

Abstract
Objective
This study aimed at exploring the correlation of microRNA (miR)‐497/fibroblast growth factor‐23 (FGF‐23) axis with major adverse cardiac and cerebral event (MACCE) occurrence in end‐stage renal disease (ESRD) patients who underwent continuous ambulatory peritoneal dialysis (CAPD).
Methods
Totally, 360 ESRD patients who underwent CAPD were enrolled. Their plasma samples were collected to detect miR‐497 expression by real‐time quantitative polymerase chain reaction, and FGF‐23 level by enzyme‐linked immunosorbent assay. All patients were followed up for 36 months, and the occurrence of MACCE during the follow‐up was documented.
Results
MiR‐497 expression negatively correlated with FGF‐23 level in ESRD patients who underwent CAPD (P < .001). The MACCE occurrence rate at 1, 2, and 3‐year was 5.6%, 11.9%, and 15.0%, respectively. Furthermore, miR‐497/FGF‐23 axis high level (P < .001) and miR‐497 high expression (P = .034) correlated with reduced accumulating MACCE occurrence, whereas FGF‐23 high level (P = .008) correlated with increased accumulating MACCE occurrence. Forward stepwise multivariate Cox's regression disclosed that miR‐497/FGF‐23 axis high level (P = .008) was an independent predictive factor for lower accumulating MACCE occurrence, whereas age (≥55 years) (P < .001), body mass index (≥21.7 kg/m2) (P = .006), peritoneal dialysis duration (≥61.0 months) (P < .001), C‐reactive protein (≥4.7 mg/L) (P = .001), serum uric acid (≥409.4 μmol/L) (P = .009), β‐fibrinogen (≥5.8 mmol/L) (P < .001), and low‐density lipoprotein cholesterol (≥2.7 mmol/L) (P = .003) were independent factors for predicting higher accumulating MACCE occurrence.
Conclusion
MiR‐497/FGF‐23 axis holds clinical significance for predicting attenuated MACCE risk in ESRD patients who underwent CAPD.
Keywords: continuous ambulatory peritoneal dialysis, end‐stage renal disease, fibroblast growth factor‐23, major adverse cardiac and cerebral event, microRNA‐497
1. INTRODUCTION
End‐stage renal disease (ESRD), a growing global health burden, is characterized by advanced irreversible dysfunction of the glomerular filter apparatus that ultimately leads to the kidney failure.1 It is estimated to affect over 2 million individuals worldwide with high mortality and hospitalization rate.2, 3 Dialysis remains as the mainstay treatment of prolonging life of ESRD patients since renal transplantation is limited by organ shortage and financial constrains.4 Continuous ambulatory peritoneal dialysis (CAPD), as a convenient mode of dialysis, is performed to exchange electrolytes, glucose, urea, albumin, and other small molecules from the blood.5, 6 However, major adverse cardiac and cerebral event (MACCE) is a frequent and severe complication in ESRD patients underwent CAPD, which profoundly damages patients’ quality of life, elevates the healthcare costs and even sudden‐death rate in ESRD patients.7 Currently, in clinical practice, there is still a lack of efficient disease monitoring and predictive biomarkers for MACCE. Therefore, the identification of plasma biomarkers for assessing MACCE risk and improving prognosis is an important goal in ESRD patients who underwent CAPD.
In our previous study, fibroblast growth factor‐23 (FGF‐23), an endocrine hormone, is illuminated to correlate with poor renal function and higher MACCE occurrence as well as have the potential for predicting shorter MACCE‐free survival in ESRD patients who underwent CAPD.8 Meanwhile, FGF‐23 was found to be a potential target of microRNA (miR)‐497 (derived by prediction using miRanda database [www.microrna.org]). As for miR‐497, a highly conserved microRNA is reported to regulate cardiosphere‐derived cells (CDCs) differentiation, alleviate myocardial ischemia‐reperfusion (I/R) injury, and suppress myocardial hypertrophy in various cardiovascular diseases.9, 10, 11 Furthermore, miR‐497 is also involved in the development and progression of cerebrovascular disease.12, 13 Additionally, our preliminary study with small sample size revealed that miR‐497 was negatively correlated with FGF‐23, and it could predict MACCE occurrence in ESRD patients who underwent CAPD to some extent.
Combining the evidences from these aforementioned studies, we speculated that miR‐497 might predict MACCE occurrence via interacting with FGF‐23. Therefore, this study aimed at exploring the correlation of miR‐497/FGF‐23 axis with MACCE occurrence in ESRD patients who underwent CAPD.
2. MATERIALS AND METHODS
2.1. Patients
From July 2011 to June 2016, 360 ESRD patients who underwent CAPD in our hospital were consecutively recruited in this study. The inclusion and exclusion criteria referred to our previous study.8 In brief, the inclusion criteria were as follows: (a) diagnosed as ESRD; (b) underwent CAPD for at least 3 years; (c) age > 18 years old; (d) no history of kidney transplantation or kidney surgery; and (e) without solid tumors or hematological malignancies. The exclusion criteria included: (a) history of hemodialysis; (b) history of cardiovascular and cerebrovascular diseases (such as coronary artery disease, myocardial infarction, stroke, thromboangiitis obliterans, arteriosclerosis, and obliterans); (c) history of major cardiovascular surgery (percutaneous coronary intervention or coronary artery bypass grafting); (d) primary diabetes mellitus (DM) nephropathy, primary hypertensive nephropathy or complicated with DM or hypertension; and (e) unable to follow up regularly.
