be encouraged, especially among antipsychotic-naïve clients starting their first medication trial. Clients with scales at home can weigh themselves and report these measures to the psychiatric care provider or nurse during the virtual encounter. Second, the pandemic increases the risk of disruption to pharmacotherapy treatments. Psychiatric care providers should review medication adherence and work with clients to ensure that they have an adequate supply of all both psychiatric and medical prescriptions, and a plan for refilling medications. The risks and benefits of a large supply of potentially lethal medications such as lithium or tricyclic antidepressants need to be weighed. Weekly medication dispensing is still recommended for clients at high risk for suicide. For clients who have medications dispensed or observed weekly or more often, psychiatric providers might consider changing this medication support from in-person visits to daily phone calls. Family support in picking up medications, pharmacy delivery services, and outreach by CMHC staff to drop off medications while observing from a safe distance are options to consider.
There are two groups of clients who require special considerations with respect to pharmacotherapy management: those receiving long-acting injectable (LAI) antipsychotic medications and those receiving clozapine. Injections require physical proximity, yet proper PPE may not be reliably available to CMHC providers. Clinics should provide large, well-ventilated areas for the administration of intramuscular injections and nurses should follow local PPE recommendations. It may be feasible to move clients from biweekly injections to other similar injectable formulations that can be given every 4 weeks, or even every 12 weeks. Alternatives to in-person visits for LAIs should be considered on a case-by-case basis, as some clients may be able to tolerate a switch to oral medications during the period of reduction of in-clinic services, particularly if coupled with support from family or other natural or housing supports.
There are several challenges in continuing high-quality clozapine treatment. Treatment with clozapine in the pre-pandemic period required regular absolute neutrophil count (ANC) monitoring (weekly for 6 months, then bi-weekly for 6 months, then monthly for the duration of treatment) to reduce the risk of a potentially life-threatening side effect of severe neutropenia. In the context of COVID-19, the Clozapine Risk Evaluation and Management Strategy (REMS)—the FDA-mandated national program for reporting and monitoring clozapine treatment and adverse events—has published new guidelines for ANC monitoring. The goal is to reduce the risk of contracting and/or transmitting COVID-19 through laboratory visits (Clozapine Product Manufacturers Group 2020). The revised guidelines allow clients to continue receiving clozapine without a current ANC. Frequency of ANC monitoring for any client should be determined using a shared decision-making process and should consider the risk of contracting COVID in their community, the individual’s risk of poor prognosis due to age and chronic medical conditions, their need to isolate due to COVID-19 diagnosis or recent exposure, and their risk of severe neutropenia. At a minimum, clients should always be screened for COVID-19 symptoms before in-person visits at the clinic or the lab. In most cases, it would be prudent to continue monitoring clients at their assigned frequency if their ANCs have fallen below normal thresholds within the past 6 months, or respective criteria for benign ethnic neutropenia (https://www.clozapinerems.com/CpmgClozapineUI/rems/pdf/resources/ANC_Table.pdf). Given that the highest risk for severe neutropenia is within 6 months of clozapine initiation, clients in this phase warrant strong consideration for continued regular monitoring. For clients in biweekly or monthly phases of ANC monitoring, the low risk of severe neutropenia makes a decision to forego regular monitoring a reasonable alternative, however a careful risk/benefit evaluation needs to be conducted for each individual client. A decision to consider pausing ANC monitoring for those no longer in weekly monitoring is consistent with a recently published consensus statement on the use of clozapine during the COVID-19 pandemic (Siskind et al. 2020). Along with reducing the ANC testing frequency, it may be appropriate to increase the dispensed amount of clozapine up to 90-day supplies, based on a careful safety assessment of the individual client, with additional consideration of local pharmacy practices and insurance approval. Additional challenges when initiating clozapine include monitoring vital signs for orthostatic hypotension and tachycardia, and monitoring for the increased risk of myocarditis. During the first month, serial troponins and C-reactive protein (CRP) should be added to the weekly blood draw. Lab monitoring should be accompanied by a targeted review of systems for myocarditis (e.g. chest pain, dyspnea, weakness, fever) and screening for other common side effects such as constipation, dizziness, weight gain, and sialorrhea. Finally, it is important to remind clients taking clozapine for any duration that fever is a symptom shared with both severe neutropenia and COVID-19, and that if they develop a fever, they require urgent laboratory testing in order to rule out clozapine-associated neutropenia.
