

Abstract
The aim of the present study was to investigate the impact of knowledge and practice on the fasting blood glucose of diabetic patients during the month of Ramadan. The simple random sampling technique was used to calculate sample size and the computed sample size was 112. Participants were recruited from the diabetic outpatient clinics at King Fahad Hospital of the University, Dammam, Saudi Arabia. The participants included male and female adults with either type 1 or 2 diabetes, aged 15–70 years. Children, pregnant women, and those who were unable to complete at least 3 weeks of fasting during the study period were excluded from the study. Fasting blood glucose reading of the participants was extracted during Ramadan and in Shawwal (after 30 days) and a first-visit questionnaire related to the knowledge and practice was provided to them. Statistical Package for Social Sciences (version 22) was used for data entry and analysis. A two way ANOVA test, two independent sample t-tests and Chi-square test were used to compare between the groups. A p-value at 0.05 was considered statistically significant. The study found that fasting blood glucose of a participant during the holy month of Ramadan (144.2) was statistically significant with p-value 0.0003 as compared with after Ramadan (178.5). Moreover, it was found that as the level of knowledge (poor, average, good) improved, the fasting blood glucose goes down with p-values 0.036 and 0.037. Our results revealed that fasting during Ramadan significantly decreases blood glucose. The overall level of knowledge and practice concerning diabetes among the participants studied during the month Ramadan is average.
Keywords: Knowledge, practice, Ramadan, diabetes mellitus, blood, glucose
1. INTRODUCTION
Fasting during the holy month of Ramadan is mandatory for all healthy adult Muslims as it is one of the five pillars of Islam. Muslims abstain from taking any oral intake or medication during fasting from dawn to dusk [1].
Prevalence of diabetes in adults is high around the world and was estimated to be 8.4% in 2017 and predicted to rise to 9.9% in 2045 [2]. Kingdom of Saudi Arabia is among the 10 countries that have the highest projection for the prevalence of diabetes in 2011 (16.2%) and 2030 (20.8%) [3]. According to the recent records of the Ministry of Health, 4660 patients with diabetes attended the family and medical clinics across Saudi Arabia in 2015 [4].
Around 50 million people with diabetes fast annually during the month of Ramadan if their diabetes is not complicated [5]. Several studies have been performed to monitor the change in lipid profile among diabetic patients during Ramadan and the results have been compared with the samples taken before or/and after Ramadan [3]. Some of the studies reported the importance of the level of knowledge and practice of diabetic patients to control diabetes during Ramadan as well as how to manage diet and dietary habits during Ramadan [6].
All people with diabetes must make some changes in their dietary habits, daily activities, and drugs adjustments during Ramadan to avoid any potential adverse effects of fasting. Data showed that improvement of knowledge and practice in the diabetic patient was reflected positively on short-term body weight, glycemic control, and lipid profile [7].
A diabetic patient who wishes to fast should be counselled properly to maintain normal levels of blood glucose. Active glucose monitoring is very essential in the documentation of hyperglycemia and hypoglycemia during fasting. Moreover, one of the cornerstones of healthy fasting is to use a balanced diet, the consumption of a large amount of food rich in fats and carbohydrates should be avoided in Ramadan by diabetic patients [8].
The health-related impacts of fasting during Ramadan are still not fully understood and literature regarding the physiological changes of Ramadan is very limited. However, fasting during Ramadan causes many metabolic, biochemical, physiological, and spiritual changes. Ramadan fasting reduces the waist circumference, body fat, body mass index, blood glucose, blood cholesterol, low density lipoprotein cholesterol, very low density lipoprotein cholesterol, triglycerides, systolic and diastolic blood pressure, and anxiety levels [9].
A few hours after fasting, the blood glucose slightly decreases to 60 mg/dl from 70 mg/dl leading to stimulation of liver gluconeogenesis because of a rise in sympathetic and glucagon hormone activities [10], which reflects positively in the glycemic control in diabetic patients but most of the diabetic patients showed variations of fasting blood glucose due to difference in their knowledge and practice [11].
There are limited papers regarding the impact of knowledge and practice on blood parameters among diabetic patients during the month of Ramadan. Thus, this study was designed to study the effect of knowledge and practice on fasting blood glucose of diabetic patients.
