

Abstract
Single atrium (SA) is one of the rare congenital anomalies in which there is a complete absence of the atrial septum without an endocardial cushion defect associated with the absence of malformation of the atrioventricular (AV) valves. The term “common atrium” is used to denote the condition where there is a complete absence of the atrial septum or it is represented by a small strand of tissue present at the superior atrial wall of the common chamber, absence of interventricular communication, and accompanying AV cushion defect. Our patient demonstrated typical echocardiographic features of three-chambered heart (SA), which is a rare entity.
Keywords: Atrial septal defect, common atrium, congenital heart disease, single atrium, two-dimensional echocardiography
INTRODUCTION
Single atrium (SA) is one of the rare congenital anomalies in which there is a complete absence of the atrial septum without an endocardial cushion defect associated with the absence of malformation of the atrioventricular (AV) valves. This case report is useful in differentiating it from the common atrium (CA), in which there is a complete absence of the atrial septum or it is represented by a small strand of tissue present at the superior atrial wall of the common chamber, absence of interventricular communication, and accompanying AV cushion defect.
CASE REPORT
A 25-year-old female presented with complaints of shortness of breath, giddiness, and generalized weakness. She had a history of recurrent abortions at the gestational age of 2–3 months twice. Currently, she was 4 months gravida and was sent to us for two-dimensional (2D) echocardiography by her treating gynecologist.
On examination, her blood pressure was 100/70 mmHg; pulse rate was 94/min; and oxygen saturation by pulse oxymeter was 88%. There was no evidence of cyanosis or clubbing. On cardiovascular examination, apex beat was present in the left 5th intercostal space in midclavicular line, parasternal heave present, P2 palpable, and S1 loud.
Ejection systolic murmur was present in the pulmonary area. Her electrocardiography was done, which revealed incomplete RBBB but no other significant abnormality [Figure 1].
Figure 1.
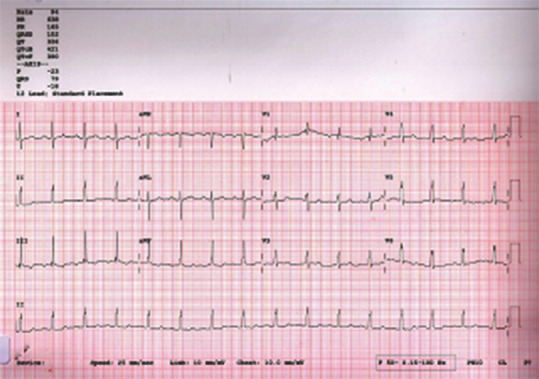
Electrocardiography of the patient shows incomplete RBBB
A 2D transthoracic echocardiogram was performed in the usual manner with a Vivid T8 General Electric (Milwaukee, Wisconsin, USA) ultrasound system and a 3 MHz transducer. It showed situs solitus of the atria, AV concordance, D-loop ventricles, and ventriculoarterial concordance. There was a complete absence of interatrial septum, dilated right atrium, and right ventricle associated with morphologically normal AV valves attached at the same level at crux [Figure 2 and Supplementary Video 1].
Figure 2.
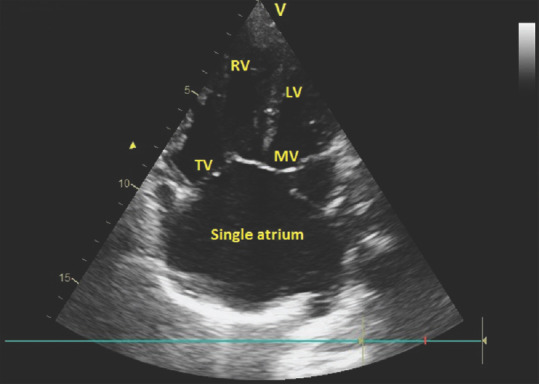
Apical 4-chamber view is showing single atrium with closed atrioventricular valves
There was no evidence of any ventricular septal defect or patent ductus arteriosus. There was no cleft in mitral leaflets, no mitral regurgitation, mild tricuspid regurgitation (TR), and significant pulmonary arterial hypertension measured by TR jet velocity [Figures 3 and 4 and Supplementary Videos 2–4].
Figure 3.
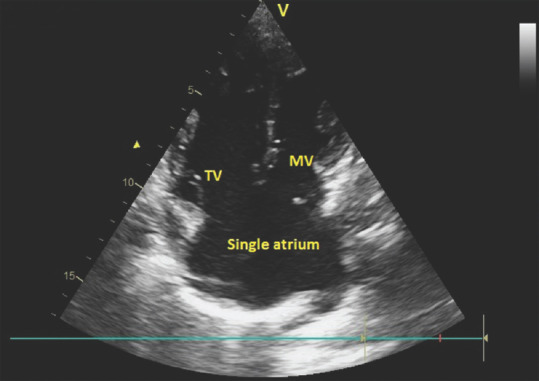
Apical 4-chamber view is showing single atrium with atrioventricular valves in opened position with no mitral regurgitation
Figure 4.
