

Abstract
Vital signs (VS) are dynamic parameters and understanding the significance of changes in VS in the acute setting may offer clinical meaning. We aimed to measure dynamic changes in vital signs (ΔVS) between site of trauma and presentation to hospital and investigate the association between ΔVS and in-hospital mortality among elderly with trauma.
We conducted a retrospective cohort study between 2004 and 2015 using data from the nationwide trauma registry. Patients aged ≥75 years were included. Data were collected at scene of trauma and at arrival of emergency department (ED) in Japan with blunt or penetrating trauma. ΔVS scoring was defined based on clinical implications and previous reports. One point was given for each of the following criteria: systolic blood pressure reduction (-ΔSBP) of ≥30 mm Hg, heart rate increase (ΔHR) of ≥20/minute, and respiratory rate increase (ΔRR) of ≥10/minute between site of trauma and ED. The primary outcome was in-hospital mortality.
Of 236,698 patients in the registry, data from 28,860 eligible patients (12.2%) were analyzed [mean age (SD), 83.2 (0.3); males, 57%]. Overall in-hospital mortality rate was 10.0%. In-hospital mortality increased from 9.0% to 16.5% for -ΔSBP; 9.2% to 22.2% for ΔHR; and 9.7% to 15.9% for ΔRR. ΔVS scores of 0, 1, 2, and 3 points were associated with in-hospital mortality of 8.2%, 14.9%, 30.1%, and 50.0%, respectively.
A score based on the dynamic changes of VS, ΔVS score, may be helpful in predicting in-hospital mortality among elderly with trauma.
Keywords: delta vital signs, dynamic vital signs, elderly, Japan Trauma Data Bank, trauma score, vital signs
1. Introduction
Several trauma scores to predict prognosis have been developed over the past several years, such as the Revised Trauma Score (RTS) and the Rapid Emergency Medicine Score.[1–3] These scoring systems use easily accessible clinical information including vital signs in pre-hospital and hospital settings. However, the clinical condition of a typical trauma patient may change from moment to moment, and static scoring systems may mislead physicians regarding the clinical prognosis of a patient upon presentation to hospital.[4] In particular, this aspect is critical for older patients, since the elderly often require more prompt and appropriate interventions than the young, as they have both higher mortality and higher rates of under-triage compared to younger patients.[5–7] Physicians would have indeed experienced that the elderly trauma patient has an underlying cause, such as cranial vascular disease, infection, drug side effects, or cardiac arrhythmias, not only frailty or cognitive impairment, which could have far more serious outcomes.
Japan is a front runner of aging countries in the world. Even among Japanese aged 65 years or older who have been internationally regarded as elderly, mental, and physical health is well maintained, and the majority of them are capable of taking part in active social activities. Taking it into consideration, the Japanese geriatric academic societies redefined the elderly as an aged 75 years and older in 2017.[8] This group accounts for 38% of all fatal trauma cases from 2013 to 2017.[9] Hence, trauma in the elderly is of great concern in Japan.
Vital signs, though typically reported as static parameters, are in reality, dynamic, reflecting the real-time condition of the bodys functions. Changes in physiological variables, reflected in changes in vital signs (ΔVS), may function as early alarms and thus better predict prognosis after trauma. Nonetheless, there is scant data in the literature focusing on these potentially important features.[5,10–13] Thus, the aim of our current study was to develop a ΔVS score for elderly with trauma based on vital sign changes between the site of trauma and presentation to hospital, as well as to analyze the association between the ΔVS score and in-hospital mortality.
