

Abstract
Background/objective:
Hearing impaired students still face stigmatization and marginalization especially in inclusive classrooms in developing regions. This negatively impacts their school engagement. The present study aimed at ascertaining the effect of video-guided educational intervention on school engagement of hearing impaired students.
Method:
Randomized controlled trial design was adopted for the present study. A total of 46 junior secondary school students with hearing impairment and low school engagement symptoms participated in this study. The students were randomly assigned to groups – intervention group and care-as-usual control group. A video-guided educational intervention package which consists of 13-minutes captioned video clips with school engagement themes served as the treatment intervention. Data were collected at 3 different times (pre-test, post-test and follow up) using School Engagement Scale created by Fredericks, Blumenfeld, Friedel and Paris (2005). Data were analyzed using independent sample t-test, paired sample t-test, Cohen d and Chi-square.
Results:
Results showed that the video-guided educational intervention significantly improved school engagement level among hearing impaired adolescent students in the intervention group in comparison with the students in the care-as-usual control group as measured by the Student Engagement Scale [Behavioral: t(24) = −9.305, P < .001; Emotional: t(24) = −7.772, P < .001; Cognitive: t(24) = −7.330 P < .001) as well as total student engagement (t(24) = 12.022, P < .001, Δ = 5.362). Also, the students who took part in the video-guided educational intervention maintained improved school engagement at follow-up.
Conclusion:
Video-guided educational intervention is an effective intervention for improving school engagement of hearing impaired adolescent students. Since acquiring relevant education is essential for leading a quality life especially among the special needs population, it was recommended that students with hearing impairment should be helped to acquire life skills through education by fostering their school engagement.
Keywords: hearing impairment, physical and health education, school engagement, schooling adolescents, video-guided educational intervention
1. Introduction
A condition whereby an individual is unable to partially or completely hear sound in 1 or both of the ears could be termed as hearing loss or hearing impairment. Hearing loss ranges from unilateral cases to profound hearing impairment.[1] Globally, current data suggest that about 360 million persons suffer disabling hearing loss.[2] Of these, 328 million people (91%) are 15years and above. The WHO estimates suggest that developing countries have a higher prevalence of hearing impairment (15.7%) among people aged 15 years and above compared to high-income countries with 4.9% of people aged 15 years and above.[2] Persons with hearing loss could lack the capacity for speech and language development.[2] Educationally, hearing impaired students may not benefit maximally from learning activities. Their effective participation in academic activities may be worse following the emphasis on inclusive education. It has been reported that although the goals of inclusive education are noble and tend to address most academic and psychosocial problems of people with disabilities,[3] hearing impaired students still face high marginalization and stigmatization in schools.[4] As a result, most of these students develop very low school engagement and high aversion for schooling.[3]
School engagement is a multifaceted concept. Generally, researchers believe that it consists of the behavioural, emotional and cognitive components.[5–7] The behavioral component of school engagement measures the degree to which a student is involved in academic and non-academic tasks, exhibits good behaviors and/or avoids troublesome behaviors. The emotional aspect describes the nature of the student's relationship with teachers, peers, and academics. The cognitive component of school engagement explains the extent the student is willing to invest in learning and go beyond the essential prerequisites to master difficult skills.[5] School engagement may lead to an improvement in academic performance,[8] and school attendance and a reduction in delinquency.[9] Therefore, achieving and sustaining school engagement for hearing impaired students is a crucial task as their impairment put them at greater risk for school disengagement.
Hearing impairment is usually associated with impairment of the vestibular system.[10] This results in postural control deficits.[11] Therefore, children with hearing impairment may lack the capability to carry out some basic motor tasks such as sustaining stability on a select leg, skipping and clapping one's hands above the head.[12] Unfortunately, these are common and basic activities in physical education classes in Nigerian secondary schools. These impediments could lead to frustration and may further exacerbate school disengagement for hearing impaired students. Fortunately, these deficiencies can be reduced by practising physical activities that enable hearing impaired students learn to make up for the vestibular shortfall, as they could make up for it with the information obtained by other senses.[13] Therefore, through sustained school engagement, hearing impaired students could overcome their postural deficiencies as they would have a greater opportunity to participate in healthy and planned physical activities during physical education classes.
