

Abstract
In this meta-analytic and narrative review, we examine several overarching issues related to the study of coping, emotion regulation, and internalizing and externalizing symptoms of psychopathology in childhood and adolescence, including the conceptualization and measurement of these constructs. We report a quantitative meta-analysis of 212 studies (N = 80,850 participants) that measured the associations between coping and emotion regulation with symptoms of internalizing and externalizing psychopathology. Within the meta-analysis we address the association of broad domains of coping and emotion regulation (e.g., total coping, emotion regulation), intermediate factors of coping and emotion regulation (e.g., primary control coping, secondary control coping), and specific coping and emotion regulation strategies (e.g., emotional expression, cognitive reappraisal) with internalizing and externalizing symptoms. For cross-sectional studies, which made up the majority of studies included, we examine three potential moderators: age, measure quality, and single vs. multiple informants. Finally, we separately consider findings from longitudinal studies as these provide stronger tests of the effects. After accounting for publication bias, findings indicate that the broad domain of emotion regulation and adaptive coping and the factors of primary control coping and secondary control coping are related to lower symptoms of psychopathology. Further, the domain of maladaptive coping, the factor of disengagement coping, and the strategies of emotional suppression, avoidance and denial are related to higher symptoms of psychopathology. Finally, we offer a critique of the current state of the field and outline an agenda for future research.
Keywords: coping, emotion regulation, children, adolescents, psychopathology
The identification of processes of risk and resilience is crucial for understanding the etiology of internalizing and externalizing symptoms and disorders in childhood and adolescence and for the development of interventions for the prevention and treatment of these symptoms and disorders (e.g., Cicchetti & Curtis, 2007; Kraemer, Lowe, & Kupfer, 2005; Luthar, 2006; Masten, 2001, 2014; Troy & Mauss, 2011). Exposure to acute and chronic stressful events and adversity is one of the most potent risk factors for psychopathology during childhood and adolescence (e.g., Evans, Li, & Whipple, 2013; Grant et al., 2003; Kushner, 2015). Yet not all who experience stress and adversity go on to develop symptoms of psychopathology, raising the question, why are some children and adolescents adversely affected while others are resilient? The ability to cope with stressful events and circumstances and regulate emotions across situations may play a primary role in the development of resilience and reducing the risk for psychopathology during childhood and adolescence (Compas, Gruhn, & Bettis, 2017; McRae & Mauss, 2016; Zimmer-Gembeck & Skinner, 2016). Given the potential to inform our understanding of processes of risk, resilience, and intervention, research on coping and emotion regulation in children and adolescents is of considerable importance for the field of developmental psychopathology and prevention science. However, despite a large and growing body of research, there has been no quantitative meta-analysis of the association of coping and emotion regulation with symptoms of internalizing and externalizing psychopathology in children and adolescents. Therefore, an integrative, quantitative review of this research is a high priority.
Although there are many commonalities between these constructs, research on coping and emotion regulation has remained relatively separate (e.g., Compas, Jaser, & Benson, 2009; Compas et al., 2014a; Kopp, 1989; Zalewski, Lengua, Wilson, Trancik, & Bazinet, 2011; Zimmer-Gembeck et al., 2014). For example, Compas et al. (2014a) found that although both coping and emotion regulation are active areas of research, only 208 of 20,804 publications (1%) between 2003 and 2012 identified in a PsycINFO search included both of these concepts as key terms. There has been little integration of the conceptualization and measurement of these two processes. Further, confusion in defining and conceptualizing coping and emotion regulation in youth, as well as identifying clear dimensions or subtypes of these processes, has inhibited the synthesis and integration of findings (Skinner, Edge, Altman, & Sherwood, 2003). In addition, the measurement of coping and emotion regulation is characterized by a large and ever-expanding number of measures, many of which are of unknown psychometric quality. Finally, it has been 16 years since the last comprehensive review of coping and internalizing and externalizing psychopathology in children and adolescents (Compas, Connor-Smith, Saltzman, Thomsen, & Wadsworth, 2001) and 7 years since the last review of emotion regulation and these broad domains of psychopathology in young people (Eisenberg, Spinrad, & Eggum, 2010). Notably, neither of these reviews provided quantitative meta-analyses.
To address these gaps in the field, we begin by examining several overarching issues related to the study of coping, emotion regulation, and psychopathology in children and adolescents. First, we consider several broad issues in this field including definitions and conceptualizations of coping and emotion regulation in childhood and adolescence, the status of the measurement of coping and emotion regulation, the role of exposure to acute and chronic stressors and the experience of emotions in the development of psychopathology, and previous reviews on the associations of coping and emotion regulation with symptoms of psychopathology. In the primary section of this review, we report on a quantitative meta-analysis of the associations between coping and emotion regulation and internalizing and externalizing symptoms. We also consider three possible moderators of the association of coping and emotion regulation with symptoms of psychopathology: child age, the quality of measures of coping and emotion regulation, and the use of single vs. multiple informants to measure coping and emotion regulation and symptoms of psychopathology. Finally, we offer a critique of the current state of the field and outline an agenda for research to advance our understanding of coping and emotion regulation in youth.
Coping and Emotion Regulation: Definitions and Conceptualization
Previous reviews have noted a lack of consensus in the definition and conceptualization of coping and emotion regulation in children and adolescents (e.g., Adrian, Zeman, & Veits, 2011; Compas et al., 2001; Eisenberg et al., 2010; Skinner et al., 2003). Clear consensus on the definitions of coping and emotion regulation is needed in order to identify the boundaries of what is and is not included within each of these constructs, shape the identification of the structure and subtypes of coping and emotion regulation, and guide the selection of measures for research on the association of coping and emotion regulation with psychopathology. It is encouraging, therefore, that since earlier reviews of coping and emotion regulation there have been some signs of convergence on the central features of these constructs.
Definitions of Coping and Emotion Regulation
The challenge of establishing consensus regarding definitions of coping and emotion regulation is reflected in the 212 studies included in the meta-analysis reported below. The most widely used definitions of coping and emotion regulation in childhood and adolescence are presented in Table 1. Both the Lazarus and Folkman (1984) and Compas et al. (2001) definitions of coping highlight the role of coping as a process of responding to stress. Further, both definitions emphasize coping as a controlled, effortful process; i.e., responses that require conscious, purposeful, and intentional thoughts and behaviors. However, Lazarus and Folkman (1984) emphasize cognitive appraisals of stress as precipitants of coping responses, whereas Compas et al. (2001) focus on objectively stressful events or circumstances in the environment as precipitants of coping responses. The Lazarus and Folkman model incorporates two broad types of coping that differ based on the focus and goals of coping efforts: problem-focused coping (i.e., efforts to resolve the source of stress, including problem solving) and emotion-focused coping (i.e., efforts to palliate one’s emotions, including seeking social support and escape/avoidance) (e.g., Folkman & Moskowitz, 2004). The Compas et al. (2001) definition is linked to a control-based model of coping that includes primary control coping (i.e., efforts to directly act on the source of stress or one’s emotions, including problem solving and emotional expression), secondary control coping (i.e., efforts to adapt to the source of stress, including acceptance and cognitive reappraisal), and disengagement coping (i.e., efforts to orient away from the source of stress or one’s emotions, including avoidance or denial) (e.g., Compas, Jaser, Dunn, & Rodriguez, 2012; Rudolph, Dennig, & Weisz, 1995; Weisz, McCabe, & Dennig, 1994). Further, the scope of the construct of coping has broadened since the earlier work of Lazarus and Folkman (1984), with a growing emphasis on coping as the regulation of a wider range of functions, including emotion, behavior, cognitions, physiology, and the environment, in response to stress (e.g., Compas et al., 2001; Eisenberg, Fabes, & Guthrie, 1997; Kopp, 1989).
Table 1.
Definitions of coping and emotion regulation.
| Citation | Construct of Interest | Definition |
|---|---|---|
| Cicchetti and colleagues (e.g., Cicchetti, Ganiban, & Barnett, 1991) | Emotion Regulation | “For the purposes of this study, emotion regulation was defined in terms of lability, flexibility, and situational responsivity and conceptualized as the capacity to modulate one’s emotional arousal such that an optimal level of engagement with one’s environment is fostered (Cicchetti, Ganiban, & Barnett, 1991; Thompson, 1994).” |
| Compas and colleagues (e.g., Compas et al., 2001; Connor-Smith et al., 2000) | Coping | “conscious and volitional efforts to regulate emotion, cognition, behavior, physiology, and the environment in response to stressful events or circumstances” (Compas et al., 2001; p. 89) |
| Eisenberg and colleagues (e.g., Eisenberg et al., 1997, 2010) | Emotion Regulation | “processes used to manage and change if, when, and how (e.g., how intensely) one experiences emotions and emotion-related motivational and physiological states, as well as how emotions are expressed behaviorally” (p. 495). |
| Thompson, Gross and colleagues (e.g., Gross & Thompson, 2007, 2010; Thompson, 1991, 1994; Thompson & Calkins, 1996) | Emotion Regulation | “the extrinsic and intrinsic processes responsible for monitoring, evaluating, and modifying emotional reactions, especially their intensive and temporal features, to accomplish one’s goals” (Thompson, 1994; p. 27–28) |
| Lazarus and colleagues (e.g., Folkman & Lazarus, 1985; Lazarus & Folkman, 1984; Lazarus & Launier, 1978) | Coping | “constantly changing cognitive and behavioral efforts to manage specific external and/or internal demands that are appraised as taxing or exceeding the re-sources of the person” (Lazarus & Folkman, 1984; p. 141) |
The most commonly cited definition of emotion regulation emphasizes processes of monitoring, evaluation, and modification of emotional reactions. Specifically, Thompson (1994) defines emotion regulation as, “the extrinsic and intrinsic processes responsible for monitoring, evaluating, and modifying emotional reactions, especially their intensive and temporal features, to accomplish one’s goals” (pp. 27–28). These regulation processes involve a series of steps that include the selection and modification of situations that give rise to emotions, the deployment of attention in response to emotion, cognitive change, and modulation of emotional responses. This process model of emotion regulation includes strategies such as problem solving, cognitive reappraisal, and emotional suppression and emphasizes the deployment of these strategies as part of the temporal process of the experience and regulation of emotions (Gross & Thompson, 2007). Similar elements can be found in the work of Eisenberg et al. (2010) who focus on the construct of emotion-related self-regulation, defined as, “processes used to manage and change if, when, and how (e.g., how intensely) one experiences emotions and emotion-related motivational and physiological states, as well as how emotions are expressed behaviorally” (p. 516). We now consider in more detail several key issues reflected in these definitions of coping and emotion regulation.
Shared features of coping and emotion regulation.
Although research on these constructs has predominately been conducted separately, there is considerable overlap in the concepts of coping and emotion regulation. A unifying feature of conceptualizations of coping and emotion regulation is the central role of regulatory processes (e.g., Compas et al., 2014a; Eisenberg et al., 1997; Gross & Thompson, 2007; Zimmer-Gembeck et al., 2014). Regulation involves a broad array of responses, including efforts to initiate, delay, terminate, modify the form/content, or modulate the amount or intensity of a thought, emotion, behavior, or physiological reaction (Compas et al., 2001). Coping includes the regulation of these processes that occur specifically in response to a stressor, whereas emotion regulation occurs in response to the presence of an emotion whether or not the emotion arises in response to a stressor (Aldao, Nolen-Hoeksema, & Schweizer, 2010; Thompson, 1994).
Kopp (1989) argued that, “emotion regulation is a term used to characterize the processes and characteristics involved in coping with heightened levels of positive and negative emotions” (p. 343; italics added). Similarly, Skinner, Zimmer-Gembeck and colleagues (e.g., Skinner & Wellborn, 1994; Skinner & Zimmer-Gembeck, 2007; Zimmer-Gembeck & Skinner, 2011; Zimmer-Gembeck et al., 2014) define coping as action regulation under stress, which includes coordination, mobilization, energizing, directing and guiding behavior, emotion, and orientation when responding to stress. Thus, the terms coping and regulation are used somewhat interchangeably in definitions of coping and emotion regulation.
In addition, the process model of emotion regulation by Gross, Thompson and colleagues includes responses that are directed toward other processes in addition to emotions (e.g., Gross, 2015; Gross & Thompson, 2007; Thompson, 1991, 1994; Thompson & Calkins, 1996; Thompson & Goodman, 2010). As noted above, this conceptual model includes efforts directed at the context in which emotions occur, the cognitive processes that may shape and influence emotions, and modulation of behavioral responses. Similarly, Eisenberg, Hofer, and Vaughan (2007) include emotions, emotion-related motivational and physiological states, and the behavioral expression of emotions within the realm of emotion regulation. In this way, emotion regulation encompasses the broad array of processes (i.e., emotion, cognition, behavior, context) that are also included within the concept of coping. Further, as discussed in more detail below, there is significant overlap in the strategies that are included as subtypes of both coping and emotion regulation. For example, problem solving, cognitive reappraisal, acceptance, emotional expression, and avoidance have all been included as strategies in both coping and emotion regulation research (Aldao et al., 2010; Skinner et al., 2003).
Conceptualizations of coping and emotion regulation also share a distinction between automatic and controlled processes (e.g., Mauss, Bunge, & Gross, 2007). A fundamental contrast throughout psychological science is made between dual-processes that are characterized as automatic vs. controlled, including distinctions between processes that are labeled as regulation vs. reactivity, intentional vs. incidental, conscious vs. non-conscious, and voluntary vs. involuntary (e.g., Bargh & Williams, 2007; Connor-Smith et al., 2000; Eisenberg et al. 2007, 2010; Gross & Thompson, 2007). Automatic, incidental, involuntary processes are rooted in temperamental differences in reactivity to the environment that emerge early in development; further, some responses are acquired through processes of associative conditioning that do not involve conscious control (e.g., Compas, Connor-Smith, & Jaser, 2004). In contrast, controlled, intentional, voluntary responses often involve higher-order, complex cognitive processes that are thought to develop more fully in middle and late childhood (Zimmer-Gembeck & Skinner, 2016).
There are several reasons to focus on controlled as opposed to automatic processes in examining the relations of coping and emotion regulation with symptoms of psychopathology. Controlled processes reflect both covert cognitive and overt behavioral strategies that children and adolescents purposefully use to cope with stress and regulate their emotions. These responses occur in both stressful and emotionally arousing situations and may be more accessible to conscious awareness than non-conscious processes (Rabiner, Lenhart, & Lochman, 1990). Consequently, controlled processes, or at least those within conscious awareness, may be more amenable to self-reports and reports by other informants of these efforts (e.g., Compas et al., 2014a). In addition, controlled processes are less likely than automatic processes to be confounded with symptoms of internalizing and externalizing psychopathology. For example, an automatic anger response may be highly correlated with symptoms of externalizing psychopathology in part because anger is included as an externalizing symptom (e.g., Achenbach & Rescorla, 2001). Lastly, controlled processes can be more readily changed than automatic processes through interventions that are designed to enhance resilience by teaching skills for coping with stress and regulating emotions. A growing body of evidence suggests that interventions targeting coping and emotion regulation skills are efficacious in the prevention and treatment of psychopathology in children and adolescents (e.g., Compas et al., 2010; Lochman & Wells, 2004; Tein, Sandler, Ayers, & Wolchik, 2006; Tein, Sandler, MacKinnon, & Wolchik 2004). Thus, the focus of the current meta-analysis will be on controlled processes of coping and emotion regulation in childhood and adolescence.
In spite of the relative importance of focusing on controlled processes of coping and emotion regulation, some examples of these processes present significant challenges, as they may reflect both automatic and controlled processes. Rather than a simple dichotomy, automatic and controlled processes lie on a continuum (Gross & Thompson, 2007; Hopp, Troy, & Mauss, 2011). Some processes that are initially automatic may be brought under purposeful control, and processes that require effort may become automatized with repeated practice (e.g., Evers et al., 2014; Hankin, Badanes, Smolen, & Young, 2015; Mauss et al., 2007). However, the distinction between controlled and automatic processes remains central to understanding both coping and emotion regulation. One noteworthy example of this comes from research on rumination (e.g., Nolen-Hoeksema, Wisco, & Lyubomirksy, 2008). Rumination can occur in the form of uncontrollable, intrusive thoughts or as purposefully dwelling on thoughts about one’s emotions, as in the case of depressive rumination. Because rumination is conceptualized and measured as both an automatic and controlled process and because previous meta-analyses have established that rumination has a large positive correlation with symptoms of psychopathology (Aldao et al., 2010), rumination and other constructs that may reflect both automatic and controlled processes were excluded from the current review.
Unique features of coping and emotion regulation.
These shared features notwithstanding, a primary distinction between models of coping and emotion regulation centers on the precipitants for these two processes. As noted above, coping refers to processes that are generated specifically in response to stressful events or circumstances. This encompasses efforts to regulate responses (including emotions) to acute life events, chronic stressors, daily hassles, and conditions of chronic adversity, all of which have been shown to be significant risk factors for symptoms of psychopathology (Harkness & Monroe, 2016). In contrast, emotion regulation includes responses aimed at the generation and modulation of emotions. Emotions arise in response to stress and adversity but also occur as a part of ongoing, normative experiences of daily life that do not involve stressful events or circumstances (e.g., an emotionally moving film or book). This contrast suggests that coping is both a narrower and broader construct than emotion regulation. Coping is a narrower construct in that it is limited to responses in the context of stressors while emotion regulation occurs in response to both stressful and non-stressful circumstances. However, coping is also a broader construct in that it encompasses the regulation of a wider range of processes that includes not only emotions, but also cognition, behavior, physiology, and sources of stress in the environment. These differences notwithstanding, given the increasing recognition of common elements between coping and emotion regulation, a review of the ways that both of these processes relate to internalizing and externalizing psychopathology in childhood and adolescence is timely and needed.
Structure and Subtypes of Coping and Emotion Regulation
A quantitative analysis of the association of coping and emotion regulation with symptoms of psychopathology requires the clear delineation of subtypes of these constructs; however, as noted above there has been relatively little agreement regarding the structure of coping and emotion regulation. For example, in a seminal review of the structure of coping, Skinner et al. (2003) identified over 400 different subtypes that have appeared in research across childhood, adolescence, and adulthood. These include widely studied coping and emotion regulation strategies such as problem solving, cognitive reappraisal, cognitive avoidance, emotional expression, and acceptance, as well as less frequently examined strategies such as physical exercise, stoicism, and thought stopping.
The lack of consensus about the structure of coping and emotion regulation has slowed progress in the field (Compas et al., 2001, 2014a; Skinner et al., 2003). The most obvious problem is the difficulty in comparing and accumulating results from different investigations. Measures differ in the items that are included within dimensions of coping and emotion regulation, making it difficult to aggregate findings relevant to the same stressor or precipitant or to compare results across different stressors or precipitants. Compas et al. (2001) concluded that “There has been little consistency in the application of these various subtypes of coping across different measures and studies … leading to considerable difficulty developing a cohesive picture of the structure of coping in childhood and adolescence” (p. 92). Notably, relatively little progress has been made to address this problem in the last 16 years.
The identification of the structure of coping and emotion regulation has been approached using either bottom-up models (i.e., derived through exploratory factor analysis [EFA] or through rational grouping of strategies) or top-down models (i.e., theory-driven and tested using confirmatory factor analysis [CFA]) systems). Problems identified with bottom-up approaches include lack of clarity, limited comprehensiveness of categories, inability to determine hierarchical structures, and difficulty determining whether categories are distinct (Skinner et al., 2003). In contrast, Skinner et al. (2003) highlight the merits of three top-down coping structures that have been supported using CFA with reference to children and adolescents (Ayers, Sandler, & Twohey, 1998; Connor-Smith et al., 2000; Walker, Smith, Garber, & Van Slyke, 1997). The strengths of these and other top-down approaches include tests of clear conceptual models of the structure of coping and emotion regulation, the development of measures that reflect these models, use detailed and complex data analytic approaches, and cross-validation with multiple large samples (Skinner et al., 2003). Further, Skinner et al. (2003) note that although these models are not without problems they “represent guideposts for empirical efforts to search for the structure of coping” (p. 232).
We consider these models of coping in more detail in the measurement section that follows. Further, we include those measures based on top-down theory-driven systems with factor structures that have been tested using CFA as an indicator of measurement quality in the moderator analyses presented as a part of the meta-analysis below. It is noteworthy that no similar efforts to catalogue and examine the structure of emotion regulation have appeared in the literature; however, some emotion regulation measures were derived using a top-down approach (e.g., Children’s Emotion Management Scales; Zeman, Cassano, Suveg, & Shipman, 2010; Zeman, Shipman, & Penza-Clyve, 2001) and construct validity has been established for these measures with CFA.
Summary
In spite of some distinctions in their conceptualization, we believe that coping and emotion regulation have many more similarities than differences and that it is timely and advantageous to collectively examine research on these processes in children and adolescents. Driven in part by these similarities, the current meta-analysis is the first to examine both coping and emotion regulation in relation to internalizing and externalizing symptoms of psychopathology in children and adolescents.
Measurement of Coping and Emotion Regulation
To test the association of coping and emotion regulation with symptoms of internalizing and externalizing psychopathology, measures must meet accepted standards of reliability and validity. As research on these constructs has grown, this growth would ideally be reflected in increasing consensus and rigor in research designs and methods of measurement. It is a concern, therefore, that the number of measures of coping and emotion regulation in children and adolescents is large and still increasing. Further, the continued proliferation of measures is partly a reflection of the lack of consensus regarding the structure of coping and emotion regulation. The over 400 subtypes of coping identified by Skinner et al. (2003) were drawn from more than 100 different measures of coping, and over a decade later, new measures continue to be developed (e.g., Maxwell & Cole, 2012; Sveinbjornsdottir & Thorsteinsson, 2014). The field of emotion regulation is somewhat newer and still emerging. Nonetheless, Adrian et al. (2011) reported on 100 measures of emotion regulation used in studies from 1975 through 2010, and new emotion regulation measures continue to be developed. In this section, we review the measures used to study the association of coping and emotion regulation with symptoms of psychopathology in children and adolescents, with a focus on self-report and other informant (e.g., parents, teachers) measures used most frequently in the meta-analysis that follows.
The measurement of coping and emotion regulation has been primarily characterized by four approaches: questionnaires completed by children and adolescents or other informants, interviews, direct observations of behavior, and measures of physiological processes (e.g., Adrian et al., 2011; Blount et al., 2008; Compas et al., 2001; Eisenberg et al., 2010; Skinner et al., 2003). Research on emotion regulation in particular has employed experimental designs to examine the processes of regulation in the laboratory, including the use if observational and physiological measures. Examples of this include paradigms that elicit negative emotions and instruct participants to use specific emotion regulation strategies to regulate the experience of negative emotion (e.g., Gross & John, 2003; Morris et al., 2011; Nolen-Hoeksema et al., 2008; Webb, Schweiger, Miles, Gollwitzer, & Sheeran, 2012). Although direct observations of behavior (e.g., displays of emotion) and measurement of physiological processes (e.g., heart rate) provide important information on how people respond to stress, these methods do not allow for the direct measurement of controlled, often covert, cognitive strategies that children and adolescents use to cope with stress and regulate their emotions. There is evidence that both self-reports and reports from other informants can provide reliable measurement of children’s coping and emotion regulation strategies, including covert cognitive strategies, as evidenced by studies demonstrating significant cross-informant correlations, such as secondary control coping (e.g., Compas et al., 2006a, 2014b; Connor-Smith et al., 2000). The focus of the current review, therefore, is on self- or other-report measures of coping and emotion regulation and internalizing and externalizing symptoms.
Quality of Questionnaire Measures of Coping and Emotion Regulation
Several features of questionnaire measures of coping and emotion regulation are important to consider: (a) the sources of stress and specific emotions that are the precipitant(s) of the regulatory responses assessed by the measure, (b) the source of information/informant, and (c) types of coping and emotion regulation that are captured by these measures. The studies included in the meta-analysis that follows were selected in part based on the criteria that they employed measures designed to assess coping or emotion regulation and that, at minimum, reliability data had been reported in the literature. In the 212 studies included, 87 distinct measures were used. Of these measures, thirteen were modified versions of existing measures; these modifications included using a single subscale from an established measure or adding or omitting items from an established measure.
In Table 2, we highlight the 16 coping and emotion regulation measures that were used in at least three studies included in the meta-analysis. The most commonly used coping measures were the Responses to Stress Questionnaire (RSQ; Connor-Smith et al., 2000) and the Children’s Coping Strategies Checklist (CCSC; Ayers, Sandler, West, & Roosa, 1996). The most commonly used measures of emotion regulation were the Emotion Regulation Checklist (ERC; Molina et al., 2014; Shields & Cicchetti, 1997) and the Cognitive Emotion Regulation Questionnaire (CERQ; Garnefski, Kraaij, & Spinhoven, 2001).
Table 2.
Coping and emotion regulation measures used in studies included in the current meta-analysis.
| Author(s) and Measure | Age Group and Informant(s) | Stressor/Emotion | Format and Scales | Reliability Data | Validity Data | Number of Studies in Meta-Analysis |
|---|---|---|---|---|---|---|
| Emotion Regulation Measures | ||||||
| Abela et al. (2000); Children’s Response Styles Quesitonnaire (CRSQ) | Developed and tested in 3rd – 7th graders; Self-report |
Depressive Symptoms | 25 items, 3 scales Domains: none Factors: none Strategies: Distraction Problem Solving |
Internal consistency: α’s ranged from .57 to .76 Test-retest correlations ranged from .55–.67 |
Three-factor and Two-factor models were tested. The two-factor model was confirmed in a Turkish sample |
5 |
| Garnefski et al. (2001); Cognitive Emotion Regulation Questionnaire (CERQ) | Age 12–17 years; Self-report |
Threatening or stressful life events | 36 items, 9 scales Domains: none Factors: none Strategies: Acceptance Positive Refocusing Refocus on Planning Positive Reappraisal Putting into Perspective Blaming Others |
Internal consistency: α’s ranged from .68 to .83 with most .80. Test-retest correlations ranged from .40 – .60 |
Principal component analyses provided empirical support to the allocation of items to subscales | 8 (1 used modified version) |
| Gratz & Roemer (2004); Weinberg & Klonsky (2009) Difficulties in Emotion Regulation Scale (DERS) | Age 18–55 years; (tested in adolescents age 13–17); Self-report |
“When I’m upset” | 36 items, 6 scales Domains: Clarity Impulse Factors: none Strategies: none |
Internal consistency: α’s > .80 for each subscale (overall DERS = .93) Test-retest correlations ranged from .57 – .89 (.88 for overall score) Adolescent sample: internal consistency (α’s ranged from .76–.89). |
Construct validity: correlations with another measure of emotion regulation and emotional expressivity. DERS subscales showed a differential pattern of association with the constructs of interest. Adolescent sample: Confirmatory factor analysis supported 6 factors. |
5 |
|
Gross & John (2003); Emotion Regulation Questionnaire (ERQ) Gullone et al., (2011) Emotion Regulation Questionnaire for Children and Adolescents (ERQ-CA) |
Developed for Adults; ERQ-CA tested in ages 10–18 years; Self-report |
Negative emotions | 10 items; 2 scales Domains: none Factors: none Strategies: Cognitive Reappraisal Emotional Suppression |
Internal consistency: α’s averaged .79 for Reappraisal (.83 in child and adolescent sample) and .73 for Suppression (.75 in child and adolescent sample); Test-retest correlations over 3 months were .69 for both scales |
Exploratory factor analyses supported two factors; confirmatory factor analyses on same sample; confirmatory factor analysis in children and adolescents supported 2 scales; tested convergent and discriminant validity with other measures of coping, personality, and mood regulation (COPE, Trait MegaMood questionnaire; Negative Mood Regulation Scale; Big Five Inventory) |
5 (1 used modified version) |
| Shields & Cicchetti (1994); Emotion Regulation Checklist (ERC) | Age 6–18 years; Other-report |
24 items, 2 scales Domains: Emotion Regulation Factors: none Strategies: none |
Internal consistency: Reliability α’s are high for the overall scale (.89) and for the subscale Regulation = .83. | Principal Components Factor Analysis yielded two factors | 12 | |
| Zeman, Shipman, & Penza-Clyve; Zeman, Cassano, Suveg & Shipman, 2010; Children’s Emotion Management Scales (CEMS) | Age 7–17 years; Self-report | Feeling angry/sad/worried | Sad and Worry - 12 items, Mad - 11 items, 3 scales Domains: Coping/Cope Emotion Regulation Factors: none Strategies: Inhibition |
Internal consistency: α’s range from .62–.77. Test-retest correlations range from .61 −.80. |
Principal Components Analysis supported 3 factors; Convergent validity demonstrated with Emotion Awareness Scale, Emotion Regulation Checklist, and Affect Regulation Interview |
6 |
| Coping Measures | ||||||
| Ayers et al., (1996); Children’s Coping Strategies Checklist (CCSC) and How I Cope Under Pressure (HICUPS) | Age 9–13 years; Self-report |
CCSC: General Coping Style; HICUPS: Child-selected stressor |
52 items, 4 scales Domains: none Factors: Active Coping Support Seeking Strategies: Avoidance Distraction |
Internal consistency: α’s ranged from .73 to .89 for secondary scales | Confirmatory factor analysis demonstrated superiority of theoretic model to other models | 22 (6 used modified version) |
|
Carver et al. (1989); Coping with Problems Experienced (COPE) And Brief COPE |
Adults; Self-report |
General Stress | 60 items, 15 scales Domains: Religious Coping Factors: Active Coping Behavioral Disengagement Seeking Social Support (emotional and instrumental) Strategies: Planning Positive Reframing Acceptance Denial Humor |
Internal consistency: α’s ranged from .43–.85. Test-retest reliability over 2 weeks ranged from .46 – .86; over 8 weeks ranged from .42 – .89 |
Inconsistent findings of factor structure | 15 (3 used modified version) |
| Causey & Dubow (1992); Self Report Coping Scale (SRCS) | 4th-6th grade; Self-report | Social and Academic Stressor versions | 34 items, 5 scales Domains: none Factors: Seeking Social Support Strategies: Self-Reliance/Problem Solving Distancing |
Internal consistency: α’s ranged from .66 to .84 Test retest over 2 weeks ranged from .66 to .84 |
Self-report scales moderately correlated with abbreviated version completed by peers | 6 (4 used modified version) |
| Connor-Smith et al. (2000); Responses to Stress Questionnaire (RSQ) | Self-report: 9–17 years; Parent report: 6–17 years | Stressor- and Domain-Specific versions (e.g., parental depression, type 1 diabetes) | 57 items, 5 scales Domains: none Factors: Primary Control Secondary Control Disengagement Strategies: none |
Internal consistency: α’s ranges from .67 – .84; test-retest 1–2 weeks .69–.81 | Confirmatory factor analysis and latent variable analyses across 7 different samples support 3 coping factors; Cross-informant correlations; convergent and discriminant validity data reported with COPE. | 28 (1 used modified version) |
| Ebata & Moos, 1991; Coping Response Inventory - Youth (CRI-Y) and CRI-YF | 12–18 years; Self-report |
Most important problem in previous year | 48 items; 2 scales; 8 subscales Domains: none Factors: Seeking Guidance Strategies: Logical Analysis Positive Reappraisal Cognitive Avoidance Acceptance/Resignation Seek Alternate Rewards Emotional Discharge |
Internal consistency: α’s ranged from .55 – .79 | Not reported | 4 |
| Frydenberg & Lewis (1993); Adolescent Coping Scale (ACS) | 12–16 years; Self-report | Specific Form - how an individual copes with a specific stressor and General Form - how individual copes in general | 88 items; 3 scales Domains: Nonproductive Coping Factors: Reference to Others Strategies: none |
Internal consistency: α’s ranged from .87 – .89; Test-retest reliability (stability over unspecified time frame): .44–.81 | Confirmatory factor analysis supported 3 coping styles in relplication study (1996) | 8 (1 used modified version) |
| Patterson & McCubbin (1991); Adolescent Coping Orientation for Problem Experience (A-COPE) | Mean age = 15 years; Self-report |
General coping style | 54 items; 12 scales Domains: Total Coping Factors: Seeking Spiritual Support Investing in Close Friends Seeking Professional Support Strategies: Seeking Diversions Avoiding Problems Engaging in Demanding Activities |
Internal consistency: α’s ranged from .50 – .76 | Not reported | 4 (1 used modified version) |
| Seiffge-Krenke (1995); Coping Across Situations Questionnaire (CASQ) | 15–27 years; Self-report | Eight age-specific problems areas | 20 items; 3 scales Domains: none Factors: Active Coping Internal Coping Strategies: Withdrawal |
Internal consistency: α’s ranged from .76–.80 | Confirmatory factor analyses replicated findings in samples from Israel and Finland | 5 |
| Spirito, Stark, & Williams (1988); KidCope | 12–18 years; Self-report |
Specific areas selected by participant or experimenter | 10 items; no specific scales Domains: Total Score Factors: none Strategies: none |
Internal consistency: None. Only provide test-retest reliability for individual items |
Item correlations with coping scales for CSI and A-COPE | 4 |
| Walker et al. (1997); Pain Response Inventory (PRI) | 8–23 years; Self-report |
Specific Stress (pain) | 60 items; 3 scales Domains: none Factors: Active Coping Passive Coping Accommodative Coping Strategies: none |
Internal consistency: α’s range from .64–.82 Test-retest reliability 1 week: .46–.71; 6 months: .34–.46 |
Confirmatory Factor Analysis validated across samples | 6 |
Note. Only scales that were included in the meta-analysis are listed.
Coping and emotion regulation: Domains, factors, and strategies.
Given the large number of measures and labels used across the studies included in the current meta-analysis, we employed an organizational framework to combine data. Studies of coping and emotion regulation in children and adolescents have examined these constructs on at least three levels: domains, factors, and strategies (see Methods and Appendix). These three levels reflect current, albeit somewhat overlapping approaches to the measurement of coping and emotion regulation in children and adolescents.
At the broadest level, domains of coping and emotion regulation are grouped into relatively undifferentiated categories including total coping, emotion regulation, emotion dysregulation, adaptive coping, and maladaptive coping. These broad domains include varied and heterogeneous coping and emotion regulation strategies. For example, examination of the association between total coping and symptoms of psychopathology ostensibly addresses the question of whether it is “better or worse” to engage in more vs. less coping, with no consideration of the strategies used to cope. The only distinction that has been made at the broadest level of domains is between those strategies that are distinguished as adaptive vs. maladaptive (or as regulation vs. dysregulation) on an a priori basis. However, the basis for this distinction is often not clear, as these categories remain very heterogeneous with regard to the strategies that they encompass. Further, labeling types of coping and emotion regulation as adaptive or maladaptive on an a priori basis can result in circular tests of the association between these processes and symptoms of psychopathology. That is, a positive association between maladaptive coping and symptoms is interpreted as evidence that this domain of coping is indeed maladaptive, which was already assumed at the outset.
Studies included in the current meta-analysis that measured the domain of total coping used a wide range of measures that capture a diverse array of strategies (e.g., Adolescent Coping Scale, ACS; Frydenberg & Lewis, 1993; CCSC; Ayers et al., 1996; CEMS; Zeman et al., 2010; Kidcope; Spirito, Stark, & Williams, 1988). Total coping captures any efforts to cope with or regulate emotions in response to stress, and therefore total coping is typically the sum or total score of all coping items on a measure. Because these scores do not differentiate among types of coping efforts, they provide little information regarding types of coping that may be more or less beneficial than others under specific stressful circumstances. Similarly, studies measuring adaptive coping in the current review used a variety of measures (e.g., A-COPE; Patterson & McCubbin, 1991; ACS; Frydenberg & Lewis, 1993; Kidcope; Spirito et al., 1988). The domain of maladaptive coping, however, was predominantly measured using the non-productive coping scale of the ACS (Frydenberg & Lewis, 1993). This scale includes items that assess the degree to which children and adolescents use strategies such as self-blame, withdrawal, wishful thinking, and avoidance to cope with stress.
Some measures of the broad domain of emotion regulation may capture more trait-like aspects of cognition and behavior rather than specific strategies used to regulate one’s emotions (e.g., ERC; Shields & Cicchetti, 1997). Emotion dysregulation has been measured primarily with the Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, 2004). Items on the DERS capture the inability to use or the ineffective use of strategies to regulate emotions. A concern with the DERS and other measures of emotion dysregulation is the considerable overlap with measures of psychopathology, particularly internalizing symptoms.
At the intermediate level, coping and emotion regulation are grouped into empirically derived or theoretically derived factors that include problem-focused coping, emotion-focused coping, engagement/approach coping, disengagement coping, primary control coping, secondary control coping, and social support coping. The most common approach to identifying coping factors has been the use of bottom-up approaches (EFA) that do not involve testing a priori models. Relatively fewer studies have used top-town approaches (CFA) to test theory-driven models of coping and emotion regulation (Skinner et al., 2003). Although these mid-level factors also include a wide range of specific strategies, they are more homogeneous with regard to the strategies that they encompass.
Presently, the most stringent tests and, therefore the strongest evidence for the structure of coping and emotion regulation come from measures that are designed to assess the factors of coping and emotion regulation. In addition to the three models of coping using CFA highlighted by Skinner et al. (2003) noted above (Ayers et al., 1996; Connor-Smith et al., 2000; Walker et al., 1997), two additional models of coping have been tested using CFA (Frydenberg & Lewis, 1993; Seiffge-Krenke, 1995). The most extensive support for the structure of coping has been generated using the RSQ (Connor-Smith et al., 2000), which has been tested using CFA in samples of children and adolescents. A total of six studies reporting on seven independent samples faced with a wide range of different stressors across a number of countries and ethnic groups using CFA have confirmed the three-factor structure of the RSQ: primary control coping (problem-solving, emotional expression, emotional modulation), secondary control coping (acceptance, cognitive reappraisal, positive thinking, distraction), and disengagement coping (avoidance, denial, wishful thinking) (Benson et al., 2011; Compas et al., 2006b; Connor-Smith & Calvete, 2004; Connor-Smith et al., 2000; Wadsworth, Rieckmann, Benson, & Compas, 2004; Xiao et al., 2010). The three factors in the RSQ parallel factors included in two other coping measures: the Pain Response Inventory (PRI; active, accommodative, passive coping; Walker et al., 1997) and the Children’s Coping Strategies Checklist (CCSC; active coping, avoidance, distraction; Ayers et al., 1996). It is noteworthy that, although several of the emotion regulation measures have established construct validity using CFA, no emotion regulation measures include scales at the factor level.