2. Methods
2.1. Data collection
We conducted a retrospective cohort study using registered data from the Japan Trauma Data Bank (JTDB) to analyze the association between a score based on changes in vital signs (ΔVS score) and in-hospital mortality among trauma patients. Data were obtained from the JTDB, a nationwide trauma registry established in 2003 and authorized and maintained by the Japanese Association for the Surgery of Trauma and the Japanese Association for Acute Medicine to improve and assure the quality of trauma care in Japan. In Japan, there is no centre which specializes in treatment of only trauma patients, and tertiary emergency medical centers are mainly responsible for treating trauma patients. A total of 260 hospitals, including 95% of certified tertiary emergency medical centers in Japan, contributed to the JTDB in 2015. The JTDB collected data regarding patient demographics, trauma cause, Injury Severity Score (ISS),[14] and vital signs at pre-hospital and at hospital. It also collected data regarding ED mortality and in-hospital mortality.[15] The primary outcome of this study was in-hospital mortality.
2.2. Patient selection
The JTDB enrolled a total of 236,698 patients between January 2004 and December 2015. Exclusion criteria were: patients who were 74 years of age and younger, or those with missing age data; those who had trauma mechanisms other than blunt or penetrating trauma, or those with missing mechanism data; patients with cardiorespiratory arrest at either the trauma scene or at ED; or those with an Abbreviated Injury Scale (AIS) score of 6 (i.e., non-survivable injury) for any reason. We also excluded patients with vital sign data at the extremes of normally reported distributions: systolic blood pressure (SBP) >300 or SBP < 40 mm Hg; heart rate (HR) >220 or <20 per minute; and respiratory rate (RR) >60 or <4 per minute. Data included in analysis were those representing complete datasets for score predictors of patient age, SBP, HR, RR at both the trauma scene and ED, and in-hospital mortality.
2.3. Statistical analyses
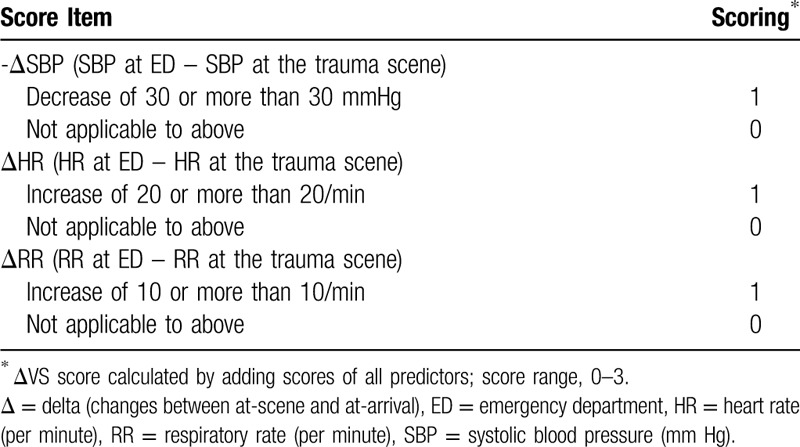
Data were described as mean +/− standard deviation (SD) or raw number with percentage. The ΔVS score was developed using the dynamic change in vital signs. Selection of included parameters was based on previous literature[5] and ease of use in the clinical settings (Table 1). One point was given for each of the following criteria: systolic blood pressure reduction (−ΔSBP) of ≥30 mm Hg, heart rate increase (ΔHR) of ≥20/minute, and respiratory rate increase (ΔRR) of ≥10/minute between site of trauma and presentation to hospital. Scoring items were assessed using c-statistic with 95% confidence interval (CI) and characteristics were evaluated using sensitivity, specificity, and positive and negative predictive values for score cutoff values of 1, 2, and 3. All analyses were performed with IBM SPSS statistics version 25 (IBM Corporation, Armonk, NY, USA).
Table 1.
Delta vital sign score (ΔVS).
2.4. Ethical approval
We received permission to use the data from the steering committee of the JTDB. This study was approved by the ethics committee of Tsukuba Medical Center Hospital. The ethics committee at our institution does not require informed consent from patients for observational studies using anonymous data previously collected for routine clinical standard of care.
2.5. Patient and public involvement
Patients (and/or the public) were not involved in the development of the research question (s), the design of the study, recruitment, and conduct of the study.
