

Abstract
Objective
To explore the leg length balance in total hip arthroplasty (THA) with shortening subtrochanteric osteotomy (SSTO) or not for unilateral Crowe type IV developmental dysplasia of the hip (DDH) through the evaluation of postoperative full‐length anteroposterior radiographs.
Methods
The postoperative radiographs of 60 patients with unilateral Crowe type IV DDH from July 2012 to May 2019 were retrospectively reviewed. All patients underwent THA using the Pinnacle Acetabular Cup system, a ceramic liner and femoral head, and the S‐ROM stem with a proximal sleeve or cone. Patients with leg length discrepancy (LLD) < 10 mm were defined as the non‐LLD group. To identify differences associated with SSTO, the group was further divided into two groups based on whether the patient underwent SSTO. A total of 48 patients (26 for SSTO and 22 for non‐SSTO) were in the non‐LLD group. There were 3 male and 45 female patients. The mean age of the patients in the non‐LLD group was 39 years. These data, including leg length, femoral length, the height of center of rotation (COR) of the hip, the depth of the sleeve or cone in the femoral medullary canal and the height of the greater trochanter, were measured.
Results
In the non‐LLD group, the femoral lengths in both SSTO and non‐SSTO groups were significantly shorter on the operated side compared with the contralateral side, and the mean discrepancy in the SSTO group was approximately equal to the mean length of the SSTO. The mean height of the COR of the hip on the operated sides in both SSTO and non‐SSTO groups was 13.2 mm, and the contralateral sides were 15.2 and 15.5 mm, respectively. The depth of the sleeve or cone in the femoral medullary canal between SSTO and non‐SSTO groups was 21.7 and 30.6 mm, respectively. The depth of the sleeve or cone in the SSTO group was negatively correlated with the length of SSTO. The heights of the greater trochanter in the operated and contralateral sides were 5.3 and 16.6 mm in the SSTO group, and 13.2 and 17.2 mm in the non‐SSTO group, respectively.
Conclusions
Shortening subtrochanteric osteotomy led to femoral shortening on the operated side for patients with unilateral Crowe type IV DDH. The position of the sleeve or cone should be close to the apex of the greater trochanter to compensate the length of the SSTO. The position of the sleeve or cone without SSTO should be adjusted to make sure that the height of the greater trochanter on the operated side is close to that on the contralateral side.
Keywords: Developmental dysplasia of the hip, Leg length discrepancy, Shortening subtrochanteric osteotomy, Total hip arthroplasty
Introduction
Developmental dislocation of the hip (DDH) describes a whole range of abnormalities involving the developing hip, including subluxation or irreducible dislocation, instability, and dysplasia of the femur and the acetabulum1, 2, 3. The Crowe classification system is proposed to characterize the DDH of adults in most published studies4, 5, 6, 7, because it is instructive for surgery. The Crowe classification system is used to assess the degree of dysplasia on an anteroposterior pelvic radiograph, and the ratio of distance between the femoral head–neck junction and the inferior teardrop to the height of pelvis is calculated8. Crowe type I has <10% subluxation, type II has between 10% and 15% subluxation, type III has between 15% and 20% subluxation, and type IV has >20% subluxation, indicating complete dislocation.
Unilateral Crowe type IV DDH is one of the most severe femur and acetabulum morphologic deformities, and results in hip and low‐back pain, a limp, compensatory scoliosis of the spine, and leg length discrepancy (LLD)9, 10. Total hip arthroplasty (THA) is one of the most effective operations to alleviate pain, improve function, and rectify compensatory scoliosis of the spine and LLD7, 9, 11. The anatomical abnormalities in Crowe type IV DDH, including the small shallow acetabulum, the narrow and stovepipe‐shaped proximal femur and excessive femoral anteversion, make THA more technical challenging5, 12, 13, 14. As recommended in many studies, the acetabular cup was located in the true acetabular region and a modular implant was used to accommodate the shape of the dysplastic femur5, 10, 15. Despite careful preoperative planning and accurate surgical techniques, complications can occur after THA. LLD is a frequent postoperative complication. LLD not only leads to gait asymmetry but also results in an increasing risk of prosthesis failure16, 17, and may have negative effects on postoperative recovery and patient satisfaction.