Other Lab Monitoring
In routine pharmacotherapy, lab tests are often required to measure therapeutic drug levels, monitor for renal or hepatic impairment, and screen and monitor for other side effects, including adverse metabolic effects. Such monitoring may also be disrupted during the COVID-19 pandemic, requiring adjustments to treatment. A client’s laboratory may not be open or have reduced hours, or they may face barriers to getting to the lab. The psychiatric care provider and team should work with the client to weigh risks and benefits of each test for continued monitoring and consider the feasibility of alternative medications that do not require monitoring.
Augmenting Care with e-Mental Health
Even among clients who maintain ongoing services through multiple modes of care, as outlined above, behavioral health care can be enhanced or extended with asynchronous or self-guided technologies, including online resources and communities, technology-focused treatment adaptations, text messaging interventions, and provider-supported use of mobile health (mHealth) apps (Andersson and Cuijpers 2009). First, providers may extend services by coaching clients to access curated online resources, such as those offered by health-related, government, non-profits and advocacy organizations (e.g., Mental Health America 2020; National Alliance on Mental Illness 2020; Centers for Disease Control and Prevention 2020). Second, providers may consider adapting typical treatment strategies in a manner that involves increased client engagement with ordinary technologies, such as social media, videoconferencing platforms, or email, providing education and learning aids when necessary. Other digital technologies such as smartphone applications can be used for direct mental health services, but the effectiveness of these interventions is enhanced by human support (Mohr et al. 2011).
Text messaging is highly accessible to individuals with serious mental illness. Many individuals with SMI own a device capable of texting (Campbell et al. 2015), and they use this feature at rates similar to the general population (Noel et al. 2019). Text messaging has been repurposed to encourage illness management (Granholm et al. 2012), support medication adherence (Montes et al. 2012), and most recently, to provide ongoing therapeutic interaction with a designated member of the clinical team, i.e. a “mobile interventionist” (Ben-Zeev et al. 2014). While text messaging offers the advantages of familiarity, ubiquity, and efficiency (Schwebel and Larimer 2018), administrators must develop policies and procedures related to SMS treatment guidelines prior to implementation and clinical adoption. Providers should always use secure, encrypted platforms, establish protocols to protect client privacy, establish clear communication to clinic staff and clients about the parameters of text messaging (e.g., whether or not 24/7 access is available), and obtain informed consent when using text messaging. Establishing these prerequisites in a CMHC that has not offered text messaging may take some time, but the asynchronous communication of text messages has several advantages. Using this medium, providers can maintain ongoing interactions with multiple clients, and clients can access support in a discrete manner.
Other forms of digital health technologies allow clients to self-deliver evidence-based interventions. A growing body of research supports the use of smartphone apps to provide clients ongoing access to interventions. Unfortunately, a few of the apps with the strongest evidence that have been designed specifically for users with serious mental illness are not yet publicly available. Two such interventions—FOCUS (Ben-Zeev et al. 2018), which targets schizophrenia self-management, and PRIME (Schlosser et al. 2018), which targets social connection and depressive symptoms—have demonstrated efficacy and high rates of engagement in randomized trials. However, recent developments may assist providers in choosing an mHealth app for other clinical concerns—e.g. anxiety, insomnia, mindfulness—in the immediate term. PsyberGuide (Neary and Schueller 2018) is a non-profit project that publishes ratings of digital health apps along several categories, including credibility (e.g., the strength of empirical evidence for the app and its interventions), user experience (e.g., the design and overall experience for users), and transparency (e.g., clarity of an app’s policies protecting user data, PsyberGuide 2018). Mindtools.io (MindTools.io 2020) similarly provides ratings of popular digital mental health apps according to quality, credibility, research evidence, and security. Providers can use these resources to better advise clients that are looking for mHealth support tools to use during disrupted clinical services.