3. Results
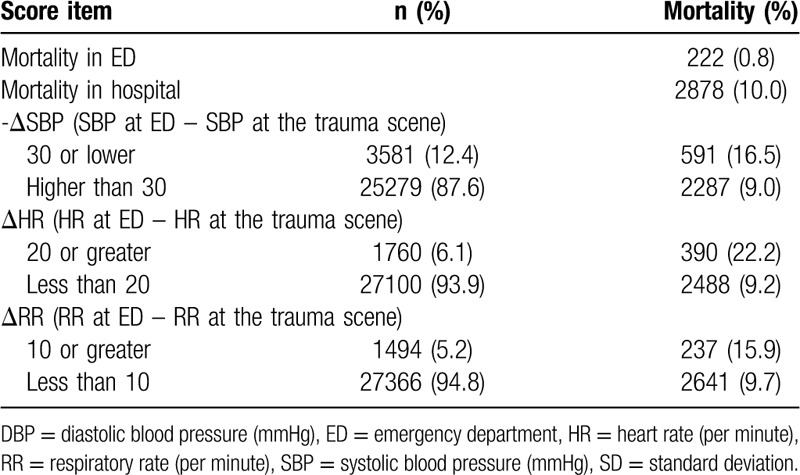
Of 236,698 patients registered in the JTDB, data from 28,860 eligible patients (12.2%) were analyzed. Table 2 shows the clinical characteristics of these patients (mean age, 83.2 years (+/− 0.3); 57% male). The majority of patients had blunt trauma (98.7%). Mortality in the ED was 0.8% (222 of 28,707 patients) and in-hospital mortality was 10.0% (2878 patients). Table 3 shows distribution of patients by score items. A -ΔSBP of ≥30 mm Hg between trauma scene and ED was seen in 12.4% patients. A ΔHR of ≥20/minute was observed in 6.1% patients, while 5.2% patients had a ΔRR of ≥10. When -ΔSBP ≥30 mm Hg, the in-hospital mortality rate increased from 9.0% to 16.5%. Similarly, mortality increased from 9.2% to 22.2% for ΔHR ≥20/minute. Mortality increased from 9.7% to 15.9% for ΔRR ≥10/minute.
Table 2.
Characteristics of patients (N = 28860).
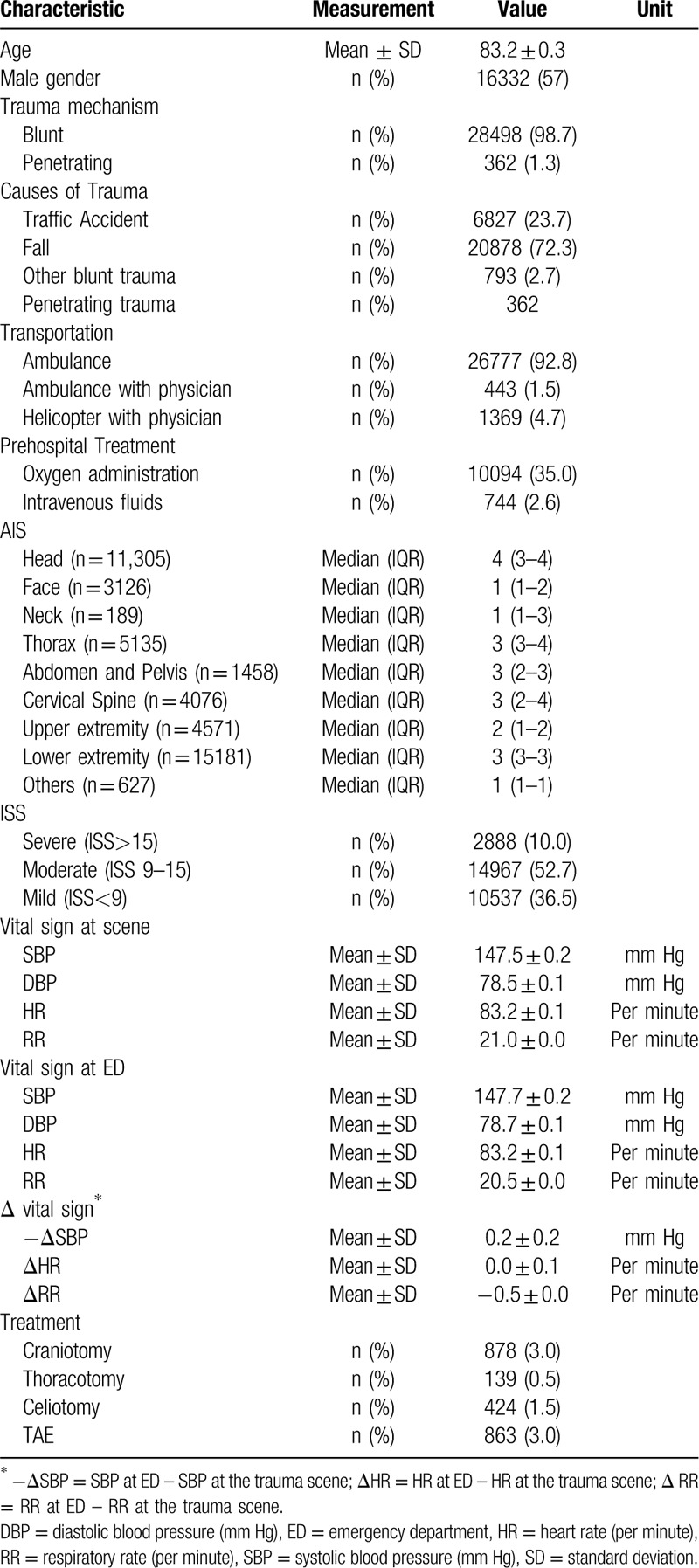
Table 3.
Mortality and distribution of patients according to score item (N = 28860).
In-hospital mortality according to ΔVS score is shown in Table 4. While patients with a score of zero had a mortality of only 8.2%, 50.0% of those with a maximum score of 3 died during the hospitalization. Score characteristics