

Editor,
The novel coronavirus, otherwise known as COVID‐19, has fast become a major health concern. 1 , 2 It has been reported that in addition to the conventional respiratory symptoms, patients also display skin manifestations such as Urticaria and angioedema. 3 Here, we present a case study of an elderly man who first presented with generalized pruritic hives ranging from 1.5 to 8.0 cm in diameter on the 5th of March 2020 (Fig. 1). The patient was investigated for another differential diagnosis of Urticaria such as parasitic and bacterial infection, for which negative results were found. On the 5th of March 2020, the patient reported these symptoms plus general malaise, fatigue, 37.90°C temperature and sore throat. Initial biochemical tests showed that the patient presented with low numbers of white blood cells (WBC) (WBC = 2.75 × 103). The most hallmark issue, which is lymphopenia, was detected in this case (lymphocytes = 852). 4 The other blood tests results were found to be normal. Real‐time polymerase chain reaction (RT‐PCR) for COVID‐19 was not performed due to the time lapse between starting the symptoms and hospital admission. Therefore, the CT chest was carried out, which showed pneumonia with bilateral and subpleural areas of ground‐glass opacification, consolidation affecting the lower lobes and confirming the diagnosis of COVID‐19 (Fig. 2).
Figure 1.
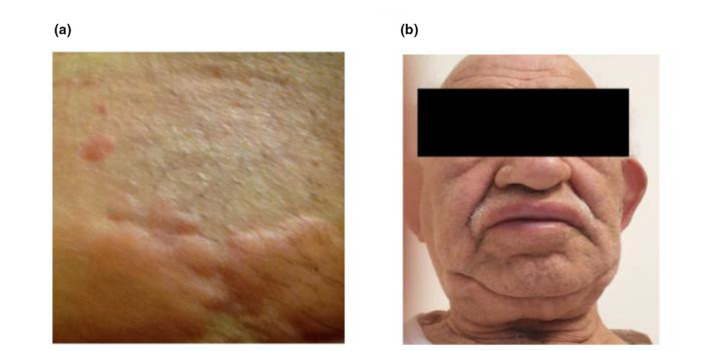
(a) shows cutaneous manifestation of urticaria. (b) Male patient displaying angioedema.
Figure 2.
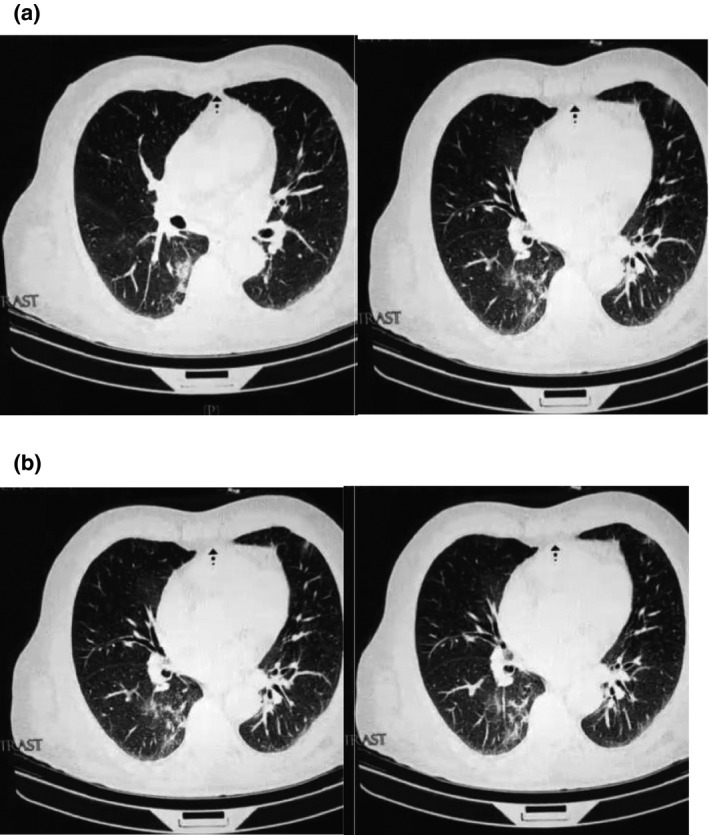
Patient CT chest at the time of hospital admission (a–d).