In the setting of Crowe type IV DDH, femoral shortening osteotomy may be necessary to safely reduce the hip to the true acetabulum, mitigate hip soft‐tissue contractions, and protect the neurovascular structures12. The most commonly used method is shortening subtrochanteric osteotomy (SSTO)3, 4. Several surgical techniques may be needed to achieve appropriate leg length. Unfortunately, it is difficult to achieve equal leg length due to the variation of femurs, acetabulums and tibias, and there are no guidelines that enable the surgeon to achieve equal leg length.
The purpose of the present study was: (i) to determine the LLD based on the postoperative full‐length standing anteroposterior radiographs in patients with unilateral Crowe type IV DDH; (ii) to measure the femoral length, the height of the center of rotation (COR) of the hip, the height of the greater trochanter on both sides, and the depth of the sleeve or cone in the femoral medullary canal on the operative side; and (iii) to analyze the influence of SSTO on the above measurements in non‐LLD patients.
Patients and Methods
Inclusion and Exclusion Criteria
The inclusion criteria were: (i) adult patients with unilateral Crowe type IV DDH with extreme impairment of daily life; (ii) patients who underwent THA by a single surgeon in our institution; (iii) patients divided into two groups based on whether or not they had SSTO during THA; (iv) outcome measures are leg length, femoral length, height of COR of the hip, depth of the sleeve or cone in the femoral medullary canal, and the height of the greater trochanter; and (v) retrospective study. The exclusion criteria included: (i) patients with prior hip or pelvic surgery, residual DDH (infection and trauma), surgery on the tibia, flexion contracture of the hip, and knee flexion deformity; and (ii) patients with a history of cerebral palsy and poliomyelitis.
Patients
We retrospectively reviewed the radiographic data of 87 patients in our institution with unilateral Crowe type IV DDH between July 2012 and May 2019. A total of 27 patients were excluded for the following reasons: 10 for prior hip or pelvic surgery, 8 for residual DDH (infection and trauma), and 9 because there were no postoperatively full standing anteroposterior radiographs. The remaining 60 patients were included in the study. The ethics committee of our hospital, the General Hospital of Chinese People's Liberation Army, approved the study protocol. All the study participants provided written informed consent for the study.
Surgery
All patients underwent THA by a single surgeon (Y. G. Zhou). The procedure has been described in detail in our previous studies5, 10. Briefly, a posterolateral approach was used in all patients. The hyperplastic capsule was removed to expose the true acetabulum; a cementless acetabular cup was placed at the level of the true acetabulum by reaming acetabulum posteriorly and inferiorly. The acetabular cup was fixed by two screws. If it was difficult to reduce the hip, the SSTO was performed. The position of osteotomy was located at the distal end of the sleeve or cone. The osteotomy length equaled the distance between the true acetabular center and the femoral head center during the trial reduction minus 15 mm. Cerclage wiring (two or three steel wires) was done around the location of the osteotomy to prevent fractures. A sleeve or cone was chosen based on the proximal femoral intramedullary morphology, and the femoral component was selected as the one that best matched the femoral intramedullary canal. The hip and knee were always held in extreme flexion to relax the sciatic nerve after successful reduction and this position was maintained for several days.
The Pinnacle Acetabular Cup system, a Biolox Delta ceramic liner and femoral head, and an S‐ROM titanium alloy femoral stem with a titanium sintered proximal sleeve or cone (DePuy, Warsaw, Indiana, USA) were used in all patients.
Groups According to Leg Length Discrepancy and Shortening Subtrochanteric Osteotomy
All patients were classified based on LLD after THA. Patients with LLD < 10 mm16 (either shorter or longer) were defined as the non‐LLD group, whereas patients with LLD ≥ 10 mm were defined as the LLD group. To identify differences associated with SSTO, each group was further divided into two groups based on whether or not patients underwent SSTO.
Radiograph Data
The postoperative full‐length standing anteroposterior radiographs were acquired in the follow‐up period (at least 3 months). A Revolution XR/d digital imaging system (GE Healthcare, Milwaukee, WI, USA) was used with the standard radiographic procedure18. We followed the methods of Zhang et al 9. The patient stood facing the X‐ray tube, and the film‐focus distance was 200 cm. The system could be set at 70 to 90 kVp and 100 to 200 mA according to the height and weight of the patient. Each leg was internally rotated (15 degree) to ensure that the patella was located anteriorly. The beam was parallel to the ground when moving from the pelvis to the ankles, enabling the system to acquire six overlapping radiographs9. Then the system combined all radiographs into one full‐length standing anteroposterior radiograph. All the radiographs were viewed and measured on a picture archiving and communication system (PACS, UniWeb Viewer, version 4.0, EBM technologies)9.
