

Abstract
Background
There is ample evidence to suggest sex- and gender-based differences in the incidence of sports-related concussions. The mechanisms of concussion may vary between male and female athletes and contribute to this observed difference. Understanding the underlying etiology by pooling data from primary studies across different settings and sport types will inform interventions that can reduce concussion rates.
Questions/purposes
Specifically, we asked: (1) In which sports are female athletes less likely to experience concussions from player contact? (2) In which sports are female athletes more likely to experience concussions because of ball or equipment contact?
Methods
PubMed, EMBASE, and Cochrane Library databases were searched to identify articles published from January 2000 to December 2018. Ten studies met the inclusion criteria, which were studies that reported concussion incidence by mechanism for both male and female athletes. Exclusion criteria included non-English studies, conference abstracts, and studies on non-sports related concussions. The sports represented by the 10 studies included ice hockey (n = 4), soccer (n = 5), basketball (n = 4), baseball/softball (n = 4), and lacrosse (n = 5). The rate ratio was calculated as the incidence rate in female athletes/male athletes for each concussion mechanism or activity. Data were pooled using the DerSimonian-Laird random-effects model. Study quality was assessed with the Newcastle-Ottawa Scale.
Results
Female athletes were at lower risk of player-contact-induced concussions in lacrosse (pooled rate ratio 0.33 [95% CI 0.25 to 0.43]; p < 0.001), basketball (pooled rate ratio 0.86 [95% CI 0.76 to 0.97]; p = 0.01), ice hockey (pooled rate ratio 0.64 [95% CI 0.56 to 0.73]; p < 0.001), soccer (pooled rate ratio 0.70 [95% CI 0.66 to 0.75]; p < 0.001), and soccer heading (pooled rate ratio 0.80 [95% CI 0.72 to 0.90]; p < 0.001); in these sports, men were at higher risk of concussions from player contact. Female athletes were more likely to experience concussions because of ball or equipment contact in lacrosse (pooled rate ratio 3.24 [95% CI 2.10 to 4.99]; p < 0.001), soccer (pooled rate ratio 2.04 [95% CI 1.67 to 2.49]; p < 0.001), and soccer heading (pooled rate ratio 2.63 [95% CI 1.84 to 3.77]; p < 0.001).
Conclusions
The mechanism or activity underlying concussions differs between male and female athletes across different sports. This finding remains the same regardless of whether there are rule differences between the men’s and women’s games. The implementation of other interventions are required to further ensure player safety, including protective head equipment, concussion prevention training, or rules limiting player contact in the men’s game.
Level of Evidence
Level III, retrospective study.
Introduction
Although sports-related concussions may occur in contact and non-contact sports, the highest incidence is in contact sports that involve frequent collisions, such as soccer and basketball [17, 18]. The mechanisms by which concussions occur may differ by sport and position, but the most common mechanism of injury is player-to-player contact [23]. In a soccer study, Chandran et al. [5] reported a 2.5 times greater risk of head injuries from player-to-player contact than from other mechanisms, such as contact with the ball, goalpost, or soccer field. In non-contact sports, there is greater variation in the mechanism of concussion by sport. Many recent studies have reported on the incidence of concussions in various sports [3, 29, 34], and there is sufficient evidence suggesting that sex-based differences affect concussion rates. We previously performed a meta-analysis comparing the incidence of concussion between male and female athletes in different sports [6].
In addition to the incidence of concussion, injury mechanisms have been shown to differ between male and female athletes [21]. Female athletes are more likely to incur a head injury because of contact with a playing surface or an apparatus than men, while male athletes are more likely to be injured by contact with another player [5]. In the context of concussions, it is important to address biological sex and societal gender because certain behaviors may contribute to health disparities. Differences in injury mechanism between male and female athletes could be due to both differences in physiology and/or differences in the way they play the sport. Our first meta-analysis included 38 studies that reported sex-based differences in the incidence of concussions. Although there is ample evidence describing the problem, there has been no meta-analysis on sex or gender differences for the concussion mechanism or activity across different types of sports. This evidence would help provide reasons behind the growing health problem of sports-related concussions. An understanding of the underlying etiology by pooling data from primary studies across different settings and sport types will inform the development of interventions that can actually reduce concussion rates.