2. MATERIALS AND METHODS
This prospective cohort study was conducted at King Fahad Hospital, Dammam, Saudi Arabia. The study period was from May to September 2017. Ethical approval for the study was obtained through the Ethical Review Board of Imam Abdulrahman Bin Faisal University (IRB 2017-01-099). Patients who visited the diabetic clinics at King Fahad Hospital of the University were participants of the study. The participants included male and female adults with either type 1 or 2 diabetes, aged 15–70 years. Diabetics younger than 15 years were excluded from the study as children and pregnant women have a different risk profile and do not normally fast. Patients with intercurrent illness requiring admission to hospital along with those who were unable to complete at least three weeks of fasting during the study period were excluded from the study.
The simple random sampling technique was used to calculate sample size and the computed sample size was 112. Consent was taken from those who agreed to participate.
While patients were visiting diabetic clinics during Ramadan (during fasting hours) they were requested to provide the blood sample. Patients were sent to the King Fahad hospital laboratory for blood extraction. They were also requested to come again to the laboratory to give another sample during Shawwal (next month after Ramadan). Hence, the second blood sample collection was done during the month of Shawwal, which blood was taken by laboratory assistants.
Questionnaires were provided to the patients during their visit to the doctor during Ramadan and the purpose of the study was explained as well. Patients were requested to give their feedback during their visit so that in case of any difficulty in understanding any of the questions they would be solved by the attending doctor. The questionnaire consisted of some demographic questions, such as onset of disease, gender, family history, marital status and so on, followed by the questions related to knowledge and practice about how do their fast during the holy month of Ramadan.
Patients’ knowledge score was assessed using eight questions related to following topics: patients with diabetes should never fast, taking insulin injection during fasting breaks the fast, Sahur (Predawn meal) can be skipped during Ramadan, checking blood glucose levels during Ramadan is prohibited, physical activity should be avoided during fasting, polyurea is one of the symptoms of hypoglycemia, polydipsia is one of symptoms of hyperglycemia, and optimum blood glucose level during fasting. The level of knowledge was categorized into three categories as: if up to three correct answers the level of knowledge was considered as poor; for four to six correct answers the knowledge was considered as average; and for more than six correct answers the level of knowledge was good.
Patients’ practice score was assessed using the following five questions: whether the patients change medication schedule based on the doctor’s advice; reduce the frequency of medication; make sure to take Sahur (predawn meal); take sweet food on breaking fast; and take supper. The practice was considered as poor for one correct answer, average of two to three correct answers, and good for more than three correct answers. These questions were taken from a previously published article [12]. Questions were translated into Arabic by a native Arabic language speaker following which those translated questions were back translated into English by another person who also had Arabic as a native language and sound knowledge of English to ensure that the questions were carrying the same meaning in both English and Arabic versions. Hence, the study participants had both options, i.e., if they were comfortable with Arabic, they were provided the Arabic questionnaire and vice versa.
Statistical Package for Social Sciences (SPSS version 22, SPSS Inc, Chicago, IL, USA) was used for data entry and analysis. Demographic data of the patients were presented in the form of tables and graphs. Two-way ANOVA was used to test the difference in blood glucose level with gender and knowledge and practice scores of the participants. Two independent sample t-tests were used to compare average blood glucose during and after the holy month of Ramadan with the different levels of knowledge and practice. Chi-square test was used to study the relationship between gender, family history, and levels of knowledge and practice.
3. RESULTS
The total number of patients who agreed to participate and fill the questionnaire was 159. However, 135 out of 159 gave a blood sample during their Ramadan visit. Of these 135 patients (who provided a sample during Ramadan), 112 came for the follow-up visit after Ramadan. Hence, 112 patients were finally included in the study out of 159 patients and the participation rate was 70.4%. There were 54 males and 58 females who participated in the study. On average, a patient diagnosed with diabetics 11.4 (±7.37) years ago. Almost 42% of the patients were taking only oral hypoglycemic agent as a diabetic treatment, 39% were using insulin, 13.4% were using both tablet and insulin, and 5.6% were not taking any medicine at all. When patients were asked about family history of diabetes, 85 replied positively and 27 responded negatively.
