

Abstract
Background:
We designed this study to assess the effects and safety of Buyang-Huanwu Decoction (BYHWD) for the treatment of patients with acute ischemic stroke (AIS).
Methods:
Electronic databases of Cochrane Library, EMBASE, MEDLINE, CINAHL, PsycINFO, Scopus, Allied and Complementary Medicine Database, VIP Database, and China National Knowledge Infrastructure will be comprehensively and systematically searched from initial time of each electronic database to the present without limitations of language and publication status. Randomized controlled trials on BYHWD alone against any other interventions for the treatment of AIS will be included. All process of study selection, data collection, and methodological quality assessment will be independently undertaken by 2 investigators. Cochrane risk of bias tool and RevMan 5.3 software will be utilized for the performance of methodological quality assessment and statistical analysis, respectively.
Results:
This study will summarize most recent high quality evidence on investigating the effects and safety of BYHWD alone against any other interventions for the treatment of patients with AIS.
Conclusions:
The findings of this study will provide helpful evidence for the clinical practice for patients with AIS using BYHWD, as well as the relevant future researches.
Study registration number: INPLASY202040169.
Keywords: acute ischemic stroke, Buyang-Huanwu Decoction, effects, randomized controlled trial, safety
1. Introduction
Acute ischemic stroke (AIS) is the most common type of stroke,[1–3] which often result in high mortality and morbidity in adult population.[4–7] It has been reported that about 13 million cases are identified worldwide each year, and about more than 5 million deaths occurred.[8] Previous study has reported that about 1,900,000 brain cells are lost, and 14,000,000,000 nerve connections are destroyed every minute in patients with AIS.[9] Thus, it is very important to treat AIS timely and effectively. Although lots of managements have utilized to treat AIS, the efficacy is still limited.
Fortunately, a variety of studies reported that Buyang-Huanwu Decoction (BYHWD) has been used for the treatment of patients with AIS.[10–23] However, there is no systematic review exploring the effect and safety of BYHWD for AIS. Thus, this study is the first one to systematically assess the effects and safety of BYHWD for patients with AIS.
2. Methods
2.1. Study registration
We have registered the present study on INPLASY202040169. It has been carried out based on the guidelines of Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols Statement.[24]
2.2. Criteria for including studies
2.2.1. Types of studies
Only published or unpublished randomized controlled trials (RCTs) will be included, which explored the effects and safety of BYHWD for the treatment of patients with AIS.
2.2.2. Types of patients
The patients will be adults (18 years old or more) who were diagnosed as AIS. No limitations on country, ethnicity, gender, economic status, and educational background will be implemented.
2.2.3. Types of interventions
All types of BYHWD for the treatment of patients with AIS will be selected as an experimental intervention. However, patients who received the combination of BYHWD with other managements are not qualified in this study.
In the control group, patients could undergo any treatments, but not any forms of BYHWD.
2.2.4. Types of outcome measurements
Primary outcomes are the proportion of recurrent ischemic stroke, symptomatic intracerebral haemorrhage, and the number of all-cause mortality.
Secondary outcomes are functional improvement, as measured by the validated Barthel index or other scales; quality of life, as assessed by the 36-Item Short Form Health Survey; and frequency and severity of adverse events.