for in-hospital mortality according to different cutoffs are shown in Table 5. For patients with a score of 1, 2, and 3, specificity was 80.0%, 98.4%, and 99.9%, respectively. Positive likelihood ratio for mortality was 5.0 for patients with score 3 and negative likelihood ratio was 0.8 for those with score zero. C-statistic of the score was 0.581 (95% CI, 0.570–0.593).
Table 4.
In-hospital mortality of patients according to delta vital sign score (N = 28860).
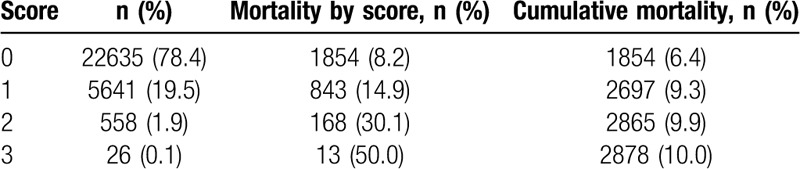
Table 5.
Score characteristics for in-hospital mortality according to different cutoffs for delta vital sign score. (N = 28860).

4. Discussion
The current study investigated the association between changes in vital signs (ΔVS) and in-hospital mortality among elderly with trauma, mainly blunt trauma, using data obtained from a nationwide trauma database in Japan. A novel prediction rule, the ΔVS score, was developed to predict in-hospital mortality. The score was developed using the following 3 items with 1 point added for each positive criterion: -ΔSBP ≥30 mm Hg, ΔHR ≥ 20/minute, and ΔRR ≥ 10/minute. In-hospital mortality was positively correlated with an increasing ΔVS score, and patients with 3 points had a 50% in-hospital mortality.