Discussion
The COVID-19 pandemic has indelibly shaped our healthcare system and our world. Community mental health clinics are demonstrating resilience in the face of a mass trauma, and systems have the opportunity to experience posttraumatic growth as we begin to emerge from the pandemic. Many of the changes that are being implemented to maintain care continuity during the pandemic can and should be maintained—at least in part—in its wake. Experts are projecting that we will continue to see broader adoption of and applications for technology in behavioral health care moving forward (Ben-Zeev 2020) and that this new, more flexible and technology-enhanced model of care can benefit our clients’ functional recoveries (Ben-Zeev et al. 2019) and may help to redress the mental healthcare disparities for underserved and marginalized populations (Schueller et al. 2019). These include greater flexibility and creativity in the way that care is delivered, with a spectrum of options for remote and in-person care; greater integration of behavioral health and physical healthcare for existing conditions; tertiary prevention of contagious illnesses due to increased risk of exposure and deleterious health effects; increased collaboration and shared decision-making related to LAI and clozapine use; updating safety plans and psychiatric advance directives to include new technologies and broader support systems; greater inclusion of natural supports; and integration of digital health interventions to treat primary and secondary psychiatric symptoms. To limit interpersonal contact, healthcare providers are rapidly pivoting to telehealth, encouraged by new Centers for Medicaid and Medicare Services’ reimbursement codes for telehealth services (Centers for Medicare & Medicaid Services 2020). Notably, CMHCs in states that have not elected to expand Medicaid may consequently have more limited access to the practices and resources recommended here and may, as a result, observe higher rates of care discontinuity and/or poorer clinical outcomes during the pandemic response.
Providers and administrators have climbed a steep learning curve in a short timeframe. Given that experts are projecting recurrent outbreaks, healthcare providers and mental health administrators will want to establish decision trees for determining medical, psychiatric, and social risks to diverse CMHC clients with corresponding care delivery options that balance risk to the individual, the clinical team, and the public. In particular, greater penetration of e-mental health may address both acute needs during the COVID-19 crisis and chronic needs after the crisis subsides. Policy makers and clinical administrators should attend not only to the emergent clinical gaps of today but also ways in which COVID-related changes might inform future sustainable workflows, which will be particularly important if outbreaks are recurrent.
Funding
Dr. Buck is currently supported by a career development award also from NIMH (K23MH122504) as well as a NARSAD Young Investigator Award from the Brain and Behavior Foundation.
Compliance with Ethical Standards
Ethical Approval
In the past 3 years, Dr. Jarskog has received research grant funding from Auspex/Teva, Boehringer-Ingelheim, and Otsuka; he has served as a consultant to UpToDate and Bracket. No other authors have conflicts of interest to disclose. All authors certify responsibility for the content of this article. This work does report on research involving human participants or animal subjects and did not require ethical approval from an Institutional Review Board.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- Adalja AA, Toner E, Inglesby TV. Priorities for the US health community responding to COVID-19. JAMA: The Journal of the American Medical Association. 2020 doi: 10.1001/jama.2020.3413. [DOI] [PubMed] [Google Scholar]
- Andersson G, Cuijpers P. Internet-based and other computerized psychological treatments for adult depression: A meta-analysis. Cognitive Behavioral Therapy. 2009;38(4):196–205. doi: 10.1080/16506070903318960.917833314. [DOI] [PubMed] [Google Scholar]