We therefore conducted a systematic review and meta-analysis in which we asked: (1) In which sports are female athletes less likely to experience concussions from player contact? (2) In which sports are female athletes more likely to experience concussions because of ball or equipment contact?
Materials and Methods
Search Strategy and Criteria
A medical librarian (BJ) performed a comprehensive search of the PubMed, EMBASE, and Cochrane Library databases according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [26]. Search terms were “sex,” “gender,” “sex differences,” “gender identity,” “brain concussion,” “concussion,” “traumatic brain injury,” “sports,” “athletes,” “incidence,” “epidemiology,” “symptoms,” and “injury rate” (see Supplemental Digital Content 1, http://links.lww.com/CORR/A240).
Studies published between January 2000 and December 2018 were included if they reported the incidence of concussion and the sport mechanism or activity for both male and female athletes so that we could perform head-to-head sex and gender comparisons. Other potential studies were identified by manually searching the reference lists of included studies and relevant review articles. Studies were excluded if they were not published in English, reported data on non-sports-related concussions (for example, emergency room settings), or were conference abstracts (grey literature). Two co-authors (JC, KS) independently screened titles and abstracts and reviewed the full text of the article. Any disagreements were resolved through consensus or by a third reviewer (DL). We assessed the quality of studies using the Newcastle-Ottawa Scale for cohort studies [31]. A score was given to each of the following categories: selection, comparability, and outcome. Scores per category were then summed to determine quality.
The following data were independently extracted from full-text articles: type of sport, incidence of concussion, mechanism of concussion (contact with player, surface, ball, or equipment), activity when the concussion occurred (for example, heading, fielding, shooting), population (university or high school), and database used. Each study in the meta-analysis contributed at least two pairs of numbers: the number of concussions in male and female athletes and the total number of male and female athletes. The rate ratio was calculated as the rate of concussions in female athletes/rate of concussions in male athletes. A value greater than 1 indicated that women experienced more concussions than men, while a value less than 1 indicated that men had a higher incidence of concussion. For studies that reported the incidence of concussion for multiple sports or for a different mechanism or activity, data were extracted separately. Thus, some studies contributed multiple sex and gender comparisons to the meta-analysis.
Ten studies were included in the meta-analysis [1, 8, 16, 22, 24, 27, 28, 30, 36, 37]. The PRISMA flowchart includes the search strategy and reasons for exclusion (Fig. 1). All studies were retrospective and used a high school or collegiate national injury surveillance database such as the National Collegiate Athletic Association-Injury Surveillance Program, High School Reporting Information Online, or National Athletic Treatment, Injury, and Outcomes Network (Table 1). The highest number of sex comparisons were found for soccer. Four studies reported concussion data for multiple sports and thus contributed multiple sex comparisons. Track and field, volleyball, and swimming and diving were excluded from the analysis because of a low incidence of concussion (five or fewer). Meta-analyses were conducted for lacrosse, soccer, baseball and softball, basketball, and ice hockey.
Fig. 1.
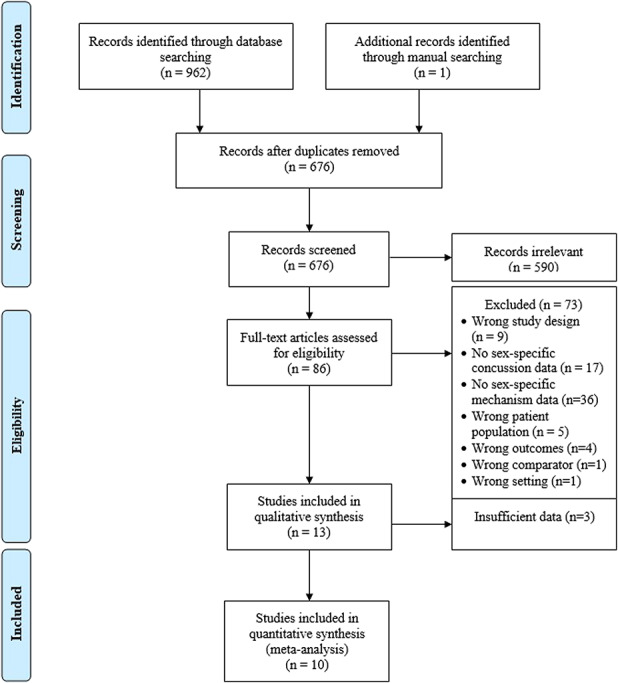
The inclusion and exclusion of studies is shown in this PRISMA flow diagram.