Several trauma scores have been developed to predict severity and prognosis of trauma patients. Some of these are anatomical scoring systems such as the AIS and the ISS, while others, like the RTS, employ physiological scoring systems. Among these, the anatomical scoring systems have shown better predictive performance compared with the physiological scoring systems for trauma patients.[16] Combinations of anatomical and physiological scores have been proposed to increase accuracy.[17] However, the calculation of these scores is often cumbersome and time-consuming. Anatomical scoring also requires a great deal of experience, as well as advanced examination such as the addition of computed tomography imaging. Meanwhile, present static physiological trauma scores may fit less well with elderly patients compared to non-elderly adults. Some studies suggest that geriatric patients may appear to have normal adult vital signs, despite the presence of life-threatening injuries.[18,19]
In order to further explore this, we developed a method to predict prognosis for elderly with trauma using a dynamic index. ΔVS is an objective and convenient dynamic indicator readily available to clinicians and paramedical providers. To our knowledge, there are few studies that have evaluated the differences between prehospital and ED vital signs and its association with mortality.[5,20] One report concluded that -ΔSBP and ΔRR was associated with 48 hour-mortality for trauma patients,[5] while another study suggested that ΔHR may be useful for identification of severely injured patients.[20] In addition, a study has recently reported that a change in the National Early Warning Score (NEWS) 12 hours after admission has far more prognostic value for patients with a high NEWS on admission, and very little value for those with a normal NEWS on admission. However, there is no previous study about combination of changes in classical vital signs including blood pressure, heart rate, and respiratory rate.
In the actual clinical settings, medical professionals are likely to be able to easily identify patients with scores of 2 or 3 points, and who are at high risk of death, even without use of a scoring system. However, the prognosis of patients with only 1 point might be underestimated by medical professionals, especially those who initially present without acute distress; although, transient vital signs changes such as a vasovagal response, anxious mood, or hyperventilation were included for patients who scored 1 point. In the current study, 1 out of 5 patients (19.5%) scored 1 point and 15% of these subsequently died in hospital, resulting in an 80% specificity. To identify patients in this “grey zone” of mortality risk, the ΔVS score might be helpful. Finally, this score can be used in any setting as assessment requires neither special experience nor expensive instrumentation. It may be useful not only in developed countries, but also in resource-limited environments such as rural areas or developing countries.
Potential limitations of this study should be acknowledged. First, this research is based on Japanese data. In Japan, it is hard for emergency medical technicians to intervene actively at the trauma scene outside of the hospital, except when they are associated with the small number of helicopter ambulances and ambulances with doctors.[21,22] Thus, this scoring system may not apply to other countries, which are associated with extensive intervention at the site. Second, patients with missing data were excluded, possibly introducing selection bias. Third, we did not have data of patients daily activity, underlying diseases, and medications. Due to their underlying illnesses, most elderly usually take some medications, which could influence their VS. Fourth, it is not clear whether patients received appropriate treatment either at the site, the ED, or the ward after hospital admission. Fifth, this current study did not design to add different points to each ΔVS, since we focused on simple use on the site for anyone, rather than for accuracy.[23,24] Finally, our study was retrospective and the results should be validated in a prospective study. A reduction of under-triage rates may be achieved using our ΔVS score; this also warrants evaluation. An optimal trauma score ideally provides higher predictive performance with simpler design.
5. Conclusions
Our novel trauma scoring system, the ΔVS score, focuses on changes in vital signs and predicts in-hospital mortality. It may be useful in improving an emergency physicians decision-making process regarding identification of patients needing close monitoring for critical care services. Validation studies are required.
Acknowledgments
We would like to thank Editage (www.editage.jp) for English language editing.
Author contributions
KK conceived and designed this study, interpreted the data, drafted the manuscript, and revised the manuscript for important intellectual content. TA contributed to the acquisition of data, conceived and designed this study, interpreted the data, drafted the manuscript, and revised the manuscript for important intellectual content. MA contributed to the acquisition of data, conducted data cleaning, interpreted the data, and revised the manuscript for important intellectual content. GD interpreted the data and revised the manuscript for important intellectual content. SD conceived and designed this study, interpreted the data, and revised the manuscript for important intellectual content. YT interpreted the data and revised the manuscript for important intellectual content. All of the authors approved the final manuscript.