The third level includes specific strategies of coping and emotion regulation, including emotional expression, emotional suppression, problem solving, cognitive reappraisal, distraction, acceptance, avoidance, wishful thinking, denial, emotional modulation, unregulated release of emotions, and humor. Although Skinner et al. (2003) identified over 400 coping strategies, we grouped individual strategies into these 12 categories to create a manageable number for the current meta-analysis and because these were the most commonly used categories among the included studies (see Appendix). These categories provide a fine-grained analysis of specific strategies that children and adolescents use to cope with stress and regulate their emotions. However, measures at this level reflect only a relatively small sample of the larger set of coping and emotion regulation strategies that children and adolescents may enact when faced with a stressor or emotion, and there is relatively less data on the psychometric properties of measures used to assess specific strategies.
Potential Moderators of Associations of Coping and Emotion Regulation with Psychopathology
Given the absence of a comprehensive quantitative review of the association of coping and emotion regulation with symptoms of psychopathology in children and adolescents, the primary focus of the current review is on the direct associations between these constructs. However, we recognize the importance of taking initial steps to examine constructs that may moderate these associations. Therefore, in addition to the direct association of coping and emotion regulation with internalizing and externalizing psychopathology in children and adolescents, we also examine age, measure quality, and informant as potential moderators of these associations in the meta-analysis that follows.
Age and Development
Processes of biological, cognitive, social, and emotional development during childhood and adolescence have implications for the development of coping and emotion regulation skills and their association with symptoms of psychopathology. Several reviews have outlined possible developmental patterns in coping and emotion regulation that would suggest increasing efficacy and flexibility in the use of specific strategies with age (Skinner & Zimmer-Gembeck, 2007, 2010; Thompson & Goodman, 2010; Zimmer-Gembeck & Skinner, 2011, 2016). Although these constructs have been analyzed relatively independently in developmentally focused research, several parallel themes in the development of coping and emotion regulation have emerged from these reviews. These include developmental shifts in the use of social partners in coping and regulating emotions vs. self-reliance to enact these processes, an increased ability to utilize cognitively complex processes (e.g., cognitive reappraisal), changes in the use of overt behavioral strategies (e.g., avoidance, distraction), and an increased capacity to use a wider range of strategies flexibly in response to stress or emotions (Skinner & Zimmer-Gembeck, 2007, 2010; Thompson & Goodman, 2010; Zimmer-Gembeck & Skinner, 2011).
Although important developmental changes in the coping and emotion regulation may occur in infancy and toddlerhood (Thompson & Goodman, 2010), we focus here on early and middle childhood and adolescence because these are the developmental periods encompassed by the studies included in the current meta-analytic review. During early childhood, children’s increased understanding of emotions enables parents to shift from directly controlling children’s emotional reactions to coaching them in the development of emotion regulation strategies. In middle childhood, children begin to use strategies that are more cognitive in nature (e.g., cognitive reappraisal or distraction) as well as relaxation strategies to reduce physiological arousal (e.g., deep breathing) (Goodman & Thompson, 2010). From middle childhood into adolescence, peer relationships gain importance and serve as a source of support as well as further learning about emotional experiences, norms for expression, and emotion regulation strategies. During middle and late adolescence, increased ability to think about one’s own and others’ emotions allows for more independent management of emotions. Additionally, the development of executive function skills allows adolescents to enlist additional cognitive emotion regulation strategies and to be more controlled in their expression of emotions (Thompson & Goodman, 2010).
In contrast, there is less clarity regarding the development of coping. This is due in part to inconsistencies in the measurement of coping across ages and studies, and in part because research has not been designed for the specific purpose of examining coping development (Skinner & Zimmer-Gembeck, 2007; Zimmer-Gembeck & Skinner, 2011). However, the aforementioned reviews provide evidence for developmental changes, many of which parallel changes in the development of emotion regulation. In early childhood (i.e., the 5 to 7-year-old-shift) social support begins to incorporate peers in addition to a continued reliance on caregivers, and children use problem solving and behavioral distraction with increasing frequency. Further, as noted above, in middle childhood, cognitive strategies develop, support seeking becomes more complex, and the ability to take others’ perspectives and understand that different situations may require different coping responses begins to form. With increased reliance on cognitive strategies, declines in the use of behavioral strategies such as escape and avoidance are observed (Skinner & Zimmer-Gembeck, 2007; Zimmer-Gembeck & Skinner, 2011). In adolescence, coping repertoires expand and coping efforts become more self-reliant. The importance of peers increases during adolescence, and adolescents continue to seek social support as a means of coping with stress; however, the majority of coping efforts are at the individual level with social partners in the role of a “back up system” if independent efforts fail (Skinner & Zimmer-Gembeck, 2010, p. 19). Additionally, adolescents are more effective at selecting different sources of social support depending on the type of stressor (Skinner & Zimmer-Gembeck, 2007). Furthermore, with the development of meta-cognitive skills, adolescents achieve greater flexibility and sophistication in their coping, and coping strategies continue to become more cognitive in nature (Skinner & Zimmer-Gembeck, 2010).
Especially relevant for the current study, the connections of coping and emotion regulation with psychopathology may become stronger as children develop and move into adolescence. As the implementation of coping and emotion regulation efforts increase in complexity, the stressful events and circumstances children and adolescents encounter likely also increase in complexity (Grant et al., 2006). Further, there is a significant increase in the incidence and prevalence of some forms of psychopathology in adolescence, including increased rates of anxiety, depression, eating disorders, and conduct problems (e.g., Copeland, Shanahan, Costello, & Angold, 2011). Notably, little research has been devoted to examining the developmental trajectory of both coping and emotion regulation and symptoms of psychopathology in tandem.
In order to further explore developmental variations in associations among coping and emotion regulation and psychopathology, we examined age as a moderator by testing these associations in studies with child samples as compared to adolescent samples. As noted above, this distinction captures a critical developmental transition, including increasing self-reliance in coping, the use of peers as social resources, and the growth of meta-cognitive and executive function skills that may provide a foundation for the use of more complex cognitive coping and emotion regulation strategies (Skinner & Zimmer-Gembeck, 2010; Thompson & Goodman, 2010).
Measure Quality
The present review includes measures of coping and emotion regulation that meet at least the most basic psychometric criterion; i.e., the availability of data on internal consistency. More stringent criteria for evidence-based methods of assessment include test-retest reliability and construct and criterion validity (e.g., Blount et al., 2008); however, these standards are rarely met in measures of coping and emotion regulation. Only three coping measures (CCSC, Ayers et al. 1996; RSQ, Connor-Smith et al., 2000; PRI, Walker et al. 1997) meet the criteria for top-down, theory-based measures of coping laid out by Skinner et al. (2003). These criteria include the use of CFA to test the fit of items into lower order coping categories and empirically examine hierarchical systems that also test the fit of multiple lower order ways of coping into higher order categories. Further, only three emotion regulation measures (DERS, Gratz & Roemer, 2004; ERQ, Gross & John, 2003; CEMS, Zeman et al., 2010) report on convergent and/or discriminant validity with other measures of emotion regulation or coping. Notably, the majority of validity data reported is from EFA or principal components analysis. These tests have typically not been replicated and therefore are not viewed as strong as tests of theoretically derived models that have been tested using CFA (Skinner et al., 2003).
Validity has also been examined infrequently through multi-informant reports of coping and emotion regulation (i.e., report from child and their caregiver). For example, the ways in which children cope with chronic pain as reported by parents and children have been shown to predict cross-informant reports of anxiety and depression in latent variable analyses (Compas et al., 2006b). Further, self-report coping questionnaires have been validated through associations with physiological measures, including glycemic control in children with diabetes (e.g., Jaser et al., 2012) and heart rate reactivity to laboratory stressors (Connor-Smith et al., 2000; Dufton, Dunn, Slosky, & Compas, 2011). Overall, the introduction of some psychometrically strong measures since the previous narrative analyses (e.g., Compas et al., 2001) suggests that more recent studies may reflect improvement in measurement quality.
Because of enduring concerns about the ability of questionnaires to adequately capture processes of coping and emotion regulation, we have included measurement quality as a potential moderator of effects in the meta-analysis that follows. To code measure quality, we used the criterion of the presence of data on the internal consistency of measures of domains, factors and strategies (see Rueger, Malecki, Pyun, Aycock, & Coyle, 2016; Skinner et al., 2003).
Informant
The assessment of child and adolescent psychopathology has a long tradition of obtaining reports of internalizing and externalizing symptoms from children’s and adolescents’ self-reports and reports from other informants including parents, teachers, mental health professionals, and trained observers (e.g., Achenbach, McConaughy, & Howell, 1987; De Los Reyes et al., 2015; Podsakoff, MacKenzie, & Podsakoff, 2012; Rescorla et al., 2013). By comparison, the measurement of coping and emotion regulation in young people has relied predominantly on self-report measures. The majority of the coping and emotion regulation measures included in the current meta-analysis were designed only for self-report and a much smaller number were designed to only obtain reports from other informants (typically parents). As a consequence, much of the literature is characterized by studies that have relied on single informant report of both coping and emotion regulation and internalizing and externalizing symptoms. The use of the same informant for both constructs may artificially inflate the magnitude of these associations due to problems of shared method variance in the measures of coping and emotion regulation with measures of psychopathology (see LeGrange & Cole, 2008). As such, we have included the use of a single informant to assess both coping and emotion regulation and psychopathology vs. the use of different informants to assess these constructs (i.e., multi-informant) as a possible moderator of the magnitude of these associations.
Cross-Sectional and Longitudinal Research Designs
Studies of the association of coping and emotion regulation with internalizing and externalizing symptoms have varied with regard to the use of cross-sectional vs. longitudinal designs. Cross-sectional designs cannot test the temporal sequence of the association between coping and emotion regulation and internalizing and externalizing symptoms (Podsakoff et al., 2012). Although longitudinal designs cannot provide evidence for causal relations, these designs are a more rigorous test of the degree to which coping and emotion regulation account for variance in symptoms across time. Therefore, studies that include longitudinal data provide important tests of the association between coping and emotion regulation and symptoms of psychopathology over time. In the meta-analytic review below, we present findings for cross-sectional and longitudinal studies separately.
Stress, Emotions and Psychopathology in Children and Adolescents
The backdrop to research on coping and emotion regulation in children and adolescents lies in current conceptualizations of psychopathology, the role of exposure to stressful events and circumstances as a source of risk, and relations between stress and emotions. As summarized in a series of reviews by Grant and colleagues (Grant et al., 2003, 2006; Grant, Compas, Thurm, McMahon, & Gipson, 2004; Grant, McMahon, Duffy, Taylor, & Compas, 2011; McMahon, Grant, Compas, Thurm, & Ey, 2003), exposure to psychosocial stressors and conditions of chronic adversity is well established as a major risk factor for internalizing and externalizing psychopathology during childhood and adolescence. Grant et al. (2004) identified over 50 prospective longitudinal studies that provided evidence that exposure to stressful events and chronic adversity predicts increases in both internalizing and externalizing symptoms over time. Consistent with the heuristic model of Nolen-Hoeksema and Watkins (2011), exposure to stressful life events appears to function as a distal risk factor whose association with internalizing and externalizing symptoms is both mediated and moderated by more proximal factors, including the ways children and adolescents cope with stressful events and regulate their emotions (Grant et al., 2003, 2006). Further, McMahon et al. (2003) found evidence that exposure to stressful events and chronic adversity is a nonspecific risk factor that places children and adolescents at risk for the full range of internalizing and externalizing forms of psychopathology.
Exposure to stressors (i.e., environmental events or chronic conditions that objectively threaten the physical and/or psychological health of individuals) is distinct from the concept of psychological stress, which is defined as an internal state experienced by the individual rather than the occurrence of stressors in the environment (Grant et al., 2003). Psychological stress as a concept has been criticized as overly vague and has been supplanted by a focus on specific emotions (Gross, 1999, 2001; Lazarus, 1999, 2006). Further, research has moved toward an increasing emphasis on physiological aspects of the stress response system including reactivity in the hypothalamic-pituitary-adrenal axis (e.g., Doom & Gunnar, 2013; Han, Miller, Cole, Zahn-Waxler, & Hasting, 2016) and cardiac vagal tone (e.g., McLaughlin, Alves, & Sheridan, 2014). With the shift in focus from psychological stress to specific emotions, research on emotion regulation has emphasized the importance of identifying and regulating discrete emotions including sadness, anger, and anxiety (e.g., Zeman, Cassano, Suveg, & Shipman, 2010; Zeman, Shipman, & Suveg, 2002). Further, in the process model of emotion regulation (e.g., Gross, 2001; Gross & Jazaieri, 2014; Gross, Sheppes, & Urry, 2011), efforts are distinguished in the context of the phases of the emotion-generative process. The phases during which specific emotions are regulated include both antecedent-focused strategies, which influence an emotion before it is fully formed, and response-focused strategies, which influence an emotion once it has been fully developed. Antecedent-focused strategies include situation selection (e.g., avoidance of emotionally arousing situations), situation modification (e.g., problem solving), attentional deployment (e.g., distraction), and cognitive change (e.g., cognitive reappraisal), and response-focused strategies include response modulation (e.g., emotional suppression).
Together, this research suggests that it is important to consider both how children and adolescents cope with the occurrence of stressors in the form of stressful events and conditions of chronic adversity in the environment and regulate specific emotions as they arise in ongoing transactions with the environment. We return to these issues in the Discussion after presenting the findings of the current meta-analysis.
Dimensional and Categorical Features of Internalizing and Externalizing Psychopathology
Examination of the association of coping and emotion regulation with psychopathology also requires careful consideration of the nature of internalizing and externalizing symptoms and disorders, as this shaped the selection of relevant studies for inclusion in this meta-analysis. After a longstanding debate regarding the structure of psychopathology, a significant shift has occurred in the conceptualization of psychopathology, with recognition that symptoms of disorder occur both on continua as well as in discrete categories (Hyman, 2010; Rutter et al., 2011). Further, the National Institute of Mental Health Research Domain Criteria (RDoC; Casey, Oliveri, & Insel, 2014; Insel, 2010; Insel & Cuthbert, 2015) represents a dimensional framework that conceptualizes mechanisms underlying psychopathology in five domains (negative valence systems, positive valence systems, cognitive systems, systems for social processes, and arousal and regulatory systems) that can be assessed across multiple levels of analysis.
The preponderance of research on coping and emotion regulation in children and adolescents has focused on dimensional approaches to psychopathology, reflected in both broad and narrowband syndromes of psychopathology. Evidence for the broad factors of internalizing and externalizing symptoms of psychopathology and narrow subtypes within these broad categories initially described by Achenbach (1966) provides strong support for dimensional models (e.g., Krueger & Markon, 2006; Lahey, Van Hulle, Singh, Waldman, & Rathouz, 2011; Seeley, Kosty, Farmer, & Lewinsohn, 2011). These dimensions have been identified in studies of children, adolescents, and adults and across a wide range of cultures and countries (e.g., Ivanova et al., 2007a; Ivanova et al., 2007b; Rescorla et al., 2012). In addition, Kraemer, Noda and O’Hara (2004) note that although both categorical and dimensional approaches are fundamentally equivalent, dimensional approaches are advantageous for hypothesis testing because of the loss of power associated with the use of categorical variables. Given the strong evidence for the broad dimensions of internalizing and externalizing symptoms (Achenbach & Rescorla, 2001), these are the focus of the current review.
Evidence of the co-occurrence of symptoms and diagnostic comorbidity (Rhee, Lahey, & Waldman, 2015) both within and across internalizing and externalizing symptoms of psychopathology has led to research on sources of risk and resilience that are either specific to or common across multiple symptom dimensions and disorders. As reflected in the 212 studies included in the current meta-analytic review, processes of coping and emotion regulation are prime candidates for transdiagnostic sources of risk and/or resilience in children and adolescents (Compas, Watson, Reising, & Dunbar, 2013).
Previous Reviews of the Association of Coping and Emotion Regulation with Psychopathology
Several reviews have examined the associations between coping and emotion regulation and symptoms of psychopathology in adults (e.g., Aldao et al., 2010; Nolen-Hoeksema, 2012; Webb et al., 2012). In one of the most comprehensive meta-analyses to date, Aldao et al. (2010) estimated associations for dispositional measures of six emotion regulation strategies with four types of symptoms of psychopathology from 114 studies (108 studies with adults and 6 studies with children). This meta-analysis found medium to large positive associations for rumination with symptoms of anxiety, depression, disordered eating, and substance use, and small to medium positive associations for avoidance and suppression with symptoms of anxiety, depression, and disordered eating. In addition, they found small to medium negative associations for problem solving with anxiety, depression, and disordered eating, and a small negative association for reappraisal with symptoms of depression. No significant associations were found for acceptance. It is noteworthy that the emotion regulation strategies included in this review have also been commonly studied as examples of coping strategies (Aldao et al., 2010). The current review builds on this important meta-analysis by focusing exclusively on coping and emotion regulation in children and adolescents and using an inclusive framework for what is considered coping and emotion regulation.
In addition, several narrative reviews have examined the relations between coping and emotion regulation and internalizing and externalizing symptoms. Eisenberg et al. (2010) described the association of children’s emotion regulation with internalizing and externalizing problems. They reported a general pattern of negative associations between emotion regulation and internalizing and externalizing problems in samples ranging from infancy through childhood and adolescence. More narrowly focused reviews have examined coping and emotion regulation with specific samples or subgroups and specific outcomes. Examples include adolescents coping with social stressors (Clarke, 2006), adolescents coping with relationship stressors (Seiffge-Krenke, 2011), children coping with the chronic stress associated with poverty (Evans & Kim, 2013), and children and adolescents coping with chronic illness (Aldridge & Roesch, 2007; Blount et al., 2008; Compas et al., 2012). We extend these narrative reviews by conducting a meta-analysis to estimate the associations of a broad range of domains, factors, and strategies of coping and emotion regulation in response to a wide range of stressors and emotions with symptoms of internalizing and externalizing symptoms in children and adolescents.
In one of the only previous meta-analyses of coping and emotion regulation in childhood and adolescence, Clarke (2006) examined the relations between active coping and psychosocial health among youth in 40 studies of coping with interpersonal stress. Four areas of psychosocial functioning were examined: externalizing and internalizing behavior problems, social competence, and academic performance. The association between active coping and psychosocial functioning across the four areas examined was small, with correlations ranging from .02 to .12 (Clarke, 2006). In a second meta-analysis of 26 studies including children and adolescents, Aldridge and Roesch (2007) examined how children cope with cancer-related stress based on two coping taxonomies: approach vs. avoidance coping and problem-focused vs. emotion-focused coping. In this analysis, approach, avoidance, and emotion-focused coping were unrelated to overall adjustment. A small positive association was found between problem-focused coping and adjustment, indicating use of problem-focused coping was associated with poorer adjustment. Most recently Schäfer, Naumann, Holmes, Tuschen-Caffier, and Samson (2017) conducted a meta-analysis of the association between emotion regulation strategies and symptoms of depression and anxiety in adolescence. Results from this review of 35 studies indicated that emotion regulation strategies considered to be adaptive (cognitive reappraisal, problem solving, and acceptance) were significantly negatively related to symptoms of anxiety and depression and those considered to be maladaptive (avoidance, suppression, and rumination) were significantly positively related to symptoms of depression and anxiety. The present meta-analysis builds on these reviews by integrating a larger and more inclusive set of studies of coping and emotion regulation in response to a wider range of stressors and emotions and including studies of both internalizing and externalizing symptoms.
The most recent comprehensive review of coping and internalizing and externalizing psychopathology in childhood and adolescence appeared 16 years ago (Compas et al., 2001). This review provided a summary of findings from 63 published studies that reported on analyses of coping and internalizing and externalizing symptoms of psychopathology in children and adolescents. The authors conducted a narrative review as a function of two broad dimensions of coping: engagement vs. disengagement coping and problem-focused vs. emotion-focused coping. The general pattern of findings suggested that forms of engagement coping and problem-focused coping were associated with lower internalizing and externalizing symptoms. In contrast, disengagement coping and emotion-focused coping were generally associated with higher levels of internalizing and externalizing symptoms. However, this review did not provide quantitative analyses of these patterns of findings.
In spite of these contributions from recent reviews, several key issues have not yet been examined. First, none of these reviews have explicitly included processes of both coping and emotion regulation in children and adolescents. Second, measures of coping and emotion regulation have not been evaluated with regard to their psychometric quality. Third, there has been no quantitative meta-analysis of the associations of coping and emotion regulation with internalizing and externalizing symptoms in children and adolescents.
The Present Study: Meta-Analysis
To determine the association of coping and emotion regulation with symptoms of internalizing and externalizing psychopathology in children and adolescents, we examine studies from 2001 through 2012 in which these constructs were measured. Our goal is to estimate effect sizes for broad domains, intermediate factors, and specific strategies of coping and emotion regulation. We examine effects for internalizing symptoms and externalizing symptoms of psychopathology.
We address three central questions: (1) Are broad domains of coping and emotion regulation associated with internalizing and externalizing symptoms of psychopathology in children and adolescents? (2) Are intermediate factors of coping and emotion regulation associated with internalizing and externalizing symptoms? (3) Are specific coping and emotion regulation strategies associated with total internalizing and externalizing symptoms? We also examine three potential moderators of these associations: age, measure quality, and informant (i.e., single informant vs. multiple informant). We also examine findings separately for cross-sectional and longitudinal studies. We consider the implications of the answers to these questions for the conceptualization of coping and emotion regulation, the measurement of these constructs, and directions for future research.
Method
Literature Search
We searched for empirical reports published from January 2001 to December 2012 to identify articles that examined coping or emotion regulation in relation to internalizing and externalizing symptoms of psychopathology in children and adolescents. The start date of 2001 covers articles since the last comprehensive review of coping and internalizing and externalizing symptoms in children and adolescents (Compas et al., 2001). We selected the date of this earlier review as the starting point for the current meta-analysis because this marked a significant shift in the measures that were most frequently used to measure coping and emotion regulation. Our systematic literature search was conducted using the PsycINFO database, with the specific search terms coping OR emotion regulation AND child* (for child or children) OR adolesc*(for adolescents or adolescence) across all fields (i.e., title, abstract, keywords). We further limited the search to peer-reviewed, English language journal articles. The initial search process yielded 7,085 articles (see Figure 1 for a PRISMA flow diagram). In addition, we supplemented our search by reviewing the reference sections of published review articles on coping and emotion regulation, yielding an additional 24 articles. A brief review of the titles and abstracts resulted in 1,107 articles that appeared to report an association between coping or emotion regulation and psychopathology in children or adolescents. Based on inclusion criteria outlined below, 212 studies were included in the quantitative meta-analysis. Book chapters, non-peer reviewed journal articles, review articles, and dissertations were not included, consistent with recent meta-analytic reviews of coping and emotion regulation (e.g., Aldao et al., 2010). We believed that restricting our search to published peer-reviewed articles would yield higher quality studies. Further, we reduced the concern for file-drawer effects by including all reported effects of coping or emotion regulation in each study, including non-significant effects.
Figure 1.
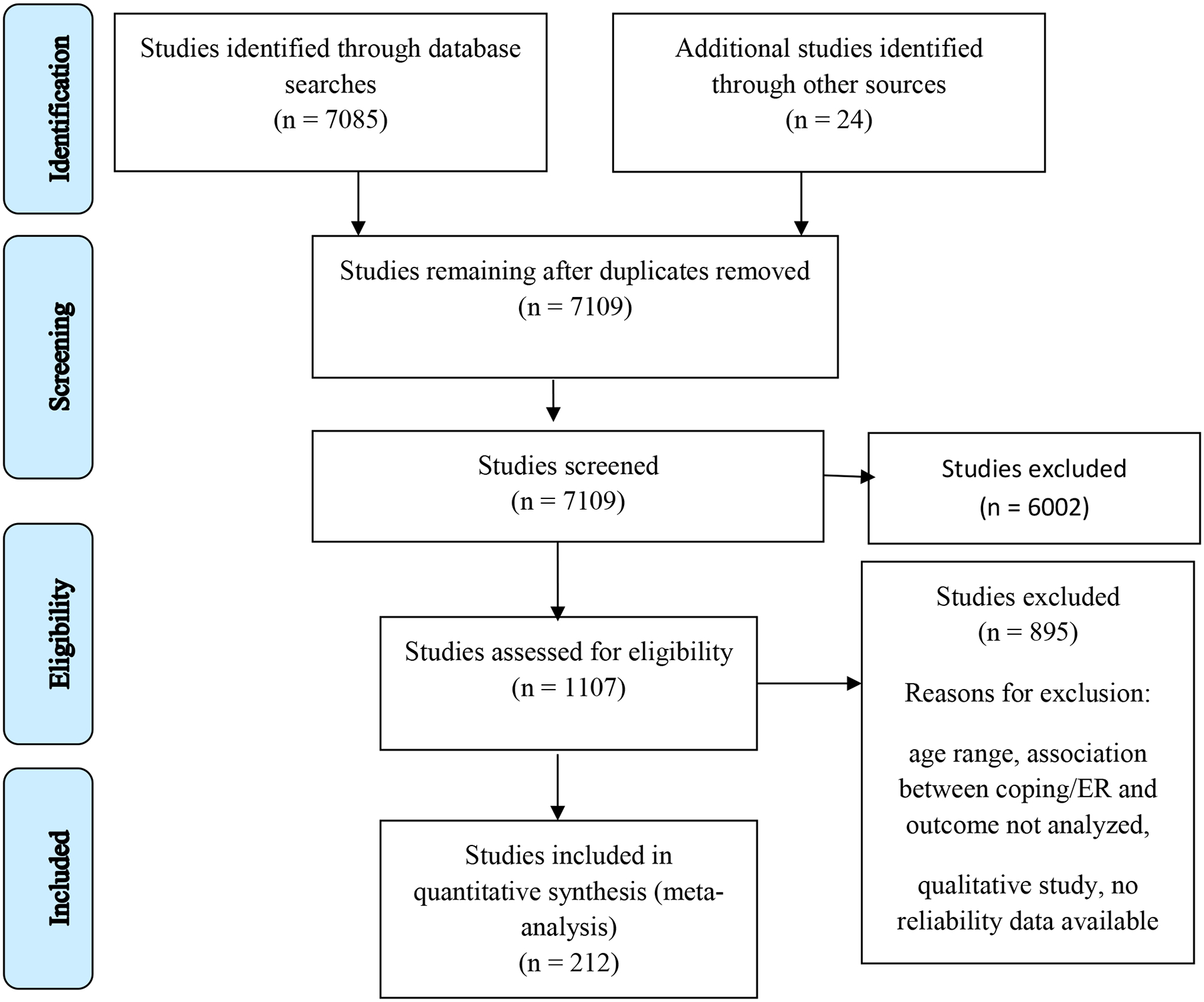
PRISMA flow diagram.
Inclusion Criteria
The following criteria determined the selection of studies included in the meta-analysis:
Studies were included if they assessed children or adolescents between the ages of 5 to 19-years-old. We excluded studies that included younger children (infants or preschool age) because the methodologies used to study coping and emotion regulation in children under age 5 differ substantially from those used with school-aged children (e.g., observation of behavior to draw inferences about regulatory strategies). Further, research on the development of coping and emotion regulation indicates that infants and preschool age children have not yet fully developed the cognitive skills needed to employ many of the more complex cognitive strategies (e.g., cognitive reappraisal, problem solving) that are the focus of this review (Zimmer-Gembeck & Skinner, 2016). We excluded older adolescents (i.e., age 20) to avoid confounding our results with college age samples.
Studies were included if they used a measure of coping and/or emotion regulation that reported reliability data in the study sample or if reliability data for that measure was reported elsewhere in the literature (e.g., Cronbach’s alpha). Further, because reliability cannot be calculated with two items or less, coping or emotion regulation scales with fewer than three items were excluded from analyses.
Studies were included if they measured reports of coping and/or emotion regulation in response to emotions or actual stressors or events. Measures that elicited responses to hypothetical scenarios, or asked participants how they would cope or regulate their emotions in a given situation, were excluded.
Studies were included if measures of coping and/or emotion regulation assessed controlled processes. Coping and/or emotion regulation scales that may reflect more automatic or involuntary responses to stress (e.g., catastrophizing, rumination, emotional or physiological reactivity) were excluded from analyses.
Studies were included if they used at least one reliable measure of internalizing or externalizing symptoms of psychopathology. The measures that were included in these studies are widely used in research on child and adolescent psychopathology (see Table 3 for a list of the measures used in the included studies). Similar to the criteria for coping and emotion regulation measures, we did not include psychopathology measures that consisted of only one or two items (e.g., alcohol use in past week).
Studies were included if they reported a test of the relationship between coping and/or emotion regulation and internalizing and/or externalizing symptoms, and if the study reported adequate statistics to calculate effect sizes. Thus, qualitative studies were not included.
Studies were excluded if they involved experimental manipulation of coping and/or emotion regulation (e.g., intervention studies). However, if pre-intervention tests of the association between coping and/or emotion regulation with symptoms of internalizing or externalizing psychopathology were reported, these were included in the meta-analysis.
Table 3.
Description of studies included in the current meta-analysis.