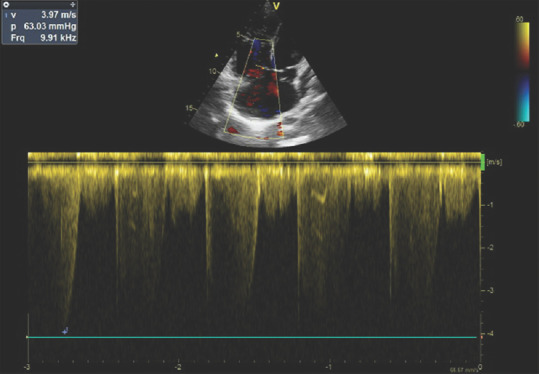
Significant pulmonary hypertension measured by tricuspid regurgitation jet velocity
On the basis of echocardiographic findings suggestive of SA, significant pulmonary hypertension, and arterial desaturation, the patient was sent for cath study followed by further management.
DISCUSSION
The terms CA and SA have been used interchangeably in the literature. CA was first reported by Young and Robinson in 1907.[1] In 1959, Ellis et al. published an article about the diagnosis and surgical treatment of CA (Cor triloculare biventriculare).[2] The term “CA” is used for the condition where there is (i) either atrial septum is completely absent or it is represented by the small strand of tissue at the superior atrial wall of the common chamber, (ii) no interventricular communication, and (iii) AV cushion defect.[3] A cleft mitral leaflet is almost always present with this condition.[4]
Levy et al. described SA (also known as cortriloculare biventriculare) as one of the rare congenital anomaly identified by the complete absence of the atrial septum without an endocardial cushion defect. It is characterized by: (i) complete absent atrial septum, (ii) no AV valves malformation, and (iii) no interventricular communication. They suggested that the term CA should be used to denote the condition of complete absence of the atrial septum, accompanied by malformation of the AV valves, with or without interventricular communication.[5]
One differential diagnosis of SA is heterotaxy syndrome, in which there is a failure of differentiation into right- and left-sided organs with resulting congenital malformations of multiple organ systems, including complex malformation of the cardiovascular system. Asplenia syndrome is associated with the absence of the spleen, which is a left-sided organ, and a tendency for bilateral right-sidedness. In polysplenia syndrome, multiple splenic tissues are present, with a tendency for bilateral left-sidedness. Our patient had a history of recurrent abortion and she underwent for sonographic examination of the abdomen multiple times in the past which did not reveal any abnormality.
Our patient demonstrated typical echocardiographic features of three-chambered heart (SA), which is a rare entity. Although 3D echo and cardiac magnetic resonance imaging are more useful modalities for the present case, the patient was not willing for any further investigation because of financial constraint.
The case study proves that echocardiography is also a useful modality for the diagnosis of SA and for differentiating it from CA.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Supplementary Videos Available on: www.jcecho.org
Acknowledgment
Dr. Ashok Garg would like to thank Dr. G. L. Sharma for collecting all relevant and useful data from various resources for writing this case report and also like to thank Dr. Deepak Agrawal for his valuable support in preparing this review article as per the criteria of journal and also for proofreading and submission of the article.
REFERENCES
- 1.Young AH, Robinson A. Some malformations of the human heart. M Chron 1907. 1908;47:96–106. [Google Scholar]
- 2.Ellis FH, Jr, Kirklin JW, Swan HJ, Dushane JW, Edwards JE. Diagnosis and surgical treatment of common atrium (cor triloculare-biventriculare) Surgery. 1959;45:160–72. [PubMed] [Google Scholar]
- 3.Rastelli GC, Rahimtoola SH, Ongley PA, McGoon DC. Common atrium: Anatomy, hemodynamics, and surgery. J Thorac Cardiovasc Surg. 1968;55:834–41. [PubMed] [Google Scholar]
- 4.Muñoz-Armas S, Gorrín JR, Anselmi G, Hernández PB, Anselmi A. Single atrium. Embryologic, anatomic, electrocardiographic and other diagnostic features. Am J Cardiol. 1968;21:639–52. doi: 10.1016/0002-9149(68)90261-0. [DOI] [PubMed] [Google Scholar]
- 5.Levy MJ, Salomon J, Vidne BA. Correction of single and common atrium, with reference to simplified terminology. Chest. 1974;66:444–6. doi: 10.1378/chest.66.4.444. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.