- Anthenelli RM, Benowitz NL, West R, St Aubin L, McRae T, Lawrence D, Ascher J, et al. Neuropsychiatric safety and efficacy of varenicline, bupropion, and nicotine patch in smokers with and without psychiatric disorders (EAGLES): A double-blind, randomised, placebo-controlled clinical trial. The Lancet. 2016 doi: 10.1016/s0140-6736(16)30272-0. [DOI] [PubMed] [Google Scholar]
- Backhaus A, Agha Z, Maglione ML, Repp A, Ross B, Zuest D, Rice-Thorp NM, et al. Videoconferencing psychotherapy: A systematic review. Psychological Services. 2012;9(2):111–131. doi: 10.1037/a0027924. [DOI] [PubMed] [Google Scholar]
- Baker AL, Turner A, Beck A, Berry K, Haddock G, Kelly PJ, Bucci S. Telephone-delivered psychosocial interventions targeting key health priorities in adults with a psychotic disorder: Systematic review. Psychological Medicine. 2018;48(16):2637–2657. doi: 10.1017/S0033291718001125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ben-Zeev, D. (2020). The digital mental health genie is out of the bottle. Psychiatric Services. [DOI] [PubMed]
- Ben-Zeev D, Brian RM, Jonathan G, Razzano L, Pashka N, Carpenter-Song E, Drake RE, et al. Mobile health (mHealth) versus clinic-based group intervention for people with serious mental illness: A randomized controlled trial. Psychiatric Services. 2018;69(9):978–985. doi: 10.1176/appi.ps.201800063. [DOI] [PubMed] [Google Scholar]
- Ben-Zeev D, Buck B, Kopelovich S, Meller S. A technology-assisted life of recovery from psychosis. NPJ Schizophrenia. 2019;5(1):1–4. doi: 10.1038/s41537-019-0083-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ben-Zeev D, Kaiser SM, Krzos I. Remote “hovering” with individuals with psychotic disorders and substance use: Feasibility, engagement, and therapeutic alliance with a text-messaging mobile interventionist. Journal of Dual Diagnosis. 2014;10(4):197–203. doi: 10.1080/15504263.2014.962336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Campbell B, Caine K, Connelly K, Doub T, Bragg A. Cell phone ownership and use among mental health outpatients in the USA. Personal and Ubiquitous Computing. 2015;19(2):367–378. doi: 10.1007/s00779-014-0822-z. [DOI] [Google Scholar]
- Centers for Disease Control and Prevention. (2020). Stress and coping. CDC.gov. Retrieved from https://www.cdc.gov/coronavirus/2019-ncov/daily-life-coping/managing-stress-anxiety.html
- Centers for Medicare & Medicaid Services. (2020). Medicare telemedicine health care provider facts. CMS.gov. Retrieved from https://www.cms.gov/newsroom/fact-sheets/medicare-telemedicine-health-care-provider-fact-sheet
- Chowkwanyun, M., & Reed Jr, A. L. (2020). Racial health disparities and COVID-19—Caution and context. New England Journal of Medicine. [DOI] [PubMed]
- Clozapine Product Manufacturers Group. (2020). What is the Clozapine REMS program? Clozapine REMS Program. Retrieved from https://www.clozapinerems.com/CpmgClozapineUI/home.u#
- Department of Health and Human Services (2020). OCR announces notification of enforcement discretion for telehealth remote communications during the COVID-19 nationwide public health emergency. Retrieved from https://www.hhs.gov/about/news/2020/03/17/ocr-announces-notification-of-enforcement-discretion-for-telehealth-remote-communications-during-the-covid-19.html
- Druss BG. Addressing the COVID-19 pandemic in populations with serious mental illness. JAMA Psychiatry. 2020 doi: 10.1001/jamapsychiatry.2020.0894. [DOI] [PubMed] [Google Scholar]
- Farrell SJ, Dunn M, Huff J, Psychiatric Outreach Team, & Royal Ottawa Health Care Group Examining health literacy levels in homeless persons and vulnerably housed persons with mental health disorders. Community mental health journal. 2020;56(4):645–651. doi: 10.1007/s10597-019-00525-2. [DOI] [PubMed] [Google Scholar]
- Freeman D. Persecutory delusions: A cognitive perspective on understanding and treatment. The Lancet Psychiatry. 2016;3(7):685–692. doi: 10.1016/S2215-0366(16)00066-3. [DOI] [PubMed] [Google Scholar]