Average fasting blood glucose of a participant during the holy month of Ramadan was 144.2 ± 62.1 (range: 50–510) and average blood glucose after the holy month of Ramadan was found to be 178.5 ± 76.7 (range: 80–490). Increase in blood glucose level after the holy month of Ramadan was statistically significant with p-value 0.0003 as shown in Figure 1.
Figure 1.
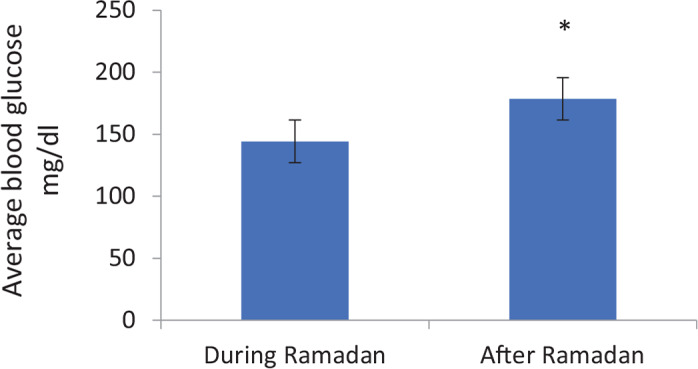
The comparison of fasting blood glucose among participants during and after Ramadan. *Statistically significant at 0.05 level of significance.
Those who had accurate knowledge regarding “Sahur (Predawn meal) can be skipped during Ramadan” (p = 0.024*), “Checking blood glucose levels during fasting is prohibited” (p = 0.027), and “physical activity should be avoided during fasting” (p = 0.014) had significantly less blood glucose level (Table 1).
Table 1.
Effect of knowledge on blood glucose
| Questions | Correct | Incorrect | p-value | ||
|---|---|---|---|---|---|
| Frequency | Blood glucose mean (SD) | Frequency | Blood glucose mean (SD) | ||
| Patients with diabetes should never fast | 24 | 155.7 (61.8) | 89 | 139.9 (62.7) | 0.275 |
| Taking insulin injection during fasting breaks the fast | 71 | 142.7 (63.8) | 42 | 144.3 (61.1) | 0.897 |
| Sahur (predawn meal) can be skipped during Ramadan | 92 | 136.9 (61.2) | 21 | 171.0 (62.3) | 0.024* |
| Checking blood glucose levels during Ramadan is prohibited | 88 | 141.4 (65.5) | 25 | 178.0 (46.7) | 0.027* |
| Physical activity should be avoided during fasting | 62 | 132.4 (49.2) | 51 | 156.5 (74.1) | 0.041* |
| Polyurea is one of the symptoms of hypoglycemia | 64 | 141.1 (66.6) | 49 | 146.2 (57.3) | 0.67 |
| Polydipsia is one of symptoms of hyperglycemia | 96 | 145.4 (65.3) | 17 | 131.2 (43.9) | 0.391 |
| Optimum blood glucose level during fasting | 76 | 142.2 (66.8) | 35 | 146.9 (54.7) | 0.713 |
Statistically significant at 0.05 level of significance.
SD: standard deviation.
Patients who changed the medicine as per doctor’s advice had significantly lower average blood glucose (p = 0.006) than the comparison group (Table 2).
Table 2.
Effect of practice on blood glucose
| Questions | Correct | Incorrect | p-value | ||
|---|---|---|---|---|---|
| Frequency | Blood glucose mean (SD) | Frequency | Blood glucose mean (SD) | ||
| Change medication schedule based on the doctor’s advice | 75 | 133.8 (47.8) | 31 | 170.4 (86.7) | 0.006* |
| Reduced frequency of medication | 40 | 136.5 (57.9) | 64 | 147.3 (65.3) | 0.38 |
| Make sure to take Sahur (predawn meal) | 82 | 143.4 (62.3) | 23 | 141.9 (63.2) | 0.921 |
| Take sweet food on breaking fast | 16 | 132.7 (55.7) | 90 | 144.2 (63.6) | 0.50 |
| Take supper | 40 | 133.9 (40.2) | 65 | 148.7 (72.3) | 0.239 |
Statistically significant at 0.05 level of significance.
