

As a result of the outbreak of Severe Acute Respiratory Syndrome CoronaVirus 2 (SARS-CoV-2) infection that developed in France during spring 2020, the French government imposed a lockdown from March 17 to May 11. All non-urgent gynecological procedures, including surgery, were postponed. A decrease in planned activity was expected, but we also observed an unexpected reduction in urgent gynecological consultations that theoretically should not have decreased (heavy menstrual bleeding, pelvic infectious disease, ectopic pregnancy, etc.).
To evaluate the impact of the COVID-19 pandemic and of lockdown on gynecological emergencies, we collected the number of consultations and admissions in the 12 gynecological emergency units of the Greater Paris University Hospitals (AP-HP; Assistance Publique - Hôpitaux de Paris, Paris, France) before and during lockdown. Data were collected from 11 hospitals (Antoine Béclère, Armand-Trousseau, Beaujon, Bichat, Cochin, Le Kremlin Bicêtre, Lariboisière, Louis-Mourier, Necker, Pitié-Salpêtrière, Robert-Debré, and Tenon).
Data were collected from January 1 to May 31, 2020 and compared to the data collected over the same period in 2019. Our hypothesis was that the global number of “emergency” consultations decreased, whereas the number of emergency hospitalizations did not. In other words, that the number of “real” life-threatening emergencies did not diminish (fewer women coming to the emergency room for benign gynecological disease, such as vaginal candidiasis).
We extracted data from the Opale database, which prospectively records monthly activity by means of the different IT/software applications of the AP-HP. Overall, there was a decrease in the number of consultations in the emergency gynecological units between 2019 and 2020 over the same period (March to May) (24,982 in 2019 vs 14,708 in 2020, a 41 % decrease). We also observed a reduction in the number of emergency gynecological hospitalizations, but twofold less when compared to the decrease in emergency consultations (−20 %) between the two periods. Finally, the hospitalization/consultation ratio increased from 3.9 % to 5.4 % (p < .0001). Data are detailed in Table 1 and Fig. 1 .
Table 1.
Comparison of urgent gynecological care between the same periods in 2019 and 2020.
| Three-month periods | Dec 2018 to Feb 2019 | March to May 2019 | Dec 2019 to Feb 2020 | March to May 2020 (lockdown) | ǂp value |
|---|---|---|---|---|---|
| Consultations in gynecological emergency units (n) | 24,095 | 24,982 | 24,217 | 14,708 | ǂp< .000000001 |
| Emergency hospitalizations for gynecological disease (n) | 1081 | 976 | 1078 | 785 | |
| Hospitalization rate | 4.4 % | 3.9 % | 4.6 % | 5.3 % |
n, number.
Comparison between the hospitalization rate during the 2020 3-month lockdown and the same period in 2019.
Fig. 1.
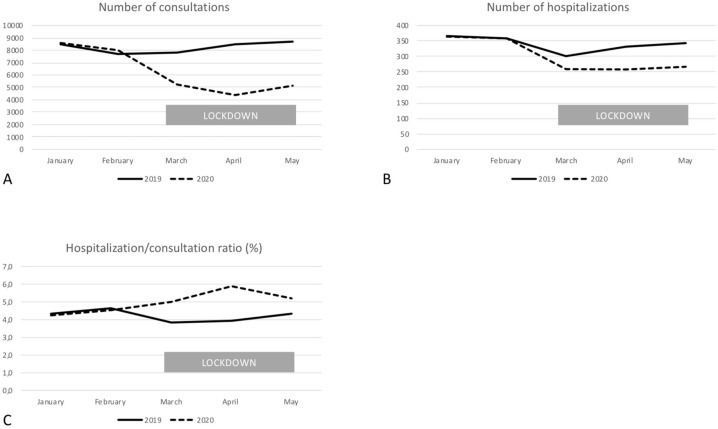
Activity in gynecological emergency units during the COVID-19 pandemic and lockdown in Paris, France. A = total consultations per month; B = total hospitalizations (emergency unit only) per month; C = ratio between consultations and hospitalizations.
Several hypotheses may be formulated to explain these findings. Firstly, during the pandemic period, patients might be reluctant to consult at hospital, since they were afraid to contract a nosocomial SARS-CoV-2 infection. We know that many consultations do not really require the emergency department. Probably, the number of these non-urgent consultations decreased, without significant clinical impact. This finding is supported by the smaller decrease in hospitalizations in comparison to consultations. However, non-urgent symptoms could reveal malignant diseases (for example post-menopausal vaginal bleeding and endometrial cancer).
Another explanation could relate to the reorganization of the health care system, with increased private practice. Unfortunately, it was not possible to assess this point precisely, but many private practices closed of reduced their activity during lockdown.
Part of the decrease in activity was possibly because there were fewer consultations for surgical complications following postponement of non-urgent gynecological procedures.
We can also imagine that the breakdown of social relations caused by outbreak may have reduced incidence of some gynaecological disease such as sexually transmitted diseases.
Furthermore, some gynecological diseases do require urgent consultation (ectopic pregnancies, pelvic infectious disease, ovarian torsion, etc.), especially when they are progressive. If women are reluctant to seek help in these situations, delayed diagnoses and delayed management will likely have short-term and long-term impacts. For example, in the case of ectopic pregnancy, delayed consultation could lead to tubal rupture and hemoperitoneum, which would have been avoided by an earlier consultation. It will be interesting to evaluate the impact of the COVID-19 pandemic on the complications or management of some specific emergency medical conditions. Likewise, there was probably a modification in the distribution of the reasons for and context of consultations.
Finally, the COVID-19 pandemic and lockdown probably limited non-urgent consultations, but gynecological emergency admissions has not decreased as much. However, no consultation or a delayed consultation for non-urgent symptoms (such as post-menopausal vaginal bleeding) may delay management of malignant diseases. The overall clinical and health consequences remain unknown. Further studies, including analysis of the diagnosis and management of patients, should be conducted.