The actual values for each measurement were obtained by calibration using the known diameter of the ceramic femoral head for references. All radiographs on the blinded images for measurement were presented in random order to ensure that the investigator was blind to the patient's data.
Measurement Details
Four measurements were made bilaterally on the full‐length standing anteroposterior radiographs of each patient:
Leg Length
The length of the lower limb was defined as leg length, which was measured as the distance from the teardrop to the center of the ankle joint (when the teardrop on the operated side was covered after THA, which was confirmed through the preoperative radiograph) (Fig. 1). The discrepancy of the bilateral leg length was defined as LLD.
Figure 1.

The measurements of leg length and femoral length on the full‐length standing anteroposterior radiograph: (A) leg length and (B) femoral length.
Femoral Length
The anatomical length of the femur was defined as femoral length, which was measured as the distance from the apex of greater trochanter to the articular surface of the lateral femoral condyle (Fig. 1).
Height of Greater Trochanter
The height of the apex of the greater trochanter relative to the interteardrop line was defined as the height of the greater trochanter, which was measured as the vertical distance from the apex of the greater trochanter to the interteardrop line (Fig. 2).
Figure 2.
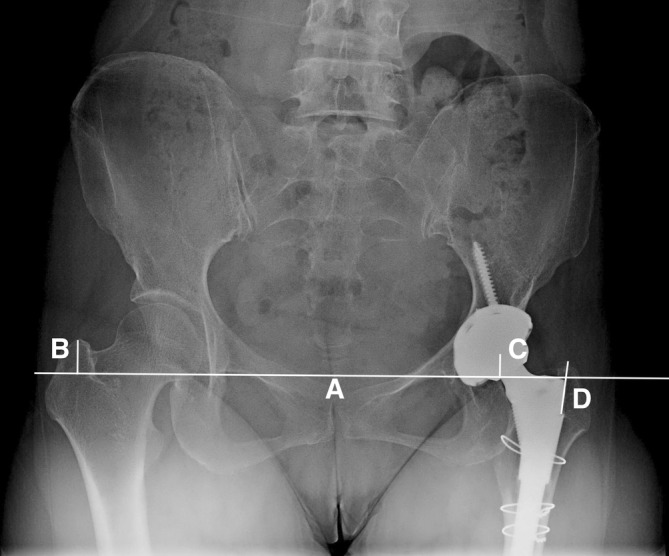
The measurements around hip joint on the radiograph. (A) Teardrop line. (B) Height of greater trochanter. (C) Height of rotational center of hip. (D) Depth of the sleeve or cone.
Height of Center of Rotation
The height of the center of the rotation of the femoral head or acetabular cup relative to the interteardrop line was defined as the height of the COR, which was measured as the vertical distance from the COR of the hip to the interteardrop line19 (Fig. 2).
One measurement was made on the operated side, the depth of the sleeve or cone.
Depth of the Sleeve or Cone
The implanted depth of the sleeve or cone in the femoral medullary canal was defined as the depth of the sleeve or cone, which was measured as the vertical distance from the apex of the greater trochanter to the proximal end of the sleeve or cone (Fig. 2).
Statistical Analysis
Categorical data were compared using a χ2‐test. A paired samples t‐test or Wilcoxon test was used to compare continuous data between the operated and contralateral sides. An independent‐samples t‐test or Mann–Whitney U‐test was used to compare continuous data between the SSTO and non‐SSTO groups.
The correlation analysis was tested using Pearson's correlation coefficients. All tests were performed using SPSS version 25 (IBM, Armonk, NY, USA). Continuous data were given as the mean and standard deviation. A P‐value <0.05 was considered significant in all analysis.
Results
Demographic Results
Of the 60 patients, the mean LLD was 3.0 ± 9.7 mm. In the SSTO group (36 patients), the operated side was shorter than the contralateral side in 32 patients (88.9%), and 4 patients (11.1%) had longer operated sides. In the non‐SSTO group (24 patients), the operated side was shorter than the contralateral side in 10 patients (41.7%), and 14 patients (58.3%) had longer operated sides (Fig. 3). There were 48 patients in the non‐LLD group and 12 were in the LLD group.
Figure 3.