2.2. Ethics
The approval of this study was acquired from the Institutional Review Board of our hospital, and all procedures were carried out in compliance with the provisions of the Declaration of Helsinki. Written informed consents were obtained from all patients before enrollment.
2.3. Data and sample collection
After enrollment, the clinical features were collected, which included demographic data, peritoneal dialysis duration, biochemical indexes and blood pressure. Besides, the adequacy of dialysis (Kt/V) was also recorded, which was calculated as clearance (K) multiplied by treatment time (t) and divided by the urea distribution volume (V). Peripheral blood samples of patients were collected after the informed consents were provided. And plasma was isolated from blood samples by centrifuging at 215 g for 15 minutes under 4°C, then the plasma was stored at −80°C until further measurement.
2.4. FGF‐23 and miR‐497 detections
The level of FGF‐23 in plasma was measured using the Human C‐terminal FGF‐23 enzyme‐linked immunosorbent assay (ELISA) kit (Immutopics), and the procedure was consistent with the study we published previously.7 The level of miR‐497 in plasma was detected by reverse transcription quantitative polymerase chain reaction (RT‐qPCR). Total RNA from plasma was isolated using QIAamp RNA Blood Mini Kit (Qiagen), then the extracted RNA was reversely transcribed to complementary DNA with the use of ReverTra Ace® qPCR RT Master Mix (Toyobo). Subsequently, complementary DNA was subjected to PCR amplification with KOD SYBR® qPCR Mix (Toyobo). The relative expression of miR‐497 was computed by 2−ΔΔ C t method, and U6 was used as an internal reference. The primer sequences applied for miR‐497 and U6 were as follows: miR‐497, forward: 5′ ACACTCCAGCTGGGCAGCAGCACACTGTGG 3′; reverse: 5′ TGTCGTGGAGTCGGCAATTC 3′; U6, forward: 5′ CTCGCTTCGGCAGCACATATACTA 3′, reverse: 5′ ACGAATTTGCGTGTCATCCTTGC 3′.
2.5. Follow‐up
Regular follow‐up was conducted by telephone or clinical visit every 1‐3 months. All patients were followed up to MACCE occurrence or 36 months after enrollment. The method for MACCE detection and the MACCE definition referred to our previous study.8 Briefly, MACCE was defined as the event of death or hospitalization caused by cardiovascular disease or cerebrovascular disease, acute coronary syndrome, stable angina pectoris requiring target vessel revascularization (TVR), transient ischemic attack (TIA), and ischemic stroke. During follow‐up, the occurrence of MACCE was recorded. For patients who lost follow‐up, the majority of them admitted to other hospitals for clinical visit. Hence, we did not have the complete follow‐up information for MACCE in these patients. And it would not be objective if they were censored on the date of last follow‐up. Therefore, they were excluded from the final analysis. Regarding patients who withdrew the informed consents, we did not have the right to use their data. Therefore, they were excluded from the final analysis.
2.6. Statistical analysis
Correlation between miR‐497 and FGF‐23 was analyzed by Spearman's rank correlation test. For accumulating MACCE occurrence analysis, patients were divided into high group and low group according to the median value of variables (such as miR‐497 high group and low group, FGF‐23 high group and low group, or miR‐497/FGF‐23 axis high group and low group). Accumulating MACCE occurrence was illustrated using Kaplan‐Meier estimates, and difference of accumulating MACCE occurrence between two groups was determined by log‐rank test. Factors affecting MACCE risk were modeled using univariate and forward stepwise Cox's multivariate proportional hazard regression. Factors affecting MACCE risk were divided into two‐category data in the Cox's multivariate proportional hazard regression based on their median value to increase statistic power and make them more clinically significant. Statistical analyses were performed using SPSS software (IBM) version 22.0, and figures were made using GraphPad Prism software (GraphPad Software) version 7.00. P value < 0.05 was considered significant.
3. RESULTS
3.1. Study flow
Initially, a total of 756 patients were invited, in which 189 patients were excluded since they declined to attend pre‐screening procedure (Figure 1). Subsequently, 567 patients were screened, while 153 patients were excluded (130 patients did not meet inclusion criteria or met exclusion criteria, 23 patients declined the informed consents). Then, among 414 eligible patients, a total of 54 patients withdrew during the follow‐up (43 patients lost follow‐up, 11 patients withdrew informed consents). Eventually, 360 patients who completed 36‐month follow‐up were included in the final analysis.
Figure 1.