The scarcity of current and representative prevalence data on hearing loss has been described as a limiting factor in promoting preventative and therapeutic interventions in developing countries such as Nigeria.[14] Mulwafu et al[15] noted that the few available studies on hearing impairment used different criteria to describe hearing impairment, hindering the comparability of their results and the development of adequate intervention strategies. Therefore, apart from estimating the hearing impairment prevalence in developing countries, much more attention is needed in providing evidence-based interventions for people with hearing impairment, particularly students as such interventions are scarce. Such interventions could aim at improving their school engagement, and in turn leading to improved academic achievements and better quality of life which have been noted to be particularly low in this group.[16]
Video-guided educational intervention is a promising intervention which could be employed to assist hearing impaired students in achieving greater school engagement. Video-guided educational intervention is a form of a group-based educational innovative technology intervention in which participants are guided to assess and reflect on the content of captioned video clips designed to address their main purposes for joining the group. The video-guided educational intervention is based on the propositions of social learning theory.[17] According to the social learning theory, desirable behaviors are learnt or acquired by an individual through direct experience or by observation of others.[17] Therefore, the intervention fundamentally hopes to guide its participants to acquire desired behaviors which encourage academic engagement after guided exposure to the video contents. Previous studies have shown the potentials of video-guided interventions on hearing impaired students and other special need students. In a previous study, Lam-Cassettari et al[18,19] found that video feedback intervention enhances the development of pre-linguistic communication in hearing impaired children. Similarly, Omoniyi and Oluniyi[20] showed that captioned video instruction had a significant positive impact on hearing-impaired pupils’ performance in English Language. Also, a video-guided intervention was used by Balkom et al[21] to show that parent-based video home training was effective and achieved long-lasting effects in children with developmental language delay.
From the foregoing, it could be observed that previous studies point to the potential benefits of video-guided interventions in assisting students with hearing impairment. Given that intervention studies targeting the hearing impaired students are scarce in developing countries, and no such intervention was developed specifically to improve the school engagement of these special need students, the present paper ascertained the effectiveness of a video-guided educational intervention on school engagement of students with hearing impairment.
2. Methodology
2.1. Ethical approval
The research and ethics committee of the Faculty of Education, University of Nigeria Nsukka approved the present study with approval number REC/FE/2018/000052. Additionally, it was ensured that the study met the ethical conditions of the World Medical Association Declaration of Helsinki.
2.2. Study participants
This study involved 46 junior secondary school students in public secondary schools in South-South Nigeria who met the following inclusion criteria: hearing threshold in decibels>35 decibel hearing level (dBHL) (moderate or worse hearing impairment based on criteria by Stevens et al[1]), attending an inclusive school, possession of a parents/guardian consent letter to participate, being adolescents aged 11 to 15 years and scoring not more than 30 overall in the School Engagement Scale (SES) at pretest (showing poor school engagement). The enrollment procedure is contained in Figure 1. To determine the adequacy of the sample size, we used G-power 3.1 Software[22] with a chosen effect size of 0.8, an alpha level of 0.05 and statistical power of 0.85 for independent sample t-test. The sample size was considered adequate.
Figure 1.
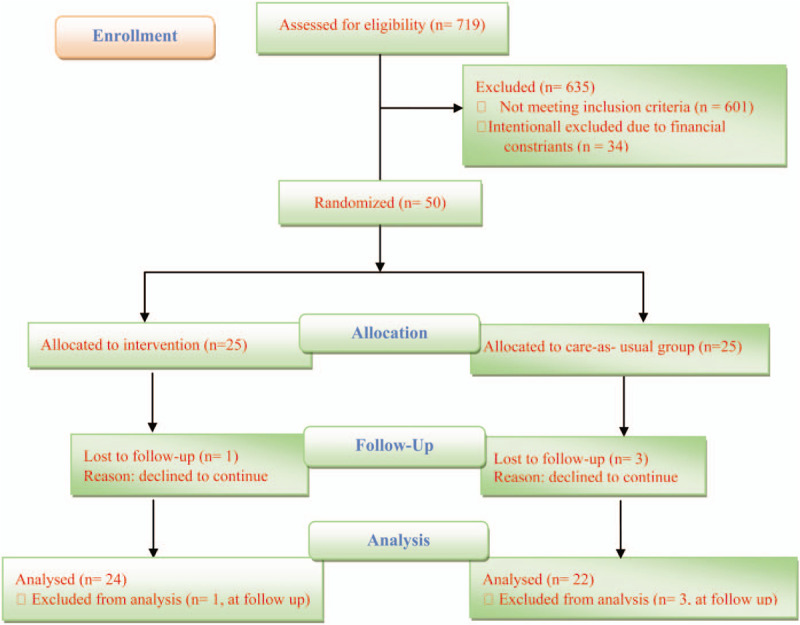
CONSORT flow diagram for participants’ eligibility.
2.3. Measures
2.3.1. SES
The study used the SES for data collection. The SES is a 19-item questionnaire developed by Fredericks et al.[5] The SES measures school engagement in 3 dimensions namely, Behavioral, Emotional, and Cognitive Engagement dimensions. Behavioural engagement dimension is measured by 5 items; the emotional dimension is measured by 6 items; while the cognitive dimension is measured by 8 items. The items are rated on a 5-point rating scale of Never (1), On Occasion (2), Some of the Time (3), Most of the Time (4), and All of the Time (5).
To determine school engagement, negatively worded items (items 2, 4 and 6) were reversed before summing up the scores, so that higher scores would reflect a higher level of engagement.