Conceptualization: Kazuhiro Kamata, Toshikazu Abe, Daizoh Saitoh, Yasuharu Tokuda.
Data curation: Kazuhiro Kamata, Toshikazu Abe, Makoto Aoki, Gautam Deshpande.
Formal analysis: Toshikazu Abe, Makoto Aoki.
Funding acquisition: Toshikazu Abe.
Methodology: Kazuhiro Kamata, Toshikazu Abe, Yasuharu Tokuda.
Resources: Toshikazu Abe, Daizoh Saitoh.
Software: Toshikazu Abe, Makoto Aoki.
Supervision: Daizoh Saitoh, Yasuharu Tokuda.
Validation: Toshikazu Abe, Makoto Aoki.
Visualization: Kazuhiro Kamata.
Writing – original draft: Kazuhiro Kamata, Toshikazu Abe.
Writing – review & editing: Kazuhiro Kamata, Toshikazu Abe, Makoto Aoki, Gautam Deshpande, Daizoh Saitoh, Yasuharu Tokuda.
Footnotes
Abbreviations: ΔHR = heart rate increase, ΔRR = respiratory rate increase, −ΔSBP = systolic blood pressure reduction, ΔVS = changes in vital signs, AIS = Abbreviated Injury Scale, CI = confidence interval, ED = emergency department, HR = heart rate, ISS = Injury Severity Score, JTDB = Japan Trauma Data Bank, NEWS = National Early Warning Score, RR = respiratory rate, RTS = Revised Trauma Score, SBP = systolic blood pressure, SD = standard deviation, VS = vital signs.
How to cite this article: Kamata K, Abe T, Aoki M, Deshpande G, Saitoh D, Tokuda Y. Dynamic vital signs may predict in-hospital mortality in elderly trauma patients. Medicine. 2020;99:25(e20741).
This work was supported by JSPS KAKENHI JP 16K15388, Japan.
We have presented this research at (European society of intensive medicine) ESICM Live 2016.
All authors declare that they have no competing interests.
The datasets generated during and/or analyzed during the current study are not publicly available, but are available from the corresponding author on reasonable request.
References
- [1].Champion HR, Sacco WJ, Copes WS, et al. A revision of the Trauma Score. J Trauma 1989;29:623–9. [DOI] [PubMed] [Google Scholar]
- [2].Boyd CR, Tolson MA, Copes WS. Evaluating trauma care: the TRISS method. Trauma Score and the Injury Severity Score. J Trauma 1987;27:370–8. [PubMed] [Google Scholar]
- [3].Sartorius D, Le Manach Y, David JS, et al. Mechanism, glasgow coma scale, age, and arterial pressure (MGAP): a new simple prehospital triage score to predict mortality in trauma patients. Crit Care Med 2010;38:831–7. [DOI] [PubMed] [Google Scholar]
- [4].Omri M, Bouaouina H, Kraiem H, et al. Missed injuries in pre-hospital trauma patients. Tunis Med 2017;95:336–40. [PubMed] [Google Scholar]
- [5].Bruijns SR, Guly HR, Bouamra O, et al. The value of the difference between ED and prehospital vital signs in predicting outcome in trauma. Emerg Med J 2014;31:579–82. [DOI] [PubMed] [Google Scholar]
- [6].Lehmann R, Beekley A, Casey L, et al. The impact of advanced age on trauma triage decisions and outcomes: a statewide analysis. Am J Surg 2009;197:571–4. discussion 4–5. [DOI] [PubMed] [Google Scholar]
- [7].Scheetz LJ. Effectiveness of prehospital trauma triage guidelines for the identification of major trauma in elderly motor vehicle crash victims. J Emerg Nurs 2003;29:109–15. [DOI] [PubMed] [Google Scholar]
- [8].Ouchi Y, Rakugi H, Arai H, et al. Redefining the elderly as aged 75 years and older: proposal from the Joint Committee of Japan Gerontological Society and the Japan Geriatrics Society. Geriatr Gerontol Int 2017;17:1045–7. [DOI] [PubMed] [Google Scholar]
- [9].Annual Report Task Force of Japan Trauma Data Bank. Japan Trauma Data Bank Report 2018 (2013–2017). https://www.jtcr-jatec.org/traumabank/dataroom/data/JTDB2018e.pdf. Published December 25, 2018. Accessed May 29, 2020. [Google Scholar]
