

Abstract
The current COVID‐19 pandemic is a pressing world crisis and people with intellectual disabilities (IDs) are vulnerable due to disparity in healthcare provision and physical and mental health multimorbidity. While most people will develop mild symptoms upon contracting severe acute respiratory syndrome coronavirus‐2 (SARS‐CoV‐2), some will develop serious complications. The aim of this study is to present guidelines for the care and treatment of people with IDs during the COVID‐19 pandemic for both community teams providing care to people with IDs and inpatient psychiatric settings. The guidelines cover specific issues associated with hospital passports, individual COVID‐19 care plans, the important role of families and carers, capacity to make decisions, issues associated with social distancing, ceiling of care/treatment escalation plans, mental health and challenging behavior, and caring for someone suspected of contracting or who has contracted SARS‐CoV‐2 within community or inpatient psychiatric settings. We have proposed that the included conditions recommended by Public Health England to categorize someone as high risk of severe illness due to COVID‐19 should also include mental health and challenging behavior. There are specific issues associated with providing care to people with IDs and appropriate action must be taken by care providers to ensure that disparity of healthcare is addressed during the COVID‐19 pandemic. We recognize that our guidance is focused upon healthcare delivery in England and invite others to augment our guidance for use in other jurisdictions.
Keywords: coronavirus, intellectual disabilities, learning disabilities, neurodevelopmental disorders, SARS‐CoV‐2, COVID‐19
Introduction
Without a doubt, severe acute respiratory syndrome coronavirus‐2 (SARS‐CoV‐2), and the development of coronavirus disease 2019 (COVID‐19) is the most pressing current world crisis. Retrospective cohort studies from patients admitted to hospital who had contracted SARS‐CoV‐2 and developed COVID‐19 indicated that death was more likely among those who were older, had diabetes, coronary heart disease, hypertension, and an elevated sequential organ failure assessment (SOFA) score or quick SOFA score (Zhou et al., 2020). Together, there was evidence that having a higher SOFA score, along with being of an older age, and having elevated fibrin degradation product (d‐dimer) at admission significantly predicted death (Zhou et al., 2020). Evidence from other countries has indicated that those who were older, had cardiovascular disease, diabetes, cancer, or had smoked tobacco were at increased risk of death (Remuzzi & Remuzzi, 2020). At the time of writing, the online interactive dashboard from the Center for Systems Science and Engineering at Johns Hopkins University reported 5595091 worldwide are infected with SARS‐CoV‐2, while 350547 lives have been lost (Dong, Du, & Gardner, 2020), and the numbers increase daily. The overall death rate has been reported to be 2.3% based upon Chinese data (Wu & McGoogan, 2020).
Although there is some variability across studies, the estimated worldwide prevalence of intellectual disabilities (IDs) is approximately 1% (Maulik, Mascarenhas, Mathers, Dua, & Saxena, 2011; McKenzie, Milton, Smith, & Ouellette‐Kuntz, 2016), with higher rates within low‐ and middle‐income countries, (Maulik et al., 2011) where healthcare systems may not be as well developed as in the Western world. People with IDs have an increased rate of mental ill‐health (Cooper et al., 2015; Cooper, Smiley, Morrison, Allan, & Williamson, 2007; Emerson & Hatton, 2007), and physical health problems including a wide ranging list of organ‐related disorders (e.g., hypothyroidism, congenital heart problems, difficulties with hearing and vision), specific conditions such as cerebral palsy, epilepsy, along with an increased incidence of pneumonia, as well as other issues such as dysphagia, gastroesophageal reflux, and feeding‐related problems (Evenhuis, Henderson, Beange, Lennox, & Chicione, 2000; Haveman et al., 2010; Krahn, Hammond, & Turner, 2006), leading to an increased risk of admission to hospital (Dunn, Hughes‐McCormack, & Cooper, 2018). Furthermore, lifestyle factors among people with IDs are known to contribute to disease burden, such as having a sedentary lifestyle, obesity, and difficulties with maintaining hygiene independently (Evenhuis et al., 2000; Haveman et al., 2010; Krahn et al., 2006). Primary care data on a large sample of people with IDs indicated that this group had substantial disease comorbidity (Cooper et al., 2015); they were more likely to have epilepsy, visual impairment, constipation, hearing loss, Parkinson's disease, but were less likely to have coronary heart disease and other‐related disorders (e.g. hypertension), as well as being less likely to have cancer and chronic obstructive pulmonary disease (COPD; Cooper et al., 2015). However, it was apparent that comorbidity increased with age (Cooper et al., 2015).
A systematic review of the causes of death among people with IDs revealed that mortality rates are substantially higher, with death coming, on average, 20 years earlier for this population (O'Leary, Cooper, & Hughes‐McCormack, 2018), and similar findings have been reported for other countries (McCarron, Carroll, Kelly, & McCallion, 2015). Conditions associated with an early death included having profound IDs, epilepsy, difficulties with hearing, vision or mobility, increasing support needs, being female, and having some specific genetic syndromes. Most notably, respiratory disease, including pneumonia, was a leading cause of death in people with IDs, along with circulatory diseases, including heart disease and cardiac failure, cancer and congenital‐related difficulties (O'Leary et al., 2018). Strikingly, there are studies that have reported that people with IDs have died from disease, such as aspiration pneumonia, urinary tract infections, and sepsis which could have been treated through the provision of good quality equitable healthcare (Glover, Williams, Heslop, Oyinlola, & Grey, 2017; Heslop et al., 2014; Hosking et al., 2016; O'Leary et al., 2018; The Learning Disability Mortality Review (LeDeR) Programme, 2019). Furthermore, a number of people with IDs will have difficulties with dysphagia (Robertson, Chadwick, Baines, Emerson, & Hatton, 2017), and this may in turn increase the risk of aspiration pneumonia. Prompt and proactive identification of physical health concerns can be a challenge with people with IDs because of diagnostic overshadowing (Reiss, Levitan, & Szyszko, 1982), which has an impact upon the correct recognition of both mental and physical health problems leading to difficulties with accessing high quality and appropriate healthcare within primary healthcare (Beange, McElduff, & Baker, 1995; Nocon, Sayce, & Nadirshaw, 2008).
The implications for people with IDs during the current COVID‐19 pandemic are clear. There is, without a doubt, likely to be some apportioning of healthcare within some regions and people with IDs will be disadvantaged. Rebecca Thomas (2020) in the Health Service Journal wrote about General Practitioners (GP) in England sending letters to care providers informing them that people with IDs will not receive priority medical treatment in the event of SARS‐CoV‐2 infection. Prior to this, the National Institute for Health and Care Excellence (NICE, 2020a published guidance for the care and treatment of people who have contracted SARS‐CoV‐2, recommending use of the Clinical Frailty Score (Rockwood et al., 2005) within decision making about access to critical care treatment for complications arising from SARS‐CoV‐2 infection, including giving consideration to the “underlying pathologies, comorbidities, and severity of acute illness on the likelihood of critical care treatment achieving the desired outcome.” The Clinical Frailty Score was originally developed for use as an index of frailty among older people. Individuals are assigned a score from 1 to 7 on a subjective scale that is meant to measure whether someone is dependent upon others in order to achieve and carry out tasks of daily living (Rockwood et al., 2005). Considering that many people with IDs are dependent upon others to help them carry out many tasks associated with daily living, and the subsequent concerns about the validity of the Clinical Frailty Score when used with this group, NICE (2020b) quickly updated their guidance and stated that this score should not be used with people who have IDs and/or autism, people with stable long term disabilities, nor younger people, and recommended the use of an individualized assessment of frailty and needs.