With the SES, the minimum engagement score is a total school engagement score of 19 while the maximum engagement score is a total school engagement score of 95. Total engagement has been determined by summing the scores of the different subscales of the SES. In this study, the following categorization was made regarding participant engagement scores on the SES: low engagement ≤ 30 marks, 30 marks < moderate engagement ≤60 marks, high engagement >60 marks. Participants who scored low on the SES during the pre-test were recruited for this study (30 marks and below). SES was validated in a previous study and the items for each subscale (Behavioral, Emotional, and Cognitive) of school engagement were found to be reliable with Cronbach alpha = 0.75, 0.8.2 and 0.83 for behavioural, emotional, and cognitive school engagement subscales.[5] In the present study, SES showed high internal consistency in the different subscales: Behavioural (α = 0.924), Cognitive (α = 0.871) and Emotional (α = 0.958). overall, the reliability of the SES was α = 0.969.
2.4. Demographic questionnaire
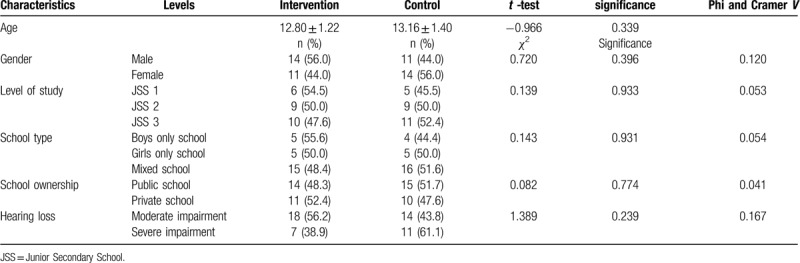
Participants’ demographic characteristics were obtained using a demographic questionnaire. Participants were asked to provide the following personal information: gender, age, level of study, school type, school ownership, hearing threshold (to be measured and provided by the researchers). See Table 1 for participant demographic characteristics.
Table 1.
Demographic characteristics of participants.
2.5. Study design
Randomized controlled trial.
2.6. Study setting
This study took place in Bayelsa State, South-South Nigeria. Geographically, the state is situated around latitude 4o 15’ and 5o 23’ N, and longitude 5o 15’ and 6o 45’ E. The state is bounded in the north by Delta State, east by Rivers State, and south and west by the Atlantic Ocean. Yenagoa is the state capital. The state occupies an area of about 21,100 Km2 and has about 2 million inhabitants. Bayelsa State is known for its rich oil and gas deposit and is considered as 1 of the greatest producers of oil and gas products in the country.
2.7. Intervention procedure
The researchers as an initial step sought the permission of the management of the chosen schools. With this permission granted, the researchers were able to work with the different schools to distribute the parents’ informed consent letter. Each student (junior secondary school students) was given a consent letter/form for their parents/guardians. Specifically, the parents’ consent forms sought the parents’ permission to allow their children to participate in the video-guided educational intervention already approved by the schools. 1578 letters/forms were given out, 1536 parents responded. Out of these, 719 consented to allow their children to participate in the intervention. Thus, the intervention had 719 potential participants who were assessed for other eligibility criteria. To determine hearing impairment prevalence among these potential participants, we defined hearing level according to Stevens et al[1] as the hearing threshold in decibels averaged in terms of frequencies 0.5, 1, 2, and 4 kHz (dBHL). Then, we set hearing impairment cut-off at hearing level ≥ 35 dBHL (moderate or worse hearing impairment).[1] 98 out of 719 students fell above the hearing impairment cut-off. This represents a 13.6% prevalence for hearing impairment. These 98 students were further subjected to school engagement pretest. 84 students met all the eligibility criteria including a low score in the school engagement pre-test. However, due to financial constraints, we purposively choose the first 50 students who met all the eligibility criteria. These students were informed about the details of the intervention and the confidential handling of their personal information. They were also notified about the possibility of quitting the intervention whenever it appealed to them. Afterwards, each participating students completed an informed assent form. The intervention lasted from September 2018 to November 2018 (about 12 weeks). At the start, participants (50 students) were randomly allocated to 1 of the 2 groups - intervention group (n = 25) and care-as-usual control group (n = 25) (see Fig. 1). The allocation sequence was generated using random allocation software in order to eliminate selection bias.[23] We used the allocation sequence to allocate students to the groups. The method employed by Onuigbo et al[24] was adopted in the allocation of students to each group. Then, the 12-week intervention program followed. After the last session of the 12th week, the SES was administered to collect post-test data on the spot. Follow-up sessions were conducted 3 months later. This lasted for 3 weeks. Data were collected at the end using the SES. Two of the researchers who are specialists in special education coordinated the intervention using sign language as a medium of communication.