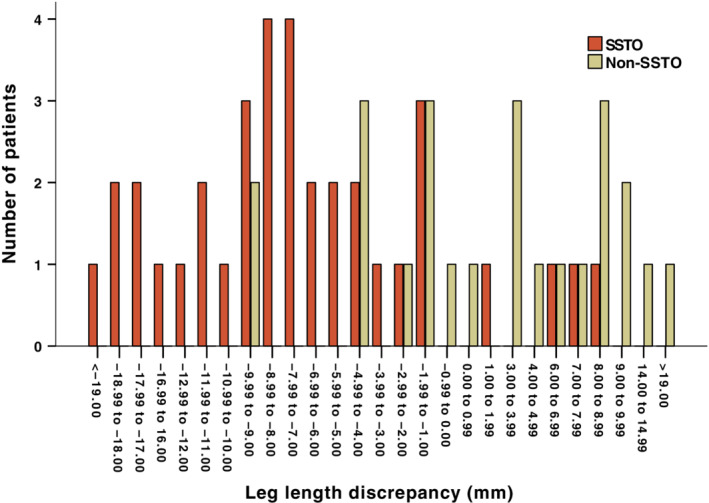
The figure demonstrates the leg length discrepancy (LLD) of all the patients for this study. SSTO, shortening subtrochanteric osteotomy.
Patient demographic characteristics for the non‐LLD group are shown in Table 1. There were no significant differences between SSTO and non‐SSTO groups in terms of gender, age, height, weight, BMI, side, and sleeve or cone.
Table 1.
Patient demographic and clinical characteristics in non‐LLD group
| Variable | SSTO | Non‐SSTO | P‐values |
|---|---|---|---|
| Patients (n) | 26 | 22 | |
| Gender (n) | 0.654 | ||
| Male | 2 (8%) | 1 (5%) | |
| Female | 24 (92%) | 21 (95%) | |
| Age (yrs)* | 39.9 ± 12.2 | 38.1 ± 10.7 | 0.555 |
| Height (cm)* | 158.4 ± 6.2 | 160.0 ± 5.6 | 0.325 |
| Weight (kg)* | 56.7 ± 9.7 | 58.5 ± 10.9 | 0.547 |
| BMI (kg/m2)* | 22.5 ± 3.0 | 22.8 ± 3.9 | 0.791 |
| Side (n) | 0.371 | ||
| Right | 14 (54%) | 9 (41%) | |
| Left | 12 (46%) | 13 (59%) | |
| Sleeve or cone (n) | 0.164 | ||
| Sleeve | 23 (88%) | 16 (73%) | |
| Cone | 3 (12%) | 6 (27%) |
BMI, body mass index; LLD, leg length discrepancy; SSTO, shortening subtrochanteric osteotomy.
The values are given as the mean and standard deviation.
Radiographic Results in Non‐Leg Length Discrepancy Group
In the non‐LLD group, 26 patients underwent SSTO and the mean length of SSTO was 29.0 ± 7.9 mm. There were 22 patients in the non‐SSTO group. The parameters of measurements on the full‐length standing anteroposterior radiographs are shown in Table 2.
Table 2.
Parameters of measurements on the full‐length standing anteroposterior radiographs in non‐LLD group
| Parameter (mm) | SSTO (n = 26) | Non‐SSTO (n = 22) | P‐value* | ||||
|---|---|---|---|---|---|---|---|
| Operated side | Contra‐side | P‐value | Operated side | Contra‐side | P‐value | ||
| Leg length | 680.6 ± 38.1 | 684.9 ± 40.0 | <0.001 | 698.8 ± 41.2 | 697.1 ± 43.1 | 0.226 | 0.120 |
| Femoral length | 358.6 ± 23.1 | 388.6 ± 21.0 | <0.001 | 387.5 ± 23.5 | 391.2 ± 27.1 | 0.022 | <0.001 |
| Height of center of rotation of hip | 13.2 ± 4.0 | 15.2 ± 2.2 | 0.046 | 13.2 ± 6.3 | 15.5 ± 3.3 | 0.157 | 0.980 |
| Height of the greater trochanter | 5.3 ± 9.3 | 16.6 ± 5.9 | <0.001 | 13.2 ± 7.5 | 17.2 ± 6.6 | 0.077 | 0.003 |
| Depth of the sleeve or cone | 21.7 ± 7.0 | ‐ | — | 30.6 ± 7.0 | — | — | <0.001 |
The values are given as the mean and standard deviation. If the value is negative, the height of the rotational center of the hip is below the greater trochanter. SSTO, shortening subtrochanteric osteotomy.