SD: standard deviation.
Interestingly, it was observed that as the level of knowledge and practice improved, the fasting blood glucose was going down, especially, when the blood glucose level was compared between the group of poor knowledge and other knowledge categories (average and good) with p-values 0.036 and 0.037, respectively. The drop in fasting blood glucose in contrast with the practice was not found statistically significant at any point (Table 3).
Table 3.
Fasting blood glucose related to categorized knowledge and practice in Ramadan
| Blood glucose | Poor mean (SD) | Average mean (SD) | Good mean (SD) |
|---|---|---|---|
| Knowledge | |||
| During Ramadan | 159.3 (62.5) | 143.15 (66.1) | 135 (48.9) |
| After Ramadan | 217.6 (77.1) | 173.9 (77.5) | 169.2 (71.6) |
| p-value | Reference group | 0.036* | 0.037* |
| Practice | |||
| During Ramadan | 159.7 (87.4) | 139.4 (46.4) | 126.0 (46.7) |
| After Ramadan | 178.1 (71.3) | 176.5 (76.8) | 159.7 (58.1) |
Statistically significant at 0.05 level of significance.
SD: standard deviation.
Furthermore, almost 70% of the patients had average knowledge regarding Ramadan fasting. Only 19.5% and 10.5% had good and poor knowledge, respectively. About practice, 47.8% had average practice level, 31% and 21.2% were having poor and good levels, respectively (Table 4).
Table 4.
Demographic variables in relation to knowledge and practice about Ramadan fasting
| Knowledge (%) | Practice (%) | |||||
|---|---|---|---|---|---|---|
| Poor | Average | Good | Poor | Average | Good | |
| Gender | ||||||
| Male | 7 (13) | 38 (70.4) | 9 (16.6) | 16 (30.2) | 27 (50.9) | 10 (18.9) |
| Female | 5 (8.5) | 41 (69.5) | 13 (22) | 19 (32.2) | 27 (45.8) | 13 (22) |
| Family history | ||||||
| Yes | 6 (7) | 60 (69.8)* | 20 (23.2) | 24 (27.9) | 42 (48.9) | 20 (23.2) |
| No | 6 (22.2) | 19 (70.4) | 2 (7.4) | 11 (40.7) | 12 (44.5) | 4 (18.8) |
| Onset (years) | ||||||
| <5 | 5 (20) | 16 (64) | 4 (16) | 6 (24) | 13 (52) | 6 (24) |
| 5–10 | 2 (10) | 17 (85) | 1 (5) | 12 (40) | 10 (33.3) | 8 (26.7) |
| >10 | 5 (7.9) | 42 (66.7) | 16 (25.4) | 15 (28.3) | 30 (56.6) | 8 (15.1) |
Statistically significant at 0.05 level of significance.
Some of the patients (23.2%), who had a family history of diabetes, had good knowledge about how to fast during the holy month of Ramadan. Patients with a family history of diabetes had significantly better knowledge compared with those who did not have a family history (p = 0.028). Furthermore, it was also found that those who had good knowledge were practicing better during Ramadan. Good and average practice during Ramadan was found among 23.2% and 48.9% of patients, respectively.
The majority of participants with long diabetic duration (>10 years) were having average (42) and good (16) knowledge. Similarly, average and good practice were observed among 30 and eight participants, respectively (Table 4).
4. DISCUSSION
The aim of the current study was to study the effect of knowledge and practice on fasting blood glucose of diabetic patients attending the King Fahad Hospital of the Imam Abdulrahman Bin Faisal University at Eastern Province, Saudi Arabia during the holy month of Ramadan. The present work found a significantly lower average fasting blood glucose during Ramadan among the participants. This is consistent with that reported in other studies [13,14].
Interestingly, as the level of knowledge and practice in terms of dietary control, adjustment of glucose-lowering medication, checking blood glucose levels during fasting, and physical exercise improved the fasting blood glucose level went down.