- Freeman D, Taylor KM, Molodynski A, Waite F. Treatable clinical intervention targets for patients with schizophrenia. Schizophrenia Research. 2019;211:44–50. doi: 10.1016/j.schres.2019.07.016. [DOI] [PubMed] [Google Scholar]
- Granholm E, Ben-Zeev D, Link PC, Bradshaw KR, Holden JL. Mobile assessment and treatment for schizophrenia (MATS): A pilot trial of an interactive text-messaging intervention for medication adherence, socialization, and auditory hallucinations. Schizophrenia Bulletin. 2012;38(3):414–425. doi: 10.1093/schbul/sbr155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hall, J. L., & McGraw, D. (2014). For telehealth to succeed, privacy and security risks must be identified and addressed. Health Affairs. Retrieved from https://www.healthaffairs.org/doi/full/10.1377/hlthaff.2013.0997 [DOI] [PubMed]
- Halstead, M. (2020). Stressed over COVID-19? Text new hotline for help from local counselors. The Southern Illinoisan. Retrieved from https://thesouthern.com/news/local/stressed-over-covid-19-text-new-hotline-for-help-from-local-counselors/article_7faa59f1-6296-568e-9c3c-90df43b80f89.html
- Hu Y, Sun J, Dai Z, Deng H, Li X, Huang Q, Wu Y, et al. Prevalence and severity of coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis. Journal of Clinical Virology. 2020;127:104371. doi: 10.1016/j.jcv.2020.104371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kasckow J, Felmet K, Appelt C, Thompson R, Rotondi A, Haas G. Telepsychiatry in the assessment and treatment of schizophrenia. Clinical Schizophrenia & Related Psychoses. 2014;8(1):21–27A. doi: 10.3371/CSRP.KAFE.021513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kingdon DG, Turkington D. Cognitive therapy of schizophrenia: Guides to evidence-based practice. New York: Guilford; 2005. pp. 234–239. [Google Scholar]
- Lal S, Adair CE. E-Mental health: A rapid review of the literature. Psychiatric Services. 2014;65(1):24–32. doi: 10.1176/appi.ps.201300009. [DOI] [PubMed] [Google Scholar]
- Matsumoto K, Sutoh C, Asano K, Seki Y, Urao Y, Yokoo M, Takanashi R, et al. Internet-based cognitive behavioral therapy with real-time therapist support via videoconference for patients with obsessive-compulsive disorder, panic disorder, and social anxiety disorder: Pilot single-arm trial. Journal of Medical Internet Research. 2018 doi: 10.2196/12091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLay L, Sutherland D, Machalicek W, Sigafoos J. Systematic review of telehealth interventions for the treatment of sleep problems in children and adolescents. Journal of Behavioral Education. 2020 doi: 10.1007/s10864-020-09364-8. [DOI] [Google Scholar]
- Mental Health America. (2020). Mental health and COVID-19—Information and resources. Mental Health America, Inc. Retrieved from https://mhanational.org/covid19
- MindTools.io. (2020). About MindTools.io. Retrieved 2020, from https://mindtools.io/about-mindtools-io/
- Mohr DC, Cuijpers P, Lehman K. Supportive accountability: A model for providing human support to enhance adherence to eHealth interventions. Journal of Medical Internet Research. 2011;13(1):e30. doi: 10.2196/jmir.1602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Montes JM, Medina E, Gomez-Beneyto M, Maurino J. A short message service (SMS)-based strategy for enhancing adherence to antipsychotic medication in schizophrenia. Psychiatry Research. 2012;200(2–3):89–95. doi: 10.1016/j.psychres.2012.07.034. [DOI] [PubMed] [Google Scholar]
- Morland LA, Mackintosh M, Glassman LH, Wells SY, Thorp SR, Rauch SAM, Cunningham PB, et al. Home-based delivery of variable length prolonged exposure therapy: A comparison of clinical efficacy between service modalities. Depression and Anxiety. 2020;37(4):346–355. doi: 10.1002/da.22979. [DOI] [PubMed] [Google Scholar]
- National Alliance on Mental Illness. (2020). COVID-19 information and resources. NAMI.org. Retrieved from https://www.nami.org/Support-Education/NAMI-HelpLine/COVID-19-Information-and-Resources