There has also been concern raised about the issuing of do not attempt resuscitation (DNAR) or cardiopulmonary resuscitation (DNACPR) orders within England because individuals may have IDs or autism (British Broadcasting Corporation, 2020). On April 3, 2020, NHS England (2020b) made it clear to hospitals and primary care providers in England, quoting Professor Stephen Powis, the National Medical Director of NHS England, who stated that IDs or Down syndrome “should never be a reason for issuing a DNACPR order or be used to describe the underlying, or only, cause of death…learning disabilities are not fatal conditions”.
While responsive changes to the guidance about the care and treatment of people who have developed COVID‐19 in England are welcomed, this population is likely to present with a series of healthcare challenges that will require specialist intervention across multiple health and social care systems. Public Health England (2020d, 2020f) have identified two groups that are most at risk, and include those at risk of severe illness who need stringent social distancing (Table 1), and those who are extremely vulnerable and are at very high risk of severe illness and require shielding to prevent infection (Table 2). According to this guidance, many people with IDs should be identified as being at risk or very high risk of severe illness from COVID‐19, and a general practitioner may have already assigned them to this category. We recommend that Tables 1 and 2 should be used to identify those with IDs at high or very high risk of severe illness due to SARS‐CoV‐2 infection, and additional and appropriate action should be taken to protect their health and well‐being. We have added three further categories of risk to Table 1 specifically including those with particular physical vulnerabilities, enduring, and severe mental illness and those who display challenging behavior which may become markedly exacerbated should they become infected with SARS‐CoV‐2 and action must be taken to guard against infection, noting the varying degrees of risk. However, and paradoxically for some in this group, stringent social distancing, and shielding may lead to an exacerbation of mental health symptoms and/or challenging behavior. Those with IDs are at higher risk than the general population from complications arising from contracting SARS‐CoV‐2, and the purpose of this article is to present our guidelines for the care and treatment of people with IDs during the COVID‐19 pandemic in an attempt to help address healthcare disparities within community, residential, and inpatient settings. The guidelines have been developed collaboratively by a group of health and social care professionals and carers who care for people with IDs, who provide specialist medical, psychiatric, and social care within both community and inpatient psychiatric settings or in their own homes. Throughout, we have attempted to focus upon the needs of people with IDs, including those within this population, who are likely to be at most risk and they are meant to complement the initial guidance provided by NHS England (2020a) about supporting people with IDs during the COVID‐19 pandemic.
TABLE 1.
Group at risk because they are clinically vulnerable due to severe acute respiratory syndrome coronavirus‐2 (SARS‐CoV‐2) infection who need particularly stringent social distancing measures
|
TABLE 2.
Extremely clinically vulnerable group at very high risk of severe illness due to severe acute respiratory syndrome coronavirus‐2 (SARS‐CoV‐2) infection who require shielding measures
|
These guidelines are subject to revision and the most recent versions can be downloaded by visiting http://radiant.nhs.uk. The aim of this study is to describe our guidelines which focus upon providing care and support before and after infection with SARS‐CoV‐2 and the development of COVID‐19. These guidelines are meant for community teams, inclusive of social care providers, who provide care and treatment within community‐based settings and care teams working within hospital settings for people with IDs. We have also included guidance about referral and admission to general hospital. Community teams providing care to people with IDs in England are referred to as community learning disabilities teams and we use this language in several places within this study. These teams provide a range of care and support to people with IDs, while during the current pandemic there will be an increased focus upon providing healthcare. We recognize that healthcare systems for people with IDs around the world vary, and while our focus is upon England, it is hoped that these guidelines will be applicable to health and social care settings for people with IDs in other countries, and as appropriate, helpful for educational settings. We completely welcome and invite groups to adapt these guidelines to fit effectively within their own local, regional or national health and social care systems.
Guidance about Responding to and Reducing the Risk of Infection
For people with IDs living in the community in England, physical healthcare is provided by primary care services, inclusive of their general practitioner. This also includes the vital and important role of carers working within shared residential settings where many people with IDs live. The role of community learning disabilities teams is to provide input into healthcare about specific vulnerabilities, highlighting disparity, and helping to reduce the risk of infection.
However, for community learning disabilities teams, if they make use of the ratings listed within Tables 1 and 2, many people with IDs receiving care will be assigned to the at risk of severe illness from COVID‐19 category, and many will also be assigned to the very high risk of severe illness from COVID‐19 due to associated comorbidity. Appropriate action should be taken to mitigate the risk of infection within community‐based settings, inclusive of residential settings. Staff working within psychiatric inpatient settings should also identify individuals with IDs who are at risk as detailed in Tables 1 and 2. A summary of our guidance and associated risk mitigation strategies are found in Figure 1.
FIGURE 1.
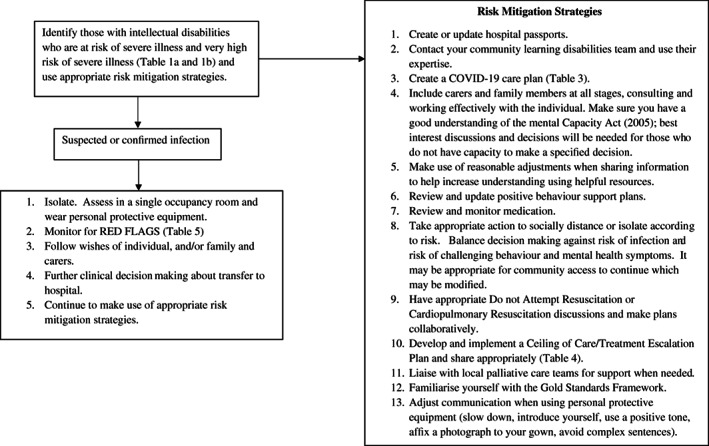
A summary of steps to take to mitigate risk and protect people who have intellectual disabilities during the COVID‐19 pandemic.
Risk Mitigation Strategies
Hospital passports
Ensure that people with IDs have an up to date hospital passport or equivalent, depending on the local, regional or national policy, which includes information from the person themselves, and all those who know them well, including their family and advocates. A hospital passport is a document that is meant to support the provision of appropriate healthcare to a person with an ID. It includes essential information about the person inclusive of important medical information, their activities, and things the person prefers or does not prefer. Ensure appropriate attention has been paid to the presence of physical health problems, including those which may increase the risk of more severe illness due to contracting SARS‐CoV‐2 (e.g., smoking history, history of heart disease, respiratory problems, body mass index (BMI) >40) and other conditions such as mental health problems, dysphagia, sensory problems, or communication needs. More information can be found about hospital passports by visiting the Mencap website (https://www.mencap.org.uk/advice-and-support/health/health-guides). All people with disabilities are entitled to reasonable adjustments to the provision of healthcare under the Equality Act (2010), and a hospital passport is an example of a reasonable adjustment. Further details about additional reasonable adjustments should be included within the hospital passport.
COVID‐19 care plan
Prepare a COVID‐19 care plan for each person with an ID within your care and this should be developed collaboratively with the person. This should set out the specific risk factors and associated needs of each individual (Table 3) and community learning disabilities teams should work collaboratively with care providers within residential settings, bearing in mind that some people with IDs live alone and may not have regular and consistent support beyond that provided by the community learning disabilities team. The care plan should include information from the person (if appropriate) and those who know the person well and refer to the hospital passport and incorporate relevant information. Issues associated with diagnostic overshadowing, the views of parents, family members and carers, the required reasonable adjustments, communication needs, specialist mental health support, anticipatory care plans, any end‐of‐life or do not attempt cardiopulmonary resuscitation (DNACPR) discussions should be reported. Associated strategies for managing hand hygiene, infection control, social distancing, and isolation when needed should be included.
TABLE 3.