P‐values means the differences between the operated side of SSTO and non‐SSTO groups.
Leg Length
In the SSTO group, the leg length on the operated side was shorter, by an average of 4.3 ± 5.2 mm, than that on the contralateral side. The mean leg lengths of the operated and contralateral sides were 680.6 ± 38.1 mm and 684.9 ± 40.0 mm, respectively (P < 0.001). In the non‐SSTO group, the leg length on the operated side was longer, by an average of 1.6 ± 6.1 mm, than that on the contralateral side. The mean leg lengths of the operated and contralateral sides were 698.8 ± 41.2 mm and 697.1 ± 43.1 mm, respectively (P = 0.226).
Femoral Length
In the SSTO group, compared with the contralateral side, the femoral length of the operated side was significantly shorter, by a mean of 30.0 ± 10.4 mm. The mean femoral lengths of the operated and contralateral sides were 358.6 ± 23.1 mm and 388.6 ± 21.0 mm, respectively (P < 0.001). The discrepancy of the femoral length on contralateral and operated sides was positively correlated with the length of SSTO (r = 0.683, P < 0.001) (Fig. 4). In non‐SSTO group, the mean femoral lengths of the operated and contralateral sides were 387.5 ± 23.5 mm and 391.2 ± 27.1 mm, respectively (P = 0.022).
Figure 4.

Correlation between the discrepancy of the femoral length on contralateral and operated sides and the length of shortening subtrochanteric osteotomy (SSTO) in the non‐LLD group.
Height of Center of Rotation
In the SSTO group, the height of the COR of the hip on the operated side (13.2 ± 4.0 mm) was lower, by an average of 2.0 ± 4.9 mm, than that on the contralateral side (15.2 ± 2.2 mm) (P = 0.046). In the non‐SSTO group, the height of the COR of the hip on the operated side (13.2 ± 6.3 mm) was lower, by an average of 2.3 ± 7.3 mm, than that on the contralateral side (15.5 ± 3.3 mm) (P = 0.157).
Height of Greater Trochanter
In the SSTO group, the heights of the greater trochanter of the operated and contralateral sides were 5.3 ± 9.3 mm and 16.6 ± 5.9 mm (P < 0.001). In the non‐SSTO group, the height of the greater trochanter of the operated and contralateral sides were 13.2 ± 7.5 mm and 17.2 ± 6.6 mm, respectively (P = 0.077).
Depth of the Sleeve or Cone
The mean depths of the sleeve or cone between SSTO and non‐SSTO groups were 21.7 ± 7.0 mm and 30.6 ± 7.0 mm, respectively (P < 0.001). The depth of the sleeve or cone in the SSTO group was negatively correlated with the length of the SSTO (r = −0.632, P = 0.001) (Fig. 5).
Figure 5.
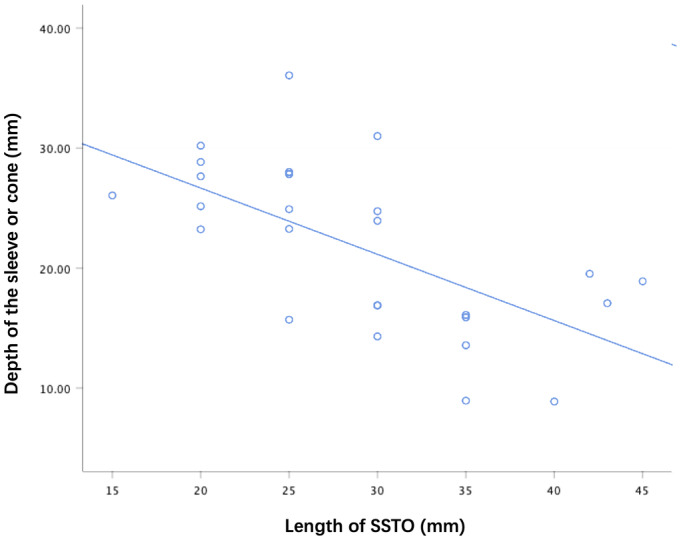
Correlation between the depth of the sleeve or cone and the length of shortening subtrochanteric osteotomy (SSTO) in the non‐LLD group.
