

Rapid spread of the new disease COVID-191 led to unprecedented need for timely information on clinical manifestations, management options, and treatment of affected patients. COVID-19 has several unique features including viral pneumonia, high inflammatory response, and significant increase in thrombotic complications.2 Direct endothelial viral infection causes diffuse microvascular thrombosis,3 mostly present in the lungs and skin.4 Skin manifestations include erythematous rash, widespread urticaria, and chickenpox-like vesicles.5 Several reports described skin changes of the lower extremities and the so-called COVID toes, but only one publication described upper extremity manifestations.6 We present an image of left hand digital ischemia secondary to COVID-19 infection. The patient's consent was obtained for publication.
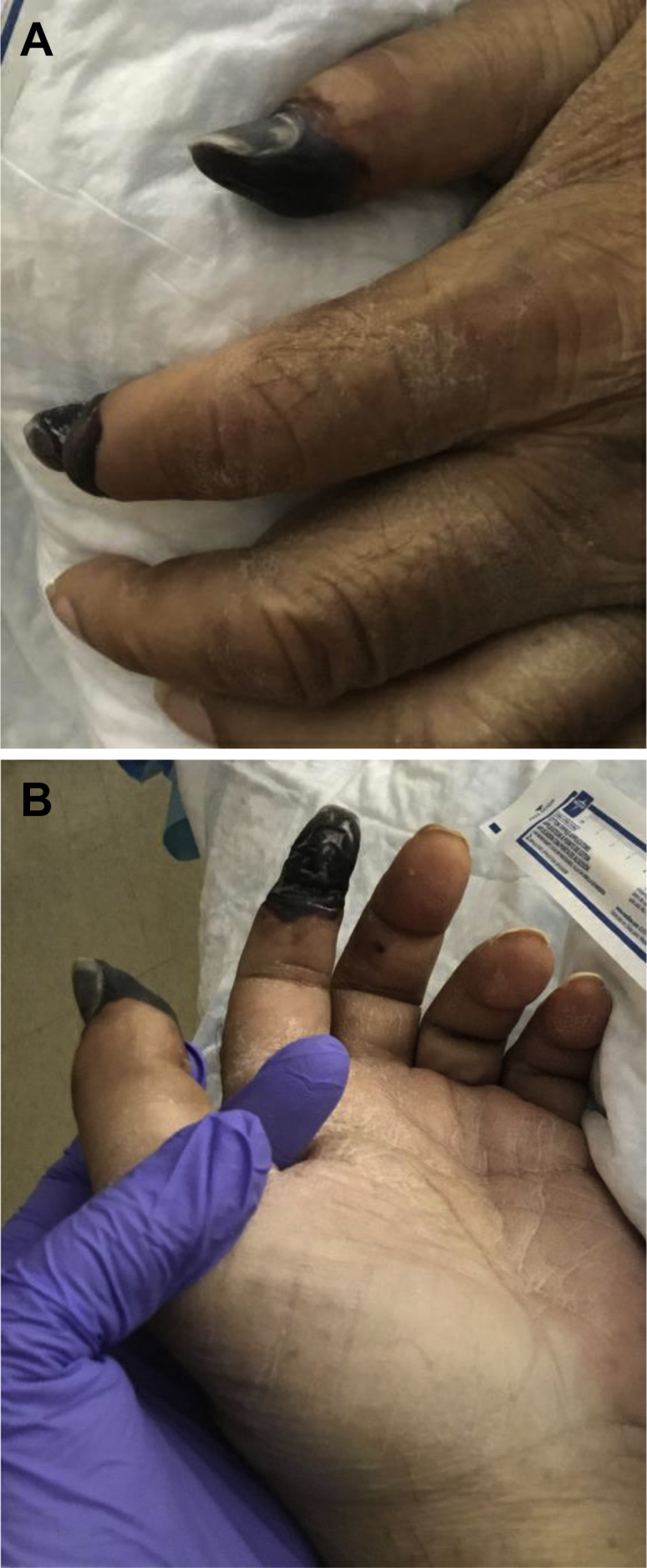
A 65-year-old male former smoker with history of hypertension presented with complaints of shortness of breath. The patient acutely decompensated, requiring intubation. He was found to be SARS-CoV-2 positive. During hospitalization, progressive left hand ischemic changes were noted involving the distal first and second digits (A and B). The patient had no prior history of cardiac arrhythmia, embolic events, vasculitis, Raynaud disease, or illicit drug use. On physical examination, the patient had palpable radial and ulnar pulses. There were no additional areas of digital ischemic changes or necrosis present. To limit exposure, noninvasive vascular studies were unable to be obtained. Weight-based enoxaparin administration was begun shortly after admission and has continued throughout hospitalization. No additional digital ischemia was seen in this patient outside of the first and second digits. In addition, the patient was not receiving vasopressor support at the time the digital ischemia was identified.
The patient's D-dimer level was elevated on presentation at 790 ng/mL and continued a trend upward until reaching a peak at 2089 ng/mL. Ultimately, the D-dimer level reached a plateau at approximately 850 ng/mL.
As digital ischemia is a common consultation for the vascular surgeon, it is important to recognize that patients diagnosed with COVID-19 may show signs of digital ischemia with otherwise normal findings on vascular examination.
Footnotes
This work was funded by the Conrad and Caroline Jobst Foundation.
Author conflict of interest: none.
The editors and reviewers of this article have no relevant financial relationships to disclose per the Journal policy that requires reviewers to decline review of any manuscript for which they may have a conflict of interest.
References
- 1.World Health Organization Coronavirus disease (COVID-19) pandemic. Available at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019.
- 2.Klok F.A., Kruip M.J., van der Meer N.J., Arbous M.S., Gommers D.A., Kant K.M. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb Res. 2020;191:145–147. doi: 10.1016/j.thromres.2020.04.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Varga Z., Flammer A.J., Steiger P., Haberecker M., Andermatt R., Zinkernagel A.S. Endothelial cell infection and endotheliitis in COVID-19. Lancet. 2020;395:1417–1418. doi: 10.1016/S0140-6736(20)30937-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Magro C., Mulvey J.J., Berlin D., Nuovo G., Salvatore S., Harp J. Complement associated microvascular injury and thrombosis in the pathogenesis of severe COVID-19 infection: a report of five cases. Transl Res. 2020;220:1–13. doi: 10.1016/j.trsl.2020.04.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Recalcati S. Cutaneous manifestations in COVID-19: a first perspective. J Eur Acad Dermatol Venereol. 2020;34:e212–e213. doi: 10.1111/jdv.16387. [DOI] [PubMed] [Google Scholar]
- 6.Schultz K., Moriatis J. Digital ischemia in COVID-19 patients: case report. J Hand Surg Am. 2020;45:518–522. doi: 10.1016/j.jhsa.2020.04.024. [DOI] [PMC free article] [PubMed] [Google Scholar]