| Study | Sample Size | Coping/ER Measure(s) Used | Coping or ER | Measure of Psychopathology | Age Group | Coping /ER Measure Validity | Informant | Study Design |
|---|---|---|---|---|---|---|---|---|
| Abela et al., (2002) | Sample 1: 130; Sample 2: 184 | CRSQ | Coping | CDI; HSC | Child and Adolescent | No | Single | Cross-sectional |
| Abela et al., (2004) | Sample 1: 70; Sample 2: 190 | CRSQ | Coping | CDI | Child and Adolescent | No | Single | Cross-sectional |
| Abela et al., (2007) | 140 | CRSQ | Coping | CDI | Child | No | Single | Cross-sectional and Longitudinal |
| Adams, Abela, & Hankin (2007) | 392 | CRSQ | Coping | CDI | Adolescent | No | Single | Cross-sectional |
| Adrian, Zeman, Erdley, Lisa, Homan, & Sim (2009) | 140 | ERC; DERS | ER | CBCL; YSR | Adolescent | Yes | Single and Multiple | Cross-sectional |
| Ahmed, Kia-Keating, & Tsai (2011) | 240 | Brief RCOPE | Coping | YSR; STAI; CES-D | Adolescent | No | Single | Cross-sectional |
| Amone-P’Olak, Garnefski, & Kraaij (2007) | 294 | CERQ | ER | IES-R; YSR | Adolescent | No | Single | Cross-sectional |
| Auerbach, Abela, Zhu, & Yao (2007) | 411 | RSQ | Coping | RBQ-A | Adolescent | Yes | Single | Cross-sectional |
| Auerbach et al. (2010) | 150 | RSQ | Coping | CES-D; MASC | Adolescent | Yes | Single | Cross-sectional |
| Bachanas, Kullgren, Suzman Schwartz, Lanier, McDaniel, Smith, & Nesheim (2001) | 36 | Coping Strategies Inventory | Coping | BASC; CBCL | Child | Yes | Single and Multiple | Cross-sectional |
| Bal, Crombez, De Bourdeaudhuij, & Van Oost (2009) | 100 | HICUPS | Coping | TSCC | Adolescent | Yes | Single | Cross-sectional |
| Bal, De Bourdeaudhuij, Crombez, & Van Oost (2005) | 65 | HICUPS | Coping | TSCC | Adolescent | Yes | Single | Longitudinal |
| Bal, Van Oost, De Bourdeaudhuij, & Crombez (2003) | 970 | HICUPS | Coping | TSCC | Adolescent | Yes | Single | Cross-sectional |
| Batum & Yagmurlu (2007) | 100 | ERC | ER | ECBI | Child | Yes | Single and Multiple | Cross-sectional |
| Bender, Reinholdt-Dunne, Esbjørn, & Pons (2012) | 544 | DERS | ER | SCARED-R | Adolescent | No | Single | Cross-sectional |
| Bowie (2010) | 126 | CSREE | ER | BASC | Adolescent | No | Single and Multiple | Longitudinal |
| Braun-Lewensohn, Sagy, & Roth (2011) | 135 | ACS | Coping | STAI; Psychosomatic Distress | Adolescent | No | Single | Cross-sectional |
| Brechting & Giancola (2007) | 326 | Wills Coping Questionnaire | Coping | DUSI - Modified | Adolescent | No | Single | Longitudinal |
| Brenning, Soenens, Braet, & Bosmans (2012) | Sample 1: 339; Sample 2: 746 | Emotion Regulation Inventory | ER | CDI | Adolescent | No | Single | Cross-sectional |
| Brumariu, Kerns, & Seibert (2012) | 87 | Children’s Coping Strategies Scale | Coping | SCARED | Adolescent | No | Multiple | Cross-sectional |
| Calvete, Camara, Estevez, & Villardon (2011) | 978 | RSQ | Coping | YSR | Adolescent | Yes | Single | Cross-sectional and Longitudinal |
| Caples & Barrera (2006) | 232 | CCSC | Coping | CDI; YSR; RCMAS; CBCL | Adolescent | Yes | Single and Multiple | Cross-sectional |
| Carlo, Mestre, McGinley, Samper, Tur, & Sandman (2012) | 1557 | ACS | Coping | Caprara & Pastorelli instrument | Adolescent | No | Single | Cross-sectional |
| Carpenter et al. (2012) | 111 | Brief RCOPE | Coping | CDI | Adolescent | No | Single | Cross-sectional and Longitudinal |
| Carthy, Horesh, Apter, Edge, & Gross (2010) | 49 | ERQ | ER | SCARED; CDI; BDI-II | Adolescent | Yes | Single | Cross-sectional |
| Cascone, Zimmermann, Auckenthaler, & Robert-Tissot (2011) | 110 | CASQ | Coping | ASI; STAI-Y | Adolescent | No | Single | Cross-sectional |
| Catanzaro & Laurent (2004) | 210 | COPE | Coping | ABQ | Adolescent | No | Single | Cross-sectional |
| Cicchetti, Rogosch, & Sturge-Apple (2007) | 339 | A-COPE | Coping | DISC | Adolescent | No | Single | Cross-sectional |
| Clark, Novak, & Dupree (2002) | 70 | A-COPE | Coping | AXS | Adolescent | No | Single | Cross-sectional |
| Compas, Boyer, Stanger, Colletti, Thomsen, Dufton, & Cole (2006) | 164 | RSQ | Coping | YSR; CBCL | Adolescent | Yes | Single and Multiple | Cross-sectional |
| d’Acremon & van der Linden (2007) | 110 | CERQ | ER | RADS | Adolescent | No | Single | Cross-sectional |
| Dahlbeck & Lightsey (2008) | 39 | CODI | Coping | STAIC | Adolescent | No | Single | Cross-sectional |
| Dalton & Pakenham (2002) | 78 | ACS | Coping | YSR; BSI | Adolescent | No | Single | Cross-sectional |
| Davies, Forman, Rasi, & Stevens (2002) | 924 | SIS | ER | YSR; CBCL | Adolescent | Yes | Single and Multiple | Cross-sectional |
| Davis & Humphrey (2012) | 748 | CCSC-R1 | Coping | BYI II | Adolescent | Yes | Single | Cross-sectional |
| Dempsey (2002) | 120 | Coping in the Home and School Environments | Coping | Checklist of Children’s Distress Symptoms; STAIC | Adolescent | No | Single | Cross-sectional |
| Downey, Johnston, Hansen, Birney, & Stough (2010) | 145 | ACS | Coping | YSR | Adolescent | No | Single | Cross-sectional |
| Dufton, Dunn, Slosky, & Compas (2011) | Sample 1: 42; Sample 2: 21 | RSQ | Coping | CBCL; YSR | Adolescent | Yes | Single and Multiple | Cross-sectional |
| Duncombe, Havighurst, Holland, & Frankling (2012) | 373 | ERC | ER | SDQ | Child | Yes | Single and Multiple | Cross-sectional |
| Durakovic-Belko et al. (2003) | 393 | WOC | Coping | Depression Self-Rating Scale | Adolescent | No | Single | Cross-sectional |
| Eccleston, Crombez, Scotford, Clinch, & Connell (2004) | 75 | PCQ | Coping | SCAS, CDI | Adolescent | No | Single | Cross-sectional |
| Edlynn, Gaylord-Harden, Richards, & Miller (2008) | 240 | Children’s Integrated Stress and Coping Scale | Coping | STAIC, CBCL | Adolescent | No | Single and Multiple | Cross-sectional |
| Elgar, Arlett, & Groves (2003) | Sample 1: 100; Sample 2: 146 | WOC-R | Coping | YSR | Adolescent | No | Single | Cross-sectional |
| Endriga, Jordan, & Speltz (2003) | 68 | Assessment of Emotion SelfRegulation | ER | CBCL | Child | No | Multiple | Longitudinal |
| Erath, Flanagan, & Bierman (2007) | 84 | Coping Strategies Interview | Coping | SAS-A | Adolescent | No | Single | Cross-sectional |
| Erdem & Slesnick (2010) | 140 | CISS-A | Coping | BDI-II | Adolescent | No | Single | Cross-sectional |
| Erdur-Baker (2009) | 250 | Problem Solving Inventory, Form-A | Coping | CDI | Adolescent | No | Single | Cross-sectional |
| Eschenbeck, Heim-Dreger, Tasdaban, Lohaus, & Kohlmann (2012) | 473 | SSKJ 3–8 | Coping | SSKJ 3–8; SDQ | Adolescent | No | Single | Cross-sectional |
| Escobar, Fernandez-Baena, Miranda, Trianes, & Cowie (2011) | 392 | ACS - Short form | Coping | BASC | Child | No | Single | Cross-sectional |
| Farrell, Bettencourt, Mays, Kramer, Sullivan, & Kliewer (2012) | 477 | CAMS, ERCT | ER | PBFS-Y; CBCL | Adolescent | No | Single | Cross-sectional |
| Fear, Champion, Reeslund, Forehand, Colletti, Roberts, & Compas (2009) | 108 | RSQ | Coping | CBCL; YSR | Adolescent | Yes | Multiple | Cross-sectional |
| Feng, Keenan, Hipwell, Henneberger, Rischall, Butch, … Babinski (2009) | 225 | CSMS; CAMS | ER | KSADS-PL | Child | No | Multiple | Cross-sectional and Longitudinal |
| Flanagan, Vanden Hoek, Ranter, & Reich (2012) | 616 | Coping measure by Kochenderfer-Ladd (2004) | Coping | Social Anxiety Scale for Adolescents | Adolescent | No | Single | Cross-sectional |
| Flanders, Simard, Paquette, Parent, Vitaro, Pihl, & Seguin (2010) | 34 | ERC | ER | NLSCY | Child | Yes | Single | Cross-sectional |
| Flannery et al. (2003) | 3691 | Coping Measure created for study | Coping | VBQ | Adolescent | No | Single | Cross-sectional |
| Flett, Druckman, Hewitt, & Wekerle (2012) | 58 | The Coping Measure | Coping | CES-D | Adolescent | No | Single | Cross-sectional |
| Flynn & Rudolph (2007) | 510 | RSQ | Coping | CDI | Adolescent | Yes | Single | Cross-sectional |
| Flynn & Rudolph (2010) | 345 | RSQ - Modified | Coping | SMFQ | Child | Yes | Single | Cross-sectional |
| Forns, Amador, Kirchner, Gomez, Muro, & Martorell (2005) | 1401 | CRI-Y | Coping | YSR | Adolescent | No | Single | Cross-sectional |
| Forns, Balluerka, Gomez-Benito, Kirchner, & Amador (2010) | 447 | CRI-Y | Coping | YSR | Adolescent | No | Single | Cross-sectional |
| Fredland, Campbell, & Han (2008) | 309 | A-COPE - modified | Coping | Pediatric Symptom Checklist | Adolescent | No | Single | Cross-sectional |
| Gardner, Archer, & Jackson (2012) | 113 | CSQ-3 | Coping | RPAQ | Adolescent | No | Single | Cross-sectional |
| Garnefski & Kraaij (2006) | Sample 1: 597; Sample 2: 1164 | CERQ | ER | SCL-90 | Adolescent | No | Single | Cross-sectional |
| Garnefski, Boon, & Kraaij (2003) | 129 | CERQ | Coping | SCL-90 | Adolescent | No | Single | Cross-sectional |
| Garnefski, Kraaij, & van Etten (2005) | 271 | CERQ | ER | YSR | Adolescent | No | Single | Cross-sectional |
| Garnefski, Legerstee, Kraaij, van den Kommer, & Teerds (2002) | 487 | CERQ | Coping | SCL-90 | Adolescent | No | Single | Cross-sectional |
| Garnefski, Rieffe, Jellesma, Meerum Terwogt, & Kraaij (2007) | 717 | CERQ-k | ER | FSSC-R; CDI | Child | No | Single | Cross-sectional |
| Gaylord-Harden (2008) | 235 | CCSC-R1 | Coping | BASC-TRS | Child | Yes | Multiple | Cross-sectional |
| Gaylord-Harden, Elmore, Campbell, & Wethington (2011) | 278 | HICUPS | Coping | RCMAS; CDI | Child | Yes | Multiple | Cross-sectional |
| Gaylord-Harden, Gipson, Mance, & Grant (2008) | 498 | CCSC | Coping | YSR | Adolescent | Yes | Single | Cross-sectional |
| Gaylord-Harden, Taylor, Campbell, Kesselring, & Grant (2009) | 393 | CCSC | Coping | CDI | Adolescent | Yes | Single | Cross-sectional |
| Gentzler, Santucci, Kovacs, & Fox (2009) | 65 | Feelings and My Child | ER | CBCL, K-SADS | Child | No | Multiple | Cross-sectional |
| Gold, Mahrer, Treadwell, Weissman, & Vichinsky (2008) | 41 | Kidcope | Coping | CBCL | Adolescent | No | Multiple | Cross-sectional |
| Gonzales, Tein, Sandler, & Friedman (2001) | 445 | CCSC | Coping | CDI; Youth Self-Report Hostility Scale | Adolescent | Yes | Single | Cross-sectional |
| Gould, Hussong, & Hersh (2012) | 75 | A-COPE | Coping | SMFQ; RCMAS | Adolescent | No | Multiple | Cross-sectional |
| Gratz, Tull, Reynolds, Bagge, Latzman, Daughters, & Lejuez (2009) | 263 | ERC | ER | RCADS | Adolescent | Yes | Multiple | Cross-sectional |
| Graziano, Reavis, Keane, & Calkins (2007) | 325 | ERC | ER | BASC | Child | Yes | Single | Cross-sectional |
| Grootenhuis & Last (2001) | 84 | CCSS-c | Coping | DQC | Adolescent | No | Single | Cross-sectional |
| Gullone & Taffe (2012) | 827 | ERQ-CA | ER | CDI | Adolescent | Yes | Single | Cross-sectional |
| Hadd & Crocker (2007) | 125 | CFQ | Coping | PANAS | Adolescent | No | Single | Cross-sectional |
| Hampel & Petermann (2006) | 286 | SVF-KJ | Coping | RAASI | Adolescent | No | Single | Cross-sectional |
| Hasking (2006) | 199 | ACS | Coping | EAT-26; AusAUDIT | Adolescent | No | Single | Cross-sectional |
| Hasking (2007) | 259 | ACS | Coping | Self-Reported Delinquency Scale | Adolescent | No | Single | Cross-sectional |
| Hasking, Scheier, & ben Abdallah (2011) | 548 | Brief COPE | Coping | BSI | Adolescent | No | Single | Cross-sectional |
| Hebert, Parent, & Daignault (2007) | Sample 1: 121; Sample 2: 57 | SRCS-S | Coping | CBCL | Child | No | Multiple | Cross-sectional |
| Hebert, Tremblay, Parent, Daignault, & Piche (2006) | 63 | SRCS - Modified | Coping | CBCL | Child | No | Multiple | Cross-sectional |
| Hermann, Hohmeister, Zohsel, Ebinger, & Flor (2007) | 401 | PRCQ-C | Coping | SDQ | Child and Adolescent | No | Multiple | Cross-sectional |
| Hilt et al. (2010) | 722 | CRSQ | Coping | CDI | Adolescent | No | Single | Cross-sectional |
| Hocking, Barnes, Shaw, Lochman, Madan-Swain, & Saeed (2011) | 44 | RSQ | Coping | MASC-10; BASC-2 | Adolescent | Yes | Single and Multiple | Cross-sectional |
| Holen, Lervag, Waaktaar, & Ystgaard (2012) | 1323 | Kidcope | Coping | SDQ | Child | No | Multiple | Cross-sectional |
| Horwitz, Hill, & King (2011) | 140 | Brief COPE | Coping | RADS-2:SF | Adolescent | No | Single | Cross-sectional |
| Hourigan, Goodman, & Southam-Gerow (2011) | 61 | CAMS; CWMS | ER | RCADS; CBCL | Child | No | Multiple | Cross-sectional |
| Hsieh & Stright (2012) | 438 | ERQ | ER | Social Skills Improvement System | Adolescent | Yes | Single and Multiple | Cross-sectional |
| Hudek-Knezevic, Kardum, & Maglica (2005) | 794 | Coping Inventory for Adolescents - short version | Coping | PILL | Adolescent | No | Single | Cross-sectional |
| Ireland, Boustead, & Ireland (2005) | 95 | CSQ-3 | Coping | GHQ-28 | Adolescent | No | Single | Cross-sectional |
| Jacob, Morelen, Suveg, Jacobsen, & Whiteside (2012) | 57 | ERC | ER | CPRS-R:S | Child | Yes | Single | Cross-sectional |
| Jaser, Champion, Dharamsi, Riesing, & Compas (2011) | 72 | RSQ | Coping | CBCL; IFIRS | Adolescent | Yes | Multiple | Cross-sectional |
| Jaser, Champion, Reeslund, Keller, Merchant, Benson, & Compas (2007) | 73 | RSQ | Coping | YSR | Adolescent | Yes | Single and Multiple | Cross-sectional |
| Jaser, Langrock, Keller, Merchant, Benson, Reeslund, … & Compas (2005) | 78 | RSQ | Coping | CBCL; YSR | Adolescent | Yes | Single and Multiple | Cross-sectional |
| Jose & Huntsinger (2005) | 113 | ACES | Coping | CES-D; SelfPerception Profile for Adolescent; Somatic Complaints and Academic Anxiety from Crystal et al. (1994) | Adolescent | No | Single | Cross-sectional |
| Jose & Schurer (2010) | 566 | Coping Strategies Scale | Coping | CDI; RCMAS; Psychosomatic Self-Esteem | Adolescent | No | Single | Cross-sectional |
| Kaczynski, Simons, & Claar (2011) | 280 | PRI | Coping | CSI | Adolescent | Yes | Single | Cross-sectional |
| Kaminsky, Robertson, & Dewey (2006) | 50 | PRI | Coping | CDI | Adolescent | Yes | Single | Cross-sectional |
| Keogh & Eccleston (2006) | 161 | PCQ | Coping | SCAS, CDI | Adolescent | No | Single | Cross-sectional |
| Kim & Cicchetti (2010) | 421 | ERC | ER | TRF | Child | Yes | Single | Cross-sectional |
| Kim & Kim (2007) | 1908 | CSCY | Coping | “Child Self-Report Aggressive Behavior” | Adolescent | No | Single | Cross-sectional |
| Kim et al., (2012) | 1957 | MHQKA | Coping | Child Psychiatry Symptoms; Zung Self-Rating Anxiety Scales | Adolescent | No | Single | Cross-sectional |
| Kochenderfer-Ladd & Skinner (2002) | 356 | SRCS | Coping | TRF | Child | No | Multiple | Cross-sectional |
| Langrock, Compas, Keller, Merchant, & Copeland (2002) | 101 | RSQ | Coping | CBCL | Adolescent | Yes | Single | Cross-sectional |
| Larsen, Vermulst, Eisinga, English, Gross, Hofman, … Engels (2012) | 2,051 | ERQ | ER | CES-D | Adolescent | Yes | Single | Cross-sectional |
| Legault, Anawati, & Flynn (2006) | 220 | Coping Scale by Flynn & Legault (2002) | Coping | NILSCY | Adolescent | No | Single | Cross-sectional |
| Lengua & Long (2002) | 101 | CCSC | Coping | CBCL; YSR | Child | Yes | Multiple | Cross-sectional |
| Lewis, Byrd, & Ollendick (2012) | 709 | HICUPS | Coping | MASC | Adolescent | Yes | Single | Cross-sectional |
| Li, DiGiuseppe, & Froh (2006) | 246 | ACS | Coping | RADS | Adolescent | No | Single | Cross-sectional |
| Libby & Glenwick (2010) | 57 | CSQ-C | Coping | CDI-S | Adolescent | No | Single | Cross-sectional |
| Lim, Stormshak, & Falkenstein (2011) | 102 | LECI | Coping | OHTS | Adolescent | No | Single | Cross-sectional |
| Lima, Guerra, & de Lemos (2010) | 89 | SCSI | Coping | CBCL | Child | No | Multiple | Cross-sectional |
| Liu, Gonzales, Fernandez, Millsap, & Dumka (2011) | 189 | CCSC-R2 | Coping | YSR; CBCL | Adolescent | Yes | Single and Multiple | Cross-sectional and Longitudinal |
| Liu & Huang (2012) | 613 | CWCQ | Coping | STAI; CDI | Adolescent | No | Single | Cross-sectional |
| Lougheed & Hollenstein (2012) | 177 | DERS; ERQ | ER | BAI; BDI-II; SAS-A short form | Adolescent | No | Single | Cross-sectional |
| Lunkenheimer, Shields, & Cortina (2007) | 87 | ERC | ER | CBCL; TRF | Child | Yes | Single and Multiple | Cross-sectional |
| Martyn-Nemeth, Penckofer, Gulanick, Velsor-Friedrich, & Bryant (2009) | 102 | CASQ | Coping | Kandel Depressive Mood Scale | Adolescent | No | Single | Cross-sectional |
| Maurice-Stam, Oort, Last, Brons, Caron, & Grootenhuis (2009) | 27 | CCSS | Coping | ZBV-K | Child | No | Single | Longitudinal |
| Mavroveli, Petrides, Rieffe, & Bakker (2007) | 282 | UCL-A | Coping | CDI; SCL | Adolescent | No | Single | Cross-sectional |
| Maxwell & Cole (2012) | 830 | RSQ; BICSI | Coping | CDI; EDDS | Adolescent | Yes and No | Single | Cross-sectional |
| Maybery, Steer, Reupert, & Goodyear (2009) | 701 | KCS | Coping | SDQ | Child | No | Multiple | Cross-sectional |
| McKee, Jones, Roland, Coffelt, Rakow, & Forehand (2007) | 108 | SCSI | Coping | CDI | Child | No | Single | Cross-sectional |
| McMahon & Watts (2002) | 209 | CCSC | Coping | RCMAS | Adolescent | Yes | Single | Cross-sectional |
| Miers, Rieffe, Terwogt, Cowan, & Linden (2007) | 692 | BARQ-C | Coping | SCL | Adolescent | No | Single | Cross-sectional |
| Miller, Vannatta, Compas, Vasey, McGoron, Salley, & Gerhardt (2009) | 75 | RSQ | Coping | CBCL | Child | Yes | Single | Cross-sectional |
| Molock, Puri, Matlin, & Barksdale (2006) | 212 | RCS | Coping | RADS | Adolescent | No | Single | Cross-sectional |
| Monopoli & Kingston (2012) | 67 | ERC | ER | BASC-2 | Child | Yes | Single | Cross-sectional |
| Morris & Age (2009) | 65 | CCSC-R1 | Coping | SDQ | Adolescent | Yes | Single | Cross-sectional |
| Mosher & Prelow (2007) | 243 | CCSC - Modified | Coping | CES-D—Brief Version | Adolescent | Yes | Single | Cross-sectional |
| Murdock, Greene, Adams, Hartmann, Bittinger, & Will (2010) | 45 | Problem-solving skills (Schmidt & Dubow, 1998) | Coping | BASC | Child | No | Single | Cross-sectional |
| Muris, Mayer, Reinders, & Wesenhagen (2011) | 376 | UCL-A | Coping | PQY; YSR | Adolescent | No | Single | Cross-sectional |
| Muris, Schmidt, Lambrichs, & Meesters (2001) | 373 | UCL-A | Coping | CDI | Adolescent | No | Single | Cross-sectional |
| Muris et al., (2004) | 337 | CRSS | Coping | CDI; SCARED | Adolescent | No | Single | Cross-sectional |
| Ng, Ang, & Ho (2012) | 719 | CRI | Coping | BDI-II; STAI; AQ-Short; TAXI-modified | Adolescent | No | Single | Cross-sectional |
| Nicolotti, El-Sheikh, & Whitson (2003) | 89 | CCSC | Coping | CDI; RCMAS; CBCL | Child | Yes | Multiple | Cross-sectional |
| Ollendick, Langley, Jones, & Kephart (2001) | 99 | HICUPS | Coping | FSSC-R | Adolescent | Yes | Single | Cross-sectional |
| Orsmond, Kuo, & Seltzer (2009) | 56 | COPE | Coping | CES-D | Adolescent | No | Single | Cross-sectional |
| Penza-Clyve & Zeman (2002) | 208 | EESC | ER | STAIC; CDI; CSI | Child | No | Single | Longitudinal |
| Phillips & Power (2007) | 225 | CREQ | ER | SDQ | Adolescent | No | Multiple | Cross-sectional |
| Piko (2001) | 1039 | WOCQ | Coping | Modified Langner Index | Adolescent | No | Single | Cross-sectional |
| Prakash & Coplan (2003) | 40 | CISS | Coping | HBSC; Competitive State Anxiety Inventory | Adolescent | No | Single | Cross-sectional |
| Pina, Villalta, Ortiz, Gottschall, Costa, & Weems (2008) | 46 | CCSC | Coping | PTSD checklist, RCADS | Adolescent | Yes | Single | Cross-sectional |
| Raviv & Wadsworth (2010) | 24 | RSQ | Coping | CBCL; RCMAS; RCDS | Child | Yes | Single | Cross-sectional |
| Rawana & Ahola Kohut (2012) | 311 | CERQ | Coping | K-SPAQ; MASC-R; CES-D | Adolescent | No | Single | Cross-sectional |
| Reschly, Huebner, Appleton, & Antaramian (2008) | 293 | SRCS | Coping | PANAS-C | Adolescent | No | Single | Cross-sectional |
| Rhoades, McIntosh, Wadsworth, Ahlkvist, Burwell, Gudmundsen, … & Rea (2007) | 154 | RSQ | Coping | RADS; STAIC; UCLA | Adolescent | Yes | Multiple | Cross-sectional |
| Rieffe, Oosterveld, Miers, Terwogt, & Ly (2008) | 665 | EAQ-30 | ER | SAS-A, CDI, SCL | Adolescent | No | Single | Cross-sectional |
| Roelofs et al. (2009) | 770 | CRSS | Coping | SCARED | Adolescent | No | Single | Cross-sectional |
| Rudolph & Troop-Gordon (2010) | 167 | RSQ | Coping | K-SADS-E-5 | Adolescent | Yes | Multiple | Cross-sectional and Longitudinal |
| Sandstrom (2004) | 95 | SCORE | Coping | CDI; SASC-R; CBCL | Child | No | Single | Cross-sectional |
| Schiff (2006) | 600 | COPE | Coping | CES-D; CPTSRI; SRQ | Adolescent | No | Single | Cross-sectional |
| Schneider & Phares (2005) | 60 | HICUPS | Coping | CBCL; CDI | Adolescent | Yes | Single and Multiple | Cross-sectional |
| Seiffge-Krenke & Stemmler (2002) | 115 | CASQ | Coping | YSR | Adolescent | No | Single | Cross-sectional |
| Šerek, Lacinová, & Macek (2012) | 444 | Coping Strategies Inventory - Modified | Coping | Mood and Feelings Questionnaire | Adolescent | No | Single | Cross-sectional |
| Shelton & Harold (2007) | 100 | Children’s Coping Strategies | Coping | CDI; YSR | Adolescent | No | Single | Cross-sectional |
| Shelton & Harold (2008) | 252 | SIS | Coping | TRF; CDI; YSR | Adolescent | Yes | Single and Multiple | Cross-sectional |
| Shirkey, Smith, & Walker (2011) | 116 | PRI | Coping | CDI | Child | Yes and No | Single | Longitudinal |
| Siener & Kerns (2012) | 87 | The Coping Questionnaire | Coping | CDI-S | Adolescent | No | Multiple | Cross-sectional |
| Siffert & Schwarz (2011) | 192 | FEEL-JK | ER | SCAS; CES-D; Self-Report Somatic Problems List; RCPM; SDQ | Child | No | Single | Cross-sectional |
| Sim & Zeman (2006) | 234 | CEMS | ER | EDI-BD; EAT-26 | Adolescent | No | Single | Cross-sectional |
| Simons, Claar, & Logan (2008) | 217 | PRI | Coping | CSI | Adolescent | Yes | Single | Cross-sectional |
| Skočić, Rudan, Brajković, & Marčinko (2010) | 101 | SCS | Coping | YSR | Adolescent | No | Single | Cross-sectional |
| Smith, Eisenberg, Spinrad, Chassin, Morris, Kupfer, … Kwok (2006) | 293 | CCSC-R1 | Coping | CBCL; Anxiety Scale; Teacher Report Index of Depression | Child | Yes | Multiple | Cross-sectional |
| Song et al. (2012) | 586 | ERSI | ER | Intensity Time Affect Scale | Adolescent | No | Single | Cross-sectional |
| Sontag, Graber, Brooks-Gunn, & Warren (2008) | 111 | RSQ | Coping | YSR | Adolescent | Yes | Single | Cross-sectional |
| Steele, Legerski, Nelson, & Phipps (2009) | 803 | AESC | ER | ChIA; CMHS; BASC-PRF; CHI | Adolescent | No | Single and Multiple | Cross-sectional |
| Sullivan, Helms, Kliewer, & Goodman (2010) | 358 | CAMS; CSMS | ER | Risk Behavior Survey; Measure of Relational Aggression | Adolescent | No | Single | Cross-sectional |
| Sung, Puskar, & Sereika (2006) | 72 | CRI-Y | Coping | RADS; SCARED | Adolescent | No | Single | Cross-sectional |
| Suveg, Shaffer, Morelen, & Thomassin (2011) | 97 | ERC; CSMS; CAMS; CWMS | ER | CBCL | Child | No | Single | Cross-sectional |
| Tam & Lam (2005) | 993 | CASQ | Coping | CDI; ABQ | Adolescent | No | Single | Cross-sectional |
| Tam (2008) | 1116 | CASQ | Coping | CDI; ABQ | Adolescent | No | Single | Cross-sectional |
| Thompson, Mata, Jaeggi, Buschkuehl, Jonides, & Gotlib (2010) | 149 | RSQ | Coping | CDI | Adolescent | Yes | Single | Cross-sectional |
| Thomsen, Compas, Colletti, Stanger, Boyer, & Konik (2002) | 190 | RSQ | Coping | CBCL | Adolescent | Yes | Single | Cross-sectional |
| Thuen & Bru (2004) | 2006 | COPE | Coping | Hopkins Symptom Checklist | Adolescent | No | Single | Cross-sectional |
| Tompkins, Hockett, Abraibesh, & Witt (2011) | 146 | RSQ | Coping | YSR; TRF | Adolescent | Yes | Single and Multiple | Cross-sectional |
| van Dijk, Grootenhuis, Imhof, Cohen-Kettenis, Moll, & Huisman (2009) | 31 | CISS | Coping | YSR | Adolescent | No | Single | Cross-sectional |
| Van Dyke, Glenwick, Cecero, & Kim (2009) | 76 | Brief RCOPE | Coping | PANAS-C; BSI-18 | Adolescent | No | Single | Cross-sectional |
| Vasilev, Crowell, Beauchaine, Mead, & Gatzke-Kopp (2009) | 165 | DERS | ER | YSR; CDI; CBCL; CSI | Adolescent | No | Single and Multiple | Cross-sectional |
| Vaughn & Roesch (2003) | 182 | COPE | Coping | BDI | Adolescent | No | Single | Cross-sectional |
| Vigna, Hernandez, Kelley, & Gresham (2010) | 261 | Kidcope | Coping | BASC-2 | Child | No | Single | Cross-sectional |
| Visconti & Troop-Gordon (2010) | 420 | SRCS - Modified | Coping | RCMAS; CES-D; Multi-Informant Peer Victimization Inventory - Modified | Child | No | Single and Multiple | Cross-sectional and Longitudinal |
| Votta & Manion (2003) | 100 | COPE | Coping | YSR; BDI | Adolescent | No | Single | Cross-sectional |
| Votta & Manion (2004) | 100 | COPE | Coping | YSR; BDI | Adolescent | No | Single | Cross-sectional |
| Vulic-Prtoric & Macuka (2006) | 331 | SUO | Coping | SKAD-62; SDD | Adolescent | No | Single | Cross-sectional |
| Wadsworth & Berger (2006) | 79 | RSQ | Coping | YSR | Adolescent | Yes | Single | Longitudinal |
| Wadsworth & Compas (2002) | 364 | RSQ | Coping | YSR | Adolescent | Yes | Single | Cross-sectional |
| Wadsworth & Santiago (2008) | 164 | RSQ | Coping | YSR; CBCL | Adolescent | Yes | Multiple | Cross-sectional |
| Wadsworth, Raviv, Compas, & Connor-Smith (2005) | 57 | RSQ | Coping | YSR; CBCL | Adolescent | Yes | Multiple | Cross-sectional |
| Wadsworth, Rieckmann, Benson, & Compas (2004) | 332 | RSQ | Coping | MMPI-A; CDI | Adolescent | Yes | Single | Cross-sectional |
| Wagner, Ferguson, & Smith (2012) | 80 | Kidcope; CHIC | Coping | CDI | Adolescent | No | Single and Multiple | Cross-sectional |
| Walker, Smith, Garber, & Claar (2005) | 133 | PRI | Coping | CSI; CDI | Child | Yes | Single | Cross-sectional |
| Walker, Smith, Garber, & Claar (2007) | 247 | PRI | Coping | CSI; CDI | Child | Yes | Single | Longitudinal |
| Wang & Gan (2011) | 460 | COPE | Coping | Zung | Adolescent | No | Single | Cross-sectional |
| Weinberg & Klonsky (2009) | 428 | DERS | ER | PHQ-A | Adolescent | No | Single | Cross-sectional |
| Wills, Sandy, & Yaeger (2002) | 1699 | Intention-Based Inventory | Coping | Substance Problems Inventory | Adolescent | No | Single | Cross-sectional |
| Wills, Sandy, Yaeger, Cleary, & Shinar (2001) | Sample 1: 1702; Sample 2: 1827; Sample 3: 1895 | Child Intention-Based Assessment | Coping | Adolescent Substance Use | Adolescent | No | Single | Cross-sectional |
| Wilson, Pritchard, & Revalee (2005) | 542 | Brief COPE | Coping | POMS | Adolescent | No | Single | Cross-sectional |
| Wolfradt, Hempel, & Miles (2003) | 276 | Coping questionnaire by Seiffge-Krenke (1989) | Coping | STAI | Adolescent | No | Single | Cross-sectional |
| Wright, Banerjee, Hoek, Rieffe, & Novin (2010) | 270 | SRCS - Modified | Coping | Social Anxiety Scale for Children - Revised; CDI-S | Child | No | Single | Cross-sectional |
| Wu, Chin, Chen, Lai, & Tseng (2011) | 229 | PCCS | Coping | RCMAS-2 | Adolescent | No | Single | Cross-sectional |
| Xiao, Yao, Zhu, Zhang, Auerbach, McWhinnie, & Abela (2010) | 1068 | RSQ | Coping | SAS-SCS | Adolescent | Yes | Single | Cross-sectional |
| Zaremba & Keiley (2011) | 62 | ERC | ER | YSR | Adolescent | Yes | Single | Cross-sectional |
| Zehnder, Prchal, Vollrath, & Landolt (2006) | 119 | HICUPS | Coping | Child PTSD RI; CBCL | Child | Yes | Multiple | Longitudinal |
| Zeidner (2005) | 227 | COPE | Coping | Dundee Stress State Questionnaire; Personal Stress Symptom Assessment; EMAS; Post-Traumatic Reaction Scale | Adolescent | No | Single | Cross-sectional |
| Zeman, Cassano, Suveg, & Shipman (2010) | 214 | CWMS | ER | CBCL, ADIS-IV | Child | No | Multiple | Cross-sectional |
| Zeman, Shipman, & Penza-Clyve (2001) | 227 | CSMS | “Emotion Regulation Coping” | STAIC; CDI; CBCL | Child | No | Single and Multiple | Cross-sectional |
| Zhou et al. (2012) | 867 | SCSQ | Coping | CMSSLSS | Adolescent | No | Single | Cross-sectional |
Note. A-COPE = Adolescent Coping Orientation for Problem Experiences; ABQ = Alcohol Behavior Questionnaire; ACES = Adolescent Coping Efforts Scale; ACS = Adolescent Coping Scale; ADIS-IV = Anxiety Disorder Interview Schedule for Children-Fourth Edition-Child/Parent Versions; AESC = Anger Expression Scale for Children; ASI = Addiction Severity Index; AusAUDIT = Australian Alcohol Use Disorders Identification Test; AXS = State-Trait Anger Expression Inventory; BAI = Beck Anxiety Inventory; BARQ-C = Behavioral Anger Response Questionnaire; BASC = Behavior Assessment System for Children; BASC-2 = Behavioral Assessment System for Children-Second Edition; BASC-PRF = Behavior Assessment Scale for Children-Parent Report Form; BASC-TRS = The Behavior Assessment Scale for Children - Teacher Rating Scales; BDI = Beck Depression Inventory; BDI-II = Beck Depression Inventory-II; BICSI = Body Image Coping Strategies Inventory; Brief RCOPE = Brief Religious Coping Measure; BSI = Brief Symptom Inventory; BSI-18 = Brief Symptom Inventory; BYI II = Beck Youth Inventories of Emotional and Social Impairment, Second Edition; CAMS = Children’s Anger Management Scales; CASQ = Coping Across Situations Questionnaire; CBCL = Child Behavior Checklist; CCSC = Children’s Coping Strategies Checklist; CCSC-R1 = The Children’s Coping Strategies Checklist - Revision 1; CCSC-R2 = Children’s Coping Strategies Checklist-2nd Revision; CCSS = Cognitive Control Strategies Scale; CCSS-c = Cognitive Control Strategy Scale for Children; CDI = Children’s Depression Inventory; CDI-S = Children’s Depression Inventory-Short Form; CEMS = Children’s Emotion Management Scales; CERQ = Cognitive Emotion Regulation Questionnaire; CERQ-k = Cognitive Emotion Regulation Questionnaire; CES-D = The Center for Epidemiologic Studies Depression Scale; CES-D—Brief Version = The Center for Epidemiologic Studies Depression Scale—Brief Version; CFQ = Coping Function Questionnaire; CHI = Children’s Hostility Inventory; ChIA = Children’s Inventory of Anger; CHIC = Coping Health Inventory for Children; CISS = Coping Inventory for Stressful Situations; CISS-A = Coping Inventory for Stressful Situations-Adolescent version; CMHS = Cook-Medley Hostility Scale, children’s version; CMSSLSS = China Multi-dimensional Life Satisfaction Scale for adolescents; CODI = Coping with a Disease; COPE = Cope Inventory; CPRS-R:S = Connor’s Parent Rating Scale-Revised - Short Version; CPTSRI = Child Post-Traumatic Stress Reaction Index; CRI = Coping Responses Inventory; CRI-Y = Coping Response Inventory - Youth Form; CRSQ = Children’s Response Styles Questionnaire; CSCY = Coping Scale for Children and Youth; CSI = Children’s Somatization Inventory; CSMS = Children’s Sadness Management Scales; CSQ-3 = Coping Styles Questionnaire; CSQ-C = Coping Strategies Questionnaire - Child version; CSREE = Child Self-Report of Emotional Experience; CWCQ = Chinese Ways of Coping Questionnaire; CWMS = Children’s Worry Management Scale; DERS = Difficulties with Emotion Regulation Scale; DISC = Diagnostic Interview Schedule for Children; DQC = Depression Questionnaire for Children; DUSI = Drug Use Screening Inventory; EAQ-30 = Emotion Awareness Questionnaire; EAT = Eating Attitudes Test; EAT-26 = Eating Attitudes Test-26; ECBI = Eyberg Child Behavior Inventory; EDDS = Eating Disorder Diagnostic Scale; EDI-BD = Eating Disorder Inventory-Body Dissatisfaction Scale; EESC = Emotional Expression Scale for Children; EMAS = Endler’s Multidimensional Anxiety Scale; ERC = Emotion Regulation Checklist; ERCT = Emotion Regulation Checklist; ERQ = Emotion Regulation Questionnaire; ERQ-CA = Emotion Regulation Questionnaire for Children and Adolescents; FEEL-KJ = Fragebogen zur Erhebung der ER bei Kindern und Jugendlichen; FSSC-R = Revised Fear Survey Schedule for Children; GHQ-28 = General Health Questionnaire; HICUPS = How I Cope Under Pressure Scale; HSC = Hopelessness Scale for Children; IES-R = Impact of Event Scale-Revised; IFIRS = Iowa Family Interaction Rating Scales; K-SADS = ‘Kiddie’ Schedule for Affective Disorders and Schizophrenia; K-SADS-E-5 = Schedule for Affective Disorders and Schizophrenia for School-Age Children - Epidemiologic Version 5; K-SPAQ = Kiddie Seasonal Pattern Assessment Questionnaire; KCS = Kids Coping Scale; KSADS-PL = Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children—Present/Lifetime Version; LECI = Life Events and Coping Inventory; MASC = Multidimensional Anxiety Scales for Children; MASC-10 = Multidimensional Anxiety Scale for Children - 10-item form; MHQKA = Mental Health Questionnaire for Korean Adolescents; MMPI-A = Minnesota Multiphasic Personality Inventory - Adolescent Version; NLSCY = National Longitudinal Study of Children and Youth Behavior Questionnaire; OHTS = Oregon Healthy Teens Survey; PANAS = Positive and Negative Affects Schedule; PANAS-C = Positive and Negative Affect Schedule for Children; PBFS-Y = Problem Behavior Frequency Scale—youth report; PCCS = Paediatric Cancer Coping Scale; PCQ = The Pain Coping Questionnaire; PHQ-A = Patient Health Questionnaire - Adolescent; PILL = Pennebaker Inventory of Limbic Languidness; POMS = Profile of Mood States; PQY = Psychopathology Questionnaire for Youths; PRCQ-C = Pain-Related Cognitions Questionnaire for Children; PRI = Pain Response Inventory for Children; RAASI = Reynolds Adolescent Adjustment Screening Inventory; RADS = The Reynolds Adolescent Depression Scale; RADS-2:SF = Reynolds Adolescent Depression Scale 2nd Edition, Short Form; RBQ-A = Risky Behavior Questionnaire for Adolescents; RCADS = Revised Child Anxiety and Depression Scale; RCDS = Reynolds Child Depression Scale; RCMAS = Revised Children’s Manifest Anxiety Scale; RCMAS-2 = Revised Children’s Manifest Anxiety Scale, Second Edition; RCPM = Revised Class Play Method; RCS = Religious Coping Scale; RI = Frederick Reaction Index; RPAQ = Reactive-Proactive Aggression Questionnaire; RSQ = Responses to Stress Questionnaire; SAS-A = Social Anxiety Scale for Adolescents; SAS-A short form = Social Anxiety Scale for Adolescents - short form; SAS-SCS = Social Anxiety Subscale of the Self-Consciousness Scale; SASC-R = Social Anxiety Scale for Children - Revised; SCARED = Screen for Child Anxiety Related Emotional Disorders; SCARED-R = Screen for Child Anxiety Related Emotional Disorders-Revised; SCAS = Spence Children’s Anxiety Scale; SCL = Somatic Complaint List; SCL-90 = Symptom Check List; SCORE = Survey for Coping with Rejection Experiences; SCS = Scale of Coping with Stress; SCSI = Schoolagers’ Coping Strategies Inventory; SCSQ = Simplified Coping Style Questionnaire; SDD = Depression Scale for Children and Adolescents; SDQ = Strengths and Difficulties Questionnaire; SIS = Security in the Interparental Subsystem Scale; SKAD-62 = Fear and Anxiety Scale for Children and Adolescents; SMFQ = Short form of the Mood and Feelings Questionnaire; SRCS = Self-Report Coping Scale; SRCS-S = Self-Report Coping Scale Short Form; SRQ = Stress Reaction Questionnaire; SSKJ 3–8 = Stress and Coping Questionnaire for Children and Adolescents; STAI = State Trait Anxiety Inventory; STAI-Y = State-Trait Anxiety Inventory for Youth; STAIC = State Trait Anxiety Inventory for Children; SUO = Coping Strategies Inventory for Children and Adolescents; SVF-KJ = German Coping Questionnaire for Children and Adolescents; TAXI-modified = State-Trait Anger Expression Inventory; TRF = Child Behavior Profile - Teacher Report Form; TSCC = Trauma Symptom Checklist for Children; UCL-A = Adolescent version of the Utrecht Coping List; UCLA = UCLA Reaction Index; WOC-R = Ways of Coping Scale - Revised; WOCQ = Ways of Coping Questionnaire; YSR = Youth Self Report; ZBV-K = Dutch version of the State-Trait Inventory for Children.
Data Coding Procedure
A standard procedure was used to structure the coding process. Each study was coded for the measure of coping and/or emotion regulation, the measure of internalizing and/or externalizing psychopathology, including scale reliabilities, sample size, and the statistics describing the relationship between coping or emotion regulation and psychopathology. We also recorded descriptive information, including year of publication and the country where the study was conducted. Studies using modified versions of validated measures were noted. Each study was independently coded by two of the study authors, and coding discrepancies were resolved through discussion between the authors of the meta-analysis.
As noted above, coping and emotion regulation scales were coded into three levels: domains, factors, and strategies (see Appendix). Each coping and emotion regulation domain, factor, and strategy was independently coded by two of the study authors (89.1% inter-rater reliability), and discrepancies were resolved through discussion. The broad domains of coping and emotion regulation included (1) total coping (e.g., self-coping, unitary coping), (2) emotion regulation (e.g., adaptive affect regulation, sadness regulation, anger management, palliative emotion regulation), (3) emotion dysregulation (e.g., abreacting, dysregulation), (4) adaptive coping (e.g., adaptive coping, positive coping, productive coping), and (5) maladaptive coping (e.g., dysfunctional coping, helpless coping, negative coping, nonproductive coping).
Second, we identified intermediate factors of coping and emotion regulation that included (1) problem-focused (e.g., problem-directed coping, task-oriented coping), (2) emotion-focused (e.g., emotional engagement, internal coping, emotion-oriented coping), (3) engagement/approach (e.g., active coping, approach coping, behavioral coping), (4) disengagement (e.g., behavioral disengagement, passive coping, detached coping), (5) primary control coping (e.g., primary control coping), (6) secondary control coping (e.g., accommodative coping), and (7) social support coping (e.g., asking for help, developing social support, seeking guidance, support coping).
Finally, specific coping and emotion regulation strategies were categorized into (1) problem solving (e.g., cognitive problem solving, decision making, planning), (2) emotional expression (e.g., expressing feelings, verbal sharing), (3) emotional suppression (e.g., anger inhibition, expressive reluctance, repression), (4) cognitive reappraisal (e.g., minimization, positive reappraisal, rationalization), (5) distraction (e.g., behavioral distraction, entertainment, seeking diversions), (6) acceptance (e.g., rational acceptance, resignation), (7) avoidance (e.g., avoidant activities, cognitive distancing, withdrawal), (8) denial (e.g., blaming others, defensive coping), and (9) wishful thinking (e.g., fantasizing, imagining), (10) emotional modulation (e.g., anger control, relaxation, tension reduction), (11) unregulated release of emotions (e.g., emotional discharge, externalizing negative coping, vent coping), and (12) humor (e.g., humor).
Similarly, the psychopathology measures were coded into categories of dependent variables. Based on the well-validated measures of Achenbach System of Empirically Based Assessment (ASEBA) of behavioral and emotional problems (Achenbach & Rescorla, 2001), the broadband categories of internalizing and externalizing symptoms were used. Internalizing symptoms included measures of depression, anxiety, and somatic complaints, and externalizing symptoms included measures of aggression, conduct problems, and substance use.