Table 1.
Characteristics of studies included in the meta-analysis

All 10 included studies were rated as having fair quality, due to the retrospective design of the studies and because the outcome of interest (the incidence of concussion) was present at the start of the study, which can lead to misclassification of the outcome or exposure (sports participation) (see Supplemental Digital Content 2, http://links.lww.com/CORR/A241).
Data from each study were pooled using the DerSimonian-Laird random-effects model in StataSE version 14 (Stata Corp, College Station, TX, USA). In the presence of heterogeneity, the random-effects model gives more conservative estimates with wider confidence intervals than fixed-effects models because it assumes that the meta-analysis includes only a sample of all possible studies [20]. In addition, the random-effects model accounts for within-study variability (random error) and between-study variability (heterogeneity). Separate meta-analyses were performed for each sport. Summary estimates of the rate ratio comparing women and men were calculated for each of the three concussion mechanisms: contact with another player, playing surface, or ball or equipment. When data were available, the pooled rate ratio was also reported for the sport-specific activity resulting in the concussion. The rate ratio for each comparison and the 95% CI are displayed in forest plots.
Results
Sports with a Lower Risk of Player Contact-induced Concussions in Female Athletes
Female athletes had a lower risk of concussions due to player contact in the sports of basketball, lacrosse, soccer, and ice hockey. Based on a small number of studies [26, 37], the pooled rate ratio estimates indicated that there were no differences between male baseball players and female softball players for concussions due to player contact (rate ratio 0.90 [95% CI 0.51 to 1.60]; p = 0.73). Male basketball players had a higher relative risk of concussion because of contact with another player (rate ratio 0.86 [95% CI 0.76 to 0.97]; p = 0.01). For basketball activity, no differences were found for defending, general play, or shooting (Fig. 2). Male basketball players were more likely to experience a concussion while rebounding than female players were (rate ratio 0.55 [95% CI 0.52 to 0.58]; p < 0.001). However, this estimate was based on only two studies [16, 37] and largely driven by Gessel et al. [16]. Male athletes had a higher relative risk of concussion due to player contact than female athletes in lacrosse (rate ratio 0.33 [95% CI 0.25 to 0.43]; p < 0.001) (Fig. 3), soccer (rate ratio 0.70 [95% CI 0.66 to 0.75]; p < 0.001) (Fig. 4), and ice hockey (rate ratio 0.64 [95% CI 0.56 to 0.73]; p < 0.001) (Fig. 5). Based on two studies [28, 30], the relative risk of concussions sustained while body-checking was higher in male hockey players than in female players (rate ratio 0.30 [95% CI 0.18 to 0.50]; p < 0.001). A few studies had data to specifically evaluate soccer activity, including the concussion mechanism while heading the soccer ball (see Supplemental Digital Content 3, http://links.lww.com/CORR/A0). Male soccer players were more likely than female players to experience concussions because of player contact (rate ratio 0.80 [95% CI 0.72 to 0.90]; p < 0.001) and surface contact (rate ratio 0.54 [95% CI 0.31 to 0.96]; p = 0.04) when heading the ball, although the latter estimate was based on only two studies [8, 24] (Fig. 6).
Fig. 2.

The pooled incidence rate ratios by concussion mechanism and activity are shown for basketball. The wide confidence intervals for the pooled estimates of equipment/ball contact and general play are due to the low number of concussions and total number of male basketball players included in the study.
Fig. 3.

The pooled incidence rate ratios by concussion mechanism and activity are shown for lacrosse.
Fig. 4.