2.8. Intervention package
We created and made use of the video-guided educational intervention package to assist the treatment group participants in improving their school engagement. The video-guided educational intervention package involves the use of 13-minutes captioned video clips with themes centred on school engagement. Each video clip discussed various themes using a group of hearing impaired characters who make signed communication in English. The themes discussed in the captioned video clips include understanding school engagement, importance of school engagement, school activities and engagement, relationship between school engagement and hearing impairment, understanding school engagement and relationship with peers, understanding school engagement and relationship with teachers and other staff, understanding school engagement and relationship with parents, relationship between school engagement and school achievement, dangers of maintaining poor school engagement, formation of high school engagement, strategies for improving and maintaining high school engagement, and relationship between school engagement with life following graduation. After viewing the video clip in each session, participants were given thirty minutes to reflect and discuss their experience and feelings, ask questions, and receive feedback using sign language. One of the researchers who is a sign language specialist moderated each discussion session.
The care-as-usual control intervention for the control group participants received the usual advisory model of assistance given to the students. All control group participants were enrolled to attend 1 group session per week for 3 months (ie, approximately 12 weeks). One of the researchers who is a sign language specialist also coordinated each discussion session. The group session was exclusively a sign language interaction which lasted for thirteen minutes per session and shared themes similar to those offered in the intervention group. At the end of each session, participants reflected, discussed their experience and feelings, and ask questions through sign language. Adequate feedback from the coordinator was always ensured. This lasted for thirty minutes. We ensured that students’ participation in the intervention was sustained through the provision of transport incentive, light refreshment at the end of each session, and session schedule reminders via their parents/guardian mobile phone contact.
2.9. Method of data analysis
As a precautionary measure against analyst bias, some portions of the questionnaire were hidden. Then we tested for violations assumptions of the chosen statistics. Shapiro-Wilk and Kolmogorov-Smirnov tests were used to check for normality assumption. The data was not significantly different from normally distributed data. Levene’ test for equality of variances was also considered in choosing the appropriate t-value for interpretation. We used descriptive statistics (means and standard deviations) in describing the continuous variables while frequency and percentages were used in describing the categorical variables. To determine the significant differences among categorical variables where appropriate, Chi-square statistic was used. Between-group comparison for the significant mean difference was performed using independent sample t-test. The paired sample t-test was employed to compare the within-group means at different periods of time. A significant value of P ≤.05 was used as a benchmark for result interpretation. The effect size was determined using Cohen d[25] and Glass delta.[26] All data processing and analysis were done using IBM SPSS version 20.
3. Results
Table 1 shows the sociodemographic information about the participants. It could be observed that participants’ mean age were 12.80 ± 1.22 and 13.16 ± 1.40 for intervention and care-as-usual control group respectively. The participants in each of the 2 groups to a large extent shared similar characteristics.
From Table 2, the descriptive statistics suggest that while the mean engagement score of the students in the intervention group appears to increase after the intervention (pre-test mean = 24.92 ± 3.53, post-test mean = 44.80 ± 7.80), that of the control group remained almost unchanged (pre-test mean = 24.36 ± 3.23, post-test mean = 24.48 ± 2.90). Also, when compared at post-test and follow up, students who experienced the intervention appear to have higher mean engagement (Intervention: post-test mean, follow-up mean = 44.80 ± 7.80, 46.29 ± 7.49; Care-as-usual: 24.48 ± 2.90, 25.36 ± 3.97).
Table 2.
Descriptive statistics summary.
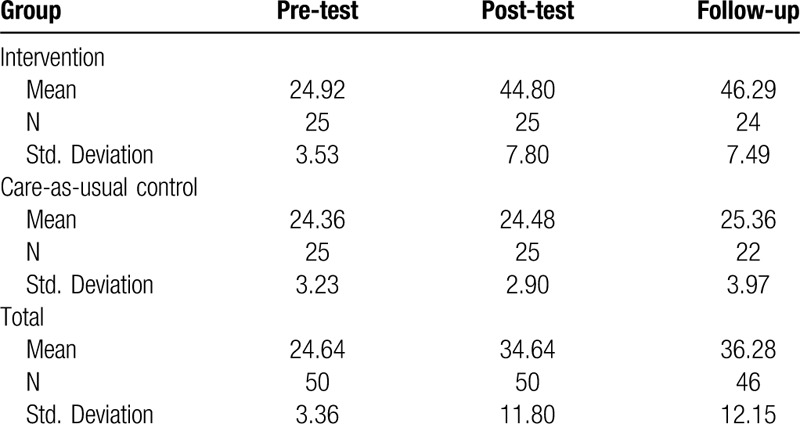
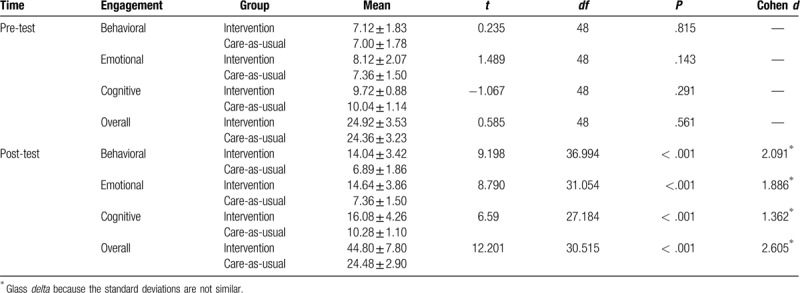
Table 3 shows that between-group comparison of the mean engagement scores of students in the intervention group and care-as-usual control group at pre-test was not significant at all dimensions of school engagement (Behavioral: t(48) = 0.235, P = .815; Emotional: t(48) = 1.489, P = .143; Cognitive: t(48) = −1.067, P = .291) as well as overall (overall: t(48) = 0.585, P = .561). However, at post-test, the mean scores of the students were significant for all the 3 dimensions of school engagement (Behavioral: t(36.99) = 9.198, P < .001; Emotional: t(31.054) = 8.790, P < .001; Cognitive: t(27.184) = 6.590, P < .001) as well as overall (overall: t(30.515) = 12.201, P < .001, Δ = 2.605). The large overall effect size suggests that the video-guided educational intervention was very effective.