Example brief COVID‐19 care plan
|
Patient name, gender, date of birth: AB, male, January 01, 1965
Actions: Information shared with GP
For any additional information from the CLDT, contact “name, address, and telephone number.” |
The above is a representative example and should be adapted as needed.
Families and Carers
Carers and family members are vital to the health and security of people with IDs (Chester, James, Rogers, Grace, & Alexander, 2020), and more so during the COVID‐19 pandemic and should be involved at all stages. Clinicians should actively seek to explain the important precautions that need to be taken with handwashing, avoiding touching the face and eyes, use of tissues while coughing and sneezing and their appropriate disposal to carers and people with IDs. It must be recognized that this is not likely to be straightforward with those who have severe and profound IDs. Limitations on access to the community need to be explained. For those living within residential settings, appropriate precautions and protocols need to be developed for isolation should someone contract COVID‐19. There are a number of resources that can be used by carers and families to help explain these challenges to people with IDs (e.g., Beyond Words, 2020) while emphasizing the need to monitor for signs and symptoms of COVID‐19 including a fever, new cough, fatigue, congestion, shortness of or difficulty breathing, chill, muscle pain, dizziness, sore throat, headache, vomiting, and diarrhea. Many people with IDs will have difficulties explaining how they are feeling, and it is important that family and carers remain vigilant to changes in presentation. For example, many people with IDs may not be able to report that they have a headache, while other symptoms are observable to others (e.g., a new cough) and tools such as the Distress and Discomfort Assessment Tool (https://www.stoswaldsuk.org/how-we-help/we-educate/education/resources/disability-distress-assessment-tool-disdat/) can be employed by carers to record symptoms of distress (Regnard et al., 2007).
Capacity and law
Within England, where questions of capacity arise regarding an individual's ability to make a decision to isolate and take appropriate action to reduce risk (e.g., social distancing), this may trigger an assessment of capacity (The Mental Capacity Act, 2005) for some individuals, bearing in mind that we will all make the assumption that all have capacity to make decisions unless there is information to the contrary. Appropriate reasonable adjustments (e.g., sharing accessible information and providing clear explanations with opportunities for individuals to ask questions) should be made when sharing and discussing information. For those who have capacity, they are entitled to make their own decisions, and this may involve not following recommendations or advice which may cause them or others harm. For those who are judged not to have capacity, this will prompt a Best Interest discussion and may lead to an authorization of Deprivation of Liberty for some. For such to be authorized in relation to COVID‐19, the person must lack capacity to consent to the arrangements, have an “impairment of their brain or mind” and the arrangements must be necessary to prevent harm and be proportionate to the likelihood and seriousness of the said harm. All of this would need to be balanced against a person's rights, autonomy, and well‐being, and for many, this could be avoided with the provision of good communication and the involvement of carers and family members which is strongly recommended. Related, and within England, The Health Protection (Coronavirus, Restrictions) (England) Regulations (Public Health England, 2020e) are relevant, which are statutory restrictions on every person which prevent people from leaving their homes without a “reasonable excuse.” The police have been granted the powers of reasonable force to return someone to their home. Furthermore, The Coronavirus Act (2020) has made it a criminal offense to fail to comply with the instructions of the police or a public health officer, and the police may use reasonable force to remove people or compel someone to remain at home. These laws are applicable to all citizens, but their interface and relationship with the Mental Capacity Act (2005) is unclear.
There are clear issues for many people who provide care to people with IDs where routine and structure are exceptionally important. Increasing isolation to protect people from infection is likely to have a negative impact upon the quality of life of people with IDs and may lead to an increase or re‐emergence of challenging behavior or the development of mental health problems. If individuals access the community, which will include opportunities to visit places to engage in exercise and activities, some individuals may require multiple support staff to be present. This may attract the attention of other members of the public and/or the police. Avoiding these activities is likely to be detrimental to the health and well‐being of many people with IDs, disrupting their quality of life. Protecting individuals from infection while maximizing quality of life is a tricky balancing act that must be navigated. Community learning disabilities teams should work with families, and where necessary, consider issuing letters to families, and carers that can be shown to the police or public health officials as appropriate.
Social distancing
For all people with IDs, stringent social distancing should be followed. This includes avoiding public transport, remaining at home, and of course, avoiding contact with those who have contracted SARS‐CoV‐2, or those who are displaying symptoms of infection. For those who are judged to be at very high risk of illness, shielding measures must be adopted. This includes strictly avoiding contact with anyone displaying symptoms, remaining at home, never attending gatherings, avoiding going out to shops or taking part in leisure activities, arranging for food and medication to be delivered, and where possible, making use of technology for social contact as best as possible (Public Health England, 2020f). For carers and those working in residential settings, Public Health England has issued separate guidance which includes reducing visits from family and friends. Individuals should be risk assessed, and where possible, reasonable adjustments made. Staff should wear personal protective equipment (PPE), and ensure proper hand and environment hygiene (Public Health England, 2020b). Changes to routine (e.g., canceling community trips) for people with IDs may result in the development of, or an increase in challenging behavior, and care plans and associated risk assessment should be inclusive of these issues. In such instances, it is reasonable to facilitate and support community trips in order to reduce or escape a risk of harm, and in certain circumstances, with careful planning to mitigate risk of infection, it may be advantageous to facilitate some appropriate community trips for people with IDs. This should be carefully considered, balancing risk, and should be fully discussed with family members and carers, as well as the community learning disabilities team.
Visits by community learning disabilities teams
As far as possible, community learning disabilities teams should make use of telephones and videoconferencing to contact carers, family members and people with IDs. Team members, when visits are necessary, should enquire as to whether anyone within a property is displaying symptoms of COVID‐19, and make use of alternatives where such symptoms are present. If a visit is needed, appropriate risk mitigation strategies should be taken, and this may include wearing PPE during the visit. As a minimum, a fluid resistant surgical mask, disposable apron, and if blood or bodily fluid contamination is anticipated, gloves and eye protection should be worn (Public Health England, 2020a). Guidance changes rapidly and readers are directed to follow the advice from their own regional or national authority. Community visits are unlikely to involve aerosol generation procedures, noting that spitting is not considered an aerosol generating procedure. If aerosol generation procedures are likely, then an appropriate respirator, long‐sleeved disposable fluid‐repellent gown, gloves, and eye protection must be work. Note that in situations where cardiopulmonary resuscitation attempts and the use of suction are likely, the continuous positive airway pressure and the use of high flow nasal oxygen are aerosol generating procedures.
Do not attempt resuscitation or cardiopulmonary resuscitation
These discussion and decisions are difficult for all people, and the vast majority of people with IDs known to community learning disabilities teams live full and rewarding lives. Hence, end‐of‐life of DNAR or DNACPR discussions and decisions are not necessary, but they may arise on some occasions. It is important to note that IDs or Down syndrome should never be used as a reason for issuing a DNACPR order (NHS England, 2020b). Those who are ageing and have multimorbidity who may suffer a marked deterioration in adaptive behaviors may suffer a precipitous decline in their physical health if they develop a virulent infection (Remuzzi & Remuzzi, 2020; Zhou et al., 2020). In the context of the current pandemic, while such discussions and decisions are likely to be disturbing for many individuals, and families and carers, carefully formulated care plans for some are likely to be required. When used appropriately, such plans are intended to reduce suffering and promote a dignified death with those who are close to the end of their life (National End of Life Care Programme, 2011). The role of the community learning disabilities team is not necessarily to oversee creating these plans, but to work closely with the individual, their family, carers, and those in primary care to help facilitate discussions as needed within the context of the COVID‐19 pandemic. The underlying principles for any such discussion are set out by the National End of Life Care Programme (2011) and should ensure that care is client‐centered and integrated, a circle of support is identified, people are treated with dignity and respect, their preferences are identified and respected, and appropriate care and support for families, carers, and staff are provided after death.