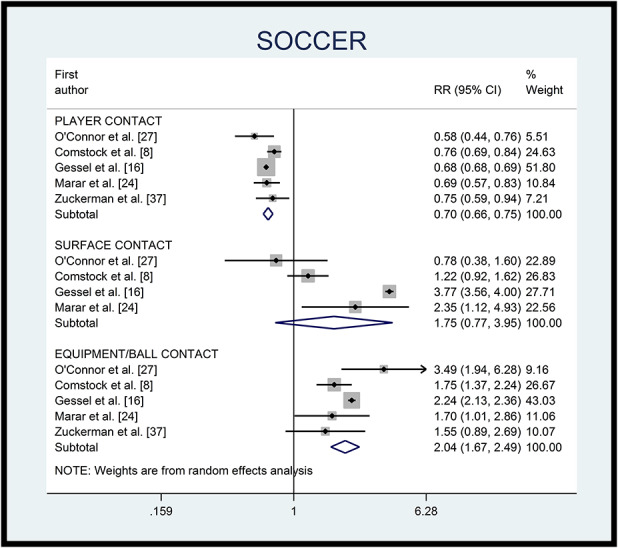
The pooled incidence rate ratios by concussion mechanism are shown for soccer.
Fig. 5.

The pooled incidence rate ratios by concussion mechanism and activity are shown for ice hockey. The studies by Simmons and Zuckerman are based on the same data for ice hockey.
Fig. 6.

The pooled incidence rate ratios by concussion mechanism while heading the ball in soccer are shown.
Sports with a Higher Risk of Ball/Equipment-induced Concussions in Female Athletes
There were no differences between male baseball and female softball players for ball/equipment-induced concussions (rate ratio 0.78 [95% CI 0.57 to 1.05]; p = 0.10) (Fig. 7). Male baseball players were more likely to experience a concussion from being hit by a pitched baseball (rate ratio 0.14 [95% CI 0.12 to 0.16]; p < 0.001), although this finding was mostly based on one large study using injury surveillance databases [16]. On the other hand, female softball players were almost twice as likely to experience a concussion while fielding the ball (rate ratio 1.77 [95% CI 1.17 to 2.70]; p = 0.007). There was no difference between male and female basketball players for surface (rate ratio 0.80 [95% CI 0.57 to 1.12]; p = 0.18) or ball contact (rate ratio 19.34 [95% CI 0.01 to 52085.47]; p = 0.46). Female lacrosse players were more likely to experience a concussion because of contact with the ball or equipment (rate ratio 3.24 [95% CI 2.10 to 4.99]; p < 0.001), as were female soccer players (rate ratio 2.04 [95% CI 1.67 to 2.49]; p < 0.001). When heading the soccer ball, female players were more likely than male soccer players to experience concussions due to ball contact (rate ratio 2.63 [95% CI 1.84 to 3.77]; p < 0.001). No studies reported concussion data on contact with the hockey puck or other equipment, but female hockey players were more likely than male hockey players to experience concussions because of contact with the ice surface (rate ratio 3.00 [95% CI 2.00 to 4.50]; p < 0.001).
Fig. 7.

The pooled incidence rate ratios by concussion mechanism and activity are shown for baseball and softball.
Discussion
The increase in participation of girls and women in sports has led to the publication of two review articles focusing on the possibility of sex or gender differences in concussion incidence [13, 14]. Although there is a large body of evidence on sex and gender differences in the incidence of concussions [3, 29, 34], fewer studies have compared the mechanisms or activities that result in concussions. Knowing the underlying etiology will enable targeted interventions that can reduce this growing health problem. To address the potential increase in injury risk among female athletes, competition rules have been altered to reduce player contact in sports such as women’s lacrosse and ice hockey. The overall findings of this meta-analysis—that concussions in male athletes tend to occur through player contact and concussions in female athletes tend to occur through ball/equipment or surface contact—remain true even for sports that have the same rules of play for men and women (for example, soccer and basketball).
Our meta-analysis has several limitations. We did not include conference abstracts or non-English articles in our search strategy, which may lead to missing unpublished data or important articles. Only a few studies contributed to the pooled estimates in some comparisons, and in these cases they were driven by one or two larger studies. Although the level of consistency was high across studies for concussion mechanisms in soccer and lacrosse, we used a random-effects model to account for any heterogeneity. This approach will lead to wider conference intervals and can reduce the precision around pooled estimates. Because of the paucity of data, we were unable to distinguish between concussions that occurred during competition and practice or at the high school and collegiate levels, which may have varying concussion rates. In addition, all of the studies were conducted in the United States and were rated as having fair quality because of their retrospective design. For lacrosse and ice hockey, the incidence of concussions in male and female players may not be directly comparable given differences in the body contact allowed and the protective equipment worn.