- Neary M, Schueller SM. State of the field of mental health apps. Cognitive and Behavioral Practice. 2018;25(4):531–537. doi: 10.1016/j.cbpra.2018.01.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Noel VA, Acquilano SC, Carpenter-Song E, Drake RE. Use of mobile and computer devices to support recovery in people with serious mental illness: Survey study. JMIR Mental Health. 2019;6(2):e12255. doi: 10.2196/12255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- PsyberGuide. (2018). App Guide. Retrieved 2020, from https://www.psyberguide.org/apps/
- Saeed SA, Bloch RM, Diamond JM. Telepsychiatry: Overcoming barriers to implementation. Current Psychiatry. 2012;11(12):28. [Google Scholar]
- Schlosser DA, Campellone TR, Truong B, Etter K, Vergani S, Komaiko K, Vinogradov S. Efficacy of PRIME, a mobile app intervention designed to improve motivation in young people with schizophrenia. Schizophrenia Bulletin. 2018;44(5):1010–1020. doi: 10.1093/schbul/sby078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schmeida M, McNeal R, Mossberger K. Policy determinants affect telehealth implementation. Telemedicine Journal and e-Health. 2007;13(2):100–107. doi: 10.1089/tmj.2006.0017. [DOI] [PubMed] [Google Scholar]
- Schueller SM, Hunter JF, Figueroa C, Aguilera A. Use of digital mental health for marginalized and underserved populations. Current Treatment Options in Psychiatry. 2019;6(3):243–255. doi: 10.1007/s40501-019-00181-z. [DOI] [Google Scholar]
- Schwebel FJ, Larimer ME. Using text message reminders in health care services: A narrative literature review. Internet interventions. 2018;13:82–104. doi: 10.1016/j.invent.2018.06.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simmons SC, Eccleston A, Saeed SA, Leonhardt GG, Lancaster M. The need for telepsychiatry and e-mental health in publicly-funded mental health systems. Psychiatrist Administrator. 2005;5(2):30–35. [Google Scholar]
- Siskind D, Honer WG, Clark S, Correll CU, Hasan A, Howes O, Kane JM, et al. Consensus statement on the use of clozapine during the COVID-19 pandemic. Journal of Psychiatry & Neuroscience: JPN. 2020;45(4):200061–200061. doi: 10.1503/jpn.200061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- SMI Advisor. (2020). My mental health crisis plan. (1.0.1) [Mobile app]. Google Play. Retrieved from https://play.google.com/store/apps/details?id=org.smiadviser.apa&hl=en_US
- Sowislo JF, Orth U. Does low self-esteem predict depression and anxiety? A meta-analysis of longitudinal studies. Psychological Bulletin. 2013;139(1):213–240. doi: 10.1037/a0028931. [DOI] [PubMed] [Google Scholar]
- Stanley B, Brown GK. Safety planning intervention: A brief intervention to mitigate suicide risk. Cognitive and Behavioral Practice. 2012;19(2):256–264. doi: 10.1016/j.cbpra.2011.01.001. [DOI] [Google Scholar]
- Stead LF, Perera R, Bullen C, Mant D, Hartmann-Boyce J, Cahill K, Lancaster T. Nicotine replacement therapy for smoking cessation. Cochrane Database of Systematic Reviews. 2012;11:CD000146. doi: 10.1002/14651858.CD000146.pub4. [DOI] [PubMed] [Google Scholar]
- Stubbings DR, Rees CS, Roberts LD, Kane RT. Comparing in-person to videoconference-based cognitive behavioral therapy for mood and anxiety disorders: Randomized controlled trial. Journal of Medical Internet Research. 2013;15(11):e258. doi: 10.2196/jmir.2564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Washington State Office of Insurance Commissioner (2020). Emergency Order No. 20-02. Retrieved from https://www.insurance.wa.gov/sites/default/files/documents/emergency-order-20-02_3.pdf?utm_content=&utm_medium=email&utm_name=&utm_source=govdelivery&utm_term=
- Williams DR, Cooper LA. COVID-19 and health equity—A new kind of “herd immunity”. JAMA. 2020 doi: 10.1001/jama.2020.8051. [DOI] [PubMed] [Google Scholar]
- Wright JH, Sudak DM, Turkington D, Thase ME. High-yield cognitive-behavior therapy for brief sessions: An illustrated guide. Philadelphia: American Psychiatric Publishing; 2010. [DOI] [PubMed] [Google Scholar]