All analyses were conducted with the Comprehensive Meta-Analysis program (Borenstein, Hedges, Higgins, & Rothstein, 2005), using random effects models, as the studies varied in methodology and design, using study as the unit of analysis and the mean of the selected outcomes. The mean effect size for each study (r) was used as the level of analysis; therefore, if a single study tested associations between multiple coping strategies or symptoms within the same category, the mean effect size was calculated. Similarly, when authors published different studies using the same sample or a smaller subset of the same sample, a mean effect size was used in analysis. When studies selectively reported only significant associations (e.g., “All other correlations were non-significant”), missing tests were conservatively coded as r = .00. As such, 54 effect sizes were estimated as .00. Excluding these non-significant effect sizes would have biased the meta-analysis, potentially overestimating the mean effect size for the association between coping and emotion regulation and symptoms. We utilized Cohen’s (1988) guidelines to interpret the magnitude of the effect size for significant correlations (i.e., r = .10 as small, .30 as medium, and above .50 as large).
In analyses, we used correlations or mean differences where reported. In line with other recent meta-analyses (e.g., Robles, Slatcher, Trombello, & McGinn, 2014), if the only statistic reported was from a multivariate analysis (standardized β), we converted the β to r using the formula (r = β + .05λ, where λ equals 0 when the β is negative and λ equals 1 when the β is nonnegative) recommended by Peterson and Brown (2005). Effect sizes in meta-analyses based on very small number of studies are subject to problem in data synthesis (Davey, Turner, Clarke, & Higgins, 2011); therefore, we set a threshold of a minimum of five studies (k = 5) to estimate effect sizes for the cross-sectional studies. However, because there were relatively few longitudinal studies (k = 17), we set the threshold at a minimum of three studies (k = 3) to estimate effects for longitudinal analyses.
For each coping and emotion regulation domain, factor, and strategy with internalizing and externalizing psychopathology, weighted mean effect sizes (r), 95% confidence intervals, and estimated a heterogeneity statistic (Q) were calculated using the procedures outlined by Hedges and Olking (1985). The 95% confidence intervals on the effect sizes represent the range in which the mean effect size falls in 95% of cases; the calculation for confidence intervals (lower limit and upper limit) is as follows:
where M* is the mean effect size in the sample, Z is the critical z value representing the confidence level, and VM* is the variance of M* (Borenstein et al., 2005). A mean effect is considered significant when the confidence interval does not include zero. The number of studies (k), total sample size (N), mean effect size (r) and significance value of the effect, 95% confidence interval (95% CI) for the mean effect size, and Q statistic and its significance value are reported for cross-sectional analyses in Table 4 and for longitudinal analyses in the text below.
Table 4.
Cross-sectional effect sizes for coping and emotion regulation and internalizing and externalizing symptoms.
| Internalizing Symptoms | Externalizing Symptoms | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Level I: Domains | k | n | r | 95% CI | Q | k | n | r | 95% CI | Q |
| Total Coping | 12 | 2867 | −.01 | [−.13, .11] | 109.98 | 4 | -- | -- | -- | -- |
| Adaptive Coping | 13 | 3077 | −.04 | [−.16, .08] | 113.87 | 7 | 4949 | −.11 | [−.20, −.02] | 25.41 |
| Maladaptive Coping | 5 | 1266 | .27 | [.18, .36] | 9.05 | 2 | -- | -- | -- | -- |
| Adjusted value | .22 | [.12, .31] | 17.99 | -- | -- | -- | ||||
| Emotion Regulation | 15 | 6437 | −.23+ | [−.34, −.11] | 282.21 | 18 | 7682 | −.27+ | [−.37, −.17] | 337.34 |
| Level II: Factors | K | n | R | 95% CI | Q | k | n | r | 95% CI | Q |
| Problem-Focused | 18 | 6597 | −.07 | [−.14, .00] | 113.83 | 4 | -- | -- | -- | -- |
| Emotion-Focused | 13 | 4728 | .11 | [−.02, .23] | 182.02 | 7 | 3276 | .03 | [−.12, .17] | 55.89 |
| Engagement/Approach | 48 | 17987 | −.07 | [−.14, −.01] | 735.70 | 25 | 21437 | −.04 | [−.09, .01] | 178.07 |
| Adjusted value | −.02 | [−.08, .04] | 1019.11 | -- | -- | -- | ||||
| Disengagement | 29 | 14684 | .18 | [.12, .24] | 360.67 | 7 | 3924 | .13+ | [.04, .22] | 31.92 |
| Primary Control | 20 | 7205 | −.17 | [−.24, −.10] | 154.75 | 6 | 1739 | −.23 | [−.33, −.14] | 15.46 |
| Adjusted value | −.14 | [−.21, −.07] | 170.67 | -- | -- | -- | ||||
| Secondary Control | 23 | 8295 | −.25 | [−.32, −.18] | 226.05 | 6 | 1815 | −.30 | [−.38, −.22] | 13.24 |
| Adjusted value | −.20 | [−.27, −.13] | 319.61 | −.29 | [−.37, −.20] | 15.98 | ||||
| Social Support | 42 | 18599 | .02 | [−.02, .05] | 246.08 | 21 | 14441 | .00 | [−.06, .07] | 239.28 |
| Level III: Strategies | K | n | R | 95% CI | Q | k | n | r | 95% CI | Q |
| Problem-Solving | 45 | 27447 | −.03 | [−.07, .01] | 408.12 | 16 | 10497 | −.02 | [−.08, .03] | 98.05 |
| Emotional Expression | 6 | 2171 | .08 | [−.10, .25] | 78.00 | 2 | -- | -- | -- | -- |
| Emotional Suppression | 10 | 10618 | .13+ | [.03, .22] | 165.15 | 6 | 2150 | .02 | [−.02, .07] | 6.11 |
| Cognitive Reappraisal | 31 | 23541 | −.05 | [−.10, .00] | 356.78 | 10 | 8633 | −.03 | [−.08, .03] | 36.11 |
| Acceptance | 12 | 6686 | .04 | [−.05, .12] | 119.82 | 1 | -- | -- | -- | -- |
| Distraction | 25 | 7950 | −.04 | [−.10, .03] | 189.55 | 11 | 3114 | .06 | [−.02, .14] | 37.55 |
| Avoidance | 65 | 29570 | .17 | [.14, .20] | 458.96 | 32 | 25255 | .09 | [.05, .13] | 271.68 |
| Adjusted value | .16 | [.13, .19] | 496.08 | -- | -- | -- | ||||
| Denial | 12 | 6880 | .10 | [.03, .17] | 80.14 | 2 | -- | -- | -- | -- |
Note: Bolded text indicates the effect size or Q statistic was significant at the p < .05 level.
Indicates the Egger’s test analyses were significant for the effect size. Adjusted values were calculated for any effect size in which the trim and fill analyses indicated significant publication bias. Adjusted values indicate the effect size when the trim and fill procedures are applied.
Moderation.
For cross-sectional analyses, categorical moderator analyses were conducted to determine whether age, measure quality, or informant significantly moderated the associations between coping and emotion regulation and symptoms of psychopathology. A significant Q statistic indicates that there is significant heterogeneity within the studies contributing to the overall effect size, and suggests that there may be moderating variables to consider (Borenstein et al., 2009). As such, for any cross-sectional effect size with a significant Q statistic, we ran analyses to determine whether age, measure quality, or informant significantly moderated associations between coping and emotion regulation and symptoms of psychopathology. Consistent with previous meta-analyses, a minimum of three studies (k = 3) per level of the moderator was required for moderator analyses (e.g., Slaget et al., 2016).
First, we coded the study sample as “child” (mean age 5–10) or “adolescent” (mean age 11–19), using the mean age of each sample. Second, measures were coded as “high quality” if they were based on a conceptual model of coping or emotion regulation and if reliability and convergent or discriminant validity data were reported. Studies were coded as “adequate quality” if the measure used reported only reliability data or minimal information on validity, following criteria for measurement quality described in previous reviews and meta-analyses (e.g., Rueger, Malecki, Pyun, Aycock, & Coyle, 2016; Skinner et al., 2003). Finally, we coded studies as “single informant” if the same respondent completed the measure of coping and emotion regulation and psychopathology. Studies were coded as “multi-informant” if one informant reported on the child’s coping and emotion regulation and another informant reported on child’s symptoms.
In the Comprehensive Meta-Analysis program, associations within studies were treated as non-independent. As such, when a study reported associations for both levels of a moderator variable (e.g., reported effects for the same category of coping/emotion regulation and symptoms for both children and adolescent samples), the effect sizes from the study were not included in the analysis. For both levels of the moderating variable, the number of studies (k), total sample size (N), mean effect size (r), and 95% confidence interval (95% CI) for the mean effect size are reported, in addition to the mixed effects total between groups factor (Qb) and its significance level.
Publication bias.
Several steps were taken to investigate the possibility of publication bias, which occurs as a result of selective publication of research findings based on the direction and size of the results. It is important for meta-analytic studies to assess its presence and impact, because this systematic bias can lead to an inflated effect size estimates and inaccurate conclusions. First, we visually examined the funnel plot for each significant effect size. The funnel plot for an effect size is a plot of the standard error of each study contributing to the overall effect size (a reflection of sample size) on the y-axis with the study’s effect estimate on the x-axis. The effect estimate should be more precise with increasing sample size. As such, in the absence of publication bias, effect estimates from studies with smaller sample sizes should be scattered symmetrically at the bottom of the plot and center more closely around the mean effect estimate at the top of the plot as the sample size increases, which creates a funnel shape. In the presence of publication bias, the plot will appear asymmetrical, suggesting that small samples reporting small to non-significant effect sizes were less likely to be published.
Second, we calculated Egger’s tests to assist in the interpretation of the funnel plots, which is a statistical test used to detect funnel plot asymmetry (Egger et al., 1997). Of note, the Egger’s test has been reported to have lower power when used for associations with fewer than 10 studies (Higgins & Green, 2011).
Third, we conducted trim and fill analyses (Duval & Tweedie, 2000) to determine how many studies would need to be included above or below the meta-analytic mean to make the funnel plot symmetrical. A higher number of studies denotes greater publication bias. Trim and fill analyses also impute the missing studies and calculate adjusted meta-analytic effect sizes that account for publication bias.
Results
Based on the inclusion criteria, a total of 212 studies with 80,850 participants were included in the analyses (see Table 3 for study details). Of the included studies, 24 studies conducted different analyses using the same sample or variants of the same sample. Several studies reported associations separately for subsamples (e.g., boys vs. girls), and some studies reported more than one measure of coping and emotion regulation or psychopathology. The number of associations ranged from 1 to 55 per article, with most articles reporting multiple effect sizes, providing a total of 1,649 effects coded for the meta-analysis. Forty-two studies used measures of emotion regulation, 169 studies used measures of coping, and one study referred to “emotion regulation coping.” Forty-six studies included a child sample, 163 studies included an adolescent sample, and three studies included both child and adolescent samples. Seventy-four studies used measures classified as “high quality”, and 138 studies used measures classified as “adequate quality”. One hundred and fifty-eight studies used reports from single informants, 30 studies used reports from multiple informants, and 24 studies reported both single and multiple informant reports. There were not a sufficient number of studies to calculate cross-sectional (k = 5 or more) or longitudinal (k = 3 or more) effect sizes for emotion modulation, unregulated release of emotions, and humor with internalizing or externalizing symptoms. Therefore, these three strategies are not included in Table 4 and are not presented in the results.
Cross-Sectional Effect Sizes
Effect sizes for the cross-sectional studies of the coping and emotion regulation domains, factors, and strategies and both internalizing and externalizing symptoms are presented in Table 4 and summarized below.
Domains.
Maladaptive coping was significantly positively associated with internalizing symptoms, indicating greater use of maladaptive coping was associated with higher levels of symptoms. A negative effect size was found for adaptive coping and externalizing symptoms, indicating greater use of adaptive coping was associated with lower symptoms. Emotion regulation was significantly negatively associated with both internalizing and externalizing symptoms, such that greater use of emotion regulation was associated with lower levels of symptoms. All other effect sizes for domains of coping and emotion regulation were non-significant or could not be calculated due to too few studies (k < 5) examining that particular domain (see Table 4).
Factors.
Engagement/approach coping was significantly negatively associated with internalizing symptoms, such that greater use of engagement/approach coping was associated with lower symptoms. A significant negative effect size was found for problem-focused coping and externalizing symptoms, indicating greater use of problem-focused coping was associated with lower symptoms. Disengagement coping was significantly positively associated with both internalizing and externalizing symptoms, such that greater use of disengagement coping was related to higher levels of symptoms. Both primary control coping and secondary control coping were significantly negatively associated with symptoms. Thus, greater use of these coping factors was related to lower internalizing and externalizing symptoms. All other effect sizes for factors of coping and emotion regulation were non-significant (see Table 4).
Strategies.
Emotional suppression and denial were significantly positively associated with internalizing symptoms, and avoidance was significantly positively associated with both internalizing and externalizing symptoms. That is, greater use of emotional suppression, denial and avoidance was associated with higher levels of symptoms. All other effect sizes for coping and emotion regulation strategies were non-significant or could not be calculated due to too few studies (k < 5) examining that particular strategy (see Table 4).
Heterogeneity of effect sizes.
For all calculated cross-sectional effects, with the exception of two effect sizes, there was a significant Q statistic (see Table 4). For all cross-sectional associations with a significant Q statistic, we analyzed age, measure quality, and informant as potential moderators. The Q statistic for maladaptive coping and internalizing symptoms and for emotional suppression and externalizing symptoms was not significant, and therefore moderator analyses were not conducted for these associations.
Moderator Analyses
Moderation analyses for the cross-sectional studies of the coping and emotion regulation domains, factors, and strategies are presented in Table 5 and the text below.
Table 5.
Categorical moderator analyses testing mean age (child vs. adolescent), measurement quality (adequate vs. high), and informant (single vs. multiple) as moderators of coping and emotion regulation with internalizing and externalizing symptoms.
| Moderator: Age | ||||||||
|---|---|---|---|---|---|---|---|---|
| Internalizing Symptoms | Externalizing Symptoms | |||||||
| Level I: Domains | Qb | k | r | 95% CI | Qb | k | R | 95% CI |
| Adaptive Coping | .01 | 13 | .34 | 7 | ||||
| Child | 3 | −.05 | [−.39, .31] | 2 | .02 | [−.43, .47] | ||
| Adolescent | 10 | −.03 | [−.15, .10] | 5 | −.12 | [−.23, −.01] | ||
| Emotion Regulation | 2.53 | 15 | 1.26 | 18 | ||||
| Child | 8 | −.30 | [−.44, −.15] | 11 | −.32 | [−.42, −.21] | ||
| Adolescent | 7 | −.13 | [−.27, .01] | 7 | −.20 | [−.38, −.01] | ||
| Level II: Factors | Qb | k | r | 95% CI | Qb | k | r | 95% CI |
| Problem-Focused | .23 | 18 | -- | |||||
| Child | 3 | −.06 | [−.11, .00] | |||||
| Adolescent | 15 | −.08 | [−.17, .01] | |||||
| Engagement/Approach | 7.60* | 48 | .29 | 25 | ||||
| Child | 9 | −.08 | [−.22, .07] | 4 | −.01 | [−.12, .10] | ||
| Adolescent | 38 | −.07 | [−.14, −.00] | 21 | −.04 | [−.09, .01] | ||
| Secondary Control | .02 | 23 | -- | |||||
| Child | 3 | −.24 | [−.49, .06] | |||||
| Adolescent | 20 | −.26 | [−.33, −.18] | |||||
| Social Support Coping | 1.29 | 42 | 1.56 | 21 | ||||
| Child | 9 | −.03 | [−.13, .07] | 5 | −.05 | [−.15, .04] | ||
| Adolescent | 33 | .03 | [−.01, .07] | 16 | .02 | [−.05, .10] | ||
| Level III: Strategies | Qb | k | r | 95% CI | Qb | k | r | 95% CI |
| Problem-Solving | 4.03 | 45 | -- | |||||
| Child | 6 | −.07 | [−.18, .04] | |||||
| Adolescent | 36 | .00 | [−.05, .04] | |||||
| Emotional Suppression | 11.16** | 10 | .46 | 6 | ||||
| Child | 3 | .01 | [−.18, .20] | 3 | .00 | [−.09, .09] | ||
| Adolescent | 6 | .16 | [.03, .28] | 3 | .04 | [−.03, .11] | ||
| Cognitive Reappraisal | 8.53* | 31 | -- | |||||
| Child | 3 | .02 | [−.07, .12] | |||||
| Adolescent | 27 | −.06 | [−.12, .01] | |||||
| Distraction | 2.78 | 25 | -- | |||||
| Child | 3 | .00 | [−.13, .12] | |||||
| Adolescent | 20 | −.01 | [−.03, .01] | |||||
| Avoidance | 2.40 | 65 | .05 | 32 | ||||
| Child | 10 | 8 | .08 | [−.03, .19] | ||||
| Adolescent | 55 | 24 | .10 | [.05, .14] | ||||
| Moderator: Measure Quality | ||||||||
| Internalizing Symptoms | Externalizing Symptoms | |||||||
| Level I: Domains | Qb | K | r | 95% CI | Qb | k | r | 95% CI |
| Adaptive Coping | -- | .26 | 7 | |||||
| Adequate Quality | 5 | −.16 | [−.19, −.14] | |||||
| High Quality | 2 | −.17 | [−.26, −.08] | |||||
| Emotion Regulation | 1.79 | 15 | 2.71 | 18 | ||||
| Adequate Quality | 8 | −.05 | [−.25, −.04] | 7 | −.19 | [−.33, −.03] | ||
| High Quality | 7 | −.34 | [−.50, −.09] | 11 | −.34 | [−.43, −.24] | ||
| Level II: Factors | Qb | k | r | 95% CI | Qb | k | r | 95% CI |
| Engagement/Approach | 1.51 | 48 | .00 | 25 | ||||
| Adequate Quality | 27 | −.11 | [−.18, −.04] | 15 | −.04 | [−.10, .02] | ||
| High Quality | 21 | −.03 | [−.14, .08] | 10 | −.04 | [−.13, .05] | ||
| Disengagement | 0.27 | 29 | -- | |||||
| Adequate Quality | 8 | .21 | [.07, .34] | |||||
| High Quality | 21 | .17 | [.11, .24] | |||||
| Social Support Coping | 0.26 | 42 | 1.56 | 21 | ||||
| Adequate Quality | 31 | .01 | [−.03, .05] | 16 | .02 | [−.05, .10] | ||
| High Quality | 11 | .04 | [−.05, .12] | 5 | −.05 | [−.15, .04] | ||
| Level III: Strategies | Qb | k | r | 95% CI | Qb | k | r | 95% CI |
| Problem-Solving | 2.80 | 45 | 2.29 | 16 | ||||
| Adequate Quality | 41 | −.04 | [−.08, .01] | 12 | −.05 | [−.12, .02] | ||
| High Quality | 4 | .04 | [−.04, .11] | 4 | .07 | [−.07, .21] | ||
| Emotional Suppression | 1.82 | 10 | -- | |||||
| Adequate Quality | 5 | .07 | [−.07, .21] | |||||
| High Quality | 5 | .19 | [.08, .30] | |||||
| Cognitive Reappraisal | 0.15 | 31 | 1.76 | 10 | ||||
| Adequate Quality | 23 | −.04 | [−.09, .01] | 6 | −.06 | [−.13, .02] | ||
| High Quality | 8 | −.07 | [−.22, .08] | 4 | .02 | [−.06, .09] | ||
| Distraction | 3.28 | 25 | .07 | 11 | ||||
| Adequate Quality | 15 | −.08 | [−.15, −.01] | 3 | .08 | [−.17, .32] | ||
| High Quality | 10 | .04 | [−.07, .14] | 8 | .04 | [−.02, .11] | ||
| Avoidance | .06 | 65 | .86 | 32 | ||||
| Adequate Quality | 45 | .17 | [.13, .21] | 18 | .11 | [.05, .16] | ||
| High Quality | 20 | .16 | [.11, .22] | 14 | .07 | [.02, .13] | ||
| Moderator: Informant | ||||||||
| Internalizing Symptoms | Externalizing Symptoms | |||||||
| Level I: Domains | Qb | k | r | 95% CI | Qb | k | r | 95% CI |
| Emotion Regulation | .35 | 15 | .41 | 50 | −.24 | −.29, −.19 | ||
| Single Informant | 5 | −.30 | [−.61, .08] | 25 | −.28 | −.41, −.15 | ||
| Multi-Informant | 6 | −.19 | [−.51, −.06] | 25 | −.24 | −.29, −.18 | ||
| Level II: Factors | Qb | k | r | 95% CI | Qb | k | r | 95% CI |
| Problem-Focused | .20 | 18 | -- | |||||
| Single Informant | 15 | −.07 | [−.15, .01] | |||||
| Multi-Informant | 3 | −.11 | [−.26, .05] | |||||
| Engagement/Approach | 3.23 | 48 | .02 | 39 | −.04 | −.08, .00 | ||
| Single Informant | 38 | −.06 | [−.13, .00] | 33 | −.04 | −.08, .00 | ||
| Multi-Informant | 7 | −.18 | [−.30, −.05] | 6 | −.04 | −.12, .05 | ||
| Disengagement | .81 | 29 | -- | |||||
| Single Informant | 19 | .20 | [.12, .28] | |||||
| Multi-Informant | 3 | .15 | [.05, .24] | |||||
| Social Support Coping | 1.89 | 42 | 5.26* | 38 | .02 | −.02, .07 | ||
| Single Informant | 34 | .02 | [−.02, .06] | 25 | .07 | .01, .12 | ||
| Multi-Informant | 6 | −.05 | [−.15, .05] | 13 | −.04 | −.11, .03 | ||
| Level III: Strategies | Qb | k | r | 95% CI | Qb | k | r | 95% CI |
| Problem-Solving | 1.33 | 45 | 5.18 | 16 | ||||
| Single Informant | 40 | −.03 | [−.07, .02] | 12 | −.06 | [−.12, −.01] | ||
| Multi-Informant | 3 | −.10 | [−.27, .08] | 3 | .12 | [−.11, .34] | ||
| Cognitive Reappraisal | 1.33 | 31 | 1.83 | |||||
| Single Informant | 25 | −.04 | [−.10, .02] | 7 | −.05 | [−.11, −.02] | ||
| Multi-Informant | 3 | 3 | .03 | [−.06, .12] | ||||
| Distraction | -- | .36 | 11 | |||||
| Single Informant | 7 | .09 | [.05, .17] | |||||
| Multi-Informant | 4 | .02 | [−.09, .14] | |||||
| Avoidance | 3.20 | 65 | .41 | 32 | ||||
| Single Informant | 49 | .17 | [.13, .21] | 18 | .10 | [.04, .15] | ||
| Multi-Informant | 10 | .13 | [.09, .18] | 11 | .07 | [−.01, .16] | ||
Note. Total coping, maladaptive coping, emotion dysregulation, emotion-focused coping, disengagement coping, emotional expression, and denial did not have enough studies in both categories (child and adolescent) to test age as a moderator of the overall effect. Total coping, maladaptive coping, emotion dysregulation, emotion-focused coping, primary control coping, secondary control coping, emotional expression, acceptance, and denial did not have enough studies in both categories (adequate and high quality) to test measure quality as a moderator of the overall effect. Total coping, adaptive coping, maladaptive coping, emotion-focused coping, primary control coping, secondary control coping, emotion expression, emotion suppression, acceptance, and denial did not have enough studies in both categories (single and multi-informant) to test informant as a moderator of the overall effect.
Age.
At the domain level, there were no significant moderating effects of age for the domains of adaptive coping or emotion regulation (see Table 5).
Among factors of coping and emotion regulation, age was a significant moderator for the association between engagement/approach coping and internalizing symptoms. Specifically, there was a significant negative association between engagement/approach coping and internalizing symptoms for adolescents, but not children. However, age was not a significant moderator of the relationship between engagement/approach coping and externalizing symptoms. All other effect sizes that could be estimated at the factor level of coping and emotion regulation with age as a moderator were non-significant (see Table 5).
For strategies of coping and emotion regulation, age was a significant moderator of the association between cognitive reappraisal and internalizing symptoms such that the association was larger for adolescents than for children. A significant moderating effect for age was also found for emotional suppression and internalizing symptoms, indicating this association was significant for adolescent samples but not child samples. All other effects of coping and emotion regulation strategies that could be estimated with age as a moderator were non-significant (see Table 5).
Measure quality.
There were no significant moderating effects of measure quality for domains, factors or strategies of coping and emotion regulation (see Table 5).
Informant.
For domains, factors, and strategies of coping and emotion regulation, informant for measures of coping and symptoms yielded no significant moderator effects (see Table 5).
Longitudinal Effect Sizes
As noted above, given the small number of longitudinal studies (k = 17; sample sizes ranged from n = 68 to 1,444) in the current meta-analysis, we calculated effects for any domain, factor, or strategy that had three or more studies contributing to the effect size.
Domains.
At the domain level, only one effect size could be calculated. Emotion regulation was not significantly associated with internalizing symptoms (k = 3, r = −.08, p = .52, 95% CI [−. −.37, .22]).
Factors.
Seven effect sizes could be calculated for factors of coping and emotion regulation, and two were significant. Disengagement coping (k = 4, r = .18, p = .01, 95% CI [.04, .31]) and social support coping (k = 4, r = .12, p < .001, 95% CI [.05, .18]) were significantly positively associated with internalizing symptoms. That is, greater use of disengagement coping and social support coping was associated with higher levels of internalizing symptoms. However, social support coping was not significantly associated with externalizing symptoms (k = 4, r = −.02, p = .72, 95% CI [−.12, .09]). Primary control coping (k = 3, r = −.07, p = .58, CI [−.29, .16]) and secondary control coping (k = 5, r = −.00, p = .90, CI [−.07, .07]) were not significantly associated with internalizing symptoms. Further, engagement/approach coping was not associated with internalizing symptoms (k = 9, r = −.02, p = .76, 95% CI [−.16, .12]) or externalizing symptoms (k = 5, r = .05, p = .20, 95% CI [−.03, .12]).
Strategies.
Four effect sizes could be calculated for coping and emotion regulation strategies, and one was significant. Avoidance was significantly positively associated with internalizing symptoms (k = 6, r = .08, p = .003, 95% CI [.03, .13]), such that greater use of avoidance was associated with higher internalizing symptoms. However, avoidance was not significantly associated with externalizing symptoms (k = 4, r = .04, p = .62, 95% CI [−.12, .19]). In addition, distraction was not significantly associated with either internalizing (k = 4, r = −.02, p = .55, 95% CI [−.11, .06]) or externalizing (k = 3, r = .02, p = .60, 95% CI [−.06, .10]) symptoms.
Heterogeneity of effect sizes.
For longitudinal associations, all but four effect sizes had a significant Q statistic. The Q statistic for the association between emotion regulation, engagement/approach coping, disengagement coping, and primary control coping with internalizing symptoms was significant. In addition, the Q statistic for the association between avoidance and social support with externalizing symptoms was significant. As such, there was significant heterogeneity within the studies contributing to these overall effect sizes. However, due to the small number of studies contributing to these effect sizes, we did not analyze potential moderators of these relationships.
Publication Bias
Of the 16 significant cross-sectional effect sizes, four effect sizes produced significant Egger’s tests, and of the three significant longitudinal effect sizes, none of these effect sizes produced significant Egger’s tests. First, at the domain level, the Egger’s test for the cross-sectional association between emotion regulation and internalizing symptoms (k = 15, regression intercept = −5.03, 95% CI [−9.62, −0.44]) as well as externalizing symptoms (k = 18, regression intercept = −4.63, 95% CI [−8.85, −0.41]) was significant. Second, at the factor level, the Egger’s test for the cross-sectional association between disengagement coping and externalizing symptoms (k = 7, regression intercept = −3.50, 95% CI [−6.30, −0.69]) was significant. Finally, at the strategy level, there was a significant Egger’s test for the cross-sectional association between emotional suppression and internalizing symptoms (k = 10, regression intercept = −6.91, 95% CI [−10.18, −3.64]).
The funnel plots for the four effect sizes with significant Egger’s tests are presented separately in Figure 2. A visual inspection of these plots shows data asymmetry for these effect estimates, suggesting that they may be affected by publication bias. It is noteworthy that data asymmetry was not evident in the other 12 significant cross-sectional effect estimates or the three longitudinal effect estimates.
Figure 2a-2d.
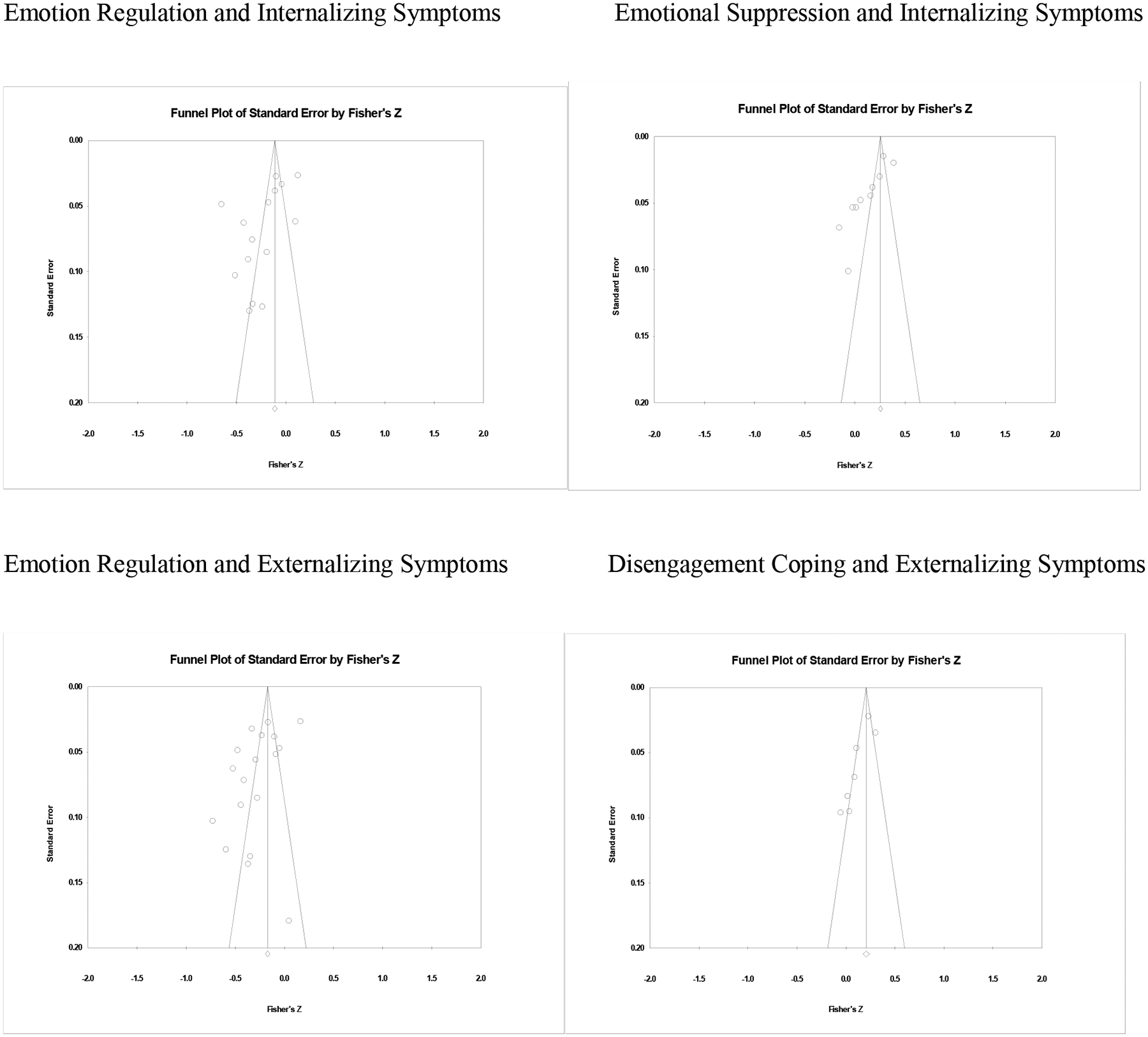
Funnel plots for the relationship between the standard error and Fisher’s Z in cross-sectional studies of coping and emotion regulation and symptoms of psychopathology.
As a third step, we conducted trim and fill analyses for all significant meta-analytic effect sizes. The results of the trim and fill analyses are presented as adjusted effect sizes in Table 4. Of the 16 significant cross-sectional effect sizes, six effect sizes required values to be added to create a symmetrical funnel plot. Of these six effect sizes, five remained significant. Notably, all five significant adjusted effect sizes were smaller in magnitude as a result of the trim and fill analyses. The effect size for the association between engagement coping and internalizing symptoms was no longer significant as a result of the trim and fill analyses.
For the longitudinal analyses, the effect size for the association between disengagement coping and internalizing symptoms had no values that needed to be added as a result of the trim and fill analyses. Two longitudinal effect sizes required values to be added to create a symmetrical funnel plot. Of these two effect sizes, the effect size for the association between social support and internalizing symptoms remained significant, and the effect size for the association between avoidance and internalizing symptoms was no longer significant.
Discussion
Coping and emotion regulation play central roles in models of risk and resilience for psychopathology in children and adolescents. In spite of the importance of these constructs, there has been no comprehensive quantitative meta-analysis of their association with internalizing and externalizing symptoms in childhood and adolescence. The primary goal of this meta-analysis is to address this gap and determine if there is evidence for an association of domains, factors, and strategies of coping and emotion regulation with internalizing and externalizing symptoms of psychopathology. The results of the meta-analysis lead to an answer of a qualified yes. Evidence of publication bias was found in both the cross-sectional and longitudinal analyses, yet clear evidence was found for significant associations between coping and emotion regulation and symptoms of internalizing and externalizing psychopathology, as the majority of findings remained significant after adjusting for publication bias. However, progress in the field has become stagnant with regard to both conceptualization and methodology. We summarize the findings from our meta-analysis as a benchmark of the current state of the field, followed by a critique and a proposed agenda for improving our understanding of coping and emotion regulation in children and adolescents.
Meta-analytic Findings
The current meta-analysis drew on a large body of evidence from 212 studies with 80,850 participants. Significant findings were found for associations between specific domains, factors and strategies of coping and emotion regulation with internalizing and externalizing symptoms of psychopathology in cross-sectional studies. Tests of three possible moderators (age, measure quality, single vs. multiple informant) yielded relatively few significant moderation effects. Further, substantially fewer significant effect sizes were found in longitudinal studies as compared to cross-sectional studies.
Publication bias.
All publication bias methods have limitations and no one approach is fully accurate; therefore, we have included multiple approaches to considering publication bias to help better approximate accurate estimations of effect sizes in the literature to date. Evidence was found for the possible influence of publication bias in both the cross-sectional and longitudinal findings. Four of the 16 significant cross-sectional effects had a significant Egger’s test, although none of the three significant longitudinal effects had significant Egger’s tests. Inspection of the funnel plots associated with the four significant Egger’s tests suggested possible publication bias in cross-sectional analyses. Further, the trim and fill analyses indicated publication bias for six of the 16 cross-sectional effect sizes. However, only one cross-sectional effect size was no longer significant in the adjusted analyses. Trim and fill analyses indicated publication bias in two of the three significant longitudinal effects, and one of these longitudinal effect sizes was no longer significant in the adjusted analyses. Taken together, the overall pattern found in the unadjusted analyses was retained in the adjusted effect sizes. However, because we focused only on published studies we cannot rule out possible additional effects of publication bias on the findings in the current meta-analysis.
Cross-sectional studies.
At the domain level, significant effect sizes ranged from small to medium in magnitude (unadjusted and adjusted ranged from r = −.11 to .27). Significant medium negative associations were found for the broad domain of emotion regulation with both internalizing and externalizing symptoms and a small significant negative association was found for the broad domain of adaptive coping with externalizing symptoms. Conversely, a significant medium positive association was found between maladaptive coping and internalizing symptoms. These findings are important in providing the first quantitative evidence that broad measures of both coping and emotion regulation are associated with symptoms of psychopathology in children and adolescents.
However, a closer examination of the items included in the broad domains of coping and emotion regulation suggests that they provide relatively limited information about what children and adolescents do to regulate their emotions or cope with stress. For example, the emotion regulation subscale of the ERC (Shields & Cicchetti, 1997) includes items such as, “Displays appropriate negative emotions in response to hostile, aggressive, or intrusive acts by peers;” “Transitions well from one activity to another; does not become anxious, angry, distressed, or overly excited when moving from one activity to another;” and “Is able to delay gratification.” Similarly, the emotion regulation coping subscale from the CEMS (e.g., Zeman, Shipman, & Penza-Clyve, 2011; Zeman et al., 2010) includes: “I keep myself from losing control of my worried/angry/sad feelings;” “I try to calmly settle the problem when I feel worried/mad/sad.” These items reflect descriptions of the degree to which children are able to regulate their emotions but do not include information about the strategies used to achieve regulation. We discuss this limitation in more detail below when we consider findings from the meta-analysis at the level of intermediate factors and specific strategies. Further, findings on the use of maladaptive coping are largely tautological. That is, if coping and emotion regulation are labeled a priori as maladaptive or dysregulated then it is circular to show that these strategies are related to higher levels of symptoms of psychopathology. Therefore, we suggest that researchers discontinue the use of measures that label coping and emotion regulation as adaptive or maladaptive on an a priori basis in favor of measures that provide more detailed descriptions of factors or strategies that are used to cope with stress and regulate emotions.