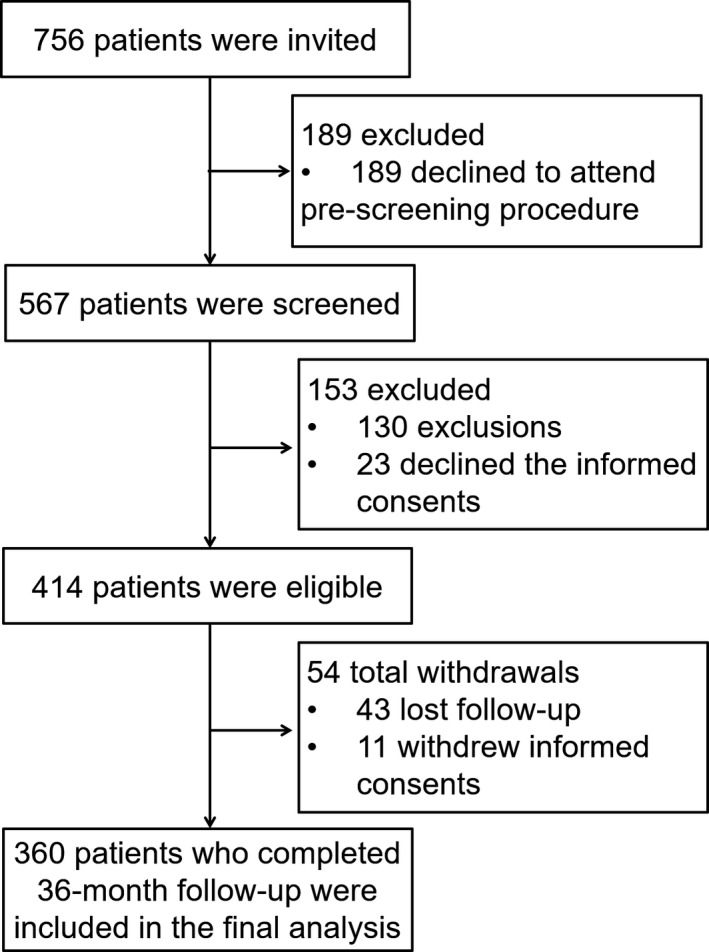
Study flow
3.2. Clinical features
In ESRD patients who underwent CAPD, the mean age was 55.2 ± 11.5 years, and there were 119 (33.1%) females as well as 241 (66.9%) males. The mean BMI was 21.8 ± 2.6 kg/m2. Besides, the number of patients with current smoking and drinking was 70 (19.4%) and 61 (16.9%), respectively. Additionally, at enrollment, the median peritoneal dialysis duration and the median Kt/V was 60.5 months (IQR: 48.0‐78.0 months) and 1.8 (IQR: 1.6‐2.1), respectively. Detailed characteristics of biochemical indexes were exhibited in Table 1.
Table 1.
Clinical characteristics of CAPD patients
| Items | CAPD patients (N = 360) |
|---|---|
| Age (years), mean ± SD | 55.2 ± 11.5 |
| Gender, No. (%) | |
| Female | 119 (33.1) |
| Male | 241 (66.9) |
| BMI (kg/m2), mean ± SD | 21.8 ± 2.6 |
| Smoke, No. (%) | 70 (19.4) |
| Drink, No. (%) | 61 (16.9) |
| Peritoneal dialysis duration (months), median (IQR) | 60.5 (48.0‐78.0) |
| Kt/V, median (IQR) | 1.8 (1.6‐2.1) |
| HB (g/L), mean ± SD | 103.5 ± 15.0 |
| WBC (×109/L), mean ± SD | 7.9 ± 2.2 |
| PLT (×109/L), mean ± SD | 209.5 ± 56.2 |
| CRP (mg/L), median (IQR) | 4.7 (2.9‐7.6) |
| Scr (μmol/L), median (IQR) | 922.6 (768.4‐1108.3) |
| SUA (μmol/L), mean ± SD | 415.9 ± 75.2 |
| Ca (mmol/L), median (IQR) | 2.2 (2.0‐2.4) |
| Phosphorus (mmol/L), mean ± SD | 1.7 ± 0.4 |
| FBG (mmol/L), median (IQR) | 5.8 (4.5‐7.2) |
| ALB (g/L), mean ± SD | 38.9 ± 6.2 |
| SBP (mm Hg), median (IQR) | 137.0 (126.0‐151.8) |
| DBP (mm Hg), mean ± SD | 83.2 ± 9.0 |
| TG (mmol/L), median (IQR) | 1.7 (1.0‐2.4) |
| TC (mmol/L), median (IQR) | 4.6 (3.9‐5.4) |
| LDL‐C (mmol/L), mean ± SD | 2.8 ± 0.6 |
| HDL‐C (mmol/L), median (IQR) | 1.0 (0.9‐1.2) |
Abbreviations: ALB, albumin; BMI, body mass index; Ca, calcium; CAPD, continuous ambulatory peritoneal dialysis; CRP, C‐reactive protein; DBP, diastolic blood pressure; FBG, β‐fibrinogen; HB, hemoglobin; HDL‐C, high‐density lipoprotein cholesterol; IQR, interquartile range; LDL‐C, low‐density lipoprotein cholesterol; PLT, platelet; SBP, systolic pressure; Scr, serum creatinine; SD, standard deviation; SUA, serum uric acid; TC, total cholesterol; TG, triglyceride; WBC, white blood cell.