- [10].Joseph B, Haider A, Ibraheem K, et al. Revitalizing vital signs: the role of Delta Shock Index. Shock 2016;46: 3 Suppl 1: 50–4. [DOI] [PubMed] [Google Scholar]
- [11].Schellenberg M, Strumwasser A, Grabo D, et al. Delta Shock Index in the emergency department predicts mortality and need for blood transfusion in trauma patients. Am Surg 2017;83:1059–62. [DOI] [PubMed] [Google Scholar]
- [12].Kellett J, Wasingya-Kasereka L, Brabrand M, et al. Are changes in objective observations or the patient's subjective feelings the day after admission the best predictors of in-hospital mortality? An observational study in a low-resource sub-Saharan hospital. Resuscitation 2018;135:130–6. [DOI] [PubMed] [Google Scholar]
- [13].Brekke IJ, Puntervoll LH, Pedersen PB, et al. The value of vital sign trends in predicting and monitoring clinical deterioration: a systematic review. PLoS One 2019;14:e0210875. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Baker SP, O’Neill B, Haddon W, Jr, et al. The injury severity score: a method for describing patients with multiple injuries and evaluating emergency care. J Trauma 1974;14:187–96. [PubMed] [Google Scholar]
- [15].Inoue J, Shiraishi A, Yoshiyuki A, et al. Resuscitative endovascular balloon occlusion of the aorta might be dangerous in patients with severe torso trauma: a propensity score analysis. J Trauma Acute Care Surg 2016;80:559–66. discussion 66–7. [DOI] [PubMed] [Google Scholar]
- [16].Kahloul M, Bouida W, Boubaker H, et al. Value of anatomic and physiologic scoring systems in outcome prediction of trauma patients. Eur J Emerg Med 2014;21:125–9. [DOI] [PubMed] [Google Scholar]
- [17].Barea-Mendoza JA, Chico-Fernandez M, Sanchez-Casado M, et al. Predicting survival in geriatric trauma patients: a comparison between the TRISS methodology and the Geriatric Trauma Outcome Score. Cir Esp 2018. [DOI] [PubMed] [Google Scholar]
- [18].Tokuda Y, Richard BB. Early recognition of sepsis. anaesthesia. Crit Care Pain Manag 2016;1:1–2. [Google Scholar]
- [19].Heffernan DS, Thakkar RK, Monaghan SF, et al. Normal presenting vital signs are unreliable in geriatric blunt trauma victims. J Trauma 2010;69:813–20. [DOI] [PubMed] [Google Scholar]
- [20].Liu NT, Holcomb JB, Wade CE, et al. Improving the prediction of mortality and the need for life-saving interventions in trauma patients using standard vital signs with heart-rate variability and complexity. Shock 2015;43:549–55. [DOI] [PubMed] [Google Scholar]
- [21].Hirano Y, Abe T, Tanaka H. Efficacy of the presence of an emergency physician in prehospital major trauma care: a nationwide cohort study in Japan. Am J Emerg Med 2018. [DOI] [PubMed] [Google Scholar]
- [22].Abe T, Takahashi O, Saitoh D, et al. Association between helicopter with physician versus ground emergency medical services and survival of adults with major trauma in Japan. Crit Care 2014;18:R146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Kondo Y, Abe T, Kohshi K, et al. Revised trauma scoring system to predict in-hospital mortality in the emergency department: glasgow coma scale, age, and systolic blood pressure score. Crit Care 2011;15:R191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Moore L, Lavoie A, Abdous B, et al. Unification of the revised trauma score. J Trauma 2006;61:718–22. discussion 22. [DOI] [PubMed] [Google Scholar]