Table 3.
Between-group comparison independent sample t-test for the intervention and care-as-usual group at pre-test and post-test.
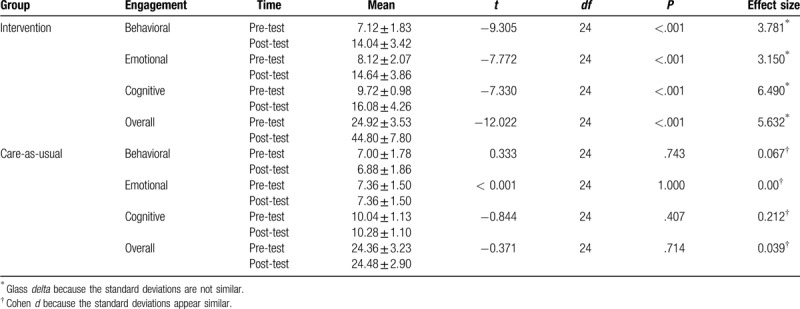
It can be deduced from Table 4 that the within-group comparison of the difference in the mean engagement scores of the students at pre-test and post-test for those who partook in the intervention was significant in all dimensions of school engagement (Behavioral: t(24) = −9.305, P < .001; Emotional: t(24) = −7.772, P = .001; Cognitive: t(24) = −7.330 P < .001) as well as overall (overall: t(24) = 12.022, P < .001, Δ = 5.362). The large effect size showed that the intervention was very effective. However, for students who were in the care-as-usual control group, the difference in their mean engagement scores at pre-test and post-test was not significant in all dimensions of the school engagement and overall (overall: t(24) = - 0.371, P = .714, d = 0.039).
Table 4.
Within-group comparison with dependent sample t-test for intervention and care-as-usual control group (pre-test and post-test paired).
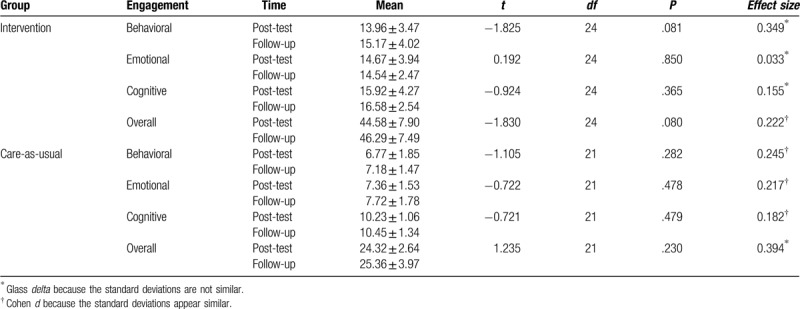
From Table 5, it could be observed that between post-test and follow-up, the mean difference in the engagement scores of students who took part in intervention was fairly similar in all dimensions of school engagement (Behavioral: t(24) = −1.825, P = .081; Emotional: t(24) = 0.192, P = .850; Cognitive: t(24) = −0.924, P = .365). Therefore, there was no significant difference in the mean engagement of students at post-test and follow-up in all dimensions of school engagement as well as overall score (overall: t(24) = −1.830, P = .080, Δ= 0.216). This suggests that the effect of the video-guided educational intervention was sustained at follow-up. Similar result was obtained for the care-as-usual control group will little effect size (overall: t(21) = 1.235, P = .230, Δ = 0.394). However, the effect size between post-test and follow-up for the intervention group decreased drastically overall when compared to the effect observed between pretest and post-test.
Table 5.
Within-group comparison with dependent sample t-test for intervention and care-as-usual control groups (post-test and follow-up paired).