This meta-analysis found that the risk of concussion in male athletes was more likely because of impact with another player in contact sports such as basketball, lacrosse, soccer, and ice hockey. Limited evidence also indicated that male hockey players had a higher relative risk because of body-checking. A few studies presented data that allowed comparing specific differences between male and female soccer player when heading the ball [8, 16, 24, 37]. Male soccer players were more likely than female players to have a heading-related concussion because of player or ground contact. This difference in the mechanism of concussion may be attributed to the fact that men are more inclined to rough play or to adopt an aggressive playing style, which implicates the role of gender, not just sex, and behaviors that contribute to concussions.
In female athletes, most concussions occurred because of contact with the ball or equipment, in lacrosse, soccer, and when heading the soccer ball. Additionally, female hockey players were more likely than male players to experience concussions after hitting the ice surface. There may be biological factors or training differences that result in reduced neck girth and strength relative to head size and head-neck length in female athletes [21]. This decreased neck strength may reduce the athlete’s ability to withstand external forces, such as when heading a soccer ball, and increase acceleration and displacement during impact [4, 15, 18, 32, 33]. One study in high school athletes has shown that neck strength protects against concussions, with each additional pound of neck strength resulting in a 5% reduction in the odds of experiencing a concussion [7]. A similar suggestion has been made for increased neck-torso strength in male athletes, who can better absorb impact throughout the upper body rather than just the head area alone [2, 12, 19]. Sex hormones have also been suggested to play a role in concussions because estrogen and progesterone can alter neuroexcitability, but few studies have been performed in humans [11, 25, 35]. In addition, cerebral blood flow and glucose metabolism have been proposed to explain the sex difference [4, 9, 10]. With no clear factors to possibly explain this difference, future concussion research should focus on how male and female athletes differ physiologically in response to biomechanical forces [5].
Conclusions
Although rule changes may have contributed to reducing the sex or gender disparity in concussion incidence for certain sports, this intervention alone is not enough to reduce concussion rates. The pattern of the underlying concussion-causing mechanism is the same regardless of whether there are differences in the men’s and women’s game. This finding indicates that further interventions are needed to truly reduce concussion rates, such as the adoption of neck-strengthening exercises or other prevention training, greater enforcement of rules to decrease levels of contact in men’s sports, or the required use of protective head equipment in women’s sports. More research is needed to determine the etiology of concussions to implement injury prevention measures and enact policies that will have a sustained impact on reducing sports-related concussions in athletes. Furthermore, reporting sex/gender differences across sports will encourage sex/gender-specific analyses and possible trials to alter concussion risk in the future. Male and female athletes may require different modes of training or protection to continue safe play.
Supplementary Material
Acknowledgments
None.
Footnotes
Each author certifies that neither she, nor any member of her immediate family, has funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Each author certifies that her institution waived approval for the reporting of this investigation and that all investigations were conducted in conformity with ethical principles of research.
This work was performed at the Hospital for Special Surgery, New York, NY, USA.