2.3. Data sources and search
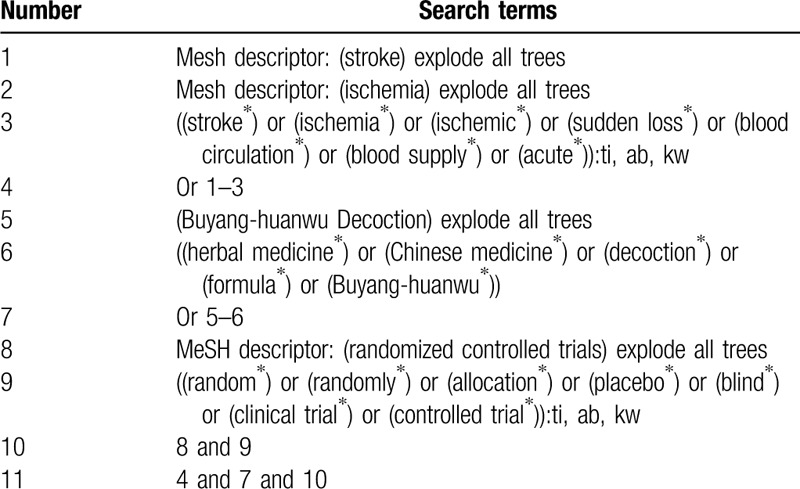
We will search Cochrane Library, EMBASE, MEDLINE, CINAHL, PsycINFO, Scopus, Allied and Complementary Medicine Database, VIP Database, and China National Knowledge Infrastructure for related trials published from initial time of each electronic database to the present without any language and publication status limitations. Any randomized controlled trials which focus on assessing the effects and safety of BYHWD alone against any other interventions for the treatment of AIS will be included. The Cochrane Library search strategy is presented in Table 1. We will adapt similar search strategies to the other electronic databases.
Table 1.
Search strategy for Cochrane Library.
In addition to the electronic databases, we will also search other sources, such as websites of clinical trial registry, dissertations, conference proceedings, and reference lists of included trials or related reviews.
2.4. Data collection and analysis
2.4.1. Study selection
Two investigators will independently check each title/abstract of all records searched and identify whether the trials fulfill the edibility criteria as described and designed in this protocol. All duplicated and irrelevant studies will be removed. Full papers of all remaining records will be carefully read against all inclusion criteria. Reasons for all excluded studies will be noted at different stages. Any disagreements between 2 investigators will be solved by discussion with a third investigator if necessary. We will present the selection of study in details in a diagram chart.
2.4.2. Data extraction
Two investigators will extract the essential data from the included trials, independently and respectively. Any different ideas between both of them will be resolved by consultation with a third investigator. The included data consists of study characteristics and methodology (such as first author, publication date, study setting, study design, randomization, study duration, follow-up duration, withdrawals, etc); participant characteristics (such as age, gender, ethnicity, diagnosis, eligibility criteria, etc); details of interventions and comparators (types of delivery, frequency, duration of delivery, dosage, etc), outcomes (all primary and secondary outcomes, safety, etc), funding information and conflict of interests. If reported data of included trials are insufficient or missing, we will contact original corresponding authors to request them.
2.4.3. Risk of bias assessment
Two investigators will independently appraise the risk of bias for each included trial using Cochrane risk of bias tool. Any divergences will be solved by a third investigator through consultation. This tool has 7 domains, and each item is evaluated as high, unclear, or uncertain risk of bias.
2.4.4. Subgroup analysis
Subgroup analysis will be undertaken to search potential causes of heterogeneity in study characteristics, participant characteristics, study methods, intervention and controls, and outcomes.
2.4.5. Sensitivity analysis
Sensitivity analysis will be carried out to identify the reliability and stability of aggregation results through eliminating trials with high risk of bias.
2.4.6. Publication bias
If over 10 trials are included, we will construct a funnel plot and Egger regression test to check possible publication bias.[25,26]
2.4.7. Evidence evaluation
We will assess all the evidence according to the criteria of Recommendations Assessment, Development, and Evaluation.[27] It covers 5 aspects, and the quality evidence of each outcome will be graded as high, moderate, low, and very low.
2.5. Data synthesis
In this study, all extracted data will be synthesized and analyzed using RevMan 5.3 software. In addition, we will perform a systematic review and meta-analysis if the collected data is judged to be similar adequate to make a certain result that is meaningful. We will express continuous values using mean difference or standardized mean difference and 95% confidence intervals (CIs), and dichotomous values utilizing risk ratio and 95% CIs. Statistical heterogeneity across included trials will be checked using I2 statistics. I2 ≤ 50% shows acceptable heterogeneity, and a fixed-effect model is used. If sufficient data on the same outcome measurement are collected, a meta-analysis will be conducted. I2 > 50% presents significant heterogeneity, and a random-effect model will be employed. Subgroup analysis will be performed to explore the causes of substantial heterogeneity. If the data is deemed not to be pooled, the results will be elaborated as a narrative summary.