4. Discussion
This study aimed at investigating the effect of a video-guided educational intervention on the school engagement of secondary school students with hearing impairment. The findings indicated that overall video-guided educational intervention was very effective in improving the school engagement level of hearing impaired students. Also, the study found that the majority of students suffering from impaired hearing (13.6% prevalence rate) were at risk of dropping out of school as indicated by their low level of school engagement. In particular, at the commencement of the intervention, students showed very low school engagement. However, after the video-guided educational intervention, it was observed that students who took part in the intervention showed significant improvement in their school engagement scores when compared to students in the control group who did not take part in the video-guided educational intervention. This improvement was sustained after 3 months follow-up. These results are in line with previous findings, reporting the effectiveness of video-guided interventions in assisting students with disabilities, further supporting their potential usefulness in improving school engagement in this group.[18,20,21,27–30] Similarly, our results on hearing loss prevalence among students (13.6%) are in line with a previous study in Nigeria.[14]
The findings of the present study are significant in several ways. First, global studies on appropriate intervention measures for improving school engagement among hearing impaired students especially in inclusive schools are scarce. Thus, the findings of the present study have provided an evidence-based strategy through which school drop-out tendency which is a direct consequence of poor school engagement in this group of special need students can be managed. Second, for a developing country such as Nigeria where scarcity of research evidence have hampered successful planning and implementation of prevention and management of relevant health policies among different populations, the findings of the present could be useful as it provided data on the prevalence rate of hearing impaired students which could guide future interventions and health management policies. Similarly, with the prevalence of hearing impairment among secondary school students in developing countries and the alarming poor school engagement of students, urgent actions must be taken to help these students regain their eagerness for schooling as education remains a sure way to ensuring a quality life. The study has offered a solution through video-guided educational intervention for sustaining the school engagement of special needs students in developing countries, particularly in Nigeria.
The findings of the present study also bear some pertinent implications for health and physical education in Nigeria. Since hearing impaired students have problems performing basic motor tasks, they could be guided to acquire and master these skills by supplementing their learning with captioned educational videos especially in inclusive health and physical education classes. Health and physical education classes could serve as a perfect place and time to achieve these as students are often required to participate in planned and guided physical exercises and movements. Mastering these skills like normal students could go a long way to improve the sense of belonging, social acceptance and school engagement of the hearing impaired students.
4.1. Strengths and limitations of the study
The findings of this study extend our knowledge on the subject by targeting a special group of physically challenged students who are at risk of dropping out of school as reflected by poor school engagement. The study showed that through guided video educational intervention, hearing impaired students could be helped to achieve and sustained high school engagement.
Despite the success of the present study, the following limitations should be borne in mind while interpreting the study results. First, the study included in-school adolescents aged 10–12 years; therefore, its findings may not effectively address school engagement issues concerning out-of-school adolescents or other student populations such as university students with hearing impairment. Therefore, future studies could target these populations unaccounted for in the present study especially in Nigeria. Second, the present study did not consider students’ family background or cause of hearing impairment. Future studies could determine the influence of these variables with respect to response to future school engagement interventions. These could improve the prescriptive value of these interventions. Finally, the present study used a self-report method for data collection. This is usually susceptible to report bias. To curb this, future studies could employ multiple means of data collection by combining qualitative and quantitative approaches for triangulation.
5. Conclusion
Video-guided educational intervention is an effective intervention for improving school engagement of hearing impaired adolescent students. Hearing impairment prevalence among adolescent students aged 11years to 15 years stands at 13.6 per cent. Since acquiring relevant education is essential for leading a quality life especially among the special needs population, it was recommended that students with hearing impairment should be helped to acquire relevant education by fostering their school engagement. This could be achieved through guided-video educational intervention.
Author contributions
Conceptualization: Uche D. Asogwa, Theresa O. Ofoegbu, Chimaobi Samuel Ogbonna, Michael Eskay, Ngozi O. Obiyo, Godfrey C. Nji, Oliver Rotachukwu Ngwoke, Chiedu Eseadi.
Data curation: Uche D. Asogwa, Theresa O. Ofoegbu, Chimaobi Samuel Ogbonna, Michael Eskay, Ngozi O. Obiyo, Godfrey C. Nji, Oliver Rotachukwu Ngwoke, Chiedu Eseadi, Christian Iheanacho Agboti, Benedict Eze.
Formal analysis: Uche D. Asogwa, Theresa O. Ofoegbu, Chimaobi Samuel Ogbonna, Michael Eskay, Ngozi O. Obiyo, Godfrey C. Nji, Oliver Rotachukwu Ngwoke, Chiedu Eseadi, Christian Iheanacho Agboti, Chinedozie Uwakwe.
Funding acquisition: Uche D. Asogwa, Theresa O. Ofoegbu, Chimaobi Samuel Ogbonna, Michael Eskay, Ngozi O. Obiyo, Godfrey C. Nji, Oliver Rotachukwu Ngwoke, Chiedu Eseadi, Christian Iheanacho Agboti, Chinedozie Uwakwe, Benedict Eze.