3.3. MiR‐497, FGF‐23 and miR‐497/FGF‐23 axis
In ESRD patients who underwent CAPD, the median miR‐497 relative expression was 1.000 (IQR: 0.551‐1.965; Range: 0.033‐8.481) (Figure 2A), and the median FGF‐23 level was 685.565 pg/mL (IQR: 526.513‐820.923 pg/mL; Range: 230.780‐1555.760 pg/mL) (Figure 2B). Furthermore, the median miR‐497/FGF‐23 axis level was 0.001 (IQR: 0.001‐0.003; Range: 0.000‐0.026) (Figure 2C). Additionally, miR‐497 relative expression was negatively correlated with FGF‐23 level in the analyzed patients (P < .001) (r = −.363) (Figure 2D).
Figure 2.
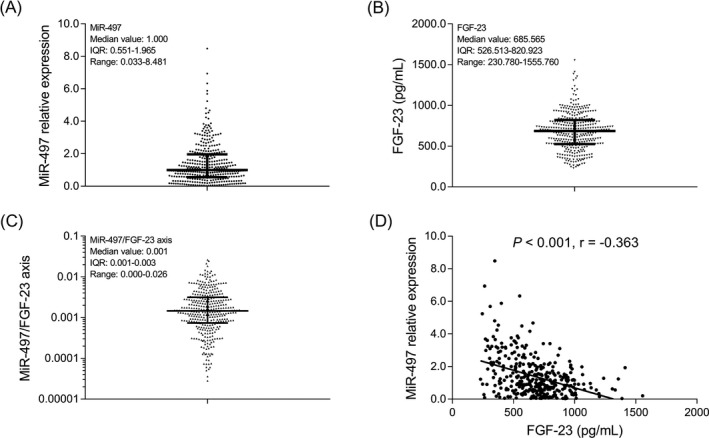
MiR‐497, FGF‐23, and miR‐497/FGF‐23 axis relative expressions. The miR‐497 relative expression (A), FGF‐23 (B), miR‐497/FGF‐23 axis (C), and association of miR‐497 relative expression with FGF‐23 in ESRD patients who underwent CAPD (D). MiR, micro RNA; FGF‐23, fibroblast growth factor‐23; ESRD, end‐stage renal disease; CAPD, continuous ambulatory peritoneal dialysis
3.4. MACCE occurrence
Kaplan‐Meier curve revealed that the mean duration for occurring MACCE was 33.1 months (95% CI: 32.3‐33.9 months) in ESRD patients who underwent CAPD (Figure 3A). The MACCE occurrence at 1, 2, and 3 year was 20 (5.6%), 43 (11.9%), and 54 (15.0%), respectively (Figure 3B).
Figure 3.
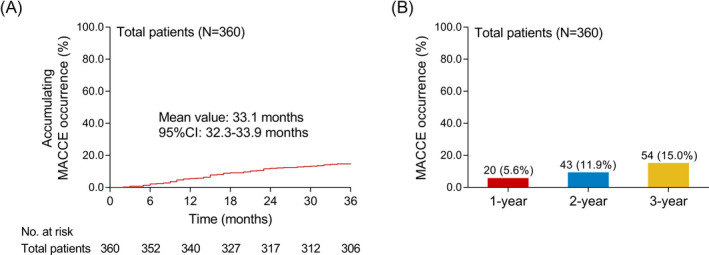
Kaplan‐Meier curve and MACCE occurrence. Accumulating MACCE occurrence (A), MACCE occurrence rate at 1, 2, and 3‐year (B) in ESRD patients who underwent CAPD. MACCE, major adverse cardiac and cerebral event; ESRD, end‐stage renal disease; CAPD, continuous ambulatory peritoneal dialysis
3.5. Correlation of miR‐497, FGF‐23, and miR‐497/FGF‐23 axis with accumulating MACCE occurrence
MiR‐497 high expression (χ 2 = 4.487) (P = .034) was correlated with reduced accumulating MACCE occurrence (Figure 4A), whereas FGF‐23 high level (χ 2 = 7.155) (P = .008) was correlated with elevated accumulating MACCE occurrence in ESRD patients who underwent CAPD (Figure 4B). As for miR‐497/FGF‐23 axis high level (χ 2 = 12.450) (P < .001), it was correlated with lower accumulating MACCE occurrence (Figure 4C). Of note, miR‐497/FGF‐23 axis had increased statistic value and decreased P value compared with miR‐497 or FGF‐23 alone numerically, which indicated that miR‐497/FGF‐23 axis might better predict the accumulating MACCE occurrence in ESRD patients who underwent CAPD to some extent. Besides, 1‐year MACCE was not obviously differed, and 2‐year MACCE was intermediately differentiated between miR‐497/FGF‐23 axis high and low level. The difference was enlarged for 2‐year MACCE, which indicated that miR‐497/FGF‐23 axis was valuable for predicting long‐term MACCE risk.
Figure 4.