Timely and honest conversations about an individual's preferences and priorities, including any advance decisions to refuse treatment should be part of the care planning for anyone who has a progressive life‐limiting illness. The Care Quality Commission (2016) has reported that the barriers to effective palliative and end‐of‐life care include a nonrecognition of end‐of‐life, poor communication, inequalities in accessing good care, and difficulties with staff awareness and noncollaborative working. For most people with IDs who contract SARS‐CoV‐2, the priority will be treatment in line with national policies and guidance including referral to general hospital as needed, and clinical decision making should be the same as for members of the general population, drawing on the same parameters. However, for some, COVID‐19 may quickly exacerbate existing illness and create a situation where an individual may become very ill and unable to benefit from intrusive treatment (Guan et al., 2020; Huang et al., 2020; Richardson et al., 2020). Considering this, honest conversations need to occur as early as practicable so that personalized care and support plans can be developed. These will need to be revisited if any situation changes, and families and those close to an individual should be involved in these discussions in line with a person's wishes where possible.
There are several steps that services need to take which will vary according to national policy and legislation. First, within England, where there are concerns about capacity to make decisions about medical treatment, a best interest discussion and decision should happen, fully inclusive of family members and carers and any attorney appointed under a Lasting Power of Attorney or Enduring Power of Attorney if applicable, or Personal Welfare Deputy. If a person has capacity to make decisions about their medical treatment, then it is their decision to refuse or accept treatment.
Second, a conversation should be started with and about those who are nearing the end of their life. This should include family members, carers, and others involved in the lives and care of individuals with IDs. It should be recognized that this is an area fraught with difficulty for people with IDs who may not be appropriately included within decision making (Voss et al., 2017). Advance care planning is something that is used to help make decisions in the future, and this process is not just about palliative care, but for any planning. The process should help make clear a person's wishes and will usually take place within the context of an anticipated deterioration of a person's illness or condition in the future when they may have lost capacity to make decisions. It is important that these decisions are done sensitively and with empathy, and it is recommended that community learning disabilities teams (or inpatient teams) identify appropriate staff members for these conversations with both the individual and their family. Staff should make use of resources to help structure and support any conversations with individuals (e.g., Books Beyond Words) to help make sure that information is understood. Make sure that a holistic assessment of end‐of‐life needs and preferences has taken place in partnership with the individualand their families and carers. Assess and respond sensitively to social, psychological, and spiritual needs and wishes of the individual, as well as their physical healthcare needs. Identify and record any further wishes and preferences as they become apparent about future care and treatment and verify with the local general practitioner as needed. If appropriate and requested, and for those who have capacity, you should support someone to make an Advance Decision to Refuse Treatment, sometimes referred to as a living will, and communicate this to all those involved in the provision of care. Within England, an Advance Decision is legally binding, and the individual must name the treatments they are deciding to refuse such as ventilation or cardiopulmonary resuscitation and the circumstances in which they would be refused. An Advance Decision to Refuse Treatment is not the same as an Advance Statement. An Advance Statement can cover any aspect of future health and social care and an individual must have capacity to make decisions pertaining to the statement. It is not legally binding, but those providing health and social care must take it into account when making decisions.
Ceiling of care/treatment escalation plan
Third, a ceiling of care/treatment escalation plan should be developed to document care planning. The purpose of this plan is to identify the wishes of the individual, their families and their carers in the case of a deterioration of physical health due to developing COVID‐19. It is to provide guidance to the attending clinicians and should not replace clinical judgment. Some individuals may already have an Advance Statement, Advance Decision to Refuse Treatment or Power of Attorney to advise and make healthcare decisions. These should be followed instead unless the clinical situation is markedly different to any envisaged by the Advance Statement. An example of the issues that should be covered when developing a ceiling of care/treatment escalation plan is found in Table 4. Ideally, this should be completed with the individual, families, carers, and clinical and social care staff, and it is vital that all are consulted and included and consideration should be given to future transfer to general hospital. During the pandemic, videoconferencing or teleconferencing could be used to facilitate discussion and meetings. Once a care plan has been completed, it should be shared with all staff caring for the individual, and in the case of deterioration, on call medical staff, out‐of‐hours general practitioners, or the paramedic crew should be made aware. Any decision to transfer an individual to hospital should be discussed with the family as soon as possible and a copy of the ceiling of care/treatment escalation plan should be sent, along with a covering letter if helpful.
TABLE 4.
Topics to be included within a ceiling of care/treatment escalation plan
|
Fourth, learning disability teams need to liaise with local Palliative Care Teams for support. As end‐of‐life approaches, this should be recognized, and symptoms documented and discussed by the clinical team. Staff should consider any recent changes in circumstances and note any new triggers in addition to SARS‐CoV‐2 infection (e.g., worsening pre‐existing physical or mental illness). Staff will need to identify whether it is appropriate to begin an open and supportive discussion with the individual, if possible, and their family and relatives about their wishes for end‐of‐life care, bearing in mind whether the individual wishes to have open discussions about prognosis and future care options. During the current pandemic, this may occur using videoconferencing or teleconferencing which may lead to some additional distress as relatives will not be able to be physically near their loved one.
Fifth, many general practitioners are likely to have implemented an end‐of‐life care register specifically in relation to COVID‐19, working within the Gold Standards Framework (see https://goldstandardsframework.org.uk/) and care must be coordinated across health and social care systems, drawing upon generic community nursing teams who deliver end‐of‐life care in conjunction with specialist palliative care teams. NHS England (2017) has published guidance about providing good quality healthcare to people with IDs at the end of their life. This includes ensuring that each person is seen as an individual, helping them to develop an awareness of death and dying, while involving families, carers, supporters, and friends. Clear communication needs to occur between all care systems ensuring that documentation is up to date, and bereavement support is available for those left behind. Everyone should work to maximize comfort and wellbeing which includes helping people to understand their illness to help reduce fear and encourage coping. This includes working to help people understand why treatment is necessary and using creative methods to help encourage understanding and coping. Related, it is important to complete effective person‐centered pain assessment.
Finally, during the last days of life it is important to be aware that an individual's condition could improve. Open discussions will be required with families, friends, and carers, and where possible adhere to patient wishes and preferences where needed, ensuring that anticipatory prescribing systems are in place, or there is a rapid system to access necessary medication. Anticipate and help plan for any specific religious, spiritual, or cultural needs that may be necessary, helpful, and beneficial to both an individual and their family. After death, it is important to be respectful of religious, spiritual or cultural needs and beliefs and that they are met. Teams need to be aware of verification and certification of death policies. Ensure that appropriate information is provided to family members and carers about what to do after death, and offer support and information about bereavement, and assist as appropriate with remembrance. Some of these activities will have to occur over the telephone or via videoconferencing during the pandemic.