Investigation: Uche D. Asogwa, Theresa O. Ofoegbu, Chimaobi Samuel Ogbonna, Michael Eskay, Ngozi O. Obiyo, Godfrey C. Nji, Oliver Rotachukwu Ngwoke, Chiedu Eseadi, Christian Iheanacho Agboti, Chinedozie Uwakwe, Benedict Eze.
Methodology: Uche D. Asogwa, Theresa O. Ofoegbu, Chimaobi Samuel Ogbonna, Michael Eskay, Ngozi O. Obiyo, Godfrey C. Nji, Oliver Rotachukwu Ngwoke, Chiedu Eseadi, Christian Iheanacho Agboti, Chinedozie Uwakwe, Benedict Eze.
Project administration: Uche D. Asogwa, Theresa O. Ofoegbu, Chimaobi Samuel Ogbonna, Michael Eskay, Ngozi O. Obiyo, Godfrey C. Nji, Oliver Rotachukwu Ngwoke, Chiedu Eseadi, Christian Iheanacho Agboti, Chinedozie Uwakwe, Benedict Eze.
Resources: Uche D. Asogwa, Theresa O. Ofoegbu, Chimaobi Samuel Ogbonna, Michael Eskay, Ngozi O. Obiyo, Godfrey C. Nji, Oliver Rotachukwu Ngwoke, Chiedu Eseadi, Benedict Eze.
Software: Uche D. Asogwa, Theresa O. Ofoegbu, Chimaobi Samuel Ogbonna, Ngozi O. Obiyo, Godfrey C. Nji, Oliver Rotachukwu Ngwoke, Chiedu Eseadi, Christian Iheanacho Agboti, Chinedozie Uwakwe.
Supervision: Theresa O. Ofoegbu, Chimaobi Samuel Ogbonna, Michael Eskay, Ngozi O. Obiyo, Godfrey C. Nji, Oliver Rotachukwu Ngwoke, Chiedu Eseadi, Chinedozie Uwakwe, Benedict Eze.
Validation: Uche D. Asogwa, Theresa O. Ofoegbu, Chimaobi Samuel Ogbonna, Michael Eskay, Chiedu Eseadi, Benedict Eze.
Visualization: Uche D. Asogwa, Ngozi O. Obiyo, Godfrey C. Nji, Oliver Rotachukwu Ngwoke, Christian Iheanacho Agboti, Chinedozie Uwakwe, Benedict Eze.
Writing – original draft: Uche D. Asogwa, Theresa O. Ofoegbu, Chimaobi Samuel Ogbonna, Michael Eskay, Ngozi O. Obiyo, Godfrey C. Nji, Oliver Rotachukwu Ngwoke, Chiedu Eseadi, Christian Iheanacho Agboti, Chinedozie Uwakwe, Benedict Eze.
Writing – review & editing: Uche D. Asogwa, Theresa O. Ofoegbu, Chimaobi Samuel Ogbonna, Michael Eskay, Ngozi O. Obiyo, Godfrey C. Nji, Oliver Rotachukwu Ngwoke, Chiedu Eseadi, Christian Iheanacho Agboti, Chinedozie Uwakwe, Benedict Eze.
Footnotes
Abbreviations: dBHL = decibel hearing level, SES = school engagement scale.
How to cite this article: Asogwa UD, Ofoegbu TO, Ogbonna CS, Eskay M, Obiyo NO, Nji GC, Ngwoke OR, Eseadi C, Agboti CI, Uwakwe C, Eze BC. Effect of video-guided educational intervention on school engagement of adolescent students with hearing impairment: implications for health and physical education. Medicine. 2020;99:23(e20643).
The authors have no conflicts of interest to disclose.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Funding: The study was self-funded.