We found evidence that intermediate factors of coping and emotion regulation are associated with both internalizing and externalizing symptoms. The general factor of engagement/approach coping had small but significant negative associations with internalizing symptoms; however, this effect was no longer significant after adjusting for possible publication bias. Disengagement coping had small significant positive associations with both internalizing and externalizing symptoms. The most consistent factor-level evidence was found for primary control coping and secondary control coping, both of which were significantly negatively associated with both internalizing and externalizing symptoms with the effect sizes ranging from small to medium in magnitude (unadjusted and adjusted effect sizes ranged from r = −.14 to −.30). These findings suggest that the control-based model that includes primary and secondary control coping has promise for understanding types of coping that are related to lower levels of symptoms (Compas et al., 2012, 2014a). At the time of the last comprehensive review of coping in children and adolescents (Compas et al., 2001), problem-focused and emotion-focused coping were the most commonly studied factors. Therefore it is noteworthy that in the current meta-analysis, problem-focused coping had only a small negative association with internalizing symptoms and neither of the effect sizes for emotion-focused coping was significant. It appears that problem-focused and emotion-focused coping have played a smaller role in research on coping in children and adolescents in the past decade and may have been supplanted at the factor level by primary control and secondary control coping, both in terms of the frequency that they are studied and the magnitude of effects they produce. Finally, social support coping continues to be widely studied, yet, despite having enough studies to calculate effect sizes, we found no significant associations between social support and symptoms of psychopathology. While these findings suggest that using social support may not be an effective means of coping or regulating emotions for children and adolescents, it is also plausible that measures of social support may not be capturing the way that social networks are used by children and adolescents to cope with stress and regulate emotions (see Rueger et al., 2016, for a meta-analysis of available and enacted social support and depressive symptoms in adolescence).
It is important to note that, although there are no emotion regulation measures that are categorized at the factor level, emotion regulation strategies are embedded within factors derived from coping measures. For example, primary control coping includes problem solving, emotional expression, and emotional modulation; secondary control coping includes cognitive reappraisal, distraction, and acceptance; and disengagement coping includes avoidance and wishful thinking (Connor-Smith et al., 2000). All of these strategies are also included in studies of emotion regulation (Aldao et al., 2010; Gross & Jazaieri, 2014; Sheppes, Suri, & Goss, 2015). Thus, findings regarding coping factors also provide indirect support for emotion regulation factors and highlight the somewhat artificial distinctions between these constructs in terms of current approaches to measurement. We return to this issue in our proposed directions for future research.
In spite of the hope that measures of specific strategies would yield a more detailed and nuanced picture of the association of coping and emotion regulation with symptoms, there was relatively little evidence at the level of strategies. Small but significant positive associations with symptoms were found for emotional suppression, avoidance, and denial. However, none of the other 11 effect sizes that could be estimated were significant. These findings differ from those reported by Aldao et al. (2010) and Schäfer et al. (2017) which found significant associations between specific strategies (e.g., avoidance, acceptance) and symptoms of psychopathology. This discrepancy may be due in part to differences in measurement; while the studies included in the current meta-analysis included reports of how children and adolescents coped with or regulated specific stressors or emotions, the studies included in the reviews by both Aldao and Schafer focused on dispositional or “habitual” use of strategies, or how individuals typically respond to stressors.
Overall this pattern of findings presents a challenge for the field. The limited findings for measures assessing specific strategies of coping and emotion regulation may reflect problems in the quality of these measures (e.g., a limited number of items in these scales). Alternatively, this may suggest that examining specific strategies in isolation may provide only a partial picture of the ways that individuals use multiple strategies to regulate their emotions and cope with stress. That is, effective coping and emotion regulation may require a repertoire of skills that can be used flexibly in response to different emotions or stressors (e.g., Aldao, Sheppes, & Gross, 2015; Cheng, Lau, & Chen, 2014). The most consistent effect sizes in the current meta-analysis were found for measures that aggregate coping and emotion regulation strategies into intermediate-level factors. This level of analysis may capture cohesive factors of coping and emotion regulation strategies that are often used together and provide a more complete picture of how these strategies function in relation to symptoms of psychopathology. For example, the effect sizes for cognitive reappraisal and acceptance were not significant but the use of secondary control coping, which includes these two strategies along with distraction, was significantly associated with fewer symptoms.
In spite of the potential benefits that may accrue from analyses of coping and emotion regulation strategies that have been aggregated into factors, a limitation of studying these processes at the factor level is the lack of information about specific strategies that may be carrying the effects and the relative use of different strategies that are included within these factors. An important step for future research is to unpack these factors to examine the associations of more comprehensive measures that include larger samples of items reflecting the specific coping and emotion regulation strategies that comprise them. That is, improvement is needed in the quality of measures of specific strategies that can be used in various combinations to understand which of a given set of strategies may have the strongest effects. For example, the RSQ (Connor-Smith et al., 2000) includes only three items to assess each of four strategies that make up secondary control coping (acceptance, cognitive reappraisal, positive thinking, distraction). Analyses of parcels that include a larger number of items for each strategy could yield more information about how the strategies that comprise secondary control coping are used flexibly in different combinations and how these patterns are related to psychopathology. As discussed below, this will also require research designs that are more sensitive to processes of coping and emotion regulation as they unfold during specific events or periods of time.
Moderator analyses of cross-sectional studies.
We examined three possible moderators of the cross-sectional associations between coping and emotion regulation and symptoms of psychopathology: age, measure quality, and informant. First, analyses of age as moderator yielded a significant effect size for the association of engagement/approach coping with internalizing symptoms, with a small but significant negative effect size for adolescents and a non-significant effect for children. There was also an effect for age as a moderator of cognitive reappraisal and internalizing symptoms with a small negative association for adolescents and a small positive association for children. Finally, age was moderator of the association of emotional suppression and internalizing symptoms; there was a significant positive association for adolescents while the association for children was non-significant. Although these findings do not support a clear developmental pattern for the association of coping and emotion regulation with symptoms, results are similar to those reported in previous reviews. Aldao et al. (2010) evaluated the role of age group (children and adolescents vs. adults) and found a significant moderating effect for age on the association of problem solving and suppression with symptoms of psychopathology such that the association was stronger for adults than children and adolescents. Similarly, Cheng et al. (2014) compared effect sizes for participants under age 30 (including a small number of studies with adolescents) and over age 30 and reported a significantly larger effect size for the association of coping flexibility and measures of psychological adjustment for older than younger participants. However, it is important to note that given relatively small numbers of studies in each category for some analyses, there may not have been sufficient power to detect age as a moderator in the current meta-analysis.
Consistent with developmental models of coping and emotion regulation (e.g., Zimmer-Gembeck & Skinner, 2016), the few significant age effects in the present met-analysis indicate a stronger association between coping and emotion regulation strategies with internalizing symptoms for adolescents as compared with children. However, the majority of the tests of age as a moderator of effect sizes were non-significant. While reviews of the development of coping and emotion regulation suggest more frequent use of cognitively demanding strategies, such as secondary control coping, in adolescents as compared to children (e.g., Skinner & Zimmer-Gembeck, 2007; Zimmer-Gembeck & Skinner, 2011, 2016), it is still unknown whether the use of these strategies is more adaptive in adolescents as compared to children. Further, the current meta-analysis indicates few differences in associations among coping and emotion regulation and symptoms related to age. It is important to note, however, that the wide variation in samples made it difficult to conduct clear comparisons by age, as the mean age of the study sample was used to code the sample as child or adolescent. For example, a study with an age range of 8–18 years may be coded as an “adolescent” sample if the mean age was above 11, as would a study with an age range of 15–17. These necessary approximations of age may have obscured findings related to development. Notably, in a recent meta-analysis by Schäfer and colleagues (2017), age was not a significant moderator of the association between emotion regulation and symptoms of depression and anxiety in adolescents. We return to the importance of understanding developmental differences in coping and emotion regulation in the agenda for future research presented below.
There was no evidence that the association of coping and emotion regulation with symptoms was affected by measure quality. The absence of significant effects for measure quality suggests that the findings are not compromised by the psychometric quality of the measures of coping and emotion regulation that were included in this review. This may be a consequence of our requirement that authors reported at least some reliability data or that reliability data be reported for the measure elsewhere in the literature, and that each scale have more than two items to be included in the current review. In addition, as noted above, we may have also had low power to detect measure quality as a moderator.
Finally, no significant moderator effects were identified for studies that used a single informant to assess coping and emotion with symptoms as compared with studies that examined effects using different informants for each construct (e.g., children and their parents). This provides some evidence that the association of coping and emotion regulation with symptoms is not simply an artifact of shared method variance that can be the consequence of obtaining self-reports of both of these constructs (Compas et al., 2014b). However, these findings should be viewed with caution as we identified relatively fewer studies that used multi-informant reports compared to those that used single-informant designs, resulting in relatively low statistical power. Further, multi-informant analyses provide the most stringent test of the association of coping and emotion regulation with symptoms of psychopathology and continue to be the method of choice (see below).
Longitudinal studies.
The evidence for the association of coping and emotion regulation with internalizing and externalizing symptoms was not supported in longitudinal studies. Specifically, only disengagement coping, social support coping, and avoidance were significantly positively associated with internalizing symptoms in longitudinal analyses (effect sizes ranged from r = .12 to .18). Thus, there is substantially less evidence for the association of coping and emotion regulation with symptoms of psychopathology in longitudinal as compared with cross-sectional studies. Several factors may have contributed to these diminished effect sizes. First, there were only 17 studies with longitudinal data that could be included in the meta-analysis, yielding a smaller body of evidence to evaluate these associations. Second, it is possible that the only longitudinal associations between coping and emotion regulation and symptoms are for those factors or strategies that are related to higher levels of symptoms over time. In contrast, factors that are associated with lower levels of symptoms (e.g., primary control coping and secondary control coping) may only be correlates of symptoms when measured at the same point in time, as evidenced by the consistent cross-sectional findings in the current meta-analysis for these factors, and may not be associated with symptoms longitudinally. We consider the implications of these findings in greater detail below.
Comparison with Previous Reviews
The pattern and magnitude of the findings in the current meta-analysis can be evaluated in part through comparison with previous meta-analyses of the association of coping and emotion regulation with symptoms of psychopathology. First, previous meta-analyses examining coping and emotion regulation and symptoms in children and adolescents found only small effects for these associations (Aldridge & Roesch, 2007; Clarke, 2006). The effect sizes reported in the current meta-analysis provide substantially stronger support for the association of coping and emotion regulation with symptoms of psychopathology than either of these two previous meta-analyses focused on research with children and adolescents. Further, compared with these previous meta-analyses with children and adolescents, the current study found much clearer and stronger evidence for associations between coping and emotion regulation factors (i.e., primary control coping and secondary control coping) and lower levels of symptoms (i.e., effect sizes that are reflected in negative correlations).
Several other meta-analyses have included only a small portion of studies with children or adolescents along with a much larger number of studies with adults. For example, a recent meta-analysis examined the association of coping flexibility in adults with psychological adjustment, and found that coping flexibility was positively associated with better adjustment (overall effect size r = .23) and the overall association between coping flexibility and psychological adjustment was moderated by individualism, SES, and age (Cheng, Lau, & Chen, 2014). In addition, Rueger et al. (2016) found a significant positive association between social support coping and depressive symptoms (overall effect size r = .26). Aldao et al. (2010) reported a meta-analysis of associations between emotion regulation strategies and symptoms of psychopathology in studies with primarily adult samples. Significant medium positive effect sizes were found for avoidance, rumination, and suppression and significant negative effect sizes were found for reappraisal and problem solving with symptoms of psychopathology (i.e., anxiety, depression, disordered eating, and substance use). Similarly, Schäfer et al. (2017) reported significant medium negative effect sizes for cognitive reappraisal, problem solving, and acceptance, and significant positive effect sizes for avoidance, suppression, and rumination) with symptoms of anxiety and depression in adolescence. The results of the current meta-analysis found associations of similar magnitude as these previous meta-analyses, while extending these findings specifically to children and adolescents and including studies of both coping and emotion regulation. Thus, the findings of the current study are in line with and expand on those of previous meta-analyses of coping and emotion regulation.
Limitations of Previous Research
In spite of the significance of these findings, research on coping and emotion regulation in children and adolescents is constrained by two fundamental limitations. First, there is a continued overreliance on the use of questionnaires to assess these processes. Although questionnaires can provide important information on the ways that children and adolescents cope with stress and regulate their emotions in their daily lives, the limitations of questionnaires to assess coping and emotion regulation are well documented. Some limitations of questionnaire measures of coping and emotion regulation include reliance on retrospective reports and concerns about accuracy of recall (particularly with children and adolescents), confounding of items with their outcomes, and variations in the recall period across different measures (Folkman & Moskowitz, 2004). As outlined in greater detail below, rather than simply recommending against the use of questionnaires to assess coping and emotion regulation, we believe questionnaires must be augmented by other methods that can provide more objective evidence for the strategies children and adolescents use to cope with stress and regulate their emotions. Second, the majority of studies included in the current meta-analysis were cross-sectional and single informant. The direction of the associations of coping and emotion regulation with symptoms cannot be determined when both are measured at a single, contemporaneous time point. Although this design remains useful as an initial step in addressing new or novel research questions, it cannot be the focus for advances in this area of research. Further, by relying on a single source of information for both coping and emotion regulation and symptoms, this level of evidence may be confounded by shared method variance. Notably, it is encouraging that the moderator analyses of informant effects were not significant, suggesting that the findings were not limited to the use of single informants. However, in some cases there were small numbers of studies contributing to the moderator analyses, and therefore these analyses may have been limited by low statistical power. Despite this limitation, it is important that the field uses the most rigorous designs possible to test the association of coping and emotion regulation with symptoms of psychopathology.
An Agenda for Future Research
The clearest conclusion that can be drawn from this meta-analysis is that questionnaire measures of coping and emotion regulation are associated with questionnaire measures of internalizing and externalizing symptoms in children and adolescents. Although these findings provide an important foundation for this field, the aim of future research on these constructs cannot be limited to showing these simple associations using a limited set of methods. We now outline an agenda for next steps in research on coping, emotion regulation and psychopathology in children and adolescents. We draw extensively on reviews of constructs that are closely related to coping and emotion regulation, including effortful control, executive function, and cognitive factors in child and adolescent psychopathology (e.g., Hankin, Snyder, & Gulley, 2016; Zhou, Chen, & Main, 2012; Zimmer-Gembeck & Skinner, 2016).
Improve conceptualization.
Research on coping and emotion regulation in children and adolescents is at a crossroads. To varying degrees, both of these constructs involve adaptive processes to regulate emotion, cognition, behavior, and physiology (Compas et al., 2014a; Skinner et al., 2003; Thompson, 1994; Zimmer-Gembeck & Skinner, 2016). However, as clearly illustrated by the studies included in the current meta-analysis, research on coping and emotion regulation continues to be reflected in separate literatures without a shared conceptual framework and little to no integration of findings from research across constructs. Based on the findings presented here, we propose that many of the distinctions between these two constructs are artificial and synthesis of these two lines of theory and research is long overdue. The following steps are suggested to increase the coordination and integration of future research.
First, the processes of coping and emotion regulation are concerned with the same set of strategies of adaptation. Specifically, all of the strategies identified in the current meta-analysis have appeared in studies of both emotion regulation and coping. The distinction between these constructs and the factors and strategies they encompass has led to an underestimation of our knowledge base of these processes. Reviews have summarized findings from studies of coping to the exclusion of studies of emotion regulation (e.g., Aldridge & Roesch, 2007) and similarly, reviews of evidence on emotion regulation have overlooked much of the research on coping (e.g., Schäfer et al., 2017). An example from recent research is illustrative. Christensen, Aldao, Sheridan, and McLaughlin (2017) presented important findings on the differential effects of emotion regulation strategies in response to controllable versus uncontrollable stressors. However, the findings regarding emotion regulation and controllable and uncontrollable stressors will be better understood when considered in light of a rich history of similar research on coping with stressors. For example, several studies have found an interaction of type of coping by controllability of a stressor in predicting levels of internalizing symptoms (e.g., Compas et al., 2012; Forsythe & Compas, 1987; Folkman, Chesney, Pollack, & Coates, 1993; Osowiecki & Compas, 1998, 1999). The current review is a first step in bringing these lines of research together for a comprehensive analysis.
Second, coping research will be informed by closer attention to specific emotions that arise in response to stress. Likewise, emotion regulation research will be informed by closer attention to the sources of stress and events that give rise to specific emotions. It can be argued that all efforts to cope with stress are motivated by the goal of reducing negative emotions and enhancing positive emotions in response stressful events and circumstances. However, coping efforts may be aimed at other goals in addition to the regulation of emotion such as altruistic efforts to help another or more instrumental goals related to personal achievement (e.g., Gross, 1999; Scheier, Weinbtraub, & Carver, 1986). A primary division between coping and emotion regulation centers on the precipitants of regulatory efforts. As discussed above, coping is conceptualized as a response to stressful events or stressful conditions in the environment, whereas emotion regulation is directed toward emotions that may occur in reaction to both stressful and normative, non-stressful experiences (e.g., Gross & Jazaieri, 2014). Conversely, many emotions arise in response to stressful events and chronic sources of adversity and one important function of coping responses is the regulation of emotions that arise in these circumstances.
Third, coping and emotion regulation include cognitive and behavioral processes that are organized and goal directed. However, the field has been lacking a framework that encompasses both of these constructs. Synthesis of research and theory will benefit from tests of competing or complementary models that include both of these processes. We propose that at least three models could be tested: (a) coping and emotion regulation are organized around specific emotions, (b) coping and emotion regulation are organized as temporal processes, and (c) coping and emotion regulation are organized around the degree actual or perceived control of precipitating events or circumstances.
Studies of coping and emotion regulation frequently examine these processes in relation to overall negative emotion that is typically measured at the aggregate level. However, it is possible that coping and emotion regulation strategies are differentiated in response to specific negative emotions, such as sadness, anger, or anxiety. This is reflected in the work of Zeman and colleagues (Zeman et al., 2001, 2002, 2010) who have developed measures of emotion regulation for use in response to specific negative emotions. Different strategies may be enacted in response to different emotions and strategies or sets of strategies may differ in their effectiveness in managing specific emotions. For example, fear and anger have different effects on attentional processes, have both shared and distinct environmental and genetic correlates, and maybe related to different processes of self-regulation (Clifford et al., 2015; Engen et al., 2017; Kim-Spoon et al., 2015). Coping and emotion regulation factors such as primary and secondary control coping or strategies such as cognitive reappraisal and distraction may have different effects on these two emotions. Testing emotion-specific models will require careful measurement of both discrete emotions and the use of sets of strategies as measured at the level of factors in response to these emotions.
The importance of process is seen most clearly in the process model of emotion regulation of Gross and colleagues (e.g., Gross, 2015; Sheppes, Suri, & Gross, 2015). As described above, in this model, emotion regulation strategies are grouped into five broad categories that act on specific stages of the emotion generative cycle as an emotion is experienced: situation selection, situation modification, attentional deployment, cognitive change, and response modulation (Gross, 1998). The process model posits that these skills are deployed sequentially with different strategies potentially being more appropriate or adaptive prior to, during, or after the experience of an emotion. Current conceptualizations of coping in children and adolescents can be expanded by considering ways in which the process of coping may unfold over the course of a stressful event or prolonged exposure to chronic stress. For example, a diagnosis of cancer or diabetes may present children and adolescents with different stressors over the course of the diagnosis, treatment, and long-term adaptation, and these stressors may require different coping and emotion regulation responses (e.g., Compas et al., 2012, 2014b; Jaser, Patel, Xu, Tamborlane, & Grey, 2016). As noted below, this will require the use of short and long-term prospective studies in which coping and emotion regulation and symptoms of psychopathology are assessed at carefully selected times over the course of a stressor. Little empirical research has tested process models in children and adolescents, either under the rubric of coping or emotion regulation, and thus more research is needed to test this proposed structure of these processes.
Levels of actual and perceived control over stressors play a central role in several conceptualizations of coping across the lifespan (e.g., Allen et al., 2016; Landau, Kay, & Whitson, 2105; Skinner & Zimmer-Gembeck, 2010; Troy, Ford, McRae, Zarolia, & Mauss, 2016; Troy, Shallcross, & Mauss, 2013). Further, current conceptualization of learned helplessness and psychopathology emphasize the importance of both controllable and uncontrollable stress in the development of adaptive and maladaptive responses to stress (Maier & Seligman, 2016). As described above, a control-based model of coping in childhood and adolescence (Compas et al., 2001, 2012, 2014a; Weisz et al., 1994) has received considerable empirical support from studies using the RSQ and is robust across cultures and nationalities and types of stressors (Connor-Smith et al., 2000). Support for this model has come from studies using CFA with Euro-American adolescents (Compas et al., 2006b; Connor-Smith et al., 2000), Native American (Navajo) adolescents (Wadsworth et al., 2004), and adolescents in Spain (Connor-Smith & Calvete, 2004), Bosnia (Benson et al., 2011), and China (Xiao et al., 2010). This model has also been supported in CFAs using the RSQ in response to a wide range of stressors including war-related trauma (Benson et al., 2011), chronic pain (Compas et al., 2006b), and peer stress (Connor-Smith et al., 2000; Connor-Smith & Calvete, 2004; Xiao et al., 2010). However, support for a control-based model of coping and emotion regulation also has several limitations. The most significant concern is that empirical evidence has not been provided that the coping responses on the RSQ are purposefully organized around the perceived or actual controllability of stressors, as the three-factor model implies. Thus, future research will benefit from more direct tests of controllability of the stressors with which children and adolescents are faced.
The potential importance of both the process model of emotion regulation and the control-based model of coping can be found in their shared emphasis on adapting responses to the demands of specific situations. That is, these models both posit that the effectiveness of types of coping and emotion regulation may depend on the context in which they are used. For example, the goodness-of-fit hypothesis suggests that the effectiveness of some coping strategies depends on the controllability of the stressor (e.g., Forsythe & Compas, 1987; Gidron, 2013; Lazarus & Folkman, 1984). Similarly, flexibility in the use of different emotion regulation strategies is related to greater regulation efficacy (e.g., Aldao & Nolen-Hoeksema, 2012, 2013; Aldao, Sheppes, & Gross, 2015; Christensen et al., 2017). We return to the broader importance of context in more detail below.
In summary, there are still issues to be resolved in defining and conceptualizing coping and emotion regulation. We propose that in instances where the context or precipitant for the process being studied is specific to the emotions that arise in the fabric of daily life (i.e., contexts and events that are not sources of stress), the process represents emotion regulation specifically. However, once a precipitating situation or context is identified as stressful, the process of adaptation lies broadly in the domain of coping. At this point, however, there is not enough evidence to distinguish coping and emotion regulation along the lines of presence or absence of a stressor. Until these distinctions are clarified empirically, we encourage the field to use the terms coping and emotion regulation together in order to be inclusive and representative of the state of the field and to lead to greater integration and synthesis of research findings. As an example of the importance of including these two concepts together, if we had used only coping or emotion regulation as search terms we would have identified very different sets of studies and drawn very different conclusions. Therefore, an approach that includes both of these concepts will provide a more complete picture of research on these adaptive processes.
Prioritize development.
Understanding the development of skills to regulate emotions and cope with stress across childhood and adolescence is central to understanding sources of risk and resilience and for the development of interventions to enhance these skills. Current knowledge about how coping and emotion regulation may change in their association with psychopathology with age is disappointing at best, as we found relatively little evidence in the current meta-analysis that the association of coping and emotion regulation with symptoms is different in childhood compared to adolescence. Guidance for future research can come from descriptive research on the development of coping and emotion regulation skills from early childhood through adolescence and into adulthood (Skinner & Zimmer-Gembeck, 2007, 2010; Zimmer-Gembeck & Skinner, 2011, 2016). Further, a roadmap for the development of coping and emotion regulation can be drawn from models of closely related constructs, including effortful control, executive function, and other related cognitive processes that develop across childhood and adolescence (Hankin et al., 2016; Zhou et al., 2012).
What is not known is whether the use of these strategies is more adaptive in adolescence as compared to childhood, or how the use of these skills changes across development. In some cases, the use of a strategy that is adaptive for one age group in response to a specific source of stress may either have no effect or be maladaptive for another age group faced with the same stressor. For example, seeking social support may be an adaptive strategy for a child to regulate feelings of sadness, but it may be maladaptive for adolescents if social support does not involve coping of controlled regulation of emotion and instead takes the form of co-rumination (e.g., Stone, Hankin, Gibb, & Abela, 2011).
Further, risk for psychopathology differs for boys and girls as they reach adolescence (e.g., Angold, 2008; Zahn-Waxler, Shirtcliff, & Marceau, 2008). Therefore, the associations of coping and emotion regulation with symptoms of psychopathology may differ by gender depending on the developmental stage at which these constructs are measured (e.g., Carlson & Grant, 2008; Sontag & Graber, 2010). This suggests that future research needs to examine carefully selected periods of development during which changes may occur both in the emergence of emotion regulation and coping skills and internalizing and externalizing symptoms. For example, it may be most important to study coping and emotion regulation as a source of risk and resilience for depressive symptoms during early and middle adolescence, as the rate of depressive symptoms and the onset of depressive disorders increases significantly during middle adolescence (e.g., Hankin et al., 1998).
We propose that the developmental course of coping and emotion regulation (a) is cumulative such that new skills are developed over time to build a broader skill set rather than replacing earlier ones as youth move into adolescence and young adulthood; (b) moves from a reliance on automatic processes in early childhood to both automatic and controlled processes in childhood and adolescence; (c) progresses from dependence primarily on caregivers to co-regulate or guide in regulation towards greater autonomy in the implementation of these processes; (d) becomes more differentiated moving into adolescence; and (e) involves increasingly more complex cognitive skills, which coincides with the development of language and executive function skills. For example, we hypothesize that coping and emotion regulation skills are used in largely undifferentiated ways in early childhood and will be best captured by the broad distinction of engagement/approach strategies vs. disengagement strategies. During late childhood and adolescence we propose that the use of engagement strategies become more differentiated based on increasing abilities to recognize varying degrees of control in stressful events and circumstances.
As a consequence of the development of the ability to perceive control, coping and emotion regulation attempts can be further differentiated into primary control and secondary control efforts (see also Skinner & Zimmer-Gembeck, 2010). This pattern of greater differentiation would reflect heterotypic continuity of coping and emotion regulation across childhood and adolescence (see Hankin et al., 2016). In contrast, an example of the homotypic continuity in the structure of coping and emotion regulation in adolescence and adulthood can be found in tests of the factor structure of a control-based model of coping. The three-factor structure of primary control coping, secondary control coping, and disengagement coping has been confirmed using CFA in diverse samples of adolescents (e.g., Benson et al., 2011; Xiao et al., 2010) and adults (e.g., Compas et al., 2006a,b). However, this model has not been tested in younger children to determine if these factors are less differentiated earlier in development.
Despite a number of remaining questions regarding the developmental course of processes of coping and emotion regulation, the skilled use of these processes emerges over the course of childhood and adolescence. Therefore coping and emotion regulation may act as a source of risk or resilience at later points in development (Skinner & Zimmer-Gembeck, 2007; Zimmer-Gembeck & Skinner, 2016). Interventions to enhance those coping and emotion regulation skills that promote resilience could be guided by more specific information about the likely points in development (i.e., sensitive periods) when children and adolescents will be responsive to learning and applying various skills and strategies.
Improve measurement and research design.
Since the previous broad reviews of measures of coping and emotion regulation in childhood and adolescence (Adrian et al., 2011; Compas et al., 2001), there has been progress in the availability of measures with established reliability and validity. We identified 16 measures of coping and emotion regulation that were used in over half of the studies reported in the meta-analysis (see Table 2). All of these measures have adequate reliability. Fourteen of these measures have at least some form of validity data, with five providing data on convergent and discriminant validity, and seven have reported findings from CFA to test the hypothesized structure of coping and emotion regulation. It is promising that research has progressed by more frequently using measures with acceptable psychometric properties. Further, because many researchers are interested in the ways that children and adolescents cope with stress and regulate their emotions in their daily lives, questionnaires and especially self-reports, will remain a central tool to study these processes.
The use of multiple informants to assess coping, emotion regulation and symptoms is important to improve the methodological rigor of the field. For example, the RSQ (Connor-Smith et al., 2000) is one of the few measures of coping with both self- and parent-report versions available. Obtaining reports on coping and emotion regulation using different methods than those used to assess symptoms of psychopathology provides stronger evidence for these associations that is not limited by problems of shared method variance that is inherent in single-informant methods (e.g., Compas et al., 2014b). Multi-informant methods need to become a standard for the field.
However, these measures need to be used in concert with other methodologies to improve external validity and generalizability. Ecological momentary assessment (EMA) of coping and emotion regulation offers an important method to understand these processes in real world contexts and closer to real time. For example, Allen et al. (2016) used EMA with a sample of children and adolescents (9–14 years old) during which they reported on perceived control, emotional reactivity (anxiety and physiological arousal), and emotion regulation strategy use in response to daily negative life events. Children’s perceptions of control over negative life events were related to less anxious reactivity and greater use of both problem solving and cognitive restructuring as reported in EMA. Tan et al. (2012) utilized an EMA approach to compare real-world emotional experiences of youth (9–13 years old) with generalized anxiety disorder, social anxiety disorder, or social phobia and age-matched healthy controls. Anxious youth reported more frequent physiological reactions in response to a negative event, and reports of avoidance, distraction and problem solving using EMA were associated with the down-regulation of negative emotions for both anxious and control youth. Further, Price et al. (2016) used EMA to assess avoidance, suppression and distraction during negative life events and linked these findings to functional neuroimaging data in a sample of adolescents. In this study, vigilance toward threat was positively associated with EMA distraction and suppression. These findings suggest the potential importance of using EMA methods along with child or adolescent and parent reports of children’s coping and emotion regulation to provide a more comprehensive picture of these processes.
Experimental designs and methods are also needed in which coping and emotion regulation are directly manipulated and causal effects on proxy measures of symptoms can be assessed under controlled conditions. Examples of this approach can be found in the rich tradition of experimental studies of emotion regulation in adults and children (e.g., Eisenberg, Smith, & Spinrad, 2011; Fox, Kirwan, & Reeb-Sutherland, 2012; Gross & Jazaieri, 2014; Penela, Walker, Degnan, Fox, & Henderson, 2015). Studies with children and adolescents have employed experimental designs to elicit negative emotions in the laboratory setting and observe automatic processes that reflect aspects of reactivity and arousal, while instructing participants to use a specific emotion regulation strategy (or strategies) to regulate the experience of the emotion in real time (e.g., Morris et al., 2011; Santucci et al., 2008). Experimental studies are not without their own limitations (e.g., only analogues of stress can be generated in the laboratory; observational methods cannot access covert cognitive forms of coping and emotion regulation) but it will be important to complement correlational designs with evidence obtained under controlled, experimental conditions.
In addition, relatively little attention has been given to sample characteristics with regard to important sources of diversity (e.g., race, ethnicity, socioeconomic status) or to comparisons of clinical as compared with non-clinical samples. It is possible that these processes differ in their associations with symptoms of psychopathology in children and adolescents faced with greater cumulative sociodemographic risk and subsequently greater levels of stress (Wadsworth, 2015). Further, it is possible that strategies typically considered a source of risk (e.g., avoidance), may be more strongly associated with psychopathology in a clinical sample, whereas those strategies may be unrelated to psychopathology in a non-clinical sample. More careful selection of samples that differ in ways that may have bearing on the association of coping and emotion regulation with symptoms of psychopathology is an important direction for future research.
Lastly, longitudinal designs are needed to test the directions of the relations of coping and emotion regulation with symptoms. Similar to multi-informant methods, longitudinal studies have been used with increasing frequency in recent research, but this design, although more costly and time consuming for researchers, needs to be prioritized. Longitudinal designs offer the opportunity to examine the direction of the association between coping and emotion regulation and symptoms of psychopathology. The degree to which coping and emotion regulation can predict changes or residual variance in levels of symptoms across time can provide better evidence about the direction of the relationship of these constructs with psychopathology. However, it is also possible that initial levels of internalizing and externalizing symptoms predict later coping and emotion regulation, in part because high levels of symptoms may impede the development of or the ability to effectively use these skills. Longitudinal designs can be used to test whether coping, emotion regulation, and symptoms of psychopathology are correlated because of the shared effect of a third variable. Finally, longitudinal designs are essential to test the developmental course of coping and emotion regulation to determine if these constructs are stable in their form across childhood and adolescence (homotypic continuity) or change in form with development (heterotypic continuity) (see Hankin et al., 2016). For example, the hypothesis presented above that coping becomes more differentiated with development would reflect heterotypic continuity and requires longitudinal studies that span childhood and the transition to adolescence to test this possibility.
Further, greater attention is needed to matching research designs to the specific questions and models being tested. For example, studies of an acute stressful event (e.g., the diagnosis of a serious illness) require assessments spaced over short periods of time, as the associations between coping and emotion regulation and symptoms may be strongest closest to and/or during the experience of that specific event (e.g., Compas et al., 2014b). In addition, an acute stressful event may also require long-term follow-up to assess the residual effects of this event and the ways in which youth coped with and regulated emotions in response to it (e.g., Compas et al., 2017). On the other hand, studies of chronic stressful conditions and adversity (e.g., economic disadvantage) need to examine processes of coping and emotion regulation over longer time frames during which the stressor is experienced.
Identify cognitive and neurobiological substrates of coping and emotion regulation.
Research in psychopathology has been reshaped by an emphasis on underlying processes as reflected in the RDoC from the National Institute of Mental Health (Casey et al., 2014; Insel & Cuthbert, 2015). A similar approach is needed to provide a better understanding of the processes that reflect the neurobiological foundations and substrates of coping and emotion regulation (see Etkin, Buchel, & Gross, 2015; Fernandez, Jazaieri, & Gross, 2016). One important avenue for future research involves the examination of neurocognitive correlates of coping and emotion regulation. Several aspects of executive function (e.g., working memory, attentional control) may provide a foundation for the use of coping and emotion regulation, as these processes often require the use of complex cognitive skills (Campbell et al., 2009; Eisenberg & Zhou, 2016; McRae et al., 2010).
Researchers have begun to identify neurobiological substrates of these processes using neuroimaging methods such as functional magnetic resonance imaging in order to identify patterns of activation in specific brain regions in children and adolescents that are associated with coping and emotion regulation skills. The most frequent target of these studies has been the use of cognitive reappraisal as a coping and emotion regulation strategy. A consistent pattern of findings has emerged, suggesting that increased activation during reappraisal of emotional stimuli occurs in several areas of the prefrontal cortex (PFC), including the ventromedial, ventrolateral, and dorsolateral PFC (e.g., Belden et al., 2014, 2015; Dougherty et al., 2015; McRae et al., 2012; Robinson et al., 2015; Stephanou et al., 2015). The associations between executive function and coping and emotion regulation can also be examined using neuroimaging methods. For example, Robinson et al. (2015) found significant correlations between activation of prefrontal brain regions in response to a standard working memory (n-back) task and parent and child reports of children’s use of secondary control coping strategies in a sample of pediatric brain tumor patients and healthy controls. Similarly, Reising et al (2017, in press) found that activation in the DLPFC, dACC, and APFC was significantly related to adolescents’ reports of their use of secondary control coping and accounted for adverse effects of stress exposure on adolescents’ coping. Neuroimaging methods can shed light on the associations between rapid automatic processes as contrasted with controlled processes of coping and emotion regulation by examining responses of both emotion (e.g., the amygdala) and executive function regions (e.g., areas of the PFC) of the brain (e.g., Belden et al., 2014, 2015).
Further, coping and emotion regulation may play an important role in explicating individual differences in genetic sources of risk and resilience (e.g., Ford, Mauss, Troy, Smolen, & Hankin, 2014). Individual differences in coping and emotion regulation may be associated with specific patterns of polymorphisms of genes that are related to stress sensitivity including the serotonin transporter polymorphism (5-HTTLPR) and corticotropin-releasing hormone receptors (CRHR) (Hankin, Badanes, Smolen, & Young, 2015). Examining correlates of coping and emotion regulation at multiple levels of analyses will provide a much richer understanding of factors that contribute to the development of these skills.
Examine context.
Research on the neurobiological substrates of coping and emotion regulation needs to be balanced by careful attention to the context in which children and adolescents are engaged in the processes of coping and emotion regulation. First, emotion regulation will be better understood by examining this process in the context in which emotions arise. For example, a child or adolescent who experiences sadness in the context of a peer rejection (e.g., not being included in a party with classmates) may be faced with a very different challenge than one who experiences sadness in the context of chronic stress associated with living with a depressed parent. Current questionnaire measures of emotion regulation often do not assess the context in which emotions occur and as a consequence possible differences in emotions as a function of the context in which they arise. Second, as noted above, it will be important to examine flexibility in coping with different types of stress including levels of objective and perceived control as important aspects of context (Skinner & Zimmer-Gembeck, 2010). Third, it will be important to give greater attention to the broader social context in which coping and emotion regulation occur, especially poverty and economic hardship. For example, the work of Wadsworth and colleagues has shown that the types of coping that may be adaptive for children and adolescents exposed to chronic economic hardship may differ from youth who live in more economically advantaged environments (e.g., Wadsworth, 2015; Wadsworth & Compas, 2002; Wadsworth, Rindlaub, Hurwich-Reiss, Rienks, Bianco, & Markman, 2013).
Intervention research.
Studies of the effects of interventions that target coping and emotion regulation skills represent an important next step for research in this field for several reasons. First, intervention studies using randomized designs can provide true experimental tests of the associations of coping and emotion regulation with psychopathology in real-world contexts. Second, intervention trials, especially preventive interventions, can provide information on the role of coping and emotion regulation in the etiology of internalizing and externalizing symptoms. And most importantly, intervention research can clarify the role that coping and emotion regulation can play in alleviating and preventing psychopathology in young people. There is promising evidence that interventions can lead to changes in specific types of coping and that these changes account for the effects of these interventions on changes in symptoms (e.g., Compas et al., 2010; Tein et al., 2004, 2006). For example, in a randomized trial testing a preventive intervention for children of parents with a history of depression, Compas et al. (2010) found that changes in children’s use of secondary control coping skills as reported by children and their parents after completion of the intervention (6 months after baseline) partially accounted for (i.e., mediated) the effects of the intervention on child and parent reports of children’s internalizing and externalizing symptoms at 12-months. Continued research in this area is a high priority to establish the importance of coping and emotion regulation in treating and preventing psychopathology.
Summary and Conclusions
This review provides another important step in the integration of research on coping and emotion regulation in children and adolescents by considering the shared features of these two concepts and providing a synthesis of empirical research on their associations with internalizing and externalizing symptoms of psychopathology. The findings from the meta-analysis provide the first clear benchmark of empirical research for the field and a base of evidence for the association of coping and emotion regulation with symptoms of internalizing and externalizing psychopathology in children and adolescents. The findings from the current review also highlight significant limitations in the field, including stagnation in conceptualization and methods. To move the field forward we have outlined an ambitious and challenging agenda for next step in this research.