3. Discussion
The literature shows that an increasing number of clinical trials have tested the effect and safety of BYHWD for AIS. So far, no systematic review has been performed to appraise the comparative effect and acceptability of BYHWD for AIS. Thus, it is necessary to develop a systematic and comprehensive study that examines the potential effect and safety of BYHWD for the treatment of AIS. The findings of this study will provide scientific evidence for clinician and future research who work in this field of knowledge.
Author contributions
Conceptualization: Chao Jiang, Xu Chao.
Data curation: Wen Zhang, Wen Pan.
Formal analysis: Chao Jiang, Wen Pan, Xu Chao.
Funding acquisition: Chao Jiang.
Investigation: Wen Pan, Xu Chao.
Methodology: Chao Jiang, Wen Zhang.
Project administration: Wen Pan, Xu Chao.
Resources: Chao Jiang, Yong-cheng Xu, Wen Zhang.
Software: Chao Jiang, Yong-cheng Xu.
Supervision: Wen Pan, Xu Chao.
Validation: Chao Jiang, Yong-cheng Xu, Wen Zhang, Wen Pan, Xu Chao.
Visualization: Chao Jiang, Wen Zhang, Wen Pan, Xu Chao.
Writing – original draft: Chao Jiang, Yong-cheng Xu, Wen Pan, Xu Chao.
Writing – review & editing: Chao Jiang, Yong-cheng Xu, Wen Zhang, Wen Pan, Xu Chao.
Footnotes
Abbreviations: AIS = acute ischemic stroke, BYHWD = Buyang-Huanwu Decoction, CIs = confidence intervals, RCTs = randomized controlled trials.
How to cite this article: Jiang C, Xu Yc, Zhang W, Pan W, Chao X. Effects and safety of Buyang-huanwu Decoction for the treatment of patients with acute ischemic stroke: a protocol of systematic review and meta-analysis. Medicine. 2020;99:23(e20534).
CJ and Y-cX contributed equally to this study.
This study was supported by the Shaanxi Provincial Key Scientific and Technological R & D Program (2017SF-348), The Science and Technology Plan Project of Yulin(2019-185-6), Shanghai Pudong New Area Science and Technology Commission Fund Innovation Funding Project (PKJ2015-Y47), Shaanxi Provincial Health and Family Planning Research Fund Project (2016D059), Shanghai Hongkou Human Resources Training Project of the Health Committee (HKYQ2018-05), National Natural Science Foundation of China (87114132), and National Key Research and Development Program (2018YFC1705900). The supporters had no role in this study.
This study will analyze data from published or unpublished trials, thus, no ethics approval is needed. We expect to publish this study on a peer-reviewed journal or to present it through a relevant meeting.
The authors have no conflicts of interests to disclose.
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
References
- [1].Phipps MS, Cronin CA. Management of acute ischemic stroke. BMJ 2020;368:l6983. [DOI] [PubMed] [Google Scholar]
- [2].Chugh C. Acute ischemic stroke: management approach. Indian J Crit Care Med 2019;23: Suppl 2: S140–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Zhang Z, Pu Y, Mi D, et al. Cerebral hemodynamic evaluation after cerebral recanalization therapy for acute ischemic stroke. Front Neurol 2019;10:719. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Fan Y, Jiang M, Gong D, et al. Cardiac troponin for predicting all-cause mortality in patients with acute ischemic stroke: a meta-analysis. Biosci Rep 2018;38:BSR20171178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Jing R, Dai HJ, Lin F, et al. Conscious sedation versus general anesthesia for patients with acute ischemic stroke undergoing endovascular therapy: a systematic review and meta-analysis. Biomed Res Int 2018;2018:2318489. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Liu M, Zheng Y, Li G. Safety of recanalization therapy in patients with acute ischemic stroke under anticoagulation: a systematic review and meta-analysis. J Stroke Cerebrovasc Dis 2018;27:2296–305. [DOI] [PubMed] [Google Scholar]