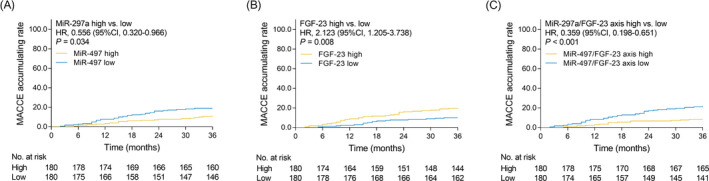
The difference of accumulating MACCE occurrence between miR‐497 high vs low, FGF‐23 high vs low, miR‐497/FGF‐23 high vs low ESRD patients. Comparison of accumulating MACCE occurrence between miR‐497 high expression vs miR‐497 low expression (A), FGF‐23 high level vs FGF‐23 low level (B), miR‐497/FGF‐23 axis high level vs miR‐497/FGF‐23 axis low level (C) ESRD patients who underwent CAPD. MACCE, major adverse cardiac and cerebral event; miR, micro RNA; FGF‐23, fibroblast growth factor‐23; ESRD, end‐stage renal disease; CAPD, continuous ambulatory peritoneal dialysis
3.6. Factors predicting accumulating MACCE occurrence by univariate Cox's regression model
Univariate Cox's regression model analysis disclosed that miR‐497 high expression (HR: 0.556, 95% CI: 0.320‐0.966, P = .037) and miR‐497/FGF‐23 axis high level (HR: 0.359, 95% CI: 0.198‐0.651, P = .001) were correlated with decreased accumulating MACCE occurrence in ESRD patients who underwent CAPD (Table 2). Whereas, FGF‐23 high level (HR: 2.123, 95% CI: 1.205‐3.738, P = .009), age (≥55 years) (HR: 1.973, 95% CI: 1.129‐3.449, P = .017), BMI (≥21.7 kg/m2) (HR: 1.829, 95% CI: 1.052‐3.177, P = .032), peritoneal dialysis duration (≥61 months) (HR: 2.793, 95% CI: 1.540‐5.067, P = .001), CRP (≥4.7 mg/L) (HR: 2.577, 95% CI: 1.437‐4.621, P = .001), SUA (≥409.4 μmol/L) (HR: 1.797, 95% CI: 1.034‐3.121, P = .038), FBG (≥5.8 mmol/L) (HR: 1.992, 95% CI: 1.140‐3.483, P = .016), TC (≥4.6 mmol/L) (HR: 1.776, 95% CI: 1.022‐3.085, P = .042), and LDL‐C (≥2.7 mmol/L) (HR: 1.952, 95% CI: 1.116‐3.412, P = .019) were correlated with increased accumulating MACCE occurrence in ESRD patients who underwent CAPD (Table 2). No correlation of other factors with accumulating MACCE occurrence was observed in ESRD patients who underwent CAPD (Table 2).
Table 2.
Univariate Cox's regression model analysis of factors predicting accumulating MACCE occurrence
| Items | Univariate Cox's proportional hazard regression | |||
|---|---|---|---|---|
| P value | HR | 95% CI | ||
| Low | High | |||
| MiR‐497 high | .037 | 0.556 | 0.320 | 0.966 |
| FGF‐23 high | .009 | 2.123 | 1.205 | 3.738 |
| MiR‐497/FGF‐23 axis high | .001 | 0.359 | 0.198 | 0.651 |
| Age (≥55 y) | .017 | 1.973 | 1.129 | 3.449 |
| Gender (male) | .713 | 0.901 | 0.515 | 1.574 |
| BMI (≥21.7 kg/m2) | .032 | 1.829 | 1.052 | 3.177 |
| Smoke (yes) | .846 | 1.068 | 0.551 | 2.070 |
| Drink (yes) | .431 | 1.305 | 0.673 | 2.530 |
| Peritoneal dialysis duration (≥61 mo) | .001 | 2.793 | 1.540 | 5.067 |
| Kt/V (≥1.8) | .790 | 0.930 | 0.545 | 1.586 |
| HB (≥103.6 g/L) | .161 | 1.475 | 0.857 | 2.538 |
| WBC (≥7.9 × 109/L) | .797 | 1.073 | 0.629 | 1.829 |
| PLT (≥212.0 × 109/L) | .521 | 0.839 | 0.492 | 1.433 |
| CRP (≥4.7mg/L) | .001 | 2.577 | 1.437 | 4.621 |
| Scr (≥922.8 μmol/L) | .775 | 1.081 | 0.634 | 1.844 |
| SUA (≥409.4 μmol/L) | .038 | 1.797 | 1.034 | 3.121 |
| Ca (≥2.2 mmol/L) | .342 | 1.297 | 0.758 | 2.219 |
| Phosphorus (≥1.6 mmol/L) | .749 | 1.091 | 0.640 | 1.861 |
| FBG (≥5.8 mmol/L) | .016 | 1.992 | 1.140 | 3.483 |
| ALB (≥38.8 g/L) | .143 | 0.667 | 0.387 | 1.147 |
| SBP (≥137.0 mm Hg) | .080 | 1.631 | 0.944 | 2.819 |
| DBP (≥83.0 mm Hg) | .537 | 0.845 | 0.495 | 1.442 |
| TG (≥1.7 mmol/L) | .364 | 1.282 | 0.750 | 2.193 |
| TC (≥4.6 mmol/L) | .042 | 1.776 | 1.022 | 3.085 |
| LDL‐C (≥2.7 mmol/L) | .019 | 1.952 | 1.116 | 3.412 |
| HDL‐C (≥1.0 mmol/L) | .773 | 0.924 | 0.542 | 1.577 |
Abbreviations: ALB, albumin; BMI, body mass index; Ca, calcium; CI, confidence interval; CRP, C‐reactive protein; DBP, diastolic blood pressure; FBG, β‐fibrinogen; FGF‐23, fibroblast growth factor‐23; HB, hemoglobin; HDL‐C, high‐density lipoprotein cholesterol; HR, hazard ratio; LDL‐C, low‐density lipoprotein cholesterol; MACCE, major adverse cardiovascular and cerebrovascular events; miR, microRNA; PLT, platelet; SBP, systolic pressure; Scr, serum creatinine; SUA, serum uric acid; TC, total cholesterol; TG, triglyceride; WBC, white blood cell.