Public significance:
This meta-analysis reveals small to medium associations between the ways that children and adolescents cope with stress and regulate their emotions with symptoms of psychopathology. The findings have important implications for understanding the ways that some children and adolescents may be resilient to stress in their lives.
Acknowledgments
This research was supported by grants R01 MH100258 from the National Institute of Mental Health, R01 CA118332 from the National Cancer Institute, and DP3 DK097678 from the National Institute of Diabetes and Digestive and Kidney Diseases.
APPENDIX
| Domains | |
| Total Coping | Cope, Coping Attempts, Coping, Religion, Religious Coping, Self Coping, Self-Directed Coping, Total Coping, Unitary Coping |
| Adaptive Coping | Adaptive Balance Score, Adaptive Coping (with Anger, Sadness, Worry), Adaptive Strategies, Mean Positive Coping Score, Palliative Ratio, Positive Coping, Positive Religious Coping, Productive Coping |
| Maladaptive Coping | Dysfunctional Coping, Helpless Coping, Internalizing Negative Coping, Maladaptive Coping, Negative Coping, Negative Religious Coping, Non-constructive Coping, Nonproductive Coping |
| Emotion Regulation | Active/Emotional Regulation, Adaptive Affect Regulation, Adjusting, Anger Management, Anger Regulation (Coping), Anger-Related Emotion Regulation, Emotion Regulation (Anger, Anger Coping, Sadness, Sadness Coping), Emotion Regulation Scale, ER Adaptive, External Functional ER, Internal Functional ER, Palliative Emotion Regulation, Regulation Anger, Regulation Coping, Regulation, Sadness Regulation, Sadness Regulation Coping |
| Emotion Dysregulation | Abreacting, Clarity, Dysregulation, Impulse |
| Factors | |
| Problem-Focused Coping | Problem Focus, Problem Focused Action, Problem Focused (Engagement) Coping, Problem-Analyzing Coping, Problem-Directed Coping, Problem-Oriented Coping, Task-Oriented Coping |
| Emotion-Focused Coping | Emotion Focused (Engagement) Coping, Emotional Coping, Emotional Engagement, Emotion Oriented Coping, Internal Coping |
| Engagement/Approach Coping | Active Coping, Active Self-Regulation, Approach Coping, Approach-Oriented Coping, Assertion, Behavioral Coping, Distraction and Problem Solving, Engagement Coping, Mobilizing, Not Hiding, Observed Active Self Regulation, Physical Exercise, Physical Exercise Coping, Positive/Approach Coping, Rational Coping, Resorting, Work Hard |
| Disengagement Coping | Behavioral Disengagement, Deferring Coping, Detached Coping, Disengagement, Disengagement Coping, Passive Coping |
| Primary Control Coping | Primary Control, Primary Control Coping, Primary Control Engagement Coping |
| Secondary Control Coping | Accommodative Coping, Secondary Control, Secondary Control Coping, Secondary Control Engagement Coping |
| Social Support Coping | Active/Support Seeking, Adult Social Support, Advice/Support, Asking for Help, Collaborative Coping, Developing Social Support, Emotional Support, Emotion-Focused (Social) Support, Friend Support Seeking, Hangout with Peers Coping, Help Seeking, Instrumental Social Support, Invest in Close Friends, Parent Support Seeking, Parental Support, Peer Social Support, Problem Focused (Social) Support, Reference to Others Coping, Seek Professional Help, Seek Spiritual Support, Seek to Belong, Seeking Guidance, Seeking Help from Family/Peers, Seeking Others, Seeking Social Support, Seeking Spiritual Support, Seeks Support, Social Support (Family/Friends/Coping/Problem-Focused), Social Support Seeking, Support Coping, Support for Actions/Feelings, Support Seeking (Coping), Teacher Support Seeking |
| Strategies | |
| Acceptance | Acceptance (Coping), Acceptance/Resignation, Rational Acceptance, Resignation, Tolerating |
| Cognitive Reappraisal | Cognitive Coping, Cognitive Reappraisal, Cognitive Restructuring, Cognitive-Palliative Coping, Comforting Thoughts, Develops Competence and Optimism, Focus on Positive, Illusory Control, Interpretive Control, Minimization, Minimize Threat, Naïve Optimism, Positive Cognition/Cognitive Restructuring, Positive Reappraisal/Refocusing/Reframing/Reinterpretation, Positive Self Statements/Instructions, Predictive Control, Putting Into Perspective, Rationalization, Reappraisal, Reappraisal Frequency, Reinterpretation, Seeking Understanding, Take Light. Trivializing, Vicarious Control |
| Emotional Expression | Anger Expression, Emotion(al) Expression, Expressing Emotions, Expressing Feelings, Expression of Emotions, Focusing and Venting of Emotions, Physical Release of Emotions, Verbal Sharing |
| Problem Solving | Appearance Fixing, Behavioral Problem Solving, Cognitive Decision Making, Cognitive Problem Solving, Complies with Treatment, Conflict Resolution, Decision Making, Direct Problem Solving, Information Seeking, Logical Analysis, Planning, Proactive Mediation, Problem Solving (Coping/Style), Refocus on Planning, Self Reliant Problem Solving, Situation Control |
| Distraction | Behavioral Distraction, Cognitive Distraction, Demanding Activities, Distracting Activities/Actions, Distraction, Distraction Coping, Engage in Physical Recreation, Entertainment, Media Use, Seek Alternate Rewards, Seek Relaxing Diversions, Seeking Diversions |
| Avoidance | Avoidance (Coping), Avoidance of Social Support, Avoidant Actions/Activities/Coping/Style, Avoidant Oriented Coping, Avoiding (Problems), Behavioral Avoidant Coping, Cognitive Avoidance/Avoidant Coping, Cognitive Distancing, Distance/ing Coping, Emotion Focused Avoidance, Escape, Feels Different and Withdraws, Hedonistic Avoidance, Ignore Problems, Intropunitive Avoidance, Keeps to Self, Passive Avoidance, Problem Avoidant Coping, Problem Focused Avoidance, Self Isolation, Withdrawal (Coping), Withdrawing |
| Denial | Blame Others, Blaming Others, Defensive Coping, Denial (Coping), Other Blame, Retaliation, Revenge |
| Emotional Suppression | Anger In, Anger Inhibition, Concealing, Emotion(al) Suppression, Expressive Reluctance, Expressive Suppression, Inhibition, Masking, Repression, Sadness Inhibition, Suppression, Worry Inhibition |
| Wishful Thinking | Fantasizing, Fantasy, Imagining, Personal Superstitious Thinking, Wishful Thinking (Coping) |
Contributor Information
Bruce E. Compas, Vanderbilt University
Sarah S. Jaser, Vanderbilt University
Alexandra H. Bettis, Vanderbilt University
Kelly H. Watson, Vanderbilt University
Meredith Gruhn, Vanderbilt University.
Jennifer P. Dunbar, Vanderbilt University
Ellen Williams, Vanderbilt University.
Jennifer C. Thigpen, Vanderbilt University
References
(*) Studies included in meta-analysis.
- *.Abela JR, Brozina K, & Haigh EP (2002). An examination of the response styles theory of depression in third-and seventh-grade children: A short-term longitudinal study. Journal of Abnormal Child Psychology, 30, 515–527. 10.1023/a:1019873015594 [DOI] [PubMed] [Google Scholar]
- *.Abela JR, Vanderbilt E, & Rochon A (2004). A test of the integration of the response styles and social support theories of depression in third and seventh grade children. Journal of Social and Clinical Psychology, 23, 653–674. 10.1521/jscp.23.5.653.50752 [DOI] [Google Scholar]
- *.Abela JR, Aydin CM, & Auerbach RP (2007). Responses to depression in children: Reconceptualizing the relation among response styles. Journal of abnormal child psychology, 35, 913–927. 10.1007/s10802-007-9143-2 [DOI] [PubMed] [Google Scholar]
- Achenbach TM (1966). The classification of children’s psychiatric symptoms: A factor-analytic study. Psychological Monographs: General and Applied, 80, 1–37. 10.1037/h0093906 [DOI] [PubMed] [Google Scholar]
- Achenbach TM, & Rescorla LA (2001). Manual for the Achenbach system of empirically based assessment school-age forms profiles. Burlington, VT: ASEBA; 10.1002/9781118625392.wbecp150 [DOI] [Google Scholar]
- Achenbach TM, McConaughy SH, & Howell CT (1987). Child/adolescent behavioral and emotional problems: Implications of cross-informant correlations for situational specificity. Psychological Bulletin, 101, 213–232. 10.1037//0033-2909.101.2.213 [DOI] [PubMed] [Google Scholar]
- *.Adams P, Abela JRZ, & Hankin BL (2007). Factorial categorization of depression-related constructs in early adolescents. Journal of Cognitive Psychotherapy, 21, 123–139. https://doi:10.1891/088983907780851540 [Google Scholar]
- Adrian M, Zeman J, & Veits G (2011). Methodological implications of the affect revolution: A 35-year review of emotion regulation assessment in children. Journal of Experimental Child Psychology, 110, 171–197. https://doi:10.1016/j.jecp.2011.03.009 [DOI] [PubMed] [Google Scholar]
- *.Adrian M, Zeman J, Erdley C, Lisa L, Homan K, & Sim L (2009). Social contextual links to emotion regulation in an adolescent psychiatric inpatient population: Do gender and symptomatology matter? Journal of Child Psychology and Psychiatry, 50, 1428–1436. https://doi:10.1111/j.1469-7610.2009.02162.x [DOI] [PubMed] [Google Scholar]
- *.Ahmed SR, Kia-Keating M, & Tsai KH (2011). A structural model of racial discrimination, acculturative stress, and cultural resources among Arab American adolescents. American Journal of Community Psychology, 48, 181–192. https://doi:10.1007/s10464-011-9424-3 [DOI] [PubMed] [Google Scholar]
- Aldao A, & Nolen-Hoeksema S (2012). When are adaptive strategies most predictive of psychopathology? Journal of Abnormal Psychology, 121, 276–281. 10.1037/a0023598 [DOI] [PubMed] [Google Scholar]
- Aldao A,& Nolen-Hoeksema S (2013). One versus many: Capturing the use of multiple emotion regulation strategies in response to an emotion-eliciting stimulus. Cognition and Emotion, 27, 753–760. 10.1080/02699931.2012.739998 [DOI] [PubMed] [Google Scholar]
- Aldao A, Sheppes G, & Gross JJ (2015). Emotion regulation flexibility. Cognitive Therapy and Research, 39, 263–278. https://doi:10.1007/s10608-014-9662-4 [Google Scholar]
- Aldao A, Nolen-Hoeksema S, & Schweizer S (2010). Emotion-regulation strategies across psychopathology: A meta-analytic review. Clinical Psychology Review, 30, 217–237. https://doi:10.1016/j.cpr.2009.11.004 [DOI] [PubMed] [Google Scholar]
- Aldridge AA, & Roesch SC (2007). Coping and adjustment in children with cancer: A meta-analytic study. Journal of Behavioral Medicine, 30, 115–129. https://doi:10.1007/s10865-006-9087-y [DOI] [PubMed] [Google Scholar]
- Allen BK, Silk JS, Meller S, Tan PZ, Ladouceur CD, Sheeber LB, … & Ryan ND (2016). Parental autonomy granting and child perceived control: Effects on the everyday emotional experience of anxious youth. Journal of Child Psychology and Psychiatry, 57, 835–842. 10.1111/jcpp.12482 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Amone-P’Olak K, Garnefski N, & Kraaij V (2007). Adolescents caught between fires: Cognitive emotion regulation in response to war experiences in Northern Uganda. Journal of Adolescence, 30, 655–669. https://doi:10.1016/j.adolescence.2006.05.004 [DOI] [PubMed] [Google Scholar]
- Angold A (2008). Sex and developmental psychopathology In Hudziak J (ed.), Developmental psychopathology and wellness: Genetic and environmental influences (pp. 109–138). American Psychiatric Publishing: Washington DC. [Google Scholar]
- *.Auerbach RP, Abela JRZ, Zhu X, & Yao S (2007). A diathesis-stress model of engagement in risky behaviors in Chinese adolescents. Behaviour Research and Therapy, 45, 2850–2860. https://doi:10.1016/j.brat.2007.05.005 [DOI] [PubMed] [Google Scholar]
- Auerbach RP, Abela JR, Zhu X, & Yao S (2010). Understanding the role of coping in the development of depressive symptoms: Symptom specificity, gender differences, and cross-cultural applicability. British Journal of Clinical Psychology, 49, 547–561. [DOI] [PubMed] [Google Scholar]
- Ayers TS, Sandler IN, & Twohey JL (1998). Conceptualization and measurement of coping in children and adolescents In Advances in clinical child psychology, (Vol. 20) (pp. 243–301). New York, NY: Springer US; 10.1007/978-1-4757-9038-2_8 [DOI] [Google Scholar]
- Ayers TS, Sandler IN, West SG, & Roosa MW (1996). A dispositional and situational assessment of children’s coping: Testing alternative models of coping. Journal of Personality, 64, 923–958. https://doi:10.1111/j.1467-6494.1996.tb00949.x [DOI] [PubMed] [Google Scholar]
- *.Bachanas PJ, Kullgren KA, Suzman Schwartz K, Lanier B, McDaniel JS, Smith J, & Nesheim S (2001). Predictors of psychological adjustment in school-aged children infected with HIV. Journal of Pediatric Psychology, 26, 343–352. https://doi:10.1093/jpepsy/26.6.343 [DOI] [PubMed] [Google Scholar]
- *.Bal S, Crombez G, De Bourdeaudhuij I, & Van Oost P (2009). Symptomatology in adolescents following initial disclosure of sexual abuse: The roles of crisis support, appraisals and coping. Child Abuse & Neglect, 33, 717–727. https://doi:10.1016/j.chiabu.2008.11.006 [DOI] [PubMed] [Google Scholar]
- *.Bal S, De Bourdeaudhuij I, Crombez G, & Van Oost P (2005). Predictors of trauma symptomatology in sexually abused adolescents: A 6-month follow-up study. Journal of Interpersonal Violence, 20, 1390–1405. https://doi:10.1177/0886260505278720 [DOI] [PubMed] [Google Scholar]
- *.Bal S, Van Oost P, De Bourdeaudhuij I, & Crombez G (2003). Avoidant coping as a mediator between self-reported sexual abuse and stress-related symptoms in adolescents. Child Abuse & Neglect, 27, 883–897. https://doi:10.1016/S0145-2134(03)00137-6 [DOI] [PubMed] [Google Scholar]
- Bargh JA, & Williams LE (2007). The nonconscious regulation of emotion In Gross J (Ed.), Handbook of emotion regulation (pp. 429–445). New York, NY: Guilford Press. [Google Scholar]
- *.Batum P, & Yagmurlu B (2007). What counts in externalizing behaviors? The contributions of emotion and behavior regulation. Current Psychology: A Journal for Diverse Perspectives on Diverse Psychological Issues, 25, 272–294. https://doi:10.1007/BF02915236 [Google Scholar]
- *.Bender PK, Reinholdt-Dunne ML, Esbjørn BH, & Pons F (2012). Emotion dysregulation and anxiety in children and adolescents: Gender differences. Personality and Individual Differences, 53, 284–288. https://doi:10.1016/j.paid.2012.03.027 [Google Scholar]
- Benson MA, Compas BE, Layne CM, Vandergrift N, Pašalić H, Katalinksi R, & Pynoos RS (2011). Measurement of post-war coping and stress responses: A study of Bosnian adolescents. Journal of Applied Developmental Psychology, 32, 323–335. https://doi:10.1016/j.appdev.2011.07.001 [Google Scholar]
- Blount RL, Simons LE, Devine KA, Jaaniste T, Psychol M, Cohen LL, … & Hayutin LG (2008). Evidence-based assessment of coping and stress in pediatric psychology. Journal of Pediatric Psychology, 33, 1021–1045. https://doi:10.1093/jpepsy/jsm071 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Bowie BH (2010). Emotion regulation related to children’s future externalizing and internalizing behaviors. Journal of Child and Adolescent Psychiatric Nursing, 23, 74–83. https://doi:10.1111/j.1744-6171.2010.00226.x [DOI] [PubMed] [Google Scholar]
- Borenstein M, Hedges L, Higgins J, & Rothstein H (2005). Comprehensive meta-analysis version 2. Englewood, NJ: Biostat. [Google Scholar]
- *.Braun-Lewensohn O, Sagy S, & Roth G (2011). Coping strategies as mediators of the relationship between sense of coherence and stress reactions: Israeli adolescents under missile attacks. Anxiety, Stress & Coping: An International Journal, 24, 327–341. https://doi:10.1080/10615806.2010.494329 [DOI] [PubMed] [Google Scholar]
- *.Brechting EH, & Giancola PR (2007). A longitudinal study of coping strategies and substance use in adolescent boys. Journal of Child & Adolescent Substance Abuse, 16, 51–67. https://doi:10.1300/J029v16n02_03 [Google Scholar]
- *.Brenning KM, Soenens B, Braet C, & Bosmans G (2012). Attachment and depressive symptoms in middle childhood and early adolescence: Testing the validity of the emotion regulation model of attachment. Personal Relationships, 19, 445–464. https://doi:10.1111/j.1475-6811.2011.01372.x [Google Scholar]
- *.Brumariu LE, Kerns KA, & Seibert A (2012). Mother-child attachment, emotion regulation, and anxiety symptoms in middle childhood. Personal Relationships, 19, 569–585. https://doi:10.1111/j.1475-6811.2011.01379.x [Google Scholar]
- *.Calvete E, Camara M, Estevez A, & Villardón L (2011). The role of coping with social stressors in the development of depressive symptoms: Gender differences. Anxiety, Stress & Coping: An International Journal, 24, 387–406. https://doi:10.1080/10615806.2010.515982 [DOI] [PubMed] [Google Scholar]
- *.Campbell LK, Scaduto M, Van Slyke D, Niarhos F, Whitlock JA, & Compas BE (2009). Executive function, coping, and behavior in survivors of childhood acute lymphocytic leukemia. Journal of Pediatric Psychology, 34, 317–327. https://doi:10.1093/jpepsy/jsn080 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Caples HS, & Barrera M Jr. (2006). Conflict, support and coping as mediators of the relation between degrading parenting and adolescent adjustment. Journal of Youth and Adolescence, 35, 599–611. https://doi:10.1007/s10964-006-9057-2 [Google Scholar]
- *.Carlo G, Mestre MV, McGinley MM, Samper P, Tur A, & Sandman D (2012). The interplay of emotional instability, empathy, and coping on prosocial and aggressive behaviors. Personality and Individual Differences, 53, 675–680. https://doi:10.1016/j.paid.2012.05.022 [Google Scholar]
- Carlson GA, & Grant KE (2008). The role of stress and coping in explaining gender differences in risk for psychopathology among African American urban adolescents. Journal of Early Adolescence, 28, 375–404. [Google Scholar]
- Carpenter TP, Laney T, & Mezulis A (2012). Religious coping, stress, and depressive symptoms among adolescents: A prospective study. Psychology of Religion and Spirituality, 4, 19 10.1037/a0023155 [DOI] [Google Scholar]
- *.Carthy T, Horesh N, Apter A, Edge MD, & Gross JJ (2010). Emotional reactivity and cognitive regulation in anxious children. Behaviour Research and Therapy, 48, 384–393. https://doi:10.1016/j.brat.2009.12.013 [DOI] [PubMed] [Google Scholar]
- Carver CS, Scheier MF, & Weintraub JK (1989). Assessing coping strategies: A theoretically based approach. Journal of Personality and Social Psychology,56, 267–283. 10.1037//0022-3514.56.2.267 [DOI] [PubMed] [Google Scholar]
- *.Cascone P, Zimmermann G, Auckenthaler B, & Robert-Tissot C (2011). Cannabis dependence in Swiss adolescents: Exploration of the role of anxiety, coping styles, and psychosocial difficulties. Swiss Journal of Psychology, 70, 129–139. https://doi:10.1024/1421-0185/a000048 [Google Scholar]
- Casey BJ, Oliveri ME, & Insel T (2014). A neurodevelopmental perspective on the Research Domain Criteria (RDoC) framework. Biological Psychiatry, 76, 350–353. https://doi:10.1016/j.biopsych.2014.01.006 [DOI] [PubMed] [Google Scholar]
- *.Catanzaro SJ & Laurent J (2004). Perceived family support, negative mood regulation expectancies, coping, and adolescent alcohol use: Evidence of mediation and moderation effects. Addictive Behaviors, 29, 1779–1797. https://doi:10.1016/j.addbeh.2004.04.001 [DOI] [PubMed] [Google Scholar]
- Causey DL, & Dubow EF (1992). Development of a self-report coping measure for elementary school children. Journal of Clinical Child and Adolescent Psychology, 21, 47–59. https://doi:10.1207/s15374424jccp2101_8 [Google Scholar]
- Cheng C, Lau HB, & Chan MS (2014). Coping flexibility and psychological adjustment to stressful life changes: A meta-analytic review. Psychological Bulletin, 140, 1582–1607. https://doi:10.1037/a0037913 [DOI] [PubMed] [Google Scholar]
- Christensen KA, Sheridan MA, & McLaughlin KA (2017). Habitual reappraisal in context: peer victimization moderates its association with physiological reactivity to social stress, Cognition and Emotion, 31, 384–394, DOI: 10.1080/02699931.2015.1103701 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cicchetti D, Ganiban J, & Barnett D (1991). Contributions from the study of high-risk populations to understanding the development of emotion regulation In Garber J & Dodge KA (Eds.), The Development of Emotion Regulation and Dysregulation. New York: Cambridge University Press; 10.1017/cbo9780511663963.003 [DOI] [Google Scholar]
- Cicchetti D, & Curtis WJ (2007). Multilevel perspectives on pathways to resilient functioning. Development and Psychopathology, 19, 627–629. https://doi:10.1017/S0954579407000314 [DOI] [PubMed] [Google Scholar]
- *.Cicchetti D, Rogosch FA, & Sturge-Apple M (2007). Interactions of child maltreatment and serotonin transporter and monoamine oxidase A polymorphisms: Depressive symptomatology among adolescents from low socioeconomic status backgrounds. Development and Psychopathology, 19, 1161–1180. https://doi:10.1017/S0954579407000600 [DOI] [PubMed] [Google Scholar]
- *.Clark R, Novak JD, & Dupree D (2002). Relationship of perceived parenting practices to anger regulation and coping strategies in African-American adolescents. Journal of Adolescence, 25, 373–384. https://doi:10.1006/jado.2002.0482 [DOI] [PubMed] [Google Scholar]
- Clarke AT (2006). Coping with interpersonal stress and psychosocial health among children and adolescents: A meta-analysis. Journal of Youth and Adolescence, 35, 10–23. https://doi:10.1007/s10964-005-9001-x [Google Scholar]
- Clifford S, Lemery-Chalfant K, & Goldsmith HH (2015). The unique and shared genetic and environmental contributions to fear, anger, and sadness in childhood. Child Development, 86, 1538–1556. DOI: 10.1111/cdev.12394 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen J (1988). Statistical power analysis for the behavioral sciences, 2nd ed Hillsdale, NJ: Erlbaum. [Google Scholar]
- Compas BE, Beckjord E, Agocha B, Sherman ML, Langrock A, Grossman C, Dausch B, Glinder J, Kaiser C, Anderson-Hanley C, & Luecken L (2006a). Measurement of coping and stress responses in women with breast cancer. Psycho-Oncology, 15, 1038–1054. [DOI] [PubMed] [Google Scholar]
- *.Compas BE, Boyer MC, Stanger C, Colletti RB, Thomsen AH, Dufton LM, & Cole DA (2006b). Latent variable analysis of coping, anxiety/depression, and somatic symptoms in adolescents with chronic pain. Journal of Consulting and Clinical Psychology, 74, 1132–1142. https://doi:10.1037/0022-006X.74.6.1132 [DOI] [PubMed] [Google Scholar]
- Compas BE, Champion JE, Forehand R, Cole DA, Reeslund KL, Fear J, … & Merchant MJ (2010). Coping and parenting: Mediators of 12-month outcomes of a family group cognitive-behavioral preventive intervention with families of depressed parents. Journal of Consulting and Clinical Psychology, 78, 623–634. https://doi:10.1037/a0020459 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Compas BE, Connor-Smith JK, & Jaser SS (2004). Temperament, stress reactivity, and coping: Implications for depression in childhood and adolescence. Journal of Clinical Child and Adolescent Psychology, 33, 21–31. https://doi:10.1207/S15374424JCCP3301_3 [DOI] [PubMed] [Google Scholar]
- Compas BE, Connor-Smith JK, Saltzman H, Thomsen AH, & Wadsworth M (2001). Coping with stress during childhood and adolescence: Problems, progress, and potential in theory and research. Psychological Bulletin, 127, 87–127. https://doi:10.1037/0033-2909.127.1.87 [PubMed] [Google Scholar]
- Compas BE, Desjardins L, Vannatta K, Young-Saleme T, Rodriguez EM, … & Gerhardt CA (2014b). Children and adolescents coping with cancer: Self- and parent-reports of coping and anxiety/depression. Health Psychology, 33, 853–861. 10.1037/hea0000083 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Compas BE, Gruhn M, & Bettis AH (2017). Risk and resilience in child and adolescent psychopathology In Beauchaine TP & Hinshaw SP (Eds.), Child and Adolescent Psychopathology (3rd ed.) (pp. 114–143). New York: Wiley. [Google Scholar]
- Compas BE, Jaser SS, & Benson MA (2009). Coping and emotion regulation: Implications for understanding depression during adolescence In Nolen-Hoeksema S & Hilt L (Eds.), Handbook of Adolescent Depression (pp. 413–339). New York: Wiley. [Google Scholar]
- Compas BE, Jaser SS, Dunbar JP, Watson KH, Bettis AH, Gruhn MA, & Williams EK (2014a). Coping and emotion regulation from childhood to early adulthood: Points of convergence and divergence. Australian Journal of Psychology, 66, 71–81. https://doi:10.1111/ajpy.12043 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Compas BE, Jaser SS, Dunn MJ, & Rodriguez EM (2012). Coping with chronic illness in childhood and adolescence. Annual Review of Clinical Psychology, 8, 455–480. https://doi:10.1146/annurev-clinpsy-032511-143108 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Compas BE, Vannatta K, Bemis H, Desjardins L, Murphy LK……& Gerhardt CA (2017). Children and adolescents coping with stress: A longitudinal multi-informant study of children coping with cancer. Manuscript submitted for publication. [Google Scholar]
- Compas BE, Watson KH, Reising MM, & Dunbar JP (2013). Stress and coping: Transdiagnostic processes in child and adolescent psychopathology In Ehrenrich-May J & Chu B (Eds.), Transdiagnostic mechanisms and treatment approaches of youth psychopathology (pp. 35–58). New York, NY: Guilford. [Google Scholar]
- Connor-Smith JK, & Calvete E (2004). Cross-cultural equivalence of coping and involuntary responses to stress in Spain and the United States. Anxiety, Stress & Coping, 17, 163–185. https://doi:10.1080/10615800410001709412 [Google Scholar]
- Connor-Smith JK, Compas BE, Wadsworth ME, Thomsen AH, & Saltzman H (2000). Responses to stress in adolescence: Measurement of coping and involuntary responses to stress. Journal of Consulting and Clinical Psychology, 68, 976–992. https://doi:10.1037/0022-006X.68.6.976 [PubMed] [Google Scholar]
- D’Acremont M, & Van der Linden M (2007). How is impulsivity related to depression in adolescence? Evidence from a French validation of the cognitive emotion regulation questionnaire. Journal of adolescence, 30, 271–282. 10.1016/j.adolescence.2006.02.007 [DOI] [PubMed] [Google Scholar]
- *.Dahlbeck DT, & Lightsey OR Jr. (2008). Generalized self-efficacy, coping, and self-esteem as predictors of psychological adjustment among children with disabilities or chronic illnesses. Children’s Health Care, 37, 293–315. https://doi:10.1080/02739610802437509 [Google Scholar]
- *.Dalton MM, & Pakenham KI (2002). Adjustment of homeless adolescents to a crisis shelter: Application of a stress and coping model. Journal of Youth and Adolescence, 31, 79–89. https://doi:10.1023/A:1014041201490 [Google Scholar]
- *.Davies PT, Forman EM, Rasi JA, & Stevens KI (2002). Assessing children’s emotional security in the interparental relationship: The Security in the Interparental Subsystem Scales. Child Development, 73, 544–562. https://doi:10.1111/1467-8624.00423 [DOI] [PubMed] [Google Scholar]
- *.Davis SK, & Humphrey N (2012). The influence of emotional intelligence (EI) on coping and mental health in adolescence: Divergent roles for trait and ability EI. Journal of Adolescence, 35, 1369–1379. https://doi:10.1016/j.adolescence.2012.05.007 [DOI] [PubMed] [Google Scholar]
- Davey J, Turner RM, Clarke MJ, & Higgins JP (2011). Characteristics of meta-analyses and their component studies in the Cochrane Database of Systematic Reviews: A cross-sectional, descriptive analysis. BMC Medical Research Methodology, 11, 160 10.1186/1471-2288-11-160 [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Los Reyes A, Augenstein TM, Aldao A, Thomas SA, Daruwala S, Kline K, & Regan T (2015). Implementing psychophysiology in clinical assessments of adolescent social anxiety: Use of rater judgments based on graphical representations of psychophysiology. Journal of Clinical Child & Adolescent Psychology, 44, 264–279. https://doi:10.1080/15374416.2013.859080 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Dempsey M (2002). Negative coping as mediator in the relation between violence and outcomes: Inner-city African American youth. American Journal of Orthopsychiatry, 72, 102–109. https://doi:10.1037/0002-9432.72.1.102 [PubMed] [Google Scholar]
- Doom JR, & Gunnar MR (2013). Stress physiology and developmental psychopathology: Past, present and future. Development and Psychopathology, 25, 1359–1373. 10.1017/s0954579413000667 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dougherty LR, Blankenship SL, Spechler PA, Padmala S, & Pessoa L (2015). An fMRI pilot study of cognitive reappraisal in children: Divergent effects on brain and behavior. Journal of Psychopathology and Behavioral Assessment, 37, 634–644. 10.1007/s10862-015-9492-zs [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Downey LA, Johnston PJ, Hansen K, Birney J, & Stough C (2010). Investigating the mediating effects of emotional intelligence and coping on problem behaviours in adolescents. Australian Journal of Psychology, 62, 20–29. https://doi:10.1080/00049530903312873 [Google Scholar]
- *.Dufton LM, Dunn MJ, Slosky LS, & Compas BE (2011). Self-reported and laboratory-based responses to stress in children with recurrent pain and anxiety. Journal of Pediatric Psychology, 36, 95–105. https://doi:10.1093/jpepsy/jsq070 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Duncombe ME, Havighurst SS, Holland KA, & Frankling EJ (2012). The contribution of parenting practices and parent emotion factors in children at risk for disruptive behavior disorders. Child Psychiatry & Human Development, 43, 715–733. https://doi:10.1007/s10578-012-0290-5 [DOI] [PubMed] [Google Scholar]
- *.Duraković-Belko E, Kulenović A, & Dapić R (2003). Determinants of posttraumatic adjustment in adolescents from Sarajevo who experienced war. Journal of Clinical Psychology, 59, 27–40. 10.1002/jclp.10115 [DOI] [PubMed] [Google Scholar]
- Duval S, & Tweedie R (2000). Trim and fill: A simple funnel-plot-based of testing and adjusting for publication bias in meta-analysis. Biometrics, 56, 455–463. [DOI] [PubMed] [Google Scholar]
- Ebata AT, & Moos RH (1991). Coping and adjustment in distressed and healthy adolescents. Journal of Applied Developmental Psychology, 12, 33–54. 10.1016/0193-3973(91)90029-4 [DOI] [Google Scholar]
- *.Eccleston C, Crombez G, Scotford A, Clinch J, & Connell H (2004). Adolescent chronic pain: Patterns and predictors of emotional distress in adolescents with chronic pain and their parents. Pain, 108, 221–229. https://doi:10.1016/j.pain.2003.11.008 [DOI] [PubMed] [Google Scholar]
- *.Edlynn ES, Gaylord-Harden N, Richards MH, & Miller SA (2008). African American inner-city youth exposed to violence: Coping skills as a moderator for anxiety. American Journal of Orthopsychiatry, 78, 249–258. https://doi:10.1037/a0013948 [DOI] [PubMed] [Google Scholar]
- Egger M, Smith GD, Schneider M, & Minder C (1997). Bias in meta-analysis detected by a simple, graphical test. British Medical Journal, 315, 629–634. 10.1136/bmj.315.7109.629 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eisenberg N, Hofer C, & Vaughan J. (2007). Effortful control and its socioemotional consequences In Gross JJ (Ed.), Handbook of emotion regulation (pp. 287–306). New York, NY: Guilford Press. [Google Scholar]
- Eisenberg N, Fabes RA, & Guthrie IK (1997). Coping with stress: The roles of regulation and development In Wolchik SA & Sandler IN (Eds.), Handbook of children’s coping: Linking theory and intervention (pp. 41–70). New York, NY: Plenum. [Google Scholar]
- Eisenberg N, Smith CL, & Spinrad TL (2011). Effortful control: Relations with emotion regulation, adjustment and socialization in childhood In Vohs KD & Baumsister RF (eds.), Handbook of self-regulation: Research, theory, and applications (2nd ed.), pp. 263–283. New York, NY: Guilford; 115–136. Washington, DC: American Psychological Association. [Google Scholar]
- Eisenberg N, Spinrad TL, & Eggum ND (2010). Emotion related self-regulation and its relation to children’s maladjustment. Annual Review of Clinical Psychology, 6, 495–525. https://doi:10.1146/annurev.clinpsy.121208.131208 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eisenberg N, & Zhou Q (2016). Conceptions of executive function and regulation: When and to what degree to they overlap? In McCardle P & Freund LS (eds.), Executive function on preschool-age children: Integrating measurement, neurodevelopment, and translational research, pp. 10.1037/14797-006 [DOI] [Google Scholar]
- *.Elgar FJ, Arlett C, & Groves R (2003). Stress, coping, and behavioural problems among rural and urban adolescents. Journal of Adolescence, 26, 574–585. https://doi:10.1016/S0140-1971(03)00057-5 [DOI] [PubMed] [Google Scholar]
- *.Endriga MC, Jordan JR, & Speltz ML (2003). Emotion self-regulation in preschool-aged children with and without orofacial clefts. Journal of Developmental and Behavioral Pediatrics, 24, 336–344. https://doi:10.1097/00004703-200310000-00004 [DOI] [PubMed] [Google Scholar]
- Engen HG, Smallwood J, & Singer T (2017). Differential impact of emotional task relevance on three indices of prioritized processing for fearful and angry facial expressions, Cognition and Emotion, 31, 175–184, DOI: 10.1080/02699931.2015.1081873 [DOI] [PubMed] [Google Scholar]
- *.Erath SA, Flanagan KS, & Bierman KL (2007). Social anxiety and peer relations in early adolescence: Behavioral and cognitive factors. Journal of Abnormal Child Psychology, 35, 405–416. https://doi:10.1007/s10802-007-9099-2 [DOI] [PubMed] [Google Scholar]
- *.Erdem G, & Slesnick N (2010). That which does not kill you makes you stronger: Runaway youth’s resilience to depression in the family context. American Journal of Orthopsychiatry, 80, 195–203. https://doi:10.1111/j.1939-0025.2010.01023.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Erdur-Baker Ö (2009). Peer victimization, rumination, and problem solving as risk contributors to adolescents’ depressive symptoms. The Journal of Psychology: Interdisciplinary and Applied, 143, 78–90. https://doi:10.3200/JRLP.143.1.78-90 [DOI] [PubMed] [Google Scholar]
- *.Eschenbeck H, Heim-Dreger U, Tasdaban E, Lohaus A, & Kohlmann C (2012). A Turkish adaptation of the coping scales from the German Stress and Coping Questionnaire for Children and Adolescents. European Journal of Psychological Assessment, 28, 32–40. https://doi:10.1027/1015-5759/a000088 [Google Scholar]
- *.Escobar M, Fernández-Baena FJ, Miranda J, Trianes MV, & Cowie H (2011). Low peer acceptance and emotional/behavioural maladjustment in schoolchildren: Effects of daily stress, coping and sex. Anales de Psicología, 27, 412–417. [Google Scholar]
- Etkin A, Buchel C, & Gross JJ (2015). The neural bases of emotion regulation. Nature Reviews: Neuroscience, 16, 693–700. [DOI] [PubMed] [Google Scholar]
- Evans GW, & Kim P (2013). Childhood poverty, chronic stress, self-regulation, and coping. Child Development Perspectives, 7, 43–48. https://doi:10.1111/cdep.12013 [Google Scholar]
- Evans GW, Li D, & Whipple SS (2013). Cumulative risk and child development. Psychological Bulletin, 139, 1342–1396. https://doi:10.1037/a0031808 [DOI] [PubMed] [Google Scholar]
- Evers C, Hopp H, Gross JJ, Fischer AH, Manstead AS, & Mauss IB (2014). Emotion response coherence: A dual-process perspective. Biological Psychology, 98, 43–49. https://doi:10.1016/j.biopsycho.2013.11.003 [DOI] [PubMed] [Google Scholar]
- *.Farrell AD, Bettencourt A, Mays S, Kramer A, Sullivan T, & Kliewer W (2012). Patterns of adolescents’ beliefs about fighting and their relation to behavior and risk factors for aggression. Journal of Abnormal Child Psychology, 40, 787–802. https://doi:10.1007/s10802-011-9609-0 [DOI] [PubMed] [Google Scholar]
- *.Fear JM, Champion JE, Reeslund KL, Forehand R, Colletti C, Roberts L, & Compas BE (2009). Parental depression and interparental conflict: Children and adolescents’ self-blame and coping responses. Journal of Family Psychology, 23, 762–766. doi: 10.1037/a0016381 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Feng X, Keenan K, Hipwell AE, Henneberger AK, Rischall MS, Butch J, … Babinski DE (2009). Longitudinal associations between emotion regulation and depression in preadolescent girls: Moderation by the caregiving environment. Developmental Psychology, 45, 798–808. https://doi:10.1037/a0014617 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fernandez KC, Jazaieri H, & Gross JJ (2016). Emotion regulation: A transdiagnostic perspective on a new RDoC domain. Cognitive Therapy and Research, 40, 426–440. 10.1007/s10608-016-9772-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Flanagan KS, Vanden Hoek KK, Ranter JM, & Reich HA (2012). The potential of forgiveness as a response for coping with negative peer experiences. Journal of Adolescence, 35, 1215–1223. https://doi:10.1016/j.adolescence.2012.04.004 [DOI] [PubMed] [Google Scholar]