References
- 1.Agel J, Harvey EJ. A 7-year review of men's and women's ice hockey injuries in the NCAA. Can J Surg. 2010;5:319-323. [PMC free article] [PubMed] [Google Scholar]
- 2.Aubry M, Cantu R, Dvorak J, Graf-Baumann T, Johnston KM, Kelly J, Lovell M, McCrory P, Meeuwisse WH, Schamasch P. Summary and agreement statement of the 1st International Symposium on Concussion in Sport, Vienna 2001. Clin J Sport Med. 2002;1:6-11. [DOI] [PubMed] [Google Scholar]
- 3.Bretzin AC, Covassin T, Fox ME, Petit KM, Savage JL, Walker LF, Gould D. Sex differences in the clinical incidence of concussions, missed school days, and time loss in high school student-athletes: Part 1. Am J Sports Med. 2018;9:2263-2269. [DOI] [PubMed] [Google Scholar]
- 4.Bretzin AC, Mansell JL, Tierney RT, McDevitt JK. Sex differences in anthropometrics and heading kinematics among Division I soccer athletes. Sports Health. 2017;2:168-173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Chandran A, Barron MJ, Westerman BJ, DiPietro L. Multifactorial examination of sex-differences in head injuries and concussions among collegiate soccer players: NCAA ISS, 2004-2009. Inj Epidemiol. 2017;1:28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Cheng J, Ammerman B, Santiago K, Jivanelli B, Lin E, Casey E, Ling D. Sex differences in the incidence of sports-related concussion: Systematic review and meta-analysis. Sports Health; [Published online ahead of print]. DOI: 10.1177/1941738119877186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Collins CL, Fletcher EN, Fields SK, Kluchurosky L, Rohrkemper MK, Comstock RD, Cantu RC. Neck strength: A protective factor reducing risk for concussion in high school sports. J Prim Prev. 2014;5:309-319. [DOI] [PubMed] [Google Scholar]
- 8.Comstock RD, Currie DW, Pierpoint LA, Grubenhoff JA, Fields SK. An evidence-based discussion of heading the ball and concussions in high school soccer. JAMA Pediatr. 2015;9:830-837. [DOI] [PubMed] [Google Scholar]
- 9.Covassin T, Elbin RJ, Harris W, Parker T, Kontos A. The role of age and sex in symptoms, neurocognitive performance, and postural stability in athletes after concussion. Am J Sports Med. 2012;6:1303-1312. [DOI] [PubMed] [Google Scholar]
- 10.Covassin T, Moran R, Elbin RJ. Sex differences in reported concussion injury rates and time loss from participation: An update of the National Collegiate Athletic Association Injury Surveillance Program from 2004-2005 through 2008-2009. J Athl Train. 2016;3:189-194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Day NL, Floyd CL, D'Alessandro TL, Hubbard WJ, Chaudry IH. 17β-estradiol confers protection after traumatic brain injury in the rat and involves activation of G protein-coupled estrogen receptor 1. J Neurotrauma. 2013;17:1531-1541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Delaney JS, Al-Kashmiri A, Correa JA. Mechanisms of injury for concussions in university football, ice hockey, and soccer. Clin J Sport Med. 2014;3:233-237. [DOI] [PubMed] [Google Scholar]
- 13.Dick RW. Is there a gender difference in concussion incidence and outcomes? Br J Sports Med. 2009:46-50. [DOI] [PubMed] [Google Scholar]
- 14.Dvorak J, McCrory P, Kirkendall DT. Head injuries in the female football player: Incidence, mechanisms, risk factors and management. Br J Sports Med. 2007:44-46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Eckner JT, Oh YK, Joshi MS, Richardson JK, Ashton-Miller JA. Effect of neck muscle strength and anticipatory cervical muscle activation on the kinematic response of the head to impulsive loads. Am J Sports Med. 2014;3:566-576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Gessel LM, Fields SK, Collins CL, Dick RW, Comstock RD. Concussions among United States high school and collegiate athletes. J Athl Train. 2007;4:495-503. [PMC free article] [PubMed] [Google Scholar]
- 17.Halstead ME, Walter KD, Moffatt K. Sport-related concussion in children and adolescents. Pediatrics. 2018;142:pii: e20183074. [DOI] [PubMed] [Google Scholar]
- 18.Harmon KG, Drezner J, Gammons M, Guskiewicz K, Halstead M, Herring S, Kutcher J, Pana A, Putukian M, Roberts W. American Medical Society for Sports Medicine Position Statement: Concussion in sport. Clin J Sport Med. 2013;1:1-18. [DOI] [PubMed] [Google Scholar]