Mental health and challenging behavior
The current restrictions upon all our lives have changed the way we live, work, and interact with each other. These changes are likely to cause distress for many people with IDs which are likely to lead to an increase in challenging behaviors and mental health symptoms. It is entirely likely that when an individual with IDs is faced with actual or suspected SARS‐CoV‐2 infection, the inevitable further restrictions may lead to a worsening of mental health symptoms and/or challenging behavior. It is important not to assume that this is inherently a relapse of mental illness, as some changes occur directly as a result of environmental changes, or could be associated with SARS‐CoV‐2 infection and unknown effects on the nervous system (Wu et al., 2020), and issues related to diagnostic overshadowing should be at the forefront of clinical decision making. It is important to carefully monitor behavior and mental state, including the use of any restrictive interventions that are used within home and residential settings. Community learning disabilities teams have an important role to play in maintaining community living and preventing inappropriate admission to psychiatric inpatient settings and should always be consulted and included. Community learning disabilities teams have an important proactive role to play by providing advice on behavior and supporting people within the home, and the Challenging Behaviour Foundation (2020a, 2020b) has produced some helpful guidance that may assist families and carers. Wider guidance is available from other organizations (e.g., British Psychological Society: https://www.bps.org.uk/responding-coronavirus). Other resources from around the world have been posted online by the International Association for the Scientific Study of Intellectual and Developmental Disabilities (2020). If needed, training and advice to home and residential settings can be delivered using videoconferencing. We are recommending that those with IDs who have severe and enduring mental health problems, inclusive of but not limited to schizophrenia, psychosis and bipolar disorder, and those with multiple mental health diagnoses, or who are taking medication that requires close monitoring (e.g., clozapine), along with those who are likely to experience an increase or reemergence of challenging behaviors that will severely impair their quality of life are rated as high risk of severe illness due to SARS‐CoV‐2 infection (Table 1). These two additional groups have been added to Table 1.
A variety of changes are likely to lead to an increase in emotional distress during the COVID‐19 pandemic and community learning disabilities teams will need to work effectively with individuals with IDs, their carers and families and providers of community‐based services to help mitigate distress. Changes to routine may cause increased anxiety, which may lead to an increase in challenging behavior and mental health symptoms. Many of these challenges are likely to be related to difficulties with effective communication and understanding the changes, mental health problems, and other associated functions such as demand avoidance, access to tangibles inclusive of previously enjoyed activities. Behavioral support plans, such as the positive behavioral support plan will need to be revised accordingly and there is an important role for the specialist advice and support of the community learning disabilities team. This would include an updated formulation as needed, along with the provision of psychological and other associated interventions to help with challenging behavior and mental health. Changes to key staff including carers, community learning disabilities team members, parents and family members (who may be absent due to isolation and illness) may cause further anxiety and disruption and will need to be effectively managed, and may have a negative impact upon the continued successful implementation of positive behavioral support plans. Further training may be needed, which could be delivered online by community learning disabilities teams as needed. For some, family members and carers may be admitted to hospital due to COVID‐19 which may result in the loss of life and will cause associated bereavement and grief for many people with IDs, and appropriate strategies should be incorporated into a positive behavior support plan. For those family members who become unwell, it is important for services to facilitate ongoing contact using electronic methods of communication. Most importantly, services must recognize the importance of normal human emotional expression during times of stress, and this should not be pathologized. People with IDs may require additional help and support to understand what is happening to successfully grieve during a time when they may not be afforded the opportunities to grieve in a traditional manner (e.g., attending a funeral, seeking comfort from loved ones and family members). There is a clear role for specialist psychological interventions delivered by community learning disabilities teams.
Personal protective equipment
The use of PPE is likely to have a substantial impact upon some people with IDs as follows: (a) it will disrupt some non‐verbal communication as facial expressions will be entirely or partially covered which are vital to good communication. In such circumstances, eyes and natural gesture should be used as much as possible to facilitate positive communication, (b) equipment which covers the mouth may change speech, making intelligibility problematic, and (c) equipment may provoke anxiety among some individuals which may change the nature and quality of the interaction. It is important that staff wearing PPE introduce themselves, continue to adopt a positive tone, and use the name of the person within the interaction. It is likely to be advantageous to add a photograph of a staff member's protective clothing to help with identification. Speech should be slowed down as appropriate, but not condescending, and if needed, increase the volume of speech and allow individuals time to process communication. Sentences should be as clear as possible, incorporating a single piece of information; complex and long sentences with multiple conjunctions and connectives should be avoided. If helpful, use can be made of writing or drawing to aid communication, and checks made to ensure that communication has been understood. It is also important for all healthcare staff to recognize that many people with severe to profound IDs may make use of signing or symbol‐based communication, and those who know individuals (usually the family members and carers) well are best placed to provide guidance and support. People with IDs are entitled to reasonable adjustments when accessing healthcare in England, and similar requirements exist in other jurisdictions around the world.
Psychotropic medication
It is vital that psychotropic medications are reviewed appropriately in line with good practice guidance (e.g., NICE, 2016). It is important to pay attention to side effects such as respiratory depression and cardiac effects. This would mean carefully analyzing the effects and side effects and weighing this against the importance of maintaining good mental health. Be aware of issues associated with diagnostic overshadowing (e.g., a high fever may be a rare side effect called neuroleptic malignant syndrome or serotonin syndrome rather than due to COVID‐19). Close liaison with pharmacy services will be needed to make sure that required medications are available, and medications may have to be delivered by healthcare staff or via the post. Changes to medication may be required to assist in the management of mental health symptoms, and some individuals may require depot medication which is administered by general practitioners, community nurses within community learning disabilities or mental health teams.
Guidance Regarding Care and Support Following Infection or Suspected Infection
For many people with IDs who are infected with SARS‐CoV‐2, they will receive care at home, and many will recover while others will not develop COVID‐19. However, some will need to be transferred to a general hospital, and when admitted, we recommend that the community learning disabilities team works closely with those in hospital to ensure a robust handover of relevant information and assist with decision making. This work may take place through liaison teams for mental health and/or IDs where they are available within the general hospital, inclusive of the valued role of specialist liaison nurses for people with IDs who will be able to provide specialist assistance with the provision of reasonable adjustments within a general hospital setting (MacArthur et al., 2015). For those who are currently detained within psychiatric settings, the treating team will have responsibility for both physical and mental healthcare.
Suspected SARS‐CoV‐2 Infection
Individuals should be assessed within a single occupancy room, and the clinician should wear PPE for all face‐to‐face interactions regardless as to whether SARS‐CoV‐2 infection is suspected. As a minimum, this should be a fluid resistant surgical mask, single‐use disposable apron, gloves, and eye protection if blood or bodily fluid contamination to the eyes or face is anticipated. If aerosol generation procedures are likely, then an appropriate respirator mask, long‐sleeved disposable fluid‐repellent gown, gloves, and eye protection must be worn. Note that in situations where cardiopulmonary resuscitation attempts, and the use of suction are likely, continuous positive airway pressure and the use of high flow nasal oxygen are aerosol generating procedures.
It is important that staff explain their policy about isolation to all individuals within the hospital should there be suspected SARS‐CoV‐2 infection. This should include the specific details as to what will happen and when. Appropriate communication aids may need to be used, and staff experienced in working with people with IDs should be called upon as they will be acutely aware of individual communication needs. Teams need to work effectively to minimize the need for restrictive interventions to implement isolation procedures through effective communication and the continued maintenance of trusted therapeutic relationships. Isolation is likely to be distressing and leads to an increase in challenging behavior and the use of PPE may cause distress and appropriate action should be taken to mitigate this distress as outlined in the previous section.
Services should make use of provided SARS‐CoV‐2 testing kits and send swabs to the designated site for testing. Anyone who has reported symptoms should be isolated for the number of days required by local or national policies, and physical monitoring must continue. Ensure adequate nutrition and hydration, and symptomatic treatment as appropriate (e.g., paracetamol for fever, asthma medication as indicated, maintain fluid intake, complete urine output charts, etc.). Watch for any signs of deterioration; fever can continue for a few days, but respiratory function may worsen between 5 and 12 days. Action must be taken if any of the red flags are present as listed in Table 5 as adapted from Greenhalgh et al. (2020). When present, these symptoms indicate that urgent assessment is needed and further action such as escalation to an acute hospital or ongoing assertive management of health is needed. Note that COVID‐19‐related pneumonia may be complicated by respiratory distress, and there are additional risks associated with dysphagia, and consistent regular physical health monitoring using standardized and validated instruments should be used (e.g., National Early Warning Score‐2; Royal College of Physicians, 2017).