- *.Flanders JL, Simard M, Paquette D, Parent S, Vitaro F, Pihl RO, & Séguin JR (2010). Rough-and-tumble play and the development of physical aggression and emotion regulation: A five-year follow-up study. Journal of Family Violence, 25, 357–367. https://doi:10.1007/s10896-009-9297-5 [Google Scholar]
- *.Flannery DJ, Singer MI, & Wester KL (2003). Violence, coping, and mental health in a community sample of adolescents. Violence and Victims, 18, 403–418. 10.1891/vivi.2003.18.4.403 [DOI] [PubMed] [Google Scholar]
- *.Flett GL, Druckman T, Hewitt PL, & Wekerle C (2012). Perfectionism, coping, social support, and depression in maltreated adolescents. Journal of Rational-Emotive & Cognitive-Behavior Therapy, 30, 118–131. https://doi:10.1007/s10942-011-0132-6 [Google Scholar]
- *.Flynn M, & Rudolph KD (2007). Perceptual asymmetry and youths’ responses to stress: Understanding vulnerability to depression. Cognition and Emotion, 21, 773–788. https://doi:10.1080/02699930600824635 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Flynn M, & Rudolph KD (2010). The contribution of deficits in emotional clarity to stress responses and depression. Journal of Applied Developmental Psychology, 31, 291–297. https://doi:10.1016/j.appdev.2010.04.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Folkman S, Chesney MA, Pollack L, & Coates TJ (1993). Stress, control, coping and depressive mood in human immunodeficiency virus-positive and -negative gay men in San Francisco. Journal of Nervous and Mental Disease 181, 409–416. [DOI] [PubMed] [Google Scholar]
- Folkman S, & Lazarus RS (1985). If it changes it must be a process: Study of emotion and coping during three stages of a college examination. Journal of Personality and Social Psychology, 48, 150–170. https://doi:10.1037/0022-3514.48.1.150 [DOI] [PubMed] [Google Scholar]
- Folkman S, & Moskowitz JT (2004). Coping: Pitfalls and promise. Annual Review of Psychology, 55, 745–774. https://doi:10.1146/annurev.psych.55.090902.141456 [DOI] [PubMed] [Google Scholar]
- Ford BQ, Mauss IB, Troy AS, Smolen A, & Hankin B (2014). Emotion regulation moderates the risk associated with the 5-HTT gene and stress in children. Emotion, 14, 930–939. 10.1037/a0036835 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Forns M, Amador JA, Kirchner T, Gómez J, Muro P, & Martorell B (2005). Psychometric properties of the Spanish version of the Moos Coping Response Inventory for youth. Psychological Reports, 97, 777–789. https://doi:10.2466/PR0.97.7.777-789 [DOI] [PubMed] [Google Scholar]
- *.Forns M, Balluerka N, Gómez-Benito J, Kirchner T, & Amador JA (2010). Multilevel approach to stressors, coping, and psychopathological symptoms. Psychological Reports, 106, 262–278. https://doi:10.2466/PR0.106.1.262-278 [DOI] [PubMed] [Google Scholar]
- Forsythe CJ, & Compas BE (1987). Interaction of cognitive appraisals of stressful events and coping: Testing the goodness of fit hypothesis. Cognitive Therapy and Research, 11, 473–485. https://doi:10.1007/BF01175357 [Google Scholar]
- Fox NA, Kirwan M, & Reeb-Sutherland B (2012). Measuring the physiology of emotion and emotion regulation—Timing is everything. Monographs of the Society for Research in Child Development, 77, 98–108. 10.1111/j.1540-5834.2011.00668.x [DOI] [Google Scholar]
- *.Fredland NM, Campbell JC, & Han H (2008). Effect of violence exposure on health outcomes among young urban adolescents. Nursing Research, 57, 157–165. https://doi:10.1097/01.NNR.0000319493.21628.c6 [DOI] [PubMed] [Google Scholar]
- Frydenberg E, & Lewis R (1993). Manual: The adolescent coping scale. Melbourne: Australian Council for Educational Research. [Google Scholar]
- *.Gardner KJ, Archer J, & Jackson S (2012). Does maladaptive coping mediate the relationship between borderline personality traits and reactive and proactive aggression? Aggressive Behavior, 38, 403–413. https://doi:10.1002/ab.21437 [DOI] [PubMed] [Google Scholar]
- *.Garnefski N, & Kraaij V (2006). Relationships between cognitive emotion regulation strategies and depressive symptoms: A comparative study of five specific samples. Personality and Individual Differences, 40, 1659–1669. https://doi:10.1016/j.paid.2005.12.009 [Google Scholar]
- *.Garnefski N, Boon S, & Kraaij V (2003). Relationships between cognitive strategies of adolescents and depressive symptomatology across different types of life event. Journal of Youth and Adolescence, 32, 401–408. https://doi:10.1023/A:1025994200559 [Google Scholar]
- Garnefski N, Kraaij V, & Spinhoven P (2001). Negative life events, cognitive emotion regulation and emotional problems. Personality and Individual Differences, 30, 1311–1327. https://doi:10.1016/S0191-8869(00)00113-6 [Google Scholar]
- *.Garnefski N, Kraaij V, & van Etten M (2005). Specificity of relations between adolescents’ cognitive emotion regulation strategies and internalizing and externalizing psychopathology. Journal of Adolescence, 28, 619–631. https://doi:10.1016/j.adolescence.2004.12.009 [DOI] [PubMed] [Google Scholar]
- *.Garnefski N, Legerstee J, Kraaij V, van den Kommer T, & Teerds J (2002). Cognitive coping strategies and symptoms of depression and anxiety: A comparison between adolescents and adults. Journal of Adolescence, 25, 603–611. https://doi:10.1006/jado.2002.0507 [DOI] [PubMed] [Google Scholar]
- *.Garnefski N, Rieffe C, Jellesma F, Meerum Terwogt M, & Kraaij V (2007). Cognitive emotion regulation strategies and emotional problems in 9–11-year-old children: The development of an instrument. European Child & Adolescent Psychiatry, 16, 1–9. https://doi:10.1007/s00787-006-0562-3 [DOI] [PubMed] [Google Scholar]
- *.Gaylord-Harden N (2008). The influence of student perceptions of parenting and coping on achievement and classroom behavior among African American children. Psychology in the Schools, 45, 763–777. https://doi:10.1002/pits.20340 [Google Scholar]
- *.Gaylord-Harden N, Elmore CA, Campbell CL, & Wethington A (2011). An examination of the tripartite model of depressive and anxiety symptoms in African American youth: Stressors and coping strategies as common and specific correlates. Journal of Clinical Child and Adolescent Psychology, 40, 360–374. https://doi:10.1080/15374416.2011.563467 [DOI] [PubMed] [Google Scholar]
- *.Gaylord-Harden N, Gipson P, Mance G, & Grant KE (2008). Coping patterns of African American adolescents: A confirmatory factor analysis and cluster analysis of the children’s coping strategies checklist. Psychological Assessment, 20, 10–22. https://doi:10.1037/1040-3590.20.1.10 [DOI] [PubMed] [Google Scholar]
- *.Gaylord-Harden N, Taylor JJ, Campbell CL, Kesselring CM, & Grant KE (2009). Maternal attachment and depressive symptoms in urban adolescents: The influence of coping strategies and gender. Journal of Clinical Child and Adolescent Psychology, 38, 684–695. https://doi:10.1080/15374410903103569 [DOI] [PubMed] [Google Scholar]
- *.Gentzler AL, Santucci AK, Kovacs M, & Fox NA (2009). Respiratory sinus arrhythmia reactivity predicts emotion regulation and depressive symptoms in at-risk and control children. Biological Psychology, 82, 156–163. https://doi:10.1016/j.biopsycho.2009.07.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gidron Y (2013). Goodness of fit In Gellman MD & Turner JR (Eds.), Encyclopedia of Behavioral Medicine (pp. 875–876). New York, NY: Springer. [Google Scholar]
- *.Gold JI, Mahrer NE, Treadwell M, Weissman L, & Vichinsky E (2008). Psychosocial and behavioral outcomes in children with sickle cell disease and their healthy siblings. Journal of Behavioral Medicine, 31, 506–516. https://doi:10.1007/s10865-008-9175-2 [DOI] [PubMed] [Google Scholar]
- *.Gonzales NA, Tein J, Sandler IN, & Friedman RJ (2001). On the limits of coping: Interaction between stress and coping for inner-city adolescents. Journal of Adolescent Research, 16, 372–395. https://doi:10.1177/0743558401164005 [Google Scholar]
- *.Gould LF, Hussong AM, & Hersh MA (2012). Emotional distress may increase risk for self-medication and lower risk for mood-related drinking consequences in adolescents. The International Journal of Emotional Education, 4, 6–24. 10.15288/jsad.2008.69.296 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grant KE, Compas BE, Stuhlmacher AF, Thurm AE, McMahon SD, & Halpert JA (2003). Stressors and child and adolescent psychopathology: Moving from markers to mechanisms of risk. Psychological Bulletin, 129, 447–466. https://doi:10.1037/0033-2909.129.3.447 [DOI] [PubMed] [Google Scholar]
- Grant KE, Compas BE, Thurm AE, McMahon SD, & Gipson PY (2004). Stressors and child and adolescent psychopathology: Measurement issues and prospective effects. Journal of Clinical Child and Adolescent Psychology, 33, 412–425. https://doi:10.1207/s15374424jccp3302_23 [DOI] [PubMed] [Google Scholar]
- Grant KE, Compas BE, Thurm AE, McMahon SD, Gipson PY, Campbell AJ, … & Westerholm RI (2006). Stressors and child and adolescent psychopathology: Evidence of moderating and mediating effects. Clinical Psychology Review, 26, 257–283. https://doi:10.1016/j.cpr.2005.06.011 [DOI] [PubMed] [Google Scholar]
- Grant KE, McMahon SD, Duffy SN, Taylor JJ, & Compas BE (2011). Stressors and mental health problems in childhood and adolescence In Contrada RJ, & Baum A (Eds.), The handbook of stress science: Biology, psychology, and health; the handbook of stress science: Biology, psychology, and health (pp. 359–372, Chapter xxii, 676 Pages) Springer Publishing Co, New York, NY. [Google Scholar]
- Gratz KL, & Roemer L (2004). Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the Difficulties in Emotion Regulation Scale. Journal of Psychopathology and Behavioral Assessment, 26, 41–54. 10.1023/b:joba.0000007455.08539.94 [DOI] [Google Scholar]
- *.Gratz KL, Tull MT, Reynolds EK, Bagge CL, Latzman RD, Daughters SB, & Lejuez CW (2009). Extending extant models of the pathogenesis of borderline personality disorder to childhood borderline personality symptoms: The roles of affective dysfunction, disinhibition, and self- and emotion-regulation deficits. Development and Psychopathology, 21, 1263–1291. https://doi:10.1017/S0954579409990150 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Graziano PA, Reavis RD, Keane SP, & Calkins SD (2007). The role of emotion regulation in children’s early academic success. Journal of School Psychology, 45, 3–19. https://doi:10.1016/j.jsp.2006.09.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Grootenhuis MA, & Last BF (2001). Children with cancer with different survival perspectives: Defensiveness, control strategies, and psychological adjustment. Psycho-Oncology, 10, 305–314. https://doi:10.1002/pon.529 [DOI] [PubMed] [Google Scholar]
- Gross JJ (1998). Antecedent-and response-focused emotion regulation: Divergent consequences for experience, expression, and physiology. Journal of Personality and Social Psychology, 74, 224 10.1037//0022-3514.74.1.224 [DOI] [PubMed] [Google Scholar]
- Gross JJ (1999). Emotion regulation: Past, present, future. Cognition & Emotion, 13, 551–573. https://doi:10.1080/026999399379186 [Google Scholar]
- Gross JJ (2001). Emotion regulation in adulthood: Timing is everything. Current Directions in Psychological Science, 10, 214–219. 10.1111/1467-8721.00152 [DOI] [Google Scholar]
- Gross JJ (2015). Emotion regulation: Current status and future directions. Psychological Inquiry, 26, 1–16. DOI: 10.1080/1047840X.2014.940781 [DOI] [Google Scholar]
- Gross JJ, & Jazaieri H (2014). Emotion, emotion regulation, and psychopathology: An affective science perspective. Clinical Psychological Science, 2, 387–401. 10.1177/2167702614536164 [DOI] [Google Scholar]
- Gross JJ, & John OP (2003). Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. Journal of Personality and Social Psychology, 85, 348–362. https://doi:10.1037/0022-3514.85.2.348 [DOI] [PubMed] [Google Scholar]
- Gross JJ, Sheppes G, & Urry HL (2011). Taking one’s lumps while https://doing the splits: A big tent perspective on emotion generation and emotion regulation. Cognition & Emotion, 25, 789–793. https://doi:10.1007/s10608-014-9662-4 [Google Scholar]
- Gross JJ, & Thompson RA (2007). Emotion regulation: Conceptual foundations In Gross JJ (Ed.), Handbook of emotion regulation (pp. 3–24). New York, NY: Guilford Press. [Google Scholar]
- *.Gullone E, & Taffe J (2012). The emotion regulation questionnaire for children and adolescents (ERQ-CA): A psychometric evaluation. Psychological Assessment, 24, 409–417. https://doi:10.1037/a0025777 [DOI] [PubMed] [Google Scholar]
- *.Hadd VN, & Crocker PRE (2007). The effect of stress-related factors on post-performance affects in competitive adolescent swimmers. International Journal of Sport and Exercise Psychology, 5, 142–157. https://doi:10.1080/1612197X.2007.9671816 [Google Scholar]
- *.Hampel P, & Petermann F (2006). Perceived stress, coping, and adjustment in adolescents. Journal of Adolescent Health, 38, 409–415. https://doi:10.1016/j.jadohealth.2005.02.014 [DOI] [PubMed] [Google Scholar]
- Han G, Miller JG, Cole PM, Zahn-Waxler C, & Hastings PD (2016). Adolescents’ internalizing and externalizing problems predict their affect-specific HPA and HPG axes reactivity. Developmental Psychobiology, 57, 769–785. [DOI] [PubMed] [Google Scholar]
- Hankin BL, Abramson LY, Moffitt TE, McGee R, Silva PA, & Angeli KE (1998). Development of depression from preadolescence to young adulthood: Emerging gender differences in a 10-year longitudinal study. Journal of Abnormal Psychology, 107, 128–140. 10.1037//0021-843x.107.1.128 [DOI] [PubMed] [Google Scholar]
- Hankin BL, Badanes LS, Smolen A, & Young JF (2015). Cortisol reactivity to stress among youth: Stability over time and genetic variants for stress sensitivity. Journal of Personality and Social Psychology, 124, 54–67. 10.1037/abn0000030 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hankin BL, Snyder HR, & Gulley L (2016). Cognitive risks in developmental psychopathology In Cecchetti D (Ed.), Developmental Psychopathology, Vol. 3: Maladaptation and Psychopathology, 3rd. edition New York: Wiley; 10.1002/9781119125556.devpsy308 [DOI] [Google Scholar]
- Harkness KL, & Monroe SM (2016). The assessment and measurement of adult life stress: Basic premises, operational principles, and design requirements. Journal of Abnormal Psychology, 125, 727–745. [DOI] [PubMed] [Google Scholar]
- *.Hasking PA (2006). Reinforcement sensitivity, coping, disordered eating and drinking behaviour in adolescents. Personality and Individual Differences, 40, 677–688. https://doi:10.1016/j.paid.2005.07.017 [Google Scholar]
- *.Hasking PA (2007). Reinforcement sensitivity, coping, and delinquent behaviour in adolescents. Journal of Adolescence, 30, 739–749. https://doi:10.1016/j.adolescence.2006.11.006 [DOI] [PubMed] [Google Scholar]
- *.Hasking PA, Scheier LM, & Abdallah A (2011). The three latent classes of adolescent delinquency and the risk factors for membership in each class. Aggressive Behavior, 37, 19–35. https://doi:10.1002/ab.20365 [DOI] [PubMed] [Google Scholar]
- *.Hébert M, Parent N, & Daignault IV (2007). The French-Canadian version of the Self-Report Coping Scale: Estimates of the reliability, validity, and development of a short form. Measurement and Evaluation in Counseling and Development, 40, 2–15. [Google Scholar]
- *.Hébert M, Tremblay C, Parent N, Daignault IV, & Piché C (2006). Correlates of behavioral outcomes in sexually abused children. Journal of Family Violence, 21, 287–299. https://doi:10.1007/s10896-006-9026-2 [Google Scholar]
- Hedges L, & Olkin I (1985). Statistical methods for meta-analysis. New York, NY: Academic Press. [Google Scholar]
- *.Hermann C, Hohmeister J, Zohsel K, Ebinger F, & Flor H (2007). The assessment of pain coping and pain-related cognitions in children and adolescents: Current methods and further development. The Journal of Pain, 8, 802–813. https://doi:10.1016/j.jpain.2007.05.010 [DOI] [PubMed] [Google Scholar]
- Higgins JPT, & Green S (2011). Cochrane handbook for systematic reviews of interventions. Retrieved from www.cochrane-handbook.org.
- *.Hilt LM, McLaughlin KA, & Nolen-Hoeksema S (2010). Examination of the response styles theory in a community sample of young adolescents. Journal of Abnormal Child Psychology, 38, 545–556. 10.1007/s10802-009-9384-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Hocking MC, Barnes M, Shaw C, Lochman JE, Madan-Swain A, & Saeed S (2011). Executive function and attention regulation as predictors of coping success in youth with functional abdominal pain. Journal of Pediatric Psychology, 36, 64–73. https://doi:10.1093/jpepsy/jsq056 [DOI] [PubMed] [Google Scholar]
- *.Holen S, Lervåg A, Waaktaar T, & Ystgaard M (2012). Exploring the associations between coping patterns for everyday stressors and mental health in young schoolchildren. Journal of School Psychology, 50, 167–193. https://doi:10.1016/j.jsp.2011.10.006 [DOI] [PubMed] [Google Scholar]
- Hopp H, Troy AS, & Mauss IB (2011). The unconscious pursuit of emotion regulation: Implications for psychological health. Cognition and Emotion, 25, 532–545. https://doi:10.1080/02699931.2010.532606 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Horwitz AG, Hill RM, & King CA (2011). Specific coping behaviors in relation to adolescent depression and suicidal ideation. Journal of Adolescence, 34, 1077–1085. https://doi:10.1016/j.adolescence.2010.10.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Hourigan SE, Goodman KL, & Southam-Gerow M (2011). Discrepancies in parents’ and children’s reports of child emotion regulation. Journal of Experimental Child Psychology, 110, 198–212. https://doi:10.1016/j.jecp.2011.03.002 [DOI] [PubMed] [Google Scholar]
- *.Hsieh M, & Stright AD (2012). Adolescents’ emotion regulation strategies, self-concept, and internalizing problems. The Journal of Early Adolescence, 32, 876–901. https://doi:10.1177/0272431611433848 [Google Scholar]
- *.Hudek-Knežević J Kardum I, & Maglica BK (2005). The sources of stress and coping styles as mediators and moderators of the relationship between personality traits and physical symptoms. Review of Psychology, 12, 91–101. 10.1016/0191-8869(95)00182-4 [DOI] [Google Scholar]
- Hyman SE (2010). The diagnosis of mental disorders: The problem of reification. Annual Review of Clinical Psychology, 6, 155–179. https://doi:10.1146/annurev.clinpsy.3.022806.091532 [DOI] [PubMed] [Google Scholar]
- Insel TR, & Cuthbert BN (2015). Brain disorders? Precisely: Precision medicine comes to psychiatry. Science, 348, 499–500. 10.1126/science.aab2358 [DOI] [PubMed] [Google Scholar]
- *.Ireland JL, Boustead R, & Ireland CA (2005). Coping style and psychological health among adolescent prisoners: A study of young and juvenile offenders. Journal of Adolescence, 28, 411–423. https://doi:10.1016/j.adolescence.2004.11.002 [DOI] [PubMed] [Google Scholar]
- Ivanova MY, Achenbach TM, Dumenci L, Rescorla LA, Almqvist F, Weintraub S, … & Verhulst FC (2007a). Testing the 8-syndrome structure of the child behavior checklist in 30 societies. Journal of Clinical Child and Adolescent Psychology, 36, 405–417. https://doi:10.1080/15374410701444363 [DOI] [PubMed] [Google Scholar]
- Ivanova MY, Achenbach TM, Rescorla LA, Dumenci L, Almqvist F, Bilenberg N, … & Verhulst FC (2007b). The generalizability of the Youth Self-Report syndrome structure in 23 societies. Journal of Consulting and Clinical Psychology, 75, 729–738. https://doi:10.1037/0022-006X.75.5.729 [DOI] [PubMed] [Google Scholar]
- *.Jacob ML, Morelen D, Suveg C, Jacobsen AMB, & Whiteside SP (2012). Emotional, behavioral, and cognitive factors that differentiate obsessive-compulsive disorder and other anxiety disorders in youth. Anxiety, Stress & Coping: An International Journal, 25, 229–237. https://doi:10.1080/10615806.2011.571255 [DOI] [PubMed] [Google Scholar]
- *.Jaser SS, Champion JE, Dharamsi KR, Reising MM, & Compas BE (2011). Coping and positive affect in adolescents of mothers with and without a history of depression. Journal of Child and Family Studies, 20, 353–360. https://doi:10.1007/s10826-010-9399-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Jaser SS, Champion JE, Reeslund KL, Keller G, Merchant MJ, Benson M, & Compas BE (2007). Cross-situational coping with peer and family stressors in adolescent offspring of depressed parents. Journal of Adolescence, 30, 917–932. https://doi:10.1016/j.adolescence.2006.11.010 [DOI] [PubMed] [Google Scholar]
- *.Jaser SS, Langrock AM, Keller G, Merchant MJ, Benson MA, Reeslund K, … Compas BE (2005). Coping with the stress of parental depression II: Adolescent and parent reports of coping and adjustment. Journal of Clinical Child and Adolescent Psychology, 34, 193–205. https://doi:10.1207/s15374424jccp3401_18 [DOI] [PubMed] [Google Scholar]
- Jaser SS, Patel N, Xu M, Tamborlane WV, & Grey M (2016). Stress and coping predicts adjustment and glycemic control in adolescents with Type 1 Diabetes. Annals of Behavioral Medicine, 1–9. 10.1007/s12160-016-9825-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Jose PE, & Huntsinger CS (2005). Moderation and mediation effects of coping by Chinese American and European American adolescents. The Journal of Genetic Psychology, 166, 16–44. https://doi:10.3200/GNTP.166.1.16-44 [DOI] [PubMed] [Google Scholar]
- *.Jose PE, & Schurer K (2010). Cultural differences in coping among New Zealand adolescents. Journal of Cross-Cultural Psychology, 41, 3–18. https://doi:10.1177/0022022109348783 [Google Scholar]
- *.Kaczynski KJ, Simons LE, & Claar RL (2011). Anxiety, coping, and disability: A test of mediation in a pediatric chronic pain sample. Journal of Pediatric Psychology, 36, 932–941. https://doi:10.1093/jpepsy/jsr024 [DOI] [PubMed] [Google Scholar]
- *.Kaminsky L, Robertson M, & Dewey D (2006). Psychological correlates of depression in children with recurrent abdominal pain. Journal of Pediatric Psychology, 31, 956–966. https://doi:10.1093/jpepsy/jsj103 [DOI] [PubMed] [Google Scholar]
- *.Keogh E, & Eccleston C (2006). Sex differences in adolescent chronic pain and pain-related coping. Pain, 123, 275–284. https://doi:10.1016/j.pain.2006.03.004 [DOI] [PubMed] [Google Scholar]
- *.Kim H, & Kim H (2007). Aggression among Korean adolescents: A comparison between delinquents and nondelinquents. Social Behavior and Personality, 35, 499–512. https://doi:10.2224/sbp.2007.35.4.499 [Google Scholar]
- *.Kim J, & Cicchetti D (2010). Longitudinal pathways linking child maltreatment, emotion regulation, peer relations, and psychopathology. Journal of Child Psychology and Psychiatry, 51, 706–716. https://doi:10.1111/j.1469-7610.2009.02202.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Kim HS, Kim HS, & Samuels-Dennis J (2012). The influence of psychosomatic symptoms, physical and sexual abuse, and coping strategies on delinquent behavior among Korean adolescents. Archives of Psychiatric Nursing, 26, 155–164. 10.1016/j.apnu.2011.06.006 [DOI] [PubMed] [Google Scholar]
- Kim-Spoon J, Holmes C, & Deater-Deckard K (2015). Attention regulates anger and fear to predict changes in adolescent risk-taking behaviors. Journal of Child Psychology and Psychiatry, 56, 756–765. doi: 10.1111/jcpp.12338 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Kochenderfer-Ladd B, & Skinner K (2002). Children’s coping strategies: Moderators of the effects of peer victimization? Developmental Psychology, 38, 267–278. https://doi:10.1037/0012-1649.38.2.267 [DOI] [PubMed] [Google Scholar]
- Kopp CB (1989). Regulation of distress and negative emotions: A developmental view. Developmental Psychology, 25, 343–354. https://doi:10.1037/0012-1649.25.3.343 [Google Scholar]
- Kraemer HC, Lowe KK, & Kupfer DJ (2005). To your health: How to understand what research tells us about risk. New York, NY: Oxford University Press. [Google Scholar]
- Kraemer HC, Noda A, & O’Hara R (2004). Categorical versus dimensional approaches to diagnosis: Methodological challenges. Journal of Psychiatric Research, 38, 17–25. https://doi:10.1016/S0022-3956(03)00097-9 [DOI] [PubMed] [Google Scholar]
- Krueger RF, & Markon KE (2006). Understanding psychopathology melding behavior genetics, personality, and quantitative psychology to develop an empirically based model. Current Directions in Psychological Science, 15, 113–117. https://doi:10.1111/j.0963-7214.2006.00418.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kushner SC (2015). A review of the direct and interactive effects of life stressors and dispositional traits on youth psychopathology. Child Psychiatry & Human Development, 46, 810–819. https://doi:10.1007/s10578-014-0523-x [DOI] [PubMed] [Google Scholar]
- Lahey BB, Van Hulle CA, Singh AL, Waldman ID, & Rathouz PJ (2011). Higher-order genetic and environmental structure of prevalent forms of child and adolescent psychopathology. Archives of General Psychiatry, 68, 181–189. https://doi:10.1001/archgenpsychiatry.2010.192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Landau MJ, Kay AC, & Whitson JA (2015). Compensatory control and the appeal of a structured world. Psychological Bulletin, 141, 694 10.1037/a0038703 [DOI] [PubMed] [Google Scholar]
- *.Langrock AM, Compas BE, Keller G, Merchant MJ, & Copeland ME (2002). Coping with the stress of parental depression: Parents’ reports of children’s coping, emotional, and behavioral problems. Journal of Clinical Child and Adolescent Psychology, 31, 312–324. https://doi:10.1207/153744202760082577 [DOI] [PubMed] [Google Scholar]
- *.Larsen JK, Vermulst AA, Eisinga R, English T, Gross JJ, Hofman E, … Engels RC (2012). Social coping by masking? Parental support and peer victimization as mediators of the relationship between depressive symptoms and expressive suppression in adolescents. Journal of Youth and Adolescence, 41, 1628–1642. https://doi:10.1007/s10964-012-9782-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lazarus RS (2006). Stress and emotion: A new synthesis. New York, NY: Springer Publishing Company. [Google Scholar]
- Lazarus RS, & Folkman S (1984). Stress, appraisal, and coping. New York, NY: Springer. [Google Scholar]
- Lazarus RS, & Launier R (1978). Stress-related transactions between person and environment In Pervin LA & Lewis M (Eds.), Perspectives in interactional psychology (pp. 287–327). New York, NY: Plenum Press. [Google Scholar]
- *.Legault L, Anawati M, & Flynn R (2006). Factors favoring psychological resilience among fostered young people. Children and Youth Services Review, 28, 1024–1038. https://doi:10.1016/j.childyouth.2005.10.006 [Google Scholar]
- LeGrange B, & Cole DA (2008). An expansion of the state-trait-occasion model: Accounting for shared method variance. Structural Equation Modeling, 15, 241–271. 10.1080/10705510801922381 [DOI] [Google Scholar]
- *.Lengua LJ, & Long AC (2002). The role of emotionality and self-regulation in the appraisal-coping process: Tests of direct and moderating effects. Journal of Applied Developmental Psychology, 23, 471–493. https://doi:10.1016/S0193-3973(02)00129-6 [Google Scholar]
- *.Lewis KM, Byrd DA, & Ollendick TH (2012). Anxiety symptoms in African-American and Caucasian youth: Relations to negative life events, social support, and coping. Journal of Anxiety Disorders, 26, 32–39. https://doi:10.1016/j.janxdis.2011.08.007 [DOI] [PubMed] [Google Scholar]
- *.Li CE, DiGiuseppe R, & Froh J (2006). The roles of sex, gender, and coping in adolescent depression. Adolescence, 41, 409–415. 10.1007/s11199-006-9076-1 [DOI] [PubMed] [Google Scholar]
- *.Libby CJ, & Glenwick DS (2010). Protective and exacerbating factors in children and adolescents with fibromyalgia. Rehabilitation Psychology, 55, 151–158. https://doi:10.1037/a0019518 [DOI] [PubMed] [Google Scholar]
- *.Lim M, Stormshak EA, & Falkenstein CA (2011). Psychosocial adjustment and substance use of Cambodian and Vietnamese immigrant youth. Journal of Cross-Cultural Psychology, 42, 104–119. https://doi:10.1177/0022022110362747 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Lima L, Guerra MP, & de Lemos MS (2010). The psychological adjustment of children with asthma: Study of associated variables. The Spanish Journal of Psychology, 13, 353–363. https://doi:10.1017/S1138741600003917 [DOI] [PubMed] [Google Scholar]
- *.Liu FF, Gonzales NA, Fernandez AC, Millsap RE, & Dumka LE (2011). Family stress and coping for Mexican origin adolescents. Journal of Clinical Child and Adolescent Psychology, 40, 385–397. https://doi:10.1080/15374416.2011.563463 [DOI] [PubMed] [Google Scholar]
- *.Liu YL, & Huang FM (2012). Mother-adolescent conflict in Taiwan: Links between attachment style and psychological distress. Social Behavior and Personality, 40, 919–931. https://doi:10.2224/sbp.2012.40.6.919 [Google Scholar]
- Lochman JE, & Wells KC (2004). The Coping Power program for preadolescent aggressive boys and their parents: Outcome effects at one-year follow-up. Journal of Consulting and Clinical Psychology, 72, 571–578. [DOI] [PubMed] [Google Scholar]
- *.Lougheed JP, & Hollenstein T (2012). A limited repertoire of emotion regulation strategies is associated with internalizing problems in adolescence. Social Development, 21, 704–721. https://doi:10.1111/j.1467-9507.2012.00663.x [Google Scholar]
- *.Lunkenheimer ES, Shields AM, & Cortina KS (2007). Parental emotion coaching and dismissing in family interaction. Social Development, 16, 232–248. https://doi:10.1111/j.1467-9507.2007.00382.x [Google Scholar]
- Luthar SS (2006). Resilience in development: A synthesis of research across five decades In Cicchetti D & Cohen DJ (Eds.), Developmental Psychopathology, Vol. 3 Risk, Disorder, and Adaptation (739–795). Hoboken, NJ: John Wiley & Sons Inc. [Google Scholar]
- Maier SF, & Seligman MEP (2016). Learned helplessness at fifty: Insights from neuroscience. Psychological Review, 123, 349–367. 10.1037/rev0000033 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Martyn-Nemeth P, Penckofer S, Gulanick M, Velsor-Friedrich B, & Bryant FB (2009). The relationships among self-esteem, stress, coping, eating behavior, and depressive mood in adolescents. Research in Nursing & Health, 32, 96–109. https://doi:10.1002/nur.20304 [DOI] [PubMed] [Google Scholar]
- Masten AS (2001). Ordinary magic: Resilience processes in development. American Psychologist, 56, 227–238. https://doi:10.1037/0003-066X.56.3.227 [DOI] [PubMed] [Google Scholar]
- Masten AS (2014). Global perspectives on resilience in children and youth. Child Development, 85, 6–20. https://doi:10.1111/cdev.12205 [DOI] [PubMed] [Google Scholar]
- *.Maurice-Stam H, Oort FJ, Last BF, Brons PPT, Caron HN, & Grootenhuis MA (2009). School-aged children after the end of successful treatment of non-central nervous system cancer: Longitudinal assessment of health-related quality of life, anxiety and coping. European Journal of Cancer Care, 18, 401–410. https://doi:10.1111/j.1365-2354.2008.01041.x [DOI] [PubMed] [Google Scholar]
- Mauss IB, Bunge SA, & Gross JJ (2007). Automatic emotion regulation. Social and Personality Psychology Compass, 1, 146–167. https://doi:10.1111/j.1751-9004.2007.00005.x [Google Scholar]
- *.Mavroveli S, Petrides KV, Rieffe C, & Bakker F (2007). Trait emotional intelligence, psychological well-being and peer-rated social competence in adolescence. British Journal of Developmental Psychology, 25, 263–275. https://doi:10.1348/026151006X118577 [Google Scholar]
- *.Maxwell MA, & Cole DA (2012). Development and initial validation of the Adolescent Responses to Body Dissatisfaction Measure. Psychological Assessment, 24, 721–737. https://doi:10.1037/a0026785 [DOI] [PubMed] [Google Scholar]
- *.Maybery D, Steer S, Reupert A, & Goodyear M (2009). The Kids Coping Scale. Stress and Health: Journal of the International Society for the Investigation of Stress, 25, 31–40. https://doi:10.1002/smi.1228 [Google Scholar]
- *.McKee L, Jones DJ, Roland E, Coffelt N, Rakow A, & Forehand R (2007). Maternal HIV/AIDS and depressive symptoms among inner-city African American youth: The role of maternal depressive symptoms, mother-child relationship quality, and child coping. American Journal of Orthopsychiatry, 77, 259–266. https://doi:10.1037/0002-9432.77.2.259 [DOI] [PubMed] [Google Scholar]
- McLaughlin KA, Alves S, & Sheridan MA (2014). Vagal regulation and internalizing psychopathology among adolescents exposed to childhood adversity. Developmental Psychobiology, 56, 1036–1051. 10.1002/dev.21187 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.McMahon SD, & Watts RJ (2002). Ethnic identity in urban African American youth: Exploring links with self-worth, aggression, and other psychosocial variables. Journal of Community Psychology, 30, 411–432. https://doi:10.1002/jcop.10013 [Google Scholar]
- McMahon SD, Grant KE, Compas BE, Thurm AE, & Ey S (2003). Stress and psychopathology in children and adolescents: Is there evidence of specificity? Journal of Child Psychology and Psychiatry, 44, 107–133. https://doi:10.1111/1469-7610.00105 [DOI] [PubMed] [Google Scholar]
- McRae K, Gross JJ, Weber J, Robertson ER, Sokol-Hessner P, Ray RD, … Ochsner KN (2012). The development of emotion regulation: An fMRI study of cognitive reappraisal in children, adolescents, and young adults. Social Cognitive and Affective Neuroscience, 7, 11–22. https://doi:10.1093/scan/nsr093 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McRae K, Hughes B, Chopra S, Gabrieli JDE, Gross JJ, & Ochsner KN (2010). The neural bases of distraction and reappraisal. Journal of Cognitive Neuroscience, 22, 248–262. https://doi:10.1162/jocn.2009.21243 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McRae K, & Mauss IB (2016). Increasing positive emotion in negative contexts: Emotional consequences, neural correlates, and implications for resilience Positive neuroscience (pp. 159–174), Greene JD, Morrison I, & Seligman MEP (Ed). New York: Oxford University Press, 2016. [Google Scholar]
- *.Miers AC, Rieffe C, Terwogt MM, Cowan R, & Linden W (2007). The relation between anger coping strategies, anger mood and somatic complaints in children and adolescents. Journal of Abnormal Child Psychology, 35, 653–664. https://doi:10.1007/s10802-007-9120-9 [DOI] [PubMed] [Google Scholar]
- *.Miller KS, Vannatta K, Compas BE, Vasey M, McGoron KD, Salley CG, & Gerhardt CA (2009). The role of coping and temperament in the adjustment of children with cancer. Journal of Pediatric Psychology, 34, 1135–1143. https://doi:10.1093/jpepsy/jsp037 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Molina BS, Sala MN, Zappulla C, Bonfigiuli C, Cavioni V,…..& Cicchetti D (2014). The Emotion Regulation Checklist—Italian Translation: Validation of parent and teacher versions. European Journal of Developmental Psychology, 11, 624–634. 10.1080/17405629.2014.898581 [DOI] [Google Scholar]
- *.Molock SD, Puri R, Matlin S, & Barksdale C (2006). Relationship between religious coping and suicidal behaviors among African American adolescents. Journal of Black Psychology, 32, 366–389. https://doi:10.1177/0095798406290466 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Monopoli JW, & Kingston S (2012). The relationships among language ability, emotion regulation and social competence in second-grade students. International Journal of Behavioral Development, 36, 398–405. https://doi:10.1177/0165025412446394 [Google Scholar]
- *.Morris AS, & Age TR (2009). Adjustment among youth in military families: The protective roles of effortful control and maternal social support. Journal of Applied Developmental Psychology, 30, 695–707. https://doi:10.1016/j.appdev.2009.01.002 [Google Scholar]
- Morris AS, Silk JS, Morris MD, Steinberg L, Aucoin KJ, & Keyes AW (2011). The influence of mother-child emotion regulation strategies on children’s expression of anger and sadness. Developmental Psychology, 47, 213 10.1037/a0021021 [DOI] [PubMed] [Google Scholar]
- *.Mosher CE, & Prelow HM (2007). Active and avoidant coping and coping efficacy as mediators of the relation of maternal involvement to depressive symptoms among urban adolescents. Journal of Child and Family Studies, 16, 876–887. https://doi:10.1007/s10826-007-9132-7 [Google Scholar]