- [7].Li Y, Zhong W, Jiang Z, et al. New progress in the approaches for blood-brain barrier protection in acute ischemic stroke. Brain Res Bull 2019;144:46–57. [DOI] [PubMed] [Google Scholar]
- [8].Feigin VL, Roth GA, Naghavi M, et al. Global burden of stroke and risk factors in 188 countries, during 1990-2013: a systematic analysis for the global burden of disease study 2013. Lancet Neurol 2016;15:913–24. [DOI] [PubMed] [Google Scholar]
- [9].Saver JL. Time is brain--quantified. Stroke 2006;37:263–6. [DOI] [PubMed] [Google Scholar]
- [10].Zhang YS, Ma YZ, Qian ZP, et al. Observation of the curative effect of Modified Buyang Huanwu Decoction on Qi deficiency and blood stasis syndrome in acute cerebral infarction. Hua Xia Medicine 2019;32:92–5. [Google Scholar]
- [11].Hao MQ, Kong L. The effect and curative effect of Buyang Huanwu Decoction combined with hyperbaric oxygen on patients with acute cerebral infarction. J Wuhan Univer (Medical Edition) 2019;40:484–7. [Google Scholar]
- [12].Cai H, Yang DQ. Effect of modified buyang huanwu decoction on blood lipid and blood rheology indexes in the treatment of acute cerebral infarction with qi deficiency and blood stasis type. J Prac Trad ChinMedicine 2018;34:785–6. [Google Scholar]
- [13].Xu AX, Yang CH, Chen Y, et al. Clinical study of Buyang Huanwu Decoction in preventing early neurological deterioration in acute ischemic stroke. J Hunan Univ Trad Chin Med 2017;37:1418–21. [Google Scholar]
- [14].Song RS. Buyang Huanwu Decoction in the treatment of 49 patients with acute ischemic stroke (qi deficiency and blood stasis type). Inner Mongolia Med J 2017;49:594–5. [Google Scholar]
- [15].Li DD. Effect of Buyang Huanwu Decoction on neurological deficits and hemorheology indexes in patients with acute cerebral infarction. J Pract Trad Chin Med 2017;33:347–8. [Google Scholar]
- [16].Zheng JS. Effect of Buyang Huanwu Decoction on collateral circulation in patients with acute cerebral infarction. China Contemp Med 2016;23:145–7. [Google Scholar]
- [17].He YQ. Efficacy and safety evaluation of Buyang Huanwu Decoction granules in the treatment of acute cerebral infarction. Clin Res Trad Chin Med 2015;7:74–5. [Google Scholar]
- [18].Hu HW, Hu ZB, Tan M, et al. Clinical effect of addition and subtraction of Buyang Huanwu Decoction on acute cerebral infarction. J Pract Heart Brain, Pulmon Vasc Dis 2015;23:115–7. [Google Scholar]
- [19].Zheng GB, Zhou XK. 40 cases of acute ischemic stroke treated with Buyang Huanwu Decoction. Henan Univ Trad Chin Med 2014;34:190–2. [Google Scholar]
- [20].Wu DH. Effect of Buyang Huanwu Decoction on curative effect and hemorheology indexes of patients with acute cerebral infarction. China Med Herald 2012;9:114–5. [Google Scholar]
- [21].Cen Y. Observation on the therapeutic effect of Buyang Huanwu Decoction on acute cerebral infarction. Modern Doctor China 2012;50:81–2. [Google Scholar]
- [22].Yuan CJ, Huang W. Observation and research on the addition and subtraction of Buyang Huanwu Decoction on acute ischemic stroke. Clin Res Trad Chin Med 2012;4:73–4. [Google Scholar]
- [23].Xie JH. 30 Cases of Qi deficiency and blood stasis syndrome treated by Buyang Huanwu Decoction. Henan Univ Chin Med 2011;31:188–9. [Google Scholar]
- [24].Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev 2015;4:1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Sutton AJ, Duval SJ, Tweedie RL, et al. Empirical assessment of effect of publication bias on meta-analyses. BMJ 2000;320:1574–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Egger M, Davey Smith G, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997;315:629–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Higgins JP, Altman DG, Gotzsche PC, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 2011;343:d5928. [DOI] [PMC free article] [PubMed] [Google Scholar]