Reasons of Leg Length Discrepancy in the Leg Length Discrepancy Group
The reasons for LLD were analyzed in the LLD group. In the SSTO group, 5 patients had length of SSTO >35 mm, three had depth of sleeve or cone >25 mm, and two had length of SSTO >35 mm and depth of sleeve or cone >25 mm. In the non‐SSTO group, the tibial length of two patients on the operated side was longer than that on contralateral side (the discrepancy of the tibial length was 12.0 and 18.0 mm, respectively).
Discussion
Leg Length Discrepancy after Total Hip Arthroplasty in Crowe Type IV Developmental Dysplasia of the Hip
Leg length discrepancy after THA with Crowe type IV DDH remains a major problem. Park et al.20 reported that the mean LLD after THA was 36 mm in 25 Crowe type IV DDH. Wang et al.21 also found postoperative LLD between 10 mm and 20 mm in 39% of patients. The leg length balance in THA for patients with unilateral Crowe type IV DDH remains a major problem. During THA, the height of the COR of the hip, the length of the SSTO, and the depth of the sleeve or cone could affect the operated leg length. Balancing the relationship of the above factors to obtain a perfect THA is challenging for surgeons. In this study, we retrospectively reviewed the radiographic data of all patients with unilateral Crowe type IV DDH and explored how to equalize the leg length through adjusting the relationship of the three factors in THA.
Height of the Center of Rotation of the Acetabular Cup in Crowe Type IV Developmental Dysplasia of the Hip
In Crowe type IV DDH, THA with placement of an acetabular cup in the false acetabulum or high hip center is an easier procedure, but cannot equalize the leg length, and leads to problems with fixation, stability, and the restoration of appropriate hip biomechanics12, 22. The placement of the cup in the true acetabulum is imperative5, 10, 20, 21. Zhou et al.10 found that it was entirely feasible to make a 46‐mm acetabular cup combined with CoC bearing in the true acetabulum by reaming acetabulum posteriorly and inferiorly using finite element analysis and clinical results. All cups were stable at a mean duration of 3.7 years follow‐up. Erdem et al.23, in a study of 26 hips with Crowe type IV DDH that were reconstructed in the true acetabulum (the height of COR of hip: 15 mm), found that all the cups were stable at a mean follow up of 7.1 years. In our study, the procedure of reconstructing the acetabular cup followed the methods of Zhou et al 10. The acetabular cup was located in the posterior and inferior position in the true acetabular region. The mean heights of the COR of the hip on the operated sides of both SSTO and non‐SSTO groups were 13.2 mm, and of the contralateral sides were 15.2 and 15.5 mm, respectively.
Effect of Shortening Subtrochanteric Osteotomy on the Femoral Length and Height of Greater Trochanter
Femoral shortening osteotomy could be an effective method to safely reduce the cup to the true acetabulum and could also protect the neurovascular tissues. The most commonly used method of osteotomy is SSTO5, 14, 21. SSTO can be performed by using several techniques, including transverse, oblique, Z‐shaped, and V‐shaped osteotomy. Muratli et al. found no difference with regard to stability of the four techniques during loading testing in a biomechanical laboratory setting24. In our study, 26 patients underwent transverse SSTO, and the mean length of SSTO was 29.0 mm in the non‐LLD group. The mean femoral length on the operated side was significantly shorter compared with that on the contralateral side, and the mean discrepancy was approximately equal to the mean length of SSTO. The mean height of the greater trochanter was also lower than that on the contralateral side after SSTO.
Effect of the False Acetabulum on Shortening Subtrochanteric Osteotomy
Not all the Crowe type IV DDH need the SSTO. Some factors or methods are reported to be able to achieve hip reduction without SSTO, such as the false acetabulum before THA, muscle release or tenotomy, and injection of muscle relaxant3, 4, 25, 26. According to our study, 22 patients did not undergo SSTO in the non‐LLD group. The false acetabula were present in 21 patients. False acetabulum may be an important factor determining SSTO application.
Effect of Shortening Subtrochanteric Osteotomy on the Depth of Sleeve or Cone
The depth of the sleeve or cone in the femoral medullary canal was an important indicator for adjusting the LLD, after which that the cup was reconstructed in the true acetabulum. In the SSTO group, the SSTO led to the femoral shortening on the operated side. The sleeve or cone should be positioned close to the greater trochanter to compensate the length of SSTO. In the non‐SSTO group, the depth of the sleeve or cone should be adjusted to ensure that the height of the greater trochanter on the operated side is close to that on the contralateral side. The sleeve or cone in the non‐SSTO group was deeper than that in the SSTO group.