The relationship between Urticaria and infection has rarely been reported; this is probably due to the difficulty in establishing a cause and effect relationship. 5 Literature suggests that Urticaria and angioedema can be induced by viral and bacterial infection. 6 , 7 Urticaria has previously been associated with Cytomegalovirus, Herpesvirus and Epstein–Barr virus. A systematic review undertaken in 2016 found that viral infections could also act as potential triggers and sometimes even as the main etiologic agent in causing both acute and chronic Urticaria. Additionally, they found that in adults, hepatitis viral infections appeared to be the most frequent cause of Urticaria, whereas, in children, herpesviral infections were more frequent. To further support these data, it was also found that urticarial manifestations cleared up after the viral infections were treated or controlled. 5 Another study found that acute Urticaria is a common manifestation of viral infections for both children and adults but more so for children. Infections were also identified as the primary cause of Urticaria in approximately 37% of cases. 8
Currently, there are no significant data regarding the association between skin manifestations such as Urticaria and COVID‐19. 9 One study, in which a group of dermatologists analysed the cutaneous involvement in COVID‐19, found that from 88 patients, 20.4% portrayed cutaneous manifestation. Of these, 8 patients developed the manifestations at disease onset whereas 10 developed the manifestations after hospitalization. These cutaneous manifestations presented themselves as erythematous rash, widespread Urticaria and chickenpox‐like vesicles. From these data, it can be speculated that the skin manifestations observed with COVID‐19 may be similar to the cutaneous involvement that is often seen during common viral infections. 9 Another case was recently seen in Bangkok, a patient presented with only a skin rash, petechiae and a low platelet count and was thus diagnosed with Dengue fever; however, after the patient was admitted with respiratory problems, the correct diagnosis for COVID‐19 was made. 10 This further highlights a possible association between skin manifestations and the novel coronavirus.
This report presents evidence regarding a possible association between urticarial skin manifestations in the early stages of COVID‐19, and thus, its used as a possible early diagnostic indicator. The patient may initially present with a skin rash such as Urticaria, which can cloud the diagnosis, resulting in misdiagnosis for another common disease. Clinicians should take this report into considerations in order to prevent misdiagnosis as well to allow early diagnosis and better patient outcomes.
References
- 1. Huang C, Wang Y, Li X et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2019; 2020: 395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Liu T, Hu J, Kang M, Lin L, Zhong H, Xiao J, He G, Song T, Huang Q, Rong Z, Deng A, Zeng W, Tan X, Zeng S, Zhu Z, Li J, Wan D, Lu J, Deng H, Ma W. Transmission dynamics of 2019 novel coronavirus (2019‐nCoV), 2020.
- 3. Sachdeva M, Gianotti R, Shah M et al. Cutaneous manifestations of COVID‐19: Report of three cases and a review of literature. J Dermatol Sci 2020; S0923‐1811(20)30149‐3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Tan L, Wang Q, Zhang D, Ding J, Huang Q, Tang Y‐Q, Wang Q, Miao H.Lymphopenia predicts disease severity of COVID‐19: a descriptive and predictive study, 2020. [DOI] [PMC free article] [PubMed]
- 5. Imbalzano E, Casciaro M, Quartuccio S et al. Association between urticaria and virus infections: a systematic review. Allergy Asthma Proc 2016; 37: 18–22. [DOI] [PubMed] [Google Scholar]
- 6. Yong S‐B, Yeh W‐C, Wu H‐J et al. Impact of mycoplasma pneumonia infection on Urticaria: A nationwide, population‐based retrospective cohort study in Taiwan. PLoS One 2019; 14: e0226759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Zuberbier T. Urticaria. Allergy 2003; 58: 1224–1234. [DOI] [PubMed] [Google Scholar]
- 8. Wedi B, Raap U, Wieczorek D, Kapp A. Urticaria and infections. Allergy Asthma Clin Immunol 2009; 5: 10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Recalcati S. Cutaneous manifestations in COVID‐ 19: a first perspective. J Eur Acad Dermatol Venereol 2020; 34: e212–e213. [DOI] [PubMed] [Google Scholar]
- 10. Joob B, Wiwanitkit V. COVID‐19 can present with a rash and be mistaken for Dengue. J Am Acad Dermatol 2020; 82(5): e177. [DOI] [PMC free article] [PubMed] [Google Scholar]
Acknowledgements
First and foremost, we express our deepest gratitude to the doctors and nurses who work on the front line, battling each day against this COVID‐19 pandemic. We thank the medical teams who, with each shift, risk their own lives to save those of their patients. Also, we acknowledge that the patients in this manuscript have given written informed consent to the publication of their case details.