There is no doubt that blood glucose monitoring is considered the ‘cornerstone’ of improving glycemic control in diabetic patients [15]. Monitoring of blood glucose level several times a day during Ramadan should be part of a regular management plan for diabetic patients due to the new scheduling of medication, activity, and food during this month to achieve the appropriate adjustment to prevent hyperglycemia during the night or hypoglycemia risks during daytime fasting. As reported in our results, accurate knowledge in this regard was found to have significant impact with glycemic control in Ramadan, which is similar to the findings of other studies [16,17].
Regarding the effects of physical activities in fasting diabetic patients, several reports have shown that light physical activities on a regular basis during Ramadan fasting is harmless for diabetic patients [18]. In the present study, a significant percentage of diabetic patients showed appropriate knowledge toward performing physical activity during Ramadan. Similarly, change medication schedule based on the doctor’s advice during Ramadan is also suggested in studies and recommendations [8,17]. In this study, the correct practice was followed and medication schedule was changed in the majority of the patients during Ramadan.
There is ample data to show that it is safe for well-controlled diabetics to fast during the month of Ramadan [19–21] by which there is continual use of glucose in the body for various physiological functions that results in a decrease in blood glucose level. Furthermore, the depletion of glycogen stores after prolonged fasting further decreases its level [21].
Most of the studied participants in our study had an average level of knowledge and practice during Ramadan toward their own responsibility to monitor and control their disease and ability to carry out Ramadan fasting. The knowledge regarding fasting in Ramadan for the diabetic patient was found to be satisfactory. The majority of participants were aware of behavioral practices, including adjustment of glucose-lowering medication accordingly, reducing the intake of sweet diets, and taking supper. Similar finding was found in another cross-sectional study conducted on 243 diabetic patients at the Hospital of Universiti Sains Malaysia [12]. The results indicate that knowledge and practice have a vital role in early detection, prevention, and any future disease development. Positive knowledge and practice are important for diabetic patients and they greatly depend on habits and cultural beliefs [22].
Our results found that having a family history of diabetes mellitus has a significant average level of diabetes knowledge, together with that knowledge those patients were practicing better. The results of this data set are presented for parents and siblings (i.e., first-degree relatives and second-degree relatives) to define family history included aunts and uncles in their definition [23]. Having a positive family history with diabetes mellitus may be a good source of health information [24]. Several studies have found that patients with a family history of diabetes mellitus were more aware of the disease than those without such a history [23,25,26]. Family history is a well-known risk factor for type 2 diabetes mellitus. A family history of diabetes mellitus may be indicative of perceived susceptibility to the disease, which would in turn influence one’s likelihood of behavior change [26]. Thus, a family history of diabetes may be a useful tool to identify individuals at increased risk of the disease and target behavior modifications that could potentially delay disease onset and improve health outcomes.
The higher knowledge and practice score observed with the longer duration of diabetes among our participants (>10 years) suggests that they could improve their knowledge and practice from experience over their long duration of the disease and other formal educational programs [27].
Ensuring good glycemic control during the month of Ramadan is a challenge for both physicians and patients [19]. It is important that doctors educate their patients about the changes in glucose-lowering medication schedule and lifestyle habits during the month of Ramadan. Patients should also be educated of the need to monitor their blood glucose on a regular basis throughout the month of Ramadan.
There are some limitations in this study. First, it was an outpatient hospital-based study, where diabetes mellitus-related education may be more readily available to participants. Second, the finding is based on self-reported data from patients themselves and such data are of questionable validity.
5. CONCLUSION
The study shows a significant reduction in fasting blood glucose with an average level of knowledge and practice toward fasting in Ramadan for diabetic patients. Encouraging such behaviors and practice for diabetic patients during their regular visits are required in diabetes management. As a result, it is expected that this increased special attention has an impact on improving the glycemic control and preventing complications during Ramadan.
ACKNOWLEDGMENTS
We are grateful to the medical students Abdulrahman Al Ruwished, Hager Al Shamrani, Houria Al Sahwan, Zahra Al Eswaikt, Khadijah Al Tarouti, and Sarraa Al Tarouti who took interest in the research and we would like to thank them for the time they had devoted to participate in this study.
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
AUTHOR CONTRIBUTIONS
M.A., S.K., W.A. and W.A. contributed to the design and implementation of the research, to the analysis of the results, and to the writing of the manuscript.