Limitations of the Study
To the best of our knowledge, this is the first study comparing SSTO and no SSTO in THA for LLD. The study explored the leg length balance in THA with or without SSTO for unilateral Crowe type IV DDH. However, there are also several limitations in the present study. First, this is a retrospective study with a relatively small number of patients in each group. The second limitation of our study is the lack of measurements using preoperative full‐length standing anteroposterior radiographs, such as the height of dislocation and the length of the femur and the tibia on the operated side, which may be influencing factors for SSTO and leg length. Finally, all surgeries were performed in the single institution by a single surgeon, which could have affected the results of this study.
Conclusion
The acetabular cup was located in the posterior and inferior position of true acetabular region for unilateral Crowe type IV DDH. SSTO led to the femoral shortening on the operated side. The sleeve or cone should be positioned close to the apex of the greater trochanter to compensate the lengh of the SSTO. The position of the sleeve or cone without SSTO should be adjusted to make sure that the height of the greater trochanter on the operated side is close to that on the contralateral side.
Acknowledgments
The authors declare that they have no competing interests. This study was funded by the National Key Research and Development Program of China (No. 2017YFB1104104).
Disclosure: All authors listed meet the authorship criteria according to the latest guidelines of the International Committee of Medical Journal Editors, and all authors are in agreement with the manuscript.
Contributor Information
Ming Ni, Email: niming301@163.com.
Yong‐gang Zhou, Email: ygzhou301@163.com.
References
- 1. Kotlarsky P, Haber R, Bialik V, Eidelman M. Developmental dysplasia of the hip: what has changed in the last 20 years?. World J Orthop, 2015, 6: 886–901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Seo LJ, Gabor J, Novikov D, Feng JE, Schwarzkopf R, Vigdorchik JM. Outcomes in 385 developmental dysplastic hips requiring total hip arthroplasty. Arch Orthop Trauma Surg, 2019, 139: 723–728. [DOI] [PubMed] [Google Scholar]
- 3. Ma HY, Zhou YG, Zheng C, et al New classification of Crowe type IV developmental dysplasia of the hip. Zhongguo Gu Shang, 2016, 29: 119–124. [PubMed] [Google Scholar]
- 4. Peng H, Zhang G, Xu C, Wang T, Wang Y. Is pseudoacetabulum an important factor determining SSTO application in total hip arthroplasty for Crowe IV hips? A retrospective cohort study. J Orthop Surg Res, 2019, 14: 201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Wang S, Zhou Y, Ma H, Du Y, Piao S, Wu W. Mid‐term results of total hip replacement with subtrochanteric osteotomy, modular stem, and ceramic surface in Crowe IV hip dysplasia. Arthroplast Today, 2018, 4: 363–369. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Montalti M, Castagnini F, Giardina F, Tassinari E, Biondi F, Toni A. Cementless total hip arthroplasty in Crowe III and IV dysplasia: high hip center and modular necks. J Arthroplasty, 2018, 33: 1813–1819. [DOI] [PubMed] [Google Scholar]
- 7. Li Y, Zhang X, Wang Q, et al Equalisation of leg lengths in total hip arthroplasty for patients with Crowe type‐IV developmental dysplasia of the hip: classification and management. Bone Joint J, 2017, 99: 872–879. [DOI] [PubMed] [Google Scholar]
- 8. Crowe JF, Mani VJ, Ranawat CS. Total hip replacement in congenital dislocation and dysplasia of the hip. J Bone Joint Surg Am, 1979, 61: 15–23. [PubMed] [Google Scholar]
- 9. Zhang Z, Luo D, Cheng H, Xiao K, Zhang H. Unexpected long lower limb in patients with unilateral Hip dislocation. J Bone Joint Surg Am, 2018, 100: 388–395. [DOI] [PubMed] [Google Scholar]
- 10. Zhou Y, Sun C, Wang Y. New method addressing the problem of using ceramic‐on‐ceramic bearing in too small acetabulum of high‐riding DDH patients with THA. Semin Arthroplasty, 2012, 23: 226–231. [Google Scholar]