3.7. Factors predicting accumulating MACCE occurrence by forward stepwise multivariate Cox's regression model
Forward stepwise multivariate Cox's regression model analysis showed that miR‐497/FGF‐23 axis high level (HR: 0.445, 95% CI: 0.244‐0.812, P = .008) was an independent predictive factor for lower accumulating MACCE occurrence, whereas age (≥55 years) (HR: 3.153, 95% CI: 1.747‐5.692, P < .001), BMI (≥21.7 kg/m2) (HR: 2.235, 95% CI: 1.256‐3.977, P = .006), peritoneal dialysis duration (≥61.0 months) (HR: 4.652, 95% CI: 2.499‐8.658, P < .001), CRP (≥4.7 mg/L) (HR: 2.791, 95% CI: 1.544‐5.044, P = .001), SUA (≥409.4 μmol/L) (HR: 2.174, 95% CI: 1.217‐3.885, P = .009), FBG (≥5.8 mmol/L) (HR: 3.315, 95% CI: 1.809‐6.074, P < .001). and LDL‐C (≥2.7 mmol/L) (HR: 2.449, 95% CI: 1.361‐4.407, P = .003) were independent predictive factors for higher accumulating MACCE occurrence in ESRD patients who underwent CAPD (Table 3).
Table 3.
Forward stepwise multivariate Cox's regression model analysis of factors predicting accumulating MACCE occurrence
| Items | Forward stepwise Cox's multivariate regression | |||
|---|---|---|---|---|
| P value | HR | 95% CI | ||
| Low | High | |||
| MiR‐497/FGF‐23 axis high | .008 | 0.445 | 0.244 | 0.812 |
| Age (≥55 y) | <.001 | 3.153 | 1.747 | 5.692 |
| BMI (≥21.7 kg/m2) | .006 | 2.235 | 1.256 | 3.977 |
| Peritoneal dialysis duration (≥61.0 mo) | <.001 | 4.652 | 2.499 | 8.658 |
| CRP (≥4.7 mg/L) | .001 | 2.791 | 1.544 | 5.044 |
| SUA (≥409.4 μmol/L) | .009 | 2.174 | 1.217 | 3.885 |
| FBG (≥5.8 mmol/L) | <.001 | 3.315 | 1.809 | 6.074 |
| LDL‐C (≥2.7 mmol/L) | .003 | 2.449 | 1.361 | 4.407 |
Abbreviations: BMI, body mass index; CI, confidence interval; CRP, C‐reactive protein; FBG, β‐fibrinogen; FGF‐23, fibroblast growth factor‐23; HR, hazard ratio; LDL‐C, low‐density lipoprotein cholesterol; MACCE, major adverse cardiovascular and cerebrovascular events; miR, microRNA; SUA, serum uric acid.
4. DISCUSSION
Continuous ambulatory peritoneal dialysis is a common and effective replacement therapy that assists renal function and improves quality of life in ESRD patients.5 MACCE, a frequent complication in ESRD patients who underwent CAPD, is caused by the thrombosis that is attributed by the disturbance of equilibrium between pro‐coagulation and anticoagulation activities.14 It remains as a major obstacle for improving prognosis in these patients.15 Therefore, the present study was performed to investigate plasma biomarkers for predicting MACCE risk and assisting MACCE management in ESRD patients who underwent CAPD.
From our previous study, FGF‐23 correlates with longer duration of dialysis, higher calcium, phosphorus, and LDL‐C levels as well as predicts reduced accumulating MACCE‐free survival in ESRD patients who underwent CAPD.8 Besides, it was predicted that FGF‐23 was the target gene of miR‐497 (obtained from miRanda database [www.microrna.org]). MiR‐497 expression can be found in almost all human organs and tissues (eg, heart and brain), which is implied in various cardiac pathogenesis.9, 10, 11 For instance, in a previous cellular experiment, miR‐497 regulates CDCs differentiation via targeting transforming growth factor beta signaling pathway.9 And in a mouse model of I/R injury, miR‐497 facilitates proliferation and suppresses apoptosis of cardiomyocytes via attenuating mitofusin 2 (Mfn2) expression.10 In cardiac hypertrophy models, overexpression of miR‐497 alleviates myocardial hypertrophy via targeting sirtuin 4 (Sirt4).11 Moreover, miR‐497 is found to trigger ischemic neuronal death via suppressing anti‐apoptotic gene (bcI‐2 and bcl‐w) expression, which is implied in the pathogenesis of cerebral ischemia.13 From a clinical study, miR‐497 also exhibits the potency to be a prognostic biomarker in acute cerebral infarction patients. Known that FGF‐23 is a predictive indictor for MACCE‐free survival and the target gene of miR‐497 and that miR‐497 plays a role in the pathogenesis of cardiovascular and cerebrovascular events, we speculated that miR‐497 might be correlated with the risk of MACCE via interacting with FGF‐23 in ESRD patients who underwent CAPD.