References
- [1].Stevens G, Flaxman S, Brunskill E, et al. Global Burden of Disease Hearing Loss Expert Group. Global and regional hearing impairment prevalence: an analysis of 42 studies in 29 countries. Eur J Public Health 2013;23:146–52. [DOI] [PubMed] [Google Scholar]
- [2].World Health Organization. Global Health Estimates 2016: Disease burden by Cause, Age, Sex, by Country and by Region, 2000–2016. Geneva, World Health Organization; 2018. Retrieved from: https://www.who.int/healthinfo/global_burden_disease/estimates/en/index1.html [accessed 19 July 2019]. [Google Scholar]
- [3].McCoy S, Banks J. Simply academic? Why children with special educational needs don’t like school. Eur J Spec Needs Educ 2012;27:81–97. [Google Scholar]
- [4].Asonye EI, Emma-Asonye E, Edward M. Deaf in Nigeria: a preliminary survey of isolated deaf communities. SAGE Open 2018;8:2158244018786538. [Google Scholar]
- [5].Fredricks JA, Blumenfeld P, Friedel J. Moore KA, Lippman LH, et al. School engagement. What do children need to flourish: Conceptualizing and measuring indicators of positive development.. New York, NY: Springer; 2005. 305–21. [Google Scholar]
- [6].Fredricks JA, Blumenfeld PC, Paris AH. School engagement: potential of the concept, state of the evidence. Rev Educ Res 2004;74:59–109. [Google Scholar]
- [7].Yazzie-Mintz E. Voices of students on engagement: a report on the 2006 high school survey of student engagement. Center for Evaluation and Education Policy Indiana University 2007. [Google Scholar]
- [8].Ketonen EE, Haarala-Muhonen A, Hirsto L, et al. Am I in the right place? Academic engagement and study success during the first years at university. Learn Individ Differ 2016;51:141–8. [Google Scholar]
- [9].National Research Council and the Institute of Medicine. Engaging schools. Washington, D.C: The National Academies Press; 2004. [Google Scholar]
- [10].Crowe TK, Horak FB. Motor proficiency associated with vestibular deficits in children with hearing impairments. Phys Ther 1988;68:1493–9. [PubMed] [Google Scholar]
- [11].Azevedo MG, Samelli AG. Comparative study of balance on deaf and hearing children. Revista CEFAC 2009;11:85–91. [Google Scholar]
- [12].Zwierzchowska A, Gawlik K, Grabara M. Energetic and coordination abilities of deaf children. J Hum Kinet 2004;11:83–92. [Google Scholar]
- [13].Almeida AC. Surdez, paixão e dança [Deafness, passion and dance]. São Paulo: Olho dágua; 2000. [Google Scholar]
- [14].Olusanya BO, Okolo AA, Ijaduola GT. The hearing profile of Nigerian school children. Int J Pediatr Otorhinolaryngol 2000;55:173–9. [DOI] [PubMed] [Google Scholar]
- [15].Mulwafu W, Kuper H, Ensink RJ. Prevalence and causes of hearing impairment in Africa. Trop Med Int Health 2016;21:158–65. [DOI] [PubMed] [Google Scholar]
- [16].Jaiyeola MT, Adeyemo AA. Quality of life of deaf and hard of hearing students in Ibadan metropolis, Nigeria. PloS one 2018;13:e0190130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Bandura A. Social learning theory. New York, NY: General Learning Press; 1971. [Google Scholar]
- [18].James DM, Wadnerkar-Kamble MB, Lam-Cassettari C. Video feedback intervention: a case series in the context of childhood hearing impairment. Int J Lang Commun Disord 2013;48:666–78. [DOI] [PubMed] [Google Scholar]
- [19].Lam-Cassettari C, Wadnerkar-Kamble MB, James DM. Enhancing parent–child communication and parental self-esteem with a video-feedback intervention: outcomes with prelingual deaf and hard-of-hearing children. J Deaf Stud Deaf Educ 2015;20:266–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Omoniyi T, Oluniyi EA. Impact of captioned video instruction on nigerian hearing-impaired pupils’ performance in English language. Acad J Interdiscip Stud 2014;3:411–6. [Google Scholar]
- [21].van Balkom H, Verhoeven L, van Weerdenburg M, et al. Effects of parent-based video home training in children with developmental language delay. Child Lang Teach Ther 2010;26:221–37. [Google Scholar]
- [22].Faul F, Erdfelder E, Buchner A, et al. Statistical power analyses using G Power 3.1: tests for correlation and regression analyses. Behav Res Methods 2009;41:1149–60. [DOI] [PubMed] [Google Scholar]
- [23].Saghaei M. Random allocation software for parallel group randomized trials. BMC Med Res Methodol 2004;4:26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Onuigbo LN, Eseadi C, Ugwoke SC, et al. Effect of rational emotive behavior therapy on stress management and irrational beliefs of special education teachers in Nigerian elementary schools. Medicine (Baltimore) 2018;97:e12191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed.Hillsdale, NJ: Erlbaum; 1988. [Google Scholar]
- [26].Glass GV, McGaw B, Smith ML. Meta-Analysis in Social Research. Beverly Hills, CA: Sage; 1981. [Google Scholar]
- [27].Arnaert A, Delesie L. Telenursing for the elderly. The case for care via video-telephony. J Telemed Telecare 2001;7:311–6. [DOI] [PubMed] [Google Scholar]
- [28].Hart JE, Whalon KJ. Using video self-modeling via iPads to increase academic responding of an adolescent with autism spectrum disorder and intellectual disability. Educ Train Autism Dev Disabil 2012;47:438–46. [Google Scholar]
- [29].Horn JA, Miltenberger RG, Weil T, et al. Teaching laundry skills to individuals with developmental disabilities using video prompting. Int J Behav Consult Ther 2008;4:279–86. [Google Scholar]
- [30].Horn JA. Teaching functional skills to individuals with developmental disabilities using video prompting. Master's thesis, College of Graduate Studies University of South Florida, 2008. Available at: https://scholarcommons.usf.edu/etd/299 [accessed July 19, 2019]. [Google Scholar]