- 11. Roidis NT, Pollalis AP, Hartofilakidis GC. Total hip arthroplasty in young females with congenital dislocation of the hip, radically improves their long‐term quality of life. J Arthroplasty, 2013, 28: 1206–1211. [DOI] [PubMed] [Google Scholar]
- 12. Greber EM, Pelt CE, Gililland JM, Anderson MB, Erickson JA, Peters CL. Challenges in total hip arthroplasty in the setting of developmental dysplasia of the hip. J Arthroplasty, 2017, 32: S38–S44. [DOI] [PubMed] [Google Scholar]
- 13. Boughton OR, Uemura K, Tamura K, et al Gender and disease severity determine proximal femoral morphology in developmental dysplasia of the hip. J Orthop Res, 2019, 37: 1123–1132. [DOI] [PubMed] [Google Scholar]
- 14. Rasi AM, Kazemian G, Khak M, Zarei R. Shortening subtrochanteric osteotomy and cup placement at true acetabulum in total hip arthroplasty of Crowe III‐IV developmental dysplasia: results of midterm follow‐up. Eur J Orthop Surg Traumatol, 2018, 28: 923–930. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Noble PC, Kamaric E, Sugano N, et al Three‐dimensional shape of the dysplastic femur: implications for THR. Clin Orthop Relat Res, 2003, 417: 27–40. [PubMed] [Google Scholar]
- 16. Chen G, Nie Y, Xie J, Cao G, Huang Q, Pei F. Gait analysis of leg length discrepancy—differentiated hip replacement patients with developmental dysplasia: a midterm follow‐up. J Arthroplasty, 2018, 33: 1437–1441. [DOI] [PubMed] [Google Scholar]
- 17. Kaufman KR, Miller LS, Sutherland DH. Gait asymmetry in patients with limb‐length inequality. J Pediatr Orthop, 1996, 16: 144–150. [DOI] [PubMed] [Google Scholar]
- 18. Sabharwal S, Zhao C. Assessment of lower limb alignment: supine fluoroscopy compared with a standing full‐length radiograph. J Bone Joint Surg Am, 2008, 90: 43–51. [DOI] [PubMed] [Google Scholar]
- 19. Silva M, Lee KH, Heisel C, Dela Rosa MA, Schmalzried TP. The biomechanical results of total hip resurfacing arthroplasty. J Bone Joint Surg Am, 2004, 86: 40–46. [DOI] [PubMed] [Google Scholar]
- 20. Park CW, Lim SJ, Cha YT, Park YS. Total hip arthroplasty with subtrochanteric shortening osteotomy in patients with high hip dislocation secondary to childhood septic arthritis: a matched comparative study with Crowe IV developmental dysplasia. J Arthroplasty, 2020, 35: 204–211. [DOI] [PubMed] [Google Scholar]
- 21. Wang D, Li LL, Wang HY, Pei FX, Zhou ZK. Long‐term results of cementless total hip arthroplasty with subtrochanteric shortening osteotomy in Crowe type IV developmental dysplasia. J Arthroplasty, 2017, 32: 1211–1219. [DOI] [PubMed] [Google Scholar]
- 22. Karaismailoglu B, Erdogan F, Kaynak G. High hip center reduces the dynamic hip range of motion and increases the hip load: a gait analysis study in hip arthroplasty patients with unilateral developmental dysplasia. J Arthroplasty, 2019, 34: 1267–1272.e1. [DOI] [PubMed] [Google Scholar]
- 23. Erdem Y, Bek D, Atbasi Z, Neyisci C, Yildiz C, Basbozkurt M. Total hip arthroplasty with rectangular stems and subtrochanteric transverse shortening osteotomy in Crowe type IV hips: a retrospective study. Arthroplast Today, 2019, 5: 234–242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Muratli KS, Karatosun V, Uzun B, Celik S. Subtrochanteric shortening in total hip arthroplasty: biomechanical comparison of four techniques. J Arthroplasty, 2014, 29: 836–842. [DOI] [PubMed] [Google Scholar]
- 25. Yan F, Chen G, Yang L, He R, Gu L, Wang F. A reduction technique of arthroplasty without subtrochanteric femoral shortening osteotomy for the treatment of developmental high dislocation of hip: a case series of 28 hips. J Arthroplasty, 2014, 29: 2289–2293. [DOI] [PubMed] [Google Scholar]
- 26. Lai KA, Shen WJ, Huang LW, Chen MY. Cementless total hip arthroplasty and limb‐length equalization in patients with unilateral Crowe type‐IV hip dislocation. J Bone Joint Surg Am, 2005, 87: 339–345. [DOI] [PubMed] [Google Scholar]