In the present study, 360 ESRD patients who underwent CAPD were recruited, and we observed that miR‐497 relative expression was negatively correlated with FGF‐23. Furthermore, the present study exhibited that miR‐497 high expression and miR‐497/FGF‐23 axis high level were both associated with attenuated accumulating MACCE occurrence, whereas FGF‐23 high level was associated with elevated accumulating MACCE occurrence in ESRD patients who underwent CAPD. Notably, miR‐497/FGF‐23 axis presented with numerically better value in predicting accumulating MACCE occurrence to some extent compared with miR‐497 or FGF‐23 alone. Besides, miR‐497/FGF‐23 axis high expression was an independent predictive factor for reduced accumulating MACCE occurrence. Herein, several explanations were proposed: (a) FGF‐23 might activate the local renin‐angiotensin‐aldosterone system to stimulate the cardiac hypertrophy and fibrosis in the heart; thereby, its high expression correlated with increased accumulating MACCE occurrence in ESRD patients who underwent CAPD.16 (b) MiR‐497 might inhibit several genes (such as Mfn2 and Sirt4) to enhance proliferation while inhibit apoptosis of cardiomyocytes and dampen inflammatory responses in cardio‐cerebral‐vascular system; thereby, its high expression correlated with lower accumulating MACCE occurrence in ESRD patients who underwent CAPD.9, 10, 11 (c) MiR‐497 might decrease FGF‐23 level in cardiovascular system, which subsequently reduced the effect of FGF‐23 on facilitating the heart tissue injury, thus, the high miR‐497/FGF‐23 axis level was associated with attenuated MACCE occurrence in ESRD patients.16, 17 Interestedly, miR‐497/FGF‐23 axis was valuable for predicting long‐term MACCE risk, which implied that the potential of miR‐497/FGF‐23 axis as a biomarker for assisting with long‐term MACCE management and prognosis improvement in ESRD patients who underwent CAPD in clinical practice.
Additionally, the present study showed that age (≥55 years), BMI (≥21.7 kg/m2), peritoneal dialysis duration (≥61.0 months), CRP (≥4.7 mg/L), SUA (≥409.4 μmol/L), FBG (≥5.8 mmol/L), and LDL‐C (≥2.7 mmol/L) were independent predictive factors for increased accumulating MACCE occurrence in ESRD patients who underwent CAPD. The possible reasons were as follows: (a) Older patients tended to have multiple comorbidities such as diabetes and hypertension, thus, increasing the risk of MACCE in ESRD patients who underwent CAPD. (b) Higher BMI was associated with increased diabetes prevalence, elevated total cholesterol, triglyceride, and CRP levels, which was responsible for MACCE occurrence.18 (c) Patients with longer peritoneal dialysis duration (≥61.0 months) might have a poor renal function, which could cause weaker cellular take up and upregulate calcium as well phosphorous levels, thus, inducing vascular calcification and higher MACCE occurrence. (d) Patients who had higher CRP level exhibited amplified inflammatory responses, which might induce carotid atherosclerosis and cardiac valve calcification; thereby, accelerating the occurrence of cardiovascular and cerebrovascular events.19 (e) Elevated SUA level, FBG, and LDL‐C might be associated with the development/progression of vascular disorders such as atherosclerosis, which contributed to higher cardiovascular and cerebrovascular risk in ESRD patient who underwent CAPD.20, 21
Several limitations should be taken into consideration in the present study. Firstly, patients were recruited from a single center, which might cause selection bias and limit the generalizability of the findings. Secondly, the follow‐up period (36 months) was relatively short; thereby, the predictive values of miR‐497 and FGF‐23 for long‐term MACCE occurrence were not explored in ESRD patients who underwent CAPD. Thirdly, only ESRD patients who underwent CAPD for at least 3 years were included, which might cause selection bias and lack a wide representation. Although it was not the aim of our study, it would be a clinical significance to explore the correlation of miR‐497/FGF‐23 axis with MACCE occurrence in ESRD patients who underwent CAPD for <3 years in the future. Lastly, the detailed molecular mechanism of miR‐497 and FGF‐23 in the development and progression of MACCE was not investigated.
In conclusion, miR‐497/FGF‐23 axis holds clinical significance as a biomarker for predicting MACCE risk, which might offer insights for the identification and management of MACCE in ESRD patients who underwent CAPD.
CONFLICT OF INTEREST
The authors declare that they have no conflict of interests.
ACKNOWLEDGMENTS
None.
Liu D, Zhou S, Mao H. MicroRNA‐497/fibroblast growth factor‐23 axis, a predictive indictor for decreased major adverse cardiac and cerebral event risk in end‐stage renal disease patients who underwent continuous ambulatory peritoneal dialysis. J Clin Lab Anal. 2020;34:e23220 10.1002/jcla.23220
Dianjun Liu and Silian Zhou contributed equally to this work.