TABLE 5.
COVID‐19 Red Flags for people with intellectual disabilities adapted from Greenhalgh, Koh, and Car (2020)
If in doubt discuss with a physician as per local arrangements. |
Public Health England (2020c) has provided guidance on when to transfer someone to a general hospital, inclusive of those within psychiatric settings. Transfer to a general hospital should occur when: (1) they have clinical or radiological evidence of pneumonia, or (2) acute respiratory distress syndrome, or (3) they have influenza like illness. This is a fever ≥37.8°C and at least one of the following respiratory symptoms with acute onset: (1) persistent cough (with or without sputum), (2) hoarseness, (3) nasal discharge, (4) shortness of breath, (5) sore throat, (6) wheezing, or (7) sneezing. Clinicians should test for SARS‐CoV‐2 when an individual is presenting with new respiratory symptoms or fever without another cause or worsening of a pre‐existing respiratory condition. Early recognition of a deteriorating individual and referral to a general hospital is critical for treatment as patients may present with sepsis, pneumonia, and adult respiratory distress syndrome. Those with underlying health conditions as set out in Tables 1 and 2 are likely to progress to a complicated illness. There are important discussions that need to take place between staff within residential care settings, or psychiatric hospitals, and the general hospital and issues to be covered are presented in Table 6.
TABLE 6.
Points to be covered in a referral discussion to a general hospital
|
When transferring an individual to a general hospital, they should be accompanied by at least one member of staff who knows them well, taking their hospital passport and COVID‐19 care plan. Staff should be supported with this task, as they may experience justifiable anxiety at the prospect of attending hospital, and can be reassured that if all the guidance is followed (e.g., regular handwashing) and wearing the correct PPE, it is safe for them to carry out escort duties. Within England, if detained under the Mental Health Act (1983, as revised in 2007) Section 17 leave must be authorized, and staff must always remain with the individual. If the individual is transferred under Section 19, then the general hospital must ensure that they have adequate mental health staff to provide support, bearing in mind it would be better to have staff with a pre‐existing positive relationship accompany them.
People Currently Detained with Psychiatric Hospitals
For many psychiatric hospitals, they will be providing care directly to patients who develop COVID‐19 during the pandemic, and many of these patients will recover without needing to be transferred to a general hospital. However, all teams should continue to work towards the successful discharge of individuals with IDs from psychiatric hospitals. Where possible and appropriate, it would be useful to expedite discharge safely.
There are related concerns about some of the changes that have been made to the provisions of the Mental Health Act (1983, as revised in 2007) as a consequence of the Coronavirus Act (2020) in terms of the implications for people with IDs. These changes include the removal of the requirement for two medical practitioners to agree to the detention of an individual under Section 2, and many Sections of Part III of the Mental Health Act, if arranging for two medical practitioners is judged to be impractical or would cause delay. Holding powers under Section 5 and Section 136 have been increased in duration, and a Responsible Clinician has been granted the authority to act as a Second Opinion Appointed Doctor, again if securing a Second Opinion Appointed Doctor is likely to be associated with unreasonable delay. There are concerns that these changes may inadvertently lead to an increase in the number of people with IDs detained under the Mental Health Act (1983, as revised in 2007). It is our view that these changes should not be used disproportionately to detain people with IDs within psychiatric hospitals if implemented, and community learning disabilities teams need to work effectively with all authorities during the pandemic to continue to provide excellent care and support to families to help guard against unnecessary admission to hospital continuing to work within the spirit of the Transforming Care (NHS England, 2017) Agenda in England.
Conclusions
The aim of this study was to present our initial guidelines for the care and treatment of people with IDs during the COVID‐19 pandemic, developing best practice guidance. This was prompted by concerns that people with IDs may be afforded poor quality care during the COVID‐19 pandemic, and especially upon contracting SARS‐CoV‐2. In England, these concerns were brought to the fore when the NICE (2020a) recommended using the Clinical Frailty Score to aid decisions about treating individuals who have contracted SARS‐CoV‐2. The guidance was rapidly revised to exclude the use of this score with people with IDs. However, there remain concerns that healthcare services will not prioritize the care of people with IDs and some GP practices have actively stated that they will adopt this course of action (Thomas, 2020).
We have developed our guidance with issues of disparity of healthcare for people with IDs in mind. This is a group that has marked comorbidity (Cooper et al., 2015; O'Leary et al., 2018), and some will be at very high risk of severe illness due to SARS‐CoV‐2 infection because of multi‐morbidity. In the absence of specific criteria for rating risk due to SARS‐CoV‐2 infection among people with IDs specifically, we have opted to adapt the risk criteria published by Public Health England (2020d, 2020f), incorporating mental health and challenging behavior which is prevalent among people with IDs and likely to impact upon the nature of course of contracting SARS‐CoV‐2 as there is a risk of a relapse or increase in both mental health symptoms and/or challenging behavior. There is no direct evidence currently that SARS‐CoV‐2 infection will cause an increase in mental health symptoms and/or challenging behavior at the moment, but the associated changes that are occurring within our society and the required treatments are likely to lead to distress and anxiety among those with IDs. It is our view, at the current time, that adapting the current guidance to include people with IDs who have severe and enduring mental health problems or those who have a substantial risk of an increase in challenging behavior is a reasonable addition.
Community learning disabilities teams and inpatient psychiatric hospitals have an important role in addressing disparity in general healthcare, collaboratively with families and carers, for people with IDs. This role is vital as it will make sure those who need help, get help, when and where it is needed, in the way that it is needed. We should all continue to work towards preventing admission to inpatient psychiatric hospitals and continue to work to facilitate timely and appropriate discharge. Once the pandemic is over, we do not want to be in a position of having an increased number of people with IDs within psychiatric hospitals due to difficulties with managing risk associated with SARS‐CoV‐2 infection or community access, or due to a deterioration in mental health or increase in challenging behavior related to the COVID‐19 pandemic. All health and social care providers need to work together to achieve this goal collaboratively, and community learning disabilities teams, together with their hospital colleagues, are vital providers of care and support.
We have explicitly outlined actions that need to be taken by health and social care staff within both the community and inpatient psychiatric settings to help organize and deliver care to people with IDs, inclusive of their families and carers. This includes the creation of a COVID‐19 care plan for individuals who are at very high risk, creating or updating hospital passports, improving psychological support and communication through the revision of positive behavioral support plans as needed, and the creation of a ceiling of care/treatment escalation plan. The goal of the ceiling of care/treatment escalation plan is to ensure that the wishes of individuals, families, and carers are recorded and followed appropriately, helping to ensure disparity is addressed. IDs are not fatal conditions and should never be the basis for authorizing DNACPR. We recognize that many of these conversations will be distressing for individuals with IDs, their families and carers, and community and inpatient staff who are experienced in providing care and treatment to people with IDs are well placed to provide high quality support and care.
Finally, we fully recognize that our guidance has been contextualized within English policy and law. Healthcare systems around the world differ, and in some countries, there are no specialist teams for people with IDs offering services within the community, residential services or within inpatient psychiatric services. However, we wish to strongly encourage others to take our work and adapt it as needed to meet the needs of their own local, regional, or national populations and to ensure that individuals with IDs exercise their human rights to appropriate healthcare support.
Conflict of Interest
The authors have no conflict of interest to declare
Acknowledgments
We wish to acknowledge the valued work of members of our consultative group in creating this guidance: Saji Alexander (Chelsea and Westminster Hospital NHS Trust), John Devapriam (Worcestershire Health and Care NHS Trust), Satheesh Gangadharan (Leicestershire Partnership NHS Trust), Churunal Hari (Shrewsbury and Telford Hospital NHS Trust and RADiANT), Anne Hunt (Hertfordshire Partnership University NHS Foundation Trust), Anupama Iyer (Hertfordshire Partnership University NHS Foundation Trust), Kasu Kiran (Hertfordshire Partnership University NHS Foundation Trust), Rohit Shankar OBE (Cornwall Partnership NHS Foundation Trust), Andy Smith (Hertfordshire Partnership University NHS Foundation Trust).