FUNDING
The authors received no financial support for this research.
REFERENCES
- [1].The Holy Quran. King Saud University Electronic Moshaf Project. 2013 Available at: http://quran.ksu.edu.sa/index.php?l=en#aya=2_182 (accessed January 13, 2014).
- [2].Cho NH, Shaw JE, Karuranga S, Huang Y, da Rocha Fernandes JD, Ohlrogge AW, et al. IDF diabetes atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract. 2018;138:271–81. doi: 10.1016/j.diabres.2018.02.023. [DOI] [PubMed] [Google Scholar]
- [3].Guariguata L, Whiting DR, Hambleton I, Beagley J, Linnenkamp U, Shaw JE. Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Res Clin Pract. 2014;103:137–49. doi: 10.1016/j.diabres.2013.11.002. [DOI] [PubMed] [Google Scholar]
- [4].Alotaibi A, Perry L, Gholizadeh L, Al-Ganmi A. Incidence and prevalence rates of diabetes mellitus in Saudi Arabia: an overview. J Epidemiol Glob Health. 2017;7:211–18. doi: 10.1016/j.jegh.2017.10.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Azizi F, Siahkolah B, Shahraz S, Sherafat-Kazemzadeh R, Zali M, Beheshti S. Ramadan fasting and diabetes mellitus. Arch Iran Med. 2003;6:237–42. [Google Scholar]
- [6].Fatim J, Karoli R, Chandra A, Naqvi N. Attitudinal determinants of fasting in type 2 diabetes mellitus patients during Ramadan. J Assoc Physicians India. 2011;59:630–4. https://www.ncbi.nlm.nih.gov/pubmed/22479742. [PubMed] [Google Scholar]
- [7].Sämann A, Mühlhauser I, Bender R, Kloos Ch, Müller UA. Glycaemic control and severe hypoglycaemia following training in flexible, intensive insulin therapy to enable dietary freedom in people with type 1 diabetes: a prospective implementation study. Diabetologia. 2005;48:1965–70. doi: 10.1007/s00125-005-1905-1. [DOI] [PubMed] [Google Scholar]
- [8].Al-Arouj M, Assaad-Khalil S, Buse J, Fahdil I, Fahmy M, Hafez S, et al. Recommendations for management of diabetes during Ramadan: update 2010. Diabetes Care. 2010;33:1895–902. doi: 10.2337/dc10-0896. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Meo SA, Hassan A. Physiological changes during fasting in Ramadan. J Pak Med Assoc. 2015;65:S6–S14. https://www.ncbi.nlm.nih.gov/pubmed/26013791. [PubMed] [Google Scholar]
- [10].Azizi F. Medical aspects of Islamic fasting. Med J IR Iran. 1996;10:241–6. [Google Scholar]
- [11].Ewis A, Afifi N. Ramadan fasting and non-insulin-dependent diabetes mellitus: effect of regular exercise. Proceedings of the 2nd International Congress on Health and Ramadan; 1997; Istanbul, Turkey. pp. 1–3. [Google Scholar]
- [12].Yaacob N, Ismail AA, Bebaker WMW. Knowledge, attitude, and practice of type 2 diabetes mellitus patients on Ramadan fasting at Hospital Universiti Sains Malaysia. J Islam Med Assoc North Am. 2007;39:6–12. doi: 10.5915/39-1-5253. [DOI] [Google Scholar]
- [13].Velayudhan M. Managing diabetes during the Muslim fasting month of Ramadan. Med J Malaysia. 2012;67:353–4. https://www.ncbi.nlm.nih.gov/pubmed/23082439. [PubMed] [Google Scholar]
- [14].Karatoprak C, Yolbas S, Cakirca M, Cinar A, Zorlu M, Kiskac M, et al. The effects of long term fasting in Ramadan on glucose regulation in type 2 diabetes mellitus. Eur Rev Med Pharmacol Sci. 2013;17:2512–16. https://www.ncbi.nlm.nih.gov/pubmed/24089232. [PubMed] [Google Scholar]