- *.Murdock KK, Greene C, Adams SK, Hartmann W, Bittinger S, & Will K (2010). The puzzle of problem-solving efficacy: Understanding anxiety among urban children coping with asthma-related and life stress. Anxiety, Stress & Coping: An International Journal, 23, 383–398. https://doi:10.1080/10615800903118049 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Muris P, Mayer B, Reinders E, & Wesenhagen C (2011). Person-related protective and vulnerability factors of psychopathology symptoms in non-clinical adolescents. Community Mental Health Journal, 47, 47–60. https://doi:10.1007/s10597-009-9249-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Muris P, Roelofs J, Meesters C, & Boomsma P (2004). Rumination and worry in nonclinical adolescents. Cognitive Therapy and Research, 28, 539–554. 10.1023/b:cotr.0000045563.66060.3e [DOI] [Google Scholar]
- *.Muris P, Schmidt H, Lambrichs R, & Meesters C (2001). Protective and vulnerability factors of depression in normal adolescents. Behaviour Research and Therapy, 39, 555–565. https://doi:10.1016/S0005-7967(00)00026-7 [DOI] [PubMed] [Google Scholar]
- *.Ng R, Ang RP, & Ho MR (2012). Coping with anxiety, depression, anger and aggression: The mediational role of resilience in adolescents. Child & Youth Care Forum, 41, 529–546. https://doi:10.1007/s10566-012-9182-x [Google Scholar]
- *.Nicolotti L, El-Sheikh M, & Whitson SM (2003). Children’s coping with marital conflict and their adjustment and physical health: Vulnerability and protective functions. Journal of Family Psychology, 17, 315–326. https://doi:10.1037/0893-3200.17.3.315 [DOI] [PubMed] [Google Scholar]
- Nolen-Hoeksema S, Wisco BE, & Lyubomirsky S (2008). Rethinking rumination. Perspectives on Psychological Science, 3, 400–424. https://doi:10.1111/j.1745-6924.2008.00088.x [DOI] [PubMed] [Google Scholar]
- Nolen-Hoeksema S (2012). Emotion regulation and psychopathology: The role of gender. Annual Review of Clinical Psychology, 8, 161–187. https://doi:10.1146/annurev-clinpsy-032511-143109 [DOI] [PubMed] [Google Scholar]
- Nolen-Hoeksema S, & Watkins ER (2011). A heuristic for developing transdiagnostic models of psychopathology explaining multifinality and divergent trajectories. Perspectives on Psychological Science, 6, 589–609. https://doi:10.1177/1745691611419672 [DOI] [PubMed] [Google Scholar]
- *.Ollendick TH, Langley AK, Jones RT, & Kephart C (2001). Fear in children and adolescents: Relations with negative life events, attributional style, and avoidant coping. Journal of Child Psychology and Psychiatry, 42, 1029–1034. https://doi:10.1111/1469-7610.00801 [PubMed] [Google Scholar]
- *.Orsmond GI, Kuo H, & Seltzer MM (2009). Siblings of individuals with an autism spectrum disorder: Sibling relationships and wellbeing in adolescence and adulthood. Autism, 13, 59–80. https://doi:10.1177/1362361308097119 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Osowiecki D, & Compas BE (1998). Psychological adjustment to cancer: Coping and control beliefs in young adult cancer patients. Cognitive Therapy and Research, 22, 483–499. [Google Scholar]
- Osowiecki DM, & Compas BE (1999). A prospective study of coping, perceived control and psychological adjustment to breast cancer. Cognitive Therapy and Research, 23, 169–180. [Google Scholar]
- Patterson JM, & McCubbin HI (1991). A-COPE: Adolescent coping orientation for problem experiences In Hamilton HI & McCubbin JM (Eds.), Family assessment inventories for research and practice (2nd ed., pp. 234–250). Madison: University of Wisconsin. [Google Scholar]
- Penela EC, Walker OL, Degnan KA, Fox NA, & Henderson HA (2015). Early behavioral inhibition and emotion regulation: Pathways toward social competence in middle childhood. Child Development, 86, 1227–1240. 10.1111/cdev.12384 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Penza-Clyve S, & Zeman J (2002). Initial validation of the Emotion Expression Scale for Children (EESC). Journal of Clinical Child and Adolescent Psychology, 31, 540–547. https://doi:10.1207/153744202320802205 [DOI] [PubMed] [Google Scholar]
- *.Phillips KFV, & Power MJ (2007). A new self-report measure of emotion regulation in adolescents: The Regulation of Emotions Questionnaire. Clinical Psychology & Psychotherapy, 14, 145–156. 10.1002/cpp.523 [DOI] [Google Scholar]
- *.Piko B (2001). Gender differences and similarities in adolescents’ ways of coping. The Psychological Record, 51, 223 10.2466/pr0.1994.74.1.115 [DOI] [Google Scholar]
- *.Pina AA, Villalta IK, Ortiz CD, Gottschall AC, Costa NM, & Weems CF (2008). Social support, discrimination, and coping as predictors of posttraumatic stress reactions in youth survivors of Hurricane Katrina. Journal of Clinical Child and Adolescent Psychology, 37, 564–574. https://doi:10.1080/15374410802148228 [DOI] [PubMed] [Google Scholar]
- Podsakoff PM, MacKenzie SB, & Podsakoff NP (2012). Sources of method bias in social science research and recommendations on how to control it. Annual Review of Psychology, 63, 539–569. https://doi:10.1146/annurev-psych-120710-100452 [DOI] [PubMed] [Google Scholar]
- *.Prakash K, & Coplan RJ (2003). Shy skaters? Shyness, coping, and adjustment outcomes in female adolescent figure skaters. Athletic Insight, 5, 1–19. [Google Scholar]
- Price RB, Allen KB, Silk JS, Ladouceur CD, Ryan ND, Dahl RE, … & Siegle GJ (2016). Vigilance in the laboratory predicts avoidance in the real world: A dimensional analysis of neural, behavioral, and ecological momentary data in anxious youth. Developmental Cognitive Neuroscience, 19, 128–136. 10.1016/j.dcn.2016.03.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rabiner DL, Lenhart L, & Lochman JE (1990). Automatic versus reflective social problem solving in relation to children’s sociometric status. Developmental Psychology, 26, 1010–1016. [Google Scholar]
- *.Raviv T, & Wadsworth ME (2010). The efficacy of a pilot prevention program for children and caregivers coping with economic strain. Cognitive Therapy and Research, 34, 216–228. https://doi:10.1007/s10608-009-9265-7 [Google Scholar]
- *.Rawana JS, & Ahola Kohut S (2012). Eating attitudes, coping styles, and peer victimization among adolescents with seasonal and nonseasonal depression symptoms. Cognitive Therapy and Research, 36, 199–209. https://doi:10.1007/s10608-010-9333-z [Google Scholar]
- Reising M, Bettis A, Dunbar J, Watson K, Gruhn M, Hoskinson K, & Compas B (2017, in press). Stress, coping, executive function, and brain activation in adolescent offspring of depressed and non-depressed mothers. Child Neuropsychology. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Reschly AL, Huebner ES, Appleton JJ, & Antaramian S (2008). Engagement as flourishing: The contribution of positive emotions and coping to adolescents’ engagement at school and with learning. Psychology in the Schools, 45, 419–431. https://doi:10.1002/pits.20306 [Google Scholar]
- Rescorla LA, Ginzburg S, Achenbach TM, Ivanova MY, Almqvist F, Begovac I, … & Döpfner M (2013). Cross-informant agreement between parent-reported and adolescent self-reported problems in 25 societies. Journal of Clinical Child & Adolescent Psychology, 42, 262–273. https://doi:10.1080/15374416.2012.717870 [DOI] [PubMed] [Google Scholar]
- Rescorla L, Ivanova MY, Achenbach TM, Begovac I, Chahed M, Drugli MB, … & Zhang EY (2012). International epidemiology of child and adolescent psychopathology II: Integration and applications of dimensional findings from 44 societies. Journal of the American Academy of Child & Adolescent Psychiatry, 51, 1273–1283. https://doi:10.1016/j.jaac.2012.09.012 [DOI] [PubMed] [Google Scholar]
- Rhee SH, Lahey BB, & Waldman ID (2015). Comorbidity among dimensions of childhood psychopathology: Converging evidence from behavior genetics. Child Development Perspectives, 9, 26–31. https://doi:10.1111/cdep.12102 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Rhoades GK, McIntosh DN, Wadsworth ME, Ahlkvist JA, Burwell RA, Gudmundsen GR, … Rea JG (2007). Forgiving the September 11th terrorists: Associations with coping, psychological distress, and religiosity. Anxiety, Stress & Coping: An International Journal, 20, 109–128. https://doi:10.1080/10615800701195405 [DOI] [PubMed] [Google Scholar]
- *.Rieffe C, Oosterveld P, Miers AC, Terwogt MM, & Ly V (2008). Emotion awareness and internalising symptoms in children and adolescents: The emotion awareness questionnaire revised. Personality and Individual Differences, 45, 756–761. https://doi:10.1016/j.paid.2008.08.001 [Google Scholar]
- Robles TF, Slatcher RB, Trombello JM, & McGinn MM (2014). Marital quality and health: A meta-analytic review. Psychological Bulletin, 140, 140–187. https://doi:10.1037/a0031859 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robinson KE, Pearson MM, Cannistraci CJ, Anderson AW, Kuttesch JF … & Compas BE (2015). Functional neuroimaging of working memory in survivors of childhood brain tumors and healthy children: Associations with coping and psychosocial outcomes. Child Neuropsychology, 21, 779–802. 10.1080/09297049.2014.924492 [DOI] [PubMed] [Google Scholar]
- *.Roelofs J, Rood L, Meesters C, Te Dorsthorst V, Bögels S, Alloy LB, & Nolen-Hoeksema S (2009). The influence of rumination and distraction on depressed and anxious mood: A prospective examination of the response styles theory in children and adolescents. European Child & Adolescent Psychiatry, 18, 635–642. 10.1007/s00787-009-0026-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosenthal R (1979). The “file drawer problem” and tolerance for null results. Psychological Bulletin, 86, 638–641. 10.1037/0033-2909.86.3.638 [DOI] [Google Scholar]
- Rueger SY, Malecki CK, Pyun Y, Aycock C, & Coyle S (2016). A meta-analytic review of the association between perceived social support and depression in childhood and adolescence. Psychological Bulletin, 142, 1017–1067. https://doi:10.1037/bul0000058 [DOI] [PubMed] [Google Scholar]
- Rudolph KD, Dennig MD, & Weisz JR (1995). Determinants and consequences of children’s coping in the medical setting: conceptualization, review, and critique. Psychological Bulletin, 118(3), 328 10.1037//0033-2909.118.3.328 [DOI] [PubMed] [Google Scholar]
- *.Rudolph KD, & Troop-Gordon W (2010). Personal-accentuation and contextual-amplification models of pubertal timing: Predicting youth depression. Development and Psychopathology, 22, 433–451. https://doi:10.1017/S0954579410000167 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rutter M, Bishop D, Pine D, Scott S, Stevenson JS, Taylor EA, & Thapar A (2011). Rutter’s child and adolescent psychiatry. John Wiley & Sons. [Google Scholar]
- *.Sandstrom MJ (2004). Pitfalls of the peer world: How children cope with common rejection experiences. Journal of Abnormal Child Psychology, 32, 67–81. https://doi:10.1023/B:JACP.0000007581.95080.8b [DOI] [PubMed] [Google Scholar]
- Santucci AK, Silk JS, Shaw DS, Gentzler A, Fox NA, & Kovacs M (2008). Vagal tone and temperament as predictors of emotion regulation strategies in young children. Developmental Psychobiology, 50, 205–216. 10.1002/dev.20283 [DOI] [PubMed] [Google Scholar]
- Scheier MF, Weinbtraub JK, & Carver CS (1986). Coping with stress: Divergent strategies of optimists and pessimists. Journal of Personality and Social Psychology, 51, 1257–1264. 10.1037//0022-3514.51.6.1257 [DOI] [PubMed] [Google Scholar]
- *.Schiff M (2006). Living in the shadow of terrorism: Psychological distress and alcohol use among religious and non-religious adolescents in Jerusalem. Social Science & Medicine, 62, 2301–2312. https://doi:10.1016/j.socscimed.2005.10.016 [DOI] [PubMed] [Google Scholar]
- *.Schneider KM, & Phares V (2005). Coping with parental loss because of termination of parental rights. Child Welfare: Journal of Policy, Practice, and Program, 84, 819–842. [PubMed] [Google Scholar]
- Seeley JR, Kosty DB, Farmer RF, & Lewinsohn PM (2011). The modeling of internalizing disorders on the basis of patterns of lifetime comorbidity: associations with psychosocial functioning and psychiatric disorders among first-degree relatives. Journal of Abnormal Psychology, 120, 308–321. https://doi:10.1037/a0022621 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seiffge-Krenke I (1995). Stress, coping, and relationships in adolescence. Mahwah, NJ: Lawrence Erlbaum. [Google Scholar]
- Seiffge-Krenke I (2011). Coping with relationship stressors: A decade review. Journal of Research on Adolescence, 21, 196–210. https://doi:10.1111/j.1532-7795.2010.00723.x [Google Scholar]
- *.Seiffge-Krenke I, & Stemmler M (2002). Factors contributing to gender differences in depressive symptoms: A test of three developmental models. Journal of Youth and Adolescence, 31, 405–417. https://doi:10.1023/A:1020269918957 [Google Scholar]
- *.Šerek J, Lacinová L, & Macek P (2012). Does family experience influence political beliefs? Relation between interparental conflict perceptions and political efficacy in late adolescence. Journal of Adolescence, 35, 577–586. https://doi:10.1016/j.adolescence.2011.10.001 [DOI] [PubMed] [Google Scholar]
- Schäfer JO, Naumann E, Holmes EA, Tuschen-Caffier B, & Samson AC (2017). Emotion regulation strategies in depressive and anxiety symptoms in youth: A meta-analytic review. Journal of Youth and Adolescence, 46, 261–276. [DOI] [PubMed] [Google Scholar]
- *.Shelton KH, & Harold GT (2007). Marital conflict and children’s adjustment: The mediating and moderating role of children’s coping strategies. Social Development, 16, 497–512. https://doi:10.1111/j.1467-9507.2007.00400.x [Google Scholar]
- *.Shelton KH, & Harold GT (2008). Pathways between interparental conflict and adolescent psychological adjustment: Bridging links through children’s cognitive appraisals and coping strategies. The Journal of Early Adolescence, 28, 555–582. https://doi:10.1177/0272431608317610 [Google Scholar]
- Sheppes G, Suri G, & Gross JJ (2015). Emotion regulation and psychopathology. Annual Review of Clinical Psychology, 11, 379–405. 10.1146/annurev-clinpsy-032814-112739 [DOI] [PubMed] [Google Scholar]
- Shields A, & Cicchetti D (1997). Emotion regulation among school-age children: The development and validation of a new criterion Q-sort scale. Developmental Psychology, 33, 906–916. https://doi:10.1037/0012-1649.33.6.906 [DOI] [PubMed] [Google Scholar]
- *.Shirkey KC, Smith CA, & Walker LS (2011). Dispositional versus episode-specific assessment of children’s coping with pain. Journal of Pediatric Psychology, 36, 74–83. https://doi:10.1093/jpepsy/jsq058 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Siener S, & Kerns KA (2012). Emotion regulation and depressive symptoms in preadolescence. Child Psychiatry & Human Development, 43, 414–430. https://doi:10.1007/s10578-011-0274-x [DOI] [PubMed] [Google Scholar]
- *.Siffert A, & Schwarz B (2011). Parental conflict resolution styles and children’s adjustment: Children’s appraisals and emotion regulation as mediators. The Journal of Genetic Psychology: Research and Theory on Human Development, 172, 21–39. https://doi:10.1080/00221325.2010.503723 [DOI] [PubMed] [Google Scholar]
- *.Sim L, & Zeman J (2006). The contribution of emotion regulation to body dissatisfaction and disordered eating in early adolescent girls. Journal of Youth and Adolescence, 35, 219–228. https://doi:10.1007/s10964-005-9003-8 [Google Scholar]
- *.Simons LE, Claar RL, & Logan DL (2008). Chronic pain in adolescence: Parental responses, adolescent coping, and their impact on adolescent’s pain behaviors. Journal of Pediatric Psychology, 33, 894–904. https://doi:10.1093/jpepsy/jsn029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Skinner EA, & Wellborn JG (1994). Coping during childhood and adolescence: A motivational perspective In Featherman DL, Lerner RM, & Perlmutter M (Eds), Life-span development and behavior, Vol. 12 (pp. 91–133). Hillsdale, NJ, England: Lawrence Erlbaum Associates, Inc. [Google Scholar]
- Skinner EA, & Zimmer-Gembeck MJ (2007). The development of coping. Annual Review of Psychology, 58, 119–144. https://doi:10.1146/annurev.psych.58.110405.085705 [DOI] [PubMed] [Google Scholar]
- Skinner EA, & Zimmer-Gembeck MJ (2010). Perceived control and the development of coping. Oxford handbook of stress, health, and coping, 35–59. [Google Scholar]
- Skinner EA, Edge K, Altman J, & Sherwood H (2003). Searching for the structure of coping: A review and critique of category systems for classifying ways of coping. Psychological Bulletin, 129, 216–269. https://doi:10.1037/0033-2909.129.2.216 [DOI] [PubMed] [Google Scholar]
- *.Skočić M, Rudan V, Brajković L, & Marčinko D (2010). Relationship among psychopathological dimensions, coping mechanisms, and glycemic control in a Croatian sample of adolescents with diabetes mellitus type 1. European Child & Adolescent Psychiatry, 19, 525–533. https://doi:10.1007/s00787-009-0066-z [DOI] [PubMed] [Google Scholar]
- *.Smith CL, Eisenberg N, Spinrad TL, Chassin L, Morris AS, Kupfer A, … Kwok O (2006). Children’s coping strategies and coping efficacy: Relations to parent socialization, child adjustment, and familial alcoholism. Development and Psychopathology, 18, 445–469. https://doi:10.1017/S095457940606024X [DOI] [PubMed] [Google Scholar]
- *.Song S, Graham JE, Susman EJ, & Sohn YW (2012). The role of ineffective emotion regulation in problem drinking varies by emotional disposition, delinquency, and gender of South Korean adolescents. Journal of Child & Adolescent Substance Abuse, 21, 367–382. 10.1080/1067828x.2012.710029 [DOI] [Google Scholar]
- Sontag LM, & Graber JA (2010). Coping with perceived peer stress: Gender-specific and common pathways to symptoms of psychopathology. Developmental Psychology, 46, 1605–1620. [DOI] [PubMed] [Google Scholar]
- *.Sontag LM, Graber JA, Brooks-Gunn J, & Warren MP (2008). Coping with social stress: Implications for psychopathology in young adolescent girls. Journal of Abnormal Child Psychology, 36, 1159–1174. https://doi:10.1007/s10802-008-9239-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spirito A, Stark LJ, & Williams C (1988). Development of a brief coping checklist for use with pediatric populations. Journal of Pediatric Psychology, 13, 555–574. 10.1093/jpepsy/13.4.555 [DOI] [PubMed] [Google Scholar]
- *.Steele RG, Legerski J, Nelson TD, & Phipps S (2009). The anger expression scale for children: Initial validation among healthy children and children with cancer. Journal of Pediatric Psychology, 34, 51–62. https://doi:10.1093/jpepsy/jsn054 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stephanou K, Davey CG, Kerestes R, Whittle S, Pujol J, Yücel M, … & Harrison BJ (2016). Brain functional correlates of emotion regulation across adolescence and young adulthood. Human Brain Mapping, 37(1), 7–19. 10.1002/hbm.22905 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stone LB, Hankin BL, Gibb BE, & Abela JR (2011). Co-rumination predicts the onset of depressive disorders during adolescence. Journal of Abnormal Psychology, 120, 752 10.1037/a0023384 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Sullivan TN, Helms SW, Kliewer W, & Goodman KL (2010). Associations between sadness and anger regulation coping, emotional expression, and physical and relational aggression among urban adolescents. Social Development, 19, 30–51. https://doi:10.1111/j.1467-9507.2008.00531.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Sung KM, Puskar KR, & Sereika S (2006). Psychosocial factors and coping strategies of adolescents in a rural Pennsylvania high school. Public Health Nursing, 23, 523–530. https://doi:10.1111/j.1525-1446.2006.00589.x [DOI] [PubMed] [Google Scholar]
- *.Suveg C, Shaffer A, Morelen D, & Thomassin K (2011). Links between maternal and child psychopathology symptoms: Mediation through child emotion regulation and moderation through maternal behavior. Child Psychiatry and Human Development, 42, 507–520. https://doi:10.1007/s10578-011-0223-8 [DOI] [PubMed] [Google Scholar]
- Sveinbjornsdottir S, & Thorsteinsson EB (2014). Psychometric properties of the Measure of Adolescent Coping Strategies (MACS). Psychology, 5, 142–147. https://doi:10.4236/psych.2014.52022 [Google Scholar]
- *.Tam VC (2008). Coping profiles among Chinese adolescents in Hong Kong: A person-centered approach. International Journal of Adolescent Medicine and Health, 20, 73–83. https://doi:10.1515/IJAMH.2008.20.1.73 [DOI] [PubMed] [Google Scholar]
- *.Tam VC, & Lam RS (2005). Stress and coping among migrant and local-born adolescents in Hong Kong. Youth & Society, 36(3), 312–332. https://doi:10.1177/0044118X04265092 [Google Scholar]
- Tan PZ, Forbes EE, Dahl RE, Ryan ND, Siegle GJ, Ladouceur CD, & Silk JS (2012). Emotional reactivity and regulation in anxious and nonanxious youth: A cell-phone ecological momentary assessment study. Journal of Child Psychology and Psychiatry, 53(2), 197–206. 10.1111/j.1469-7610.2011.02469.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tein JY, Sandler IN, Ayers TS, & Wolchik SA (2006). Mediation of the effects of the Family Bereavement Program on mental health problems of bereaved children and adolescents. Prevention Science, 7, 179–195. https://doi:10.1007/s11121-006-0037-2 [DOI] [PubMed] [Google Scholar]
- Tein JY, Sandler IN, MacKinnon DP, & Wolchik SA (2004). How did it work? Who did it work for? Mediation in the context of a moderated prevention effect for children of divorce. Journal of Consulting and Clinical Psychology, 72, 617–624. https://doi:10.1037/0022-006X.72.4.617 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thompson RA (1991). Emotional regulation and emotional development. Educational Psychology Review, 3, 269–307. https://doi:1040-726X/91/1200-0269506.50 [Google Scholar]
- Thompson RA (1994). Emotion regulation: A theme in search of definition In Fox NA (Ed.), The development of emotion regulation: Biological and behavioral considerations. Monographs of the Society for Research in Child Development, 59(2–3, Serial No. 240), 25–52. https://doi:10.2307/1166137 [PubMed] [Google Scholar]
- Thompson RA, & Calkins SD (1996). The double-edged sword: Emotional regulation for children at risk. Development and Psychopathology, 8, 163–182. https://doi:10.1017/S0954579400007021 [Google Scholar]
- Thompson RA, & Goodman M (2010). Development of emotion regulation: More than meets the eye In Kring AM & Sloan DM (Eds.), Emotion regulation and psychopathology: A transdiagnostic approach to etiology and treatment (pp. 38–58). New York, NY: Guilford. [Google Scholar]
- *.Thompson RJ, Mata J, Jaeggi SM, Buschkuehl M, Jonides J, & Gotlib IH (2010). Maladaptive coping, adaptive coping, and depressive symptoms: Variations across age and depressive state. Behaviour Research and Therapy, 48, 459–466. https://doi:10.1016/j.brat.2010.01.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Thomsen AH, Compas BE, Colletti RB, Stanger C, Boyer MC, & Konik BS (2002). Parent reports of coping and stress responses in children with recurrent abdominal pain. Journal of Pediatric Psychology, 27, 215–226. https://doi:10.1093/jpepsy/27.3.215 [DOI] [PubMed] [Google Scholar]
- *.Thuen E, & Bru E (2004). Coping styles and emotional and behavioural problems among Norwegian grade 9 students. Scandinavian Journal of Educational Research, 48, 493–510. https://doi:10.1080/003138042000272140 [Google Scholar]
- *.Tompkins TL, Hockett AR, Abraibesh N, & Witt JL (2011). A closer look at co-rumination: Gender, coping, peer functioning and internalizing/externalizing problems. Journal of Adolescence, 34, 801–811. https://doi:10.1016/j.adolescence.2011.02.005 [DOI] [PubMed] [Google Scholar]
- Troy AS, Ford BQ, McRae K, Zarolia P, & Mauss IB (2016). Change the Things You Can: Emotion Regulation Is More Beneficial for People From Lower Than From Higher Socioeconomic Status Emotion (Washington, DC: ). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Troy AS, Shallcross AJ, & Mauss IB (2013). A person-by-situation approach to emotion regulation cognitive reappraisal can either help or hurt, depending on the context. Psychological Science, 24, 2505–2514. https://doi:10.1177/0956797613496434 [DOI] [PubMed] [Google Scholar]
- Troy AS, & Mauss IB (2011). Resilience in the face of stress: Emotion regulation as a protective factor. Resilience and mental health: Challenges across the lifespan, 30–44. [Google Scholar]
- *.van Dijk J, Grootenhuis MA, Imhof SM, Cohen-Kettenis P, Moll AC, & Huisman J (2009). Coping strategies of retinoblastoma survivors in relation to behavioural problems. Psycho-Oncology, 18, 1281–1289. https://doi:10.1002/pon.1507 [DOI] [PubMed] [Google Scholar]
- *.Van Dyke CJ, Glenwick DS, Cecero JJ, & Kim S (2009). The relationship of religious coping and spirituality to adjustment and psychological distress in urban early adolescents. Mental Health, Religion & Culture, 12, 369–383. https://doi:10.1080/13674670902737723 [Google Scholar]
- *.Vasilev CA, Crowell SE, Beauchaine TP, Mead HK, & Gatzke-Kopp L (2009). Correspondence between physiological and self-report measures of emotion dysregulation: A longitudinal investigation of youth with and without psychopathology. Journal of Child Psychology and Psychiatry, 50, 1357–1364. https://doi:10.1111/j.1469-7610.2009.02172.x [DOI] [PubMed] [Google Scholar]
- *.Vaughn AA, & Roesch SC (2003). Psychological and physical health correlates of coping in minority adolescents. Journal of Health Psychology, 8, 671–683. https://doi:10.1177/13591053030086002 [DOI] [PubMed] [Google Scholar]
- *.Vigna JF, Hernandez BC, Kelley ML, & Gresham FM (2010). Coping behavior in hurricane-affected African American youth: Psychometric properties of the Kidcope. Journal of Black Psychology, 36, 98–121. https://doi:10.1177/0095798408329948 [Google Scholar]
- *.Visconti KJ, & Troop-Gordon W (2010). Prospective relations between children’s responses to peer victimization and their socioemotional adjustment. Journal of Applied Developmental Psychology, 31, 261–272. https://doi:10.1016/j.appdev.2010.05.003 [Google Scholar]
- *.Votta E, & Manion IG (2003). Factors in the psychological adjustment of homeless adolescent males: The role of coping style. Journal of the American Academy of Child & Adolescent Psychiatry, 42, 778–785. https://doi:10.1097/01.CHI.0000046871.56865.D9 [DOI] [PubMed] [Google Scholar]
- *.Votta E, & Manion I (2004). Suicide, high-risk behaviors, and coping style in homeless adolescent males’ adjustment. Journal of Adolescent Health, 34, 237–243. https://doi:10.1016/j.jadohealth.2003.06.002 [DOI] [PubMed] [Google Scholar]
- *.Vulic-Prtorić A, & Macuka I (2006). Family and coping factors in the differentiation of childhood anxiety and depression. Psychology and Psychotherapy: Theory, Research and Practice, 79, 199–214. https://doi:10.1348/147608305X52676 [DOI] [PubMed] [Google Scholar]
- Wadsworth ME (2015). Development of maladaptive coping: A functional adaptation to chronic, uncontrollable stress. Child Development Perspectives, 9(2), 96–100. 10.1111/cdep.12112 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Wadsworth ME, & Berger LE (2006). Adolescents coping with poverty-related family stress: Prospective predictors of coping and psychological symptoms. Journal of Youth and Adolescence, 35, 57–70. https://doi:10.1007/s10964-005-9022-5 [Google Scholar]
- *.Wadsworth ME, & Compas BE (2002). Coping with family conflict and economic strain: The adolescent perspective. Journal of Research on Adolescence, 12, 243–274. https://doi:10.1111/1532-7795.00033 [Google Scholar]
- *.Wadsworth ME, & Santiago CD (2008). Risk and resiliency processes in ethnically diverse families in poverty. Journal of Family Psychology, 22, 399–410. https://doi:10.1037/0893-3200.22.3.399 [DOI] [PubMed] [Google Scholar]
- *.Wadsworth ME, Raviv T, Compas BE, & Connor-Smith J (2005). Parent and adolescent responses to poverty-related stress: Tests of mediated and moderated coping models. Journal of Child and Family Studies, 14, 283–298. https://doi:10.1007/s10826-005-5056-2 [Google Scholar]
- *.Wadsworth ME, Rieckmann T, Benson MA, & Compas BE (2004). Coping and responses to stress in Navajo adolescents: Psychometric properties of the Responses to Stress Questionnaire. Journal of Community Psychology, 32, 391–411. https://doi:10.1002/jcop.20008 [Google Scholar]
- Wadsworth ME, Rindlaub L, Hurwich-Reiss E, Rienks S, Bianco H, & Markman HJ (2013). A longitudinal examination of the adaptation to poverty-related stress model: Predicting child and adolescent adjustment over time. Journal of Clinical Child & Adolescent Psychology, 42(5), 713–725. [DOI] [PubMed] [Google Scholar]
- *.Wagner JL, Ferguson PL, & Smith G (2012). The relationship of coping behaviors to depressive symptoms in youth with epilepsy: An examination of caregiver and youth proxy report. Epilepsy & Behavior, 24, 86–92. https://doi:10.1016/j.yebeh.2012.02.017 [DOI] [PubMed] [Google Scholar]
- *.Walker LS, Smith CA, Garber J, & Claar RL (2005). Testing a model of pain appraisal and coping in children with chronic abdominal pain. Health Psychology, 24, 364–374. https://doi:10.1037/0278-6133.24.4.364 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Walker LS, Smith CA, Garber J, & Claar RL (2007). Appraisal and coping with daily stressors by pediatric patients with chronic abdominal pain. Journal of Pediatric Psychology, 32, 206–216. https://doi:10.1093/jpepsy/jsj124 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walker LS, Smith CA, Garber J, & Van Slyke DA (1997). Development and validation of the pain response inventory for children. Psychological Assessment, 9, 392–405. https://doi:10.1037/1040-3590.9.4.392 [Google Scholar]
- *.Wang Z, & Gan Y (2011). Coping mediates between social support, neuroticism, and depression after earthquake and examination stress among adolescents. Anxiety, Stress, & Coping, 24, 343–358. 10.1080/10615806.2010.515026 [DOI] [PubMed] [Google Scholar]
- Webb TL, Miles E, & Sheeran P (2012). Dealing with feeling: A meta-analysis of the effectiveness of strategies derived from the process model of emotion regulation. Psychological Bulletin, 138, 775–808. 10.1037/a0027600 [DOI] [PubMed] [Google Scholar]
- Webb TL, Gallo IS, Miles E, Gollwitzer PM, & Sheeran P (2012). Effective regulation of affect: An action control perspective on emotion regulation. European Review of Social Psychology, 23, 143–186. 10.1080/10463283.2012.718134 [DOI] [Google Scholar]
- *.Weinberg A, & Klonsky ED (2009). Measurement of emotion dysregulation in adolescents. Psychological Assessment, 21, 616–621. https://doi:10.1037/a0016669 [DOI] [PubMed] [Google Scholar]
- Weisz JR, McCabe MA, & Dennig MD (1994). Primary and secondary control among children undergoing medical procedures: Adjustment as a function of coping style. Journal of Consulting and Clinical Psychology, 62, 324–332. https://doi:10.1037/0022-006X.62.2.324 [DOI] [PubMed] [Google Scholar]
- *.Wills TA, Sandy JM, & Yaeger AM (2002). Moderators of the relation between substance use level and problems: Test of a self-regulation model in middle adolescence. Journal of Abnormal Psychology, 111, 3–21. https://doi:10.1037/0021-843X.111.1.3 [PubMed] [Google Scholar]
- *.Wills TA, Sandy JM, Yaeger AM, Cleary SD, & Shinar O (2001). Coping dimensions, life stress, and adolescent substance use: A latent growth analysis. Journal of Abnormal Psychology, 110, 309–323. https://doi:10.1037/0021-843X.110.2.309 [DOI] [PubMed] [Google Scholar]
- *.Wilson GS, Pritchard ME, & Revalee B (2005). Individual differences in adolescent health symptoms: The effects of gender and coping. Journal of Adolescence, 28, 369–379. https://doi:10.1016/j.adolescence.2004.08.004 [DOI] [PubMed] [Google Scholar]
- *.Wolfradt U, Hempel S, & Miles JNV (2003). Perceived parenting styles, depersonalisation, anxiety and coping behavior in adolescents. Personality and Individual Differences, 34, 521–532. https://doi:10.1016/S0191-8869(02)00092-2 [Google Scholar]
- *.Wright M, Banerjee R, Hoek W, Rieffe C, & Novin S (2010). Depression and social anxiety in children: Differential links with coping strategies. Journal of Abnormal Child Psychology, 38, 405–419. https://doi:10.1007/s10802-009-9375-4 [DOI] [PubMed] [Google Scholar]
- *.Wu LM, Chin CC, Chen CH, Lai FC, & Tseng YY (2011). Development and validation of the paediatric cancer coping scale. Journal of Advanced Nursing, 67, 1142–1151. https://doi:10.1111/j.1365-2648.2010.05567.x [DOI] [PubMed] [Google Scholar]
- *.Xiao J, Yao S, Zhu X, Zhang C, Auerbach RP, McWhinnie CM, & Abela JRZ (2010). The responses to stress questionnaire: Construct validity and prediction of depressive and social anxiety symptoms in a sample of Chinese adolescents. Stress and Health: Journal of the International Society for the Investigation of Stress, 26, 238–249. https://doi:10.1002/smi.1291 [Google Scholar]
- Zahn-Waxler C, Shirtcliff EA, & Marceau K (2008). Disorders of childhood and adolescence: Gender and psychopathology. Annual Review of Clinical Psychology, 4, 275–303. [DOI] [PubMed] [Google Scholar]
- Zalewski M, Lengua LJ, Wilson AC, Trancik A, & Bazinet A (2011). Associations of coping and appraisal styles with emotion regulation during preadolescence. Journal of Experimental Child Psychology, 110, 141–158. https://doi:10.1016/j.jecp.2011.03.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Zaremba LA, & Keiley MK (2011). The mediational effect of affect regulation on the relationship between attachment and internalizing/externalizing behaviors in adolescent males who have sexually offended. Children and Youth Services Review, 33, 1599–1607. https://doi:10.1016/j.childyouth.2011.04.001 [Google Scholar]
- *.Zehnder D, Prchal A, Vollrath M, & Landolt MA (2006). Prospective study of the effectiveness of coping in pediatric patients. Child Psychiatry and Human Development, 36, 351–368. https://doi:10.1007/s10578-005-0007-0 [DOI] [PubMed] [Google Scholar]
- *.Zeidner M (2005). Contextual and personal predictors of adaptive outcomes under terror attack: The case of Israeli adolescents. Journal of Youth and Adolescence, 34, 459–470. https://doi:10.1007/s10964-005-7263-y [Google Scholar]
- *.Zeman JL, Cassano M, Suveg C, & Shipman K (2010). Initial validation of the Children’s Worry Management Scale. Journal of Child and Family Studies, 19, 381–392. https://doi:10.1007/s10826-009-9308-4 [Google Scholar]
- *.Zeman J, Shipman K, & Penza-Clyve S (2001). Development and initial validation of the children’s sadness management scale. Journal of Nonverbal Behavior, 25, 187–205. https://doi:10.1023/A:1010623226626 [Google Scholar]
- Zeman J, Shipman K, & Suveg C (2002). Anger and sadness regulation: Predictions to internalizing and externalizing symptoms in children. Journal of Clinical Child and Adolescent Psychology, 31, 393–398. https://doi:10.1207/153744202760082658 [DOI] [PubMed] [Google Scholar]
- Zhou Q, Chen SH, & Main A (2012). Commonalities and differences in the research on children’s effortful control and executive function: a call for an integrated model of self-regulation. Child Development Perspectives, 6, 112–121. 10.1111/j.1750-8606.2011.00176.x [DOI] [Google Scholar]
- *.Zhou T, Wu D, & Lin L (2012). On the intermediary function of coping styles: Between self-concept and subjective well being of adolescents of Han, Qiang and Yi nationalities. Psychology, 3, 136 10.4236/psych.2012.32021 [DOI] [Google Scholar]
- Zimmer-Gembeck MJ, Dunbar MJ, Ferguson S, Rowe SL, Webb H, & Skinner EA (2014). Guest editorial: Introduction to special issue. Australian Journal of Psychology, 66, 65–70. 10.1111/ajpy.12056 [DOI] [Google Scholar]
- Zimmer-Gembeck MJ, & Skinner EA (2011). The development of coping across childhood and adolescence: An integrative review and critique of research. International Journal of Behavioral Development, 35, 1–17. https://doi:10.1177/0165025410384923 [Google Scholar]
- Zimmer-Gembeck MJ, & Skinner EA (2016). The development of coping: Implications for psychopathology and resilience In Cicchetti D (Ed.), Developmental Psychopathology. Oxford, England: Wiley & Sons. [Google Scholar]
- Zimmer-Gembeck MJ, & Skinner EA (2011). The development of coping across childhood and adolescence: An integrative review and critique of research. International Journal of Behavioral Development, 35, 1–17. https://doi:10.1177/0165025410384923 [Google Scholar]