References
- Beange, H. , McElduff, A. , & Baker, W. (1995). Medical disorders of adults with mental retardation: A population study. American Journal on Mental Retardation, 99, 595–604. [PubMed] [Google Scholar]
- Beyond Words . (2020). Beating the virus. London: Beyond Words. [Google Scholar]
- British Broadcasting Corporation . (2020). Coronavirus: Autistic support group “told it needed DNR orders”, London: British Broadcasting Corporation. Retrieved from https://www.bbc.co.uk/news/uk‐england‐somerset‐52217868 [Google Scholar]
- Care Quality Commission . (2016). A different ending: Addressing inequalities in end of life care. Newcastle, UK: Care Quality Commission. [Google Scholar]
- Challenging Behaviour Foundation . (2020a). Challenging behaviour—Supporting your loved one at home. London: Challenging Behaviour Foundation. Retrieved from https://www.challengingbehaviour.org.uk/learning‐disability‐assets/3challengingbehavioursupportingyourlovedoneathome.pdf [Google Scholar]
- Challenging Behaviour Foundation . (2020b). Supporting children and adults with severe learning disabilities at home during the cornovirus pandemic. London: Challenging Behaviour Foundation. Retrieved from https://www.challengingbehaviour.org.uk/learning‐disability‐assets/supportingchildrenandadultswithsevrelearningdisabilitesathomeduringthecoronaviruspandemic.pdf [Google Scholar]
- Chester, V. , James, N. , Rogers, I. , Grace, J. , & Alexander, R. (2020). Family experiences of psychiatric services for their relative with intellectual and developmental disabilities. In Bhaumik S. & Alexander R. (Eds.), Oxford textbook of the psychiatry of intellectual disability (pp. 265–274). Oxford, UK: Oxford University Press. [Google Scholar]
- Cooper, S. A. , McLean, G. , Guthrie, B. , McConnachie, A. , Mercer, S. , Sullivan, F. , & Morrison, J. (2015). Multiple physical and mental health comorbidity in adults with intellectual disabilities: Population‐based cross‐sectional analysis. BMC Family Practice, 16, 110. 10.1186/s12875-015-0329-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cooper, S. A. , Smiley, E. , Morrison, J. , Allan, L. , & Williamson, A. (2007). Prevalence of and association with mental ill health in adults with intellectual disabilities. British Journal of Psychiatry, 190, 27–35. [DOI] [PubMed] [Google Scholar]
- Coronavirus Act: The Coronavirus Act, (2020). London: HMSO. [Google Scholar]
- Dong, E. , Du, H. , & Gardner, L. (2020). An interactive web‐based dashboard to track COVID‐19 in real time. The Lancet Infectious Diseases, 20, 533–534. 10.1016/s1473-3099(20)30120-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dunn, K. , Hughes‐McCormack, L. , & Cooper, S. A. (2018). Hospital admissions for physical health conditions for people with intellectual disabilities: Systematic review. Journal of Applied Research in Intellectual Disabilities, 31, 1–10. [DOI] [PubMed] [Google Scholar]
- Emerson, E. , & Hatton, C. (2007). Mental health of children and adolescents with intellectual disabilities in Britain. The British Journal of Psychiatry, 191, 493–499. [DOI] [PubMed] [Google Scholar]
- Equality Act . (2010). London: HMSO.
- Evenhuis, H. , Henderson, C. M. , Beange, H. , Lennox, N. , & Chicione, B. (2000). Healthly ageing—Adults with intellectual disabilities: Physical health issues. Geneva, Switzerland: World Health Organization. [Google Scholar]
- Glover, G. , Williams, R. , Heslop, P. , Oyinlola, J. , & Grey, J. (2017). Mortality in people with intellectual disabilities in England. Journal of Intellectual Disability Research, 61, 62–74. 10.1111/jir.12314 [DOI] [PubMed] [Google Scholar]
- Greenhalgh, T. , Koh, G. C. H. , & Car, J. (2020). Covid‐19: A remote assessment in primary care. BMJ, 368, m1182. 10.1136/bmj.m1182 [DOI] [PubMed] [Google Scholar]
- Guan, W.‐J. , Liang, W.‐H. , Zhao, Y. , Liang, H.‐R. , Chen, Z.‐S. , Li, Y.‐M. , … Wang, T. (2020). Comorbidity and its impact on 1590 patients with Covid‐19 in China: A Nationwide Analysis. European Respiratory Journal. 55, 2000547 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haveman, M. , Heller, T. , Lee, L. , Maaskant, M. , Shooshtari, S. , & Strydom, A. (2010). Major health risks in aging persons with intellectual disabilities: An overview of recent studies. Journal of Policy and Practice in Intellectual Disabilities, 7, 59–69. [Google Scholar]
- Heslop, P. , Blair, P. S. , Fleming, P. , Hoghton, M. , Marriott, A. , & Russ, L. (2014). The confidential inquiry into premature deaths of people with intellectual disabilities in the UK: A population‐based study. The Lancet, 383, 889–895. 10.1016/s0140-6736(13)62026-7 [DOI] [PubMed] [Google Scholar]
- Hosking, F. J. , Carey, I. M. , Shah, S. M. , Harris, T. , DeWilde, S. , Beighton, C. , & Cook, D. G. (2016). Mortality among adults with intellectual disability in England: Comparisons with the general population. American Journal of Public Health, 106, 1483–1490. 10.2105/AJPH.2016.303240 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huang, Y. , Zhou, H. , Yang, R. , Xu, Y. , Feng, X. , & Gong, P. (2020). Clinical characteristics of 36 non‐survivors with COVID‐19 in Wuhan, China. medRxiv. (Under Review). [Google Scholar]
- International Association for the Scientific Study of Intellectual and Developmental Disabilities . (2020). COVID‐19 resources, Hobart, Tasmania: International Association for the Scientific Study of Intellectual and Developmental Disabilities. Retrieved from https://www.iassidd.org/covid-19-resources/ [Google Scholar]
- Krahn, G. L. , Hammond, L. , & Turner, A. (2006). A cascade of disparities: Health and health care access for people with intellectual disabilities. Mental Retardation and Developmental Disabilities Research Reviews, 12, 70–82. [DOI] [PubMed] [Google Scholar]
- MacArthur, J. , Brown, M. , McKechanie, A. , Mack, S. , Hayes, M. , & Fletcher, J. (2015). Making reasonable and achievable adjustments: The contributions of learning disability liaison nurses in “getting it right” for people with learning disabilities receiving general hospitals care. Journal of Advanced Nursing, 71, 1552–1563. [DOI] [PubMed] [Google Scholar]
- Maulik, P. K. , Mascarenhas, M. N. , Mathers, C. D. , Dua, T. , & Saxena, S. (2011). Prevalence of intellectual disability: A meta‐analysis of population‐based studies. Research in Developmental Disabilities, 32, 419–436. 10.1016/j.ridd.2010.12.018 [DOI] [PubMed] [Google Scholar]
- McCarron, M. , Carroll, R. , Kelly, C. , & McCallion, P. (2015). Mortality rates in the general Irish population compared to those with an intellectual disability from 2003 to 2012. Journal of Applied Research in Intellectual Disabilities, 28, 406–413. [DOI] [PubMed] [Google Scholar]
- McKenzie, K. , Milton, M. , Smith, G. , & Ouellette‐Kuntz, H. (2016). Systematic review of the prevalence and incidence of intellectual disabilities: Current trends and issues. Current Developmental Disorders Reports, 3, 104–115. 10.1007/s40474-016-0085-7 [DOI] [Google Scholar]
- Mental Capacity Act: The Mental Capacity Act, (2005). London: HMSO. [Google Scholar]
- Mental Health Act . (1983, as revised in 2007). London: HMSO.