- [15].Karter AJ, Ackerson LM, Darbinian JA, D’Agostino RB, Ferrara A, Liu J, et al. Self-monitoring of blood glucose levels and glycemic control: the Northern California Kaiser Permanente Diabetes registry. Am J Med. 2001;111:1–9. doi: 10.1016/S0002-9343(01)00742-2. [DOI] [PubMed] [Google Scholar]
- [16].Ahmedani MY, Alvi SF, Haque MS, Fawwad A, Basit A. Implementation of Ramadan-specific diabetes management recommendations: a multi-centered prospective study from Pakistan. J Diabetes Metab Disord. 2014;13:37. doi: 10.1186/2251-6581-13-37. https://www.ncbi.nlm.nih.gov/pubmed/24559109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Ibrahim M, Abu Al Magd M, Annabi FA, Assaad-Khalil S, Ba-Essa EM, Fahdil I, et al. Recommendations for management of diabetes during Ramadan: update 2015. BMJ Open Diabetes Res Care. 2015;3:e000108. doi: 10.1136/bmjdrc-2015-000108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Benaji B, Mounib N, Roky R, Aadil N, Houti IE, Moussamih S, et al. Diabetes and Ramadan: review of the literature. Diabetes Res Clin Pract. 2006;73:117–25. doi: 10.1016/j.diabres.2005.10.028. [DOI] [PubMed] [Google Scholar]
- [19].Salti I, Bénard E, Detournay B, Bianchi-Biscay M, Le Brigand C, Voinet C, et al. A population-based study of diabetes and its characteristics during the fasting month of Ramadan in 13 countries: results of the epidemiology of diabetes and Ramadan 1422/2001 (EPIDIAR) study. Diabetes Care. 2004;27:2306–11. doi: 10.2337/diacare.27.10.2306. [DOI] [PubMed] [Google Scholar]
- [20].Katibi IA, Akande AA, Bojuwoye BJ, Okesina AB. Blood sugar control among fasting Muslims with type 2 diabetes mellitus in Ilorin. Niger J Med. 2001;10:132–4. https://www.ncbi.nlm.nih.gov/pubmed/11806014. [PubMed] [Google Scholar]
- [21].Rehman J, Shafiq M. Changes in blood glucose and lipid profile during Ramadan fasting. J Ayub Med Coll. 2000;12:13–15. [Google Scholar]
- [22].Badruddin N, Basit A, Hydrie MZI, Hakeem R. Knowledge, attitude and practices of patients visiting a diabetes care unit. Pak J Nutr. 2002;1:99–102. doi: 10.3923/pjn.2002.99.102. [DOI] [Google Scholar]
- [23].Erasmus RT, Blanco Blanco E, Okesina AB, Mesa Arana J, Gqweta Z, Matsha T. Importance of family history in type 2 black South African diabetic patients. Postgrad Med J. 2001;77:323–5. doi: 10.1136/pmj.77.907.323. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Al-Qazaz HKh, Sulaiman SA, Hassali MA, Shafie AA, Sundram S, Al-Nuri R, et al. Diabetes knowledge, medication adherence and glycemic control among patients with type 2 diabetes. Int J Clin Pharm. 2011;33:1028–35. doi: 10.1007/s11096-011-9582-2. [DOI] [PubMed] [Google Scholar]
- [25].Baptiste-Roberts K, Gary TL, Beckles GL, Gregg EW, Owens M, Porterfield D, et al. Family history of diabetes, awareness of risk factors, and health behaviors among African Americans. Am J Public Health. 2007;97:907–12. doi: 10.2105/AJPH.2005.077032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Harrison TA, Hindorff LA, Kim H, Wines RC, Bowen DJ, McGrath BB, et al. Family history of diabetes as a potential public health tool. Am J Prev Med. 2003;24:152–9. doi: 10.1016/S0749-3797(02)00588-3. [DOI] [PubMed] [Google Scholar]
- [27].Al-Adsani AMS, Moussa MAA, Al-Jasem LI, Abdella NA, Al-Hamad NM. The level and determinants of diabetes knowledge in Kuwaiti adults with type 2 diabetes. Diabetes Metab. 2009;35:121–8. doi: 10.1016/j.diabet.2008.09.005. [DOI] [PubMed] [Google Scholar]