- 19.Johnston KM, McCrory P, Mohtadi NG, Meeuwisse W. Evidence-based review of sport-related concussion: Clinical science. Clin J Sport Med. 2001;3:150-159. [DOI] [PubMed] [Google Scholar]
- 20.Lau J, Ioannidis JP, Schmid CH. Quantitative synthesis in systematic reviews. Ann Intern Med. 1997;9:820-826. [DOI] [PubMed] [Google Scholar]
- 21.Lin CY, Casey E, Herman DC, Katz N, Tenforde AS. Sex differences in common sports injuries. PM R. 2018;10:1073-1082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Lincoln AE, Hinton RY, Almquist JL, Lager SL, Head Dick RW., face, and eye injuries in scholastic and collegiate lacrosse: A 4-year prospective study. Am J Sports Med. 2007;2:207-215. [DOI] [PubMed] [Google Scholar]
- 23.Maher ME, Hutchison M, Cusimano M, Comper P, Schweizer TA. Concussions and heading in soccer: A review of the evidence of incidence, mechanisms, biomarkers and neurocognitive outcomes. Brain Inj. 2014;3:271-285. [DOI] [PubMed] [Google Scholar]
- 24.Marar M, McIlvain NM, Fields SK, Comstock RD. Epidemiology of concussions among United States high school athletes in 20 sports. Am J Sports Med. 2012;4:747-755. [DOI] [PubMed] [Google Scholar]
- 25.Mihalik JP, Ondrak KS, Guskiewicz KM, McMurray RG. The effects of menstrual cycle phase on clinical measures of concussion in healthy college-aged females. J Sci Med Sport. 2009;3:383-387. [DOI] [PubMed] [Google Scholar]
- 26.Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA statement. PLoS Med. 2009;7:e1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.O'Connor KL, Baker MM, Dalton SL, Dompier TP, Broglio SP, Kerr ZY. Epidemiology of sport-related concussions in high school athletes: National Athletic Treatment, Injury and Outcomes Network (NATION), 2011-2012 through 2013-2014. J Athl Train. 2017;3:175-185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Rosene JM, Raksnis B, Silva B, Woefel T, Visich PS, Dompier TP, Kerr ZY. Comparison of concussion rates between NCAA Division I and Division III men's and women's ice hockey players. Am J Sports Med. 2017;11:2622-2629. [DOI] [PubMed] [Google Scholar]
- 29.Schallmo MS, Weiner JA, Hsu WK. Sport and sex-specific reporting trends in the epidemiology of concussions sustained by high school athletes. J Bone Joint Surg Am. 2017;15:1314-1320. [DOI] [PubMed] [Google Scholar]
- 30.Simmons MM, Swedler DI, Kerr ZY. Injury surveillance of head, neck, and facial injuries in collegiate ice hockey players, 2009-2010 through 2013-2014 academic years. J Athl Train. 2017;8:776-784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;9:603-605. [DOI] [PubMed] [Google Scholar]
- 32.Tierney RT, Higgins M, Caswell SV, Brady J, McHardy K, Driban JB, Darvish K. Sex differences in head acceleration during heading while wearing soccer headgear. J Athl Train. 2008;6:578-584. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Tierney RT, Sitler MR, Swanik CB, Swanik KA, Higgins M, Torg J. Gender differences in head-neck segment dynamic stabilization during head acceleration. Med Sci Sports Exerc. 2005;2:272-279. [DOI] [PubMed] [Google Scholar]
- 34.Tsushima WT, Siu AM, Ahn HJ, Chang BL, Murata NM. Incidence and risk of concussions in youth athletes: Comparisons of age, sex, concussion history, sport, and football position. Arch Clin Neuropsychol. 2019;1:60-69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Wunderle K, Hoeger KM, Wasserman E, Bazarian JJ. Menstrual phase as predictor of outcome after mild traumatic brain injury in women. J Head Trauma Rehabil. 2014;5:1-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Xiang J, Collins CL, Liu D, McKenzie LB, Comstock RD. Lacrosse injuries among high school boys and girls in the United States: Academic years 2008-2009 through 2011-2012. Am J Sports Med. 2014;9:2082-2088. [DOI] [PubMed] [Google Scholar]
- 37.Zuckerman SL, Kerr ZY, Yengo-Kahn A, Wasserman E, Covassin T, Solomon GS. Epidemiology of sports-related concussion in NCAA athletes from 2009-2010 to 2013-2014: Incidence, recurrence, and mechanisms. Am J Sports Med. 2015;11:2654-2662. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.