- National End of Life Care Programme . (2011). The route to success in end of life care—Achieving quality for people with learning disabilities, London: National Health Service. [Google Scholar]
- National Institute for Health and Care Excellence . (2016). Mental health problems in people with learning disabilities: Prevention, assessment and management [NG54], London: National Institute for Health and Care Excellence. [PubMed] [Google Scholar]
- National Institute for Health and Care Excellence . (2020a). COVID‐19 rapid guideline: Critical care in adults. NICE Guideline [NG159], London: National Institute for Health and Care Excellence. https://www.nice.org.uk/guidance/ng159 [Google Scholar]
- National Institute for Health and Care Excellence . (2020b). NICE updates rapid COVID‐19 guideline on critical care, London: National Institute for Health and Care Excellence. Retrieved from https://www.nice.org.uk/news/article/nice-updates-rapid-covid-19-guideline-on-critical-care [Google Scholar]
- NHS England . (2017). Delivering high quality end of life care for people who have a learning disabiilty, London: NHS England. [Google Scholar]
- NHS England . (2020a). Clinical guide for front line staff to support the management of patients with a learning disability, autism or both during the coronavirus pandemic—Relevant to all clinical specialities, London: NHS England. Retrieved from https://www.england.nhs.uk/coronavirus/wp‐content/uploads/sites/52/2020/03/C0031_Specialty‐guide_LD‐and‐coronavirus‐v1_‐24‐March.pdf [Google Scholar]
- NHS England . (2020b). Letter from Claire Murdoch, London: National Mental Health Director, NHS England and NHS Improvement. Retrieved from. https://www.england.nhs.uk/coronavirus/wp‐content/uploads/sites/52/2020/04/C0166‐Letter‐DNACPR.pdf [Google Scholar]
- Nocon, A. , Sayce, L. , & Nadirshaw, Z. (2008). Health inequalities experienced by people with learning disabilities: Problems and possibilities in primary care. Tizard Learning Disability Review, 13, 28–36. [Google Scholar]
- O'Leary, L. , Cooper, S. A. , & Hughes‐McCormack, L. (2018). Early death and causes of death of people with intellectual disabilities: A systematic review. Journal of Applied Research in Intellectual Disabilities, 31, 325–342. 10.1111/jar.12417 [DOI] [PubMed] [Google Scholar]
- Public Health England (2020a). Coronavirus (COVID‐19): Personal protective equipment (PPE) hub. In Guidance about coronavirus (COVID‐19) personal protective equipment (PPE). London, UK: Author. [Google Scholar]
- Public Health England . (2020b). COVID‐19: Guidance on residential care provision. London, UK: Author. [Google Scholar]
- Public Health England . (2020c). COVID‐19: Investigation and initial clinical management of possible cases. London, UK: Author. [Google Scholar]
- Public Health England . (2020d). Guidance on shielding and protecting people who are clinically extremely vulnerable from COVID‐19. London, UK: Author. [Google Scholar]
- Public Health England . (2020e). The health protection (coronavirus, restrictions) (England) regulations. London, UK: Author. [Google Scholar]
- Public Health England . (2020f). Staying at home and away from others (social distancing). London, UK: Author. [Google Scholar]
- Regnard, C. , Reynolds, J. , Watson, B. , Matthews, D. , Gibson, L. , & Clarke, C. (2007). Understanding distress in people with severe communication difficulties: Developing and assessing the Disability Distress Assessment Tool (DisDAT). Journal of Intellectual Disability Research, 51, 277–292. [DOI] [PubMed] [Google Scholar]
- Reiss, S. , Levitan, G. W. , & Szyszko, J. (1982). Emotional disturbance and mental retardation: Diagnostic overshadowing. American Journal of Mental Deficiency. 86, 567–574. [PubMed] [Google Scholar]
- Remuzzi, A. , & Remuzzi, G. (2020). COVID‐19 and Italy: What next? The Lancet., 395, 1225–1228. 10.1016/s0140-6736(20)30627-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Richardson, S. , Hirsch, J. S. , Narasimhan, M. , Crawford, J. M. , McGinn, T. , Davidson, K. W. , … Zanos, T. P. (2020). Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID‐19 in the New York City area. Journal of the American Medical Association, 323, 2052–2059. 10.1001/jama.2020.6775 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robertson, J. , Chadwick, D. , Baines, S. , Emerson, E. , & Hatton, C. (2017). Prevalence of dysphagia in people with intellectual disability: A systematic review. Intellectual and Developmental Disabilities, 55, 377–391. [DOI] [PubMed] [Google Scholar]
- Rockwood, K. , Song, X. , MacKnight, C. , Bergman, H. , Hogan, D. B. , McDowell, I. , & Mitnitski, A. (2005). A global clinical measure of fitness and frailty in elderly people. CMAJ, 173, 489–495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Royal College of Physicians . (2017). National early warning score (NEWS)‐2, London: Royal College of Physicians. Retrieved from https://www.rcplondon.ac.uk/projects/outputs/national‐early‐warning‐score‐news‐2 [Google Scholar]
- The Coronavirus Act (2020). London: HMSO.
- The Learning Disability Mortality Review (LeDeR) Programme . (2019). Annual report—2018. Bristol, UK: University of Bristol. [Google Scholar]
- The Mental Capacity Act . (2005). London: HMSO.
- Thomas, R. (2020). Learning disabilities patients told they may be “too frail” for mechanical ventilation if they get COVID‐19. Health Service Journal, London: Wilmington Healthcare Limited. Retrieved from. https://www.hsj.co.uk/coronavirus/learning‐disabilities‐patients‐told‐they‐may‐be‐too‐frail‐for‐mechanical‐ventilation‐if‐they‐get‐covid‐19/7027318.article [Google Scholar]
- Transforming Care: NHS England, (2017). Transforming Care ‐ ModelService Specifications: Supporting implementation of the service model, London: NHS England. [Google Scholar]
- Voss, H. , Vogel, A. , Wagemans, A. M. , Francke, A. L. , Metsemakers, J. F. , Courtens, A. M. , & de Veer, A. J. (2017). Advance care planning in palliative care for people with intellectual disabilities: A systematic review. Journal of Pain and Symptom Management, 54, 938–960.e931. [DOI] [PubMed] [Google Scholar]
- Wu, Y. , Xu, X. , Chen, Z. , Duan, J. , Hashimoto, K. , Yang, L. , … Yang, C. (2020). Nervous system involvement after infection with COVID‐19 and other coronaviruses. Brain, Behavior, and Immunity. 10.1016/j.bbi.2020.03.031. (in press) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wu, Z. , & McGoogan, J. M. (2020). Characteristics of and important lessons from the coronavirus disease 2019 (COVID‐19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. Journal of the American Medical Association, 323, 1239. 10.1001/jama.2020.2648 [DOI] [PubMed] [Google Scholar]
- Zhou, F. , Yu, T. , Du, R. , Fan, G. , Liu, Y. , Liu, Z. , … Cao, B. (2020). Clinical course and risk factors for mortality of adult inpatients with COVID‐19 in Wuhan, China: A retrospective cohort study. The Lancet, 395, 1054–1062. 10.1016/s0140-6736(20)30566-3 [DOI] [PMC free article] [PubMed] [Google Scholar]