REFERENCES
- 1. Hakeem A, Bhatti S, Chang SM. Screening and risk stratification of coronary artery disease in end‐stage renal disease. JACC Cardiovasc Imaging. 2014;7(7):715‐728. [DOI] [PubMed] [Google Scholar]
- 2. Robinson BM, Akizawa T, Jager KJ, et al. Factors affecting outcomes in patients reaching end‐stage kidney disease worldwide: differences in access to renal replacement therapy, modality use, and haemodialysis practices. Lancet. 2016;388(10041):294‐306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Mathew AT, Strippoli GF, Ruospo M, et al. Reducing hospital readmissions in patients with end‐stage kidney disease. Kidney Int. 2015;88(6):1250‐1260. [DOI] [PubMed] [Google Scholar]
- 4. Li H, Xie L, Yang J, et al. Symptom burden amongst patients suffering from end‐stage renal disease and receiving dialysis: A literature review. Int J Nurs Sci. 2018;5(4):427‐431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Su X, Zhang K, Guo F, et al. Ischemia‐modified albumin, a predictive marker of major adverse cardiovascular events in continuous ambulatory peritoneal dialysis patients. Clin Biochem. 2013;46(15):1410‐1413. [DOI] [PubMed] [Google Scholar]
- 6. Goldstein M, Carrillo M, Ghai S. Continuous ambulatory peritoneal dialysis‐a guide to imaging appearances and complications. Insights Imaging. 2013;4(1):85‐92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Morton RL, Snelling P, Webster AC, et al. Factors influencing patient choice of dialysis versus conservative care to treat end‐stage kidney disease. CMAJ. 2012;184(5):E277‐E283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Xu L, Hu X, Chen W. Fibroblast growth factor‐23 correlates with advanced disease conditions and predicts high risk of major adverse cardiac and cerebral events in end‐stage renal disease patients undergoing continuous ambulatory peritoneal dialysis. J Nephrol. 2019;32(2):307‐314. [DOI] [PubMed] [Google Scholar]
- 9. Jafarzadeh M, Mohammad Soltani B, Ekhteraei Tousi S, et al. Hsa‐miR‐497 as a new regulator in TGFbeta signaling pathway and cardiac differentiation process. Gene. 2018;675:150‐156. [DOI] [PubMed] [Google Scholar]
- 10. Qin L, Yang W, Wang YX, et al. MicroRNA‐497 promotes proliferation and inhibits apoptosis of cardiomyocytes through the downregulation of Mfn2 in a mouse model of myocardial ischemia‐reperfusion injury. Biomed Pharmacother. 2018;105:103‐114. [DOI] [PubMed] [Google Scholar]
- 11. Xiao Y, Zhang X, Fan S, et al. MicroRNA‐497 inhibits cardiac hypertrophy by targeting Sirt4. PLoS ONE. 2016;11(12):e0168078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Wang J, Lin M, Ren H, et al. Expression and clinical significance of serum miR‐497 in Patients with acute cerebral infarction. Clin Lab. 2019;65(4). [DOI] [PubMed] [Google Scholar]
- 13. Yin KJ, Deng Z, Huang H, et al. miR‐497 regulates neuronal death in mouse brain after transient focal cerebral ischemia. Neurobiol Dis. 2010;38(1):17‐26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Liu YL, Saraf A, Catanese B, et al. Obesity and survival in the neoadjuvant breast cancer setting: role of tumor subtype in an ethnically diverse population. Breast Cancer Res Treat. 2018;167(1):277‐288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Kim H, Kim KH, Ahn SV, et al. Risk of major cardiovascular events among incident dialysis patients: A Korean national population‐based study. Int J Cardiol. 2015;198:95‐101. [DOI] [PubMed] [Google Scholar]
- 16. Bockmann I, Lischka J, Richter B, et al. FGF23‐Mediated Activation of Local RAAS Promotes Cardiac Hypertrophy and Fibrosis. Int J Mol Sci. 2019;20(18):4634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Komaba H, Fukagawa M. The role of FGF23 in CKD–with or without Klotho. Nat Rev Nephrol. 2012;8(8):484‐490. [DOI] [PubMed] [Google Scholar]
- 18. Xiong L, Cao S, Xu F, et al. Association of body mass index and body mass index change with mortality in incident peritoneal dialysis patients. Nutrients. 2015;7(10):8444‐8455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Ducloux D, Bresson‐Vautrin C, Kribs M, et al. C‐reactive protein and cardiovascular disease in peritoneal dialysis patients. Kidney Int. 2002;62(4):1417‐1422. [DOI] [PubMed] [Google Scholar]
- 20. Khosla UM, Zharikov S, Finch JL, et al. Hyperuricemia induces endothelial dysfunction. Kidney Int. 2005;67(5):1739‐1742. [DOI] [PubMed] [Google Scholar]
- 21. Tomura S, Nakamura Y, Doi M, et al. Fibrinogen, coagulation factor VII, tissue plasminogen activator, plasminogen activator inhibitor‐1, and lipid as cardiovascular risk factors in chronic hemodialysis and continuous ambulatory peritoneal dialysis patients. Am J Kidney Dis. 1996;27(6):848‐854. [DOI] [PubMed] [Google Scholar]