

Abstract
To evaluate tooth behaviours under various maxillary incisor retraction protocols for clear aligner therapy. A three-dimensional finite element model of maxillary dentition was constructed for first premolar extraction. A loading method was developed to mimic the mode of action of clear aligners for incisor en masse retraction. Three protocols with different amounts of retraction and intrusion on incisors were designed. Initial tooth displacements and stresses on periodontal ligaments were analysed with ANSYS software. The central (U1) and lateral (U2) incisors exhibited uncontrolled lingual tipping and extrusion upon 0.25 mm retraction. U1 exhibited translation movement, while U2 underwent less tipping during 0.2 mm retraction and 0.15 mm intrusion. Labial tipping and intrusion of U1 and bodily intrusion of U2 were observed during 0.1 mm of retraction and 0.23 mm of intrusion. With the additional intrusion on incisors, canine showed extrusion movement, and higher stresses on periodontal ligaments were shifted from U2 to canines. Incisors also exhibited different mesial-distal angulation in the three simulations, while posterior teeth all suffered mesial inclination. Incorporating intrusion displacement in clear aligners led to a tendency of lingual root movement during incisor retraction. The complexity of tooth movement should be recognized regarding clear aligner therapy.
Subject terms: Dental treatment planning, Cone-beam computed tomography
Introduction
In 1997, Align Technology (Align Technology, California, USA) introduced clear aligner treatment (CAT). In this system, serial thermoplastic aligners were produced based on the stages of tooth movement simulated in a computer. Each aligner is worn for 1 to 2 weeks to gradually move misaligned teeth to planned positions. As an inconspicuous alternative to traditional fixed instruments, CAT has attracted an increasing number of adult patients seeking orthodontic therapy1.
In the early stages, clear aligners were only considered to treat simple orthodontic problems of mild or moderate anterior crowding2. With the development of computer technology and the gradual recognition of the biomechanical properties of aligner materials, CAT has demonstrated the capacity to treat more complex cases, such as cases requiring tooth extraction3–6. Nevertheless, these case reports pointed out the limitations of using clear aligners to complete the gap closure in extraction treatment. Clear aligners are not rigid enough to retain their original shape in space closure, which might result in torque loss and adverse extrusion of the anterior teeth7–10. Therefore, a certain amount of intrusion is intentionally added during the setup when the incisors are designed to be retracted. However, the effectiveness of extra intrusion in controlling the movement of incisors has not been proven, and the most efficient ratio between the amount of retraction and intrusion is unclear.
Finite element analysis can calculate initial tooth movement instantly after force loading. It has been widely used in biomechanics to analyse the stress and strain response of external forces in residential structures and has been demonstrated to be an effective tool to simulate tooth displacement patterns in orthodontics11,12.
The purpose of this study is to determine the behaviours and stress distributions of both anterior and posterior teeth under different amounts of retraction and intrusion protocols with clear aligners by three-dimensional finite element (3D FE) analysis.
Methods
3D FE models of the maxillary dentition with extracted first premolars, periodontal ligaments (PDLs), and alveolar bone were built using GEOMAGIC studio (Raindrop Geomagic, North Carolina, USA). Teeth and maxillary bone were reconstructed based on cone-beam computed tomography (CBCT) scanning of an adult male subject with well-aligned dentition and a normal upper incisor to maxillary plane of 110 degrees13. PDLs were fabricated as a linear elastic film with an average thickness of 0.25 mm around the roots of all teeth14. To simulate a sequential pattern of space closure by which canines were distalized first followed by en masse retraction of incisors, a 0.5 mm space was designed in the model between canines and lateral incisors15. Horizontal rectangular attachments (2 mm height, 3 mm width, and 1 mm thickness) were designed for lateral incisors, and vertical rectangular attachments (3 mm height, 2 mm width, and 1 mm thickness) were designed for teeth other than centre incisors. The aligners had a thickness of 0.38 mm, in which external offset devices for all crowns and attachments were developed in the simulation (Fig. 1A,B)16. All components were imported for FE analysis by ANSYS Workbench 15.0 (Ansys, Pennsylvania, USA).
Figure 1.

Three-dimensional finite element model for incisor retraction in a 1st premolar extraction case. (A) Maxillary arch with 1st premolar removal and attachments on the vestibular surfaces of crowns. (B) Geometric model of the clear aligner. (C) Mesh division on the model assembly with the aligner on dentition.
Material properties
Teeth and attachments were regarded as isotropic and homogeneous materials with rigid stiffness properties, while PDLs were set up as hyperelastic materials to mimic its true mechanical properties as much as possible. In the calculation of the stress on the PDLs, the alveolar bone was designed as a rigid body. Aligners were set as isotropic and homogeneous materials (Table 1).
Table 1.
Material properties used in FE model.
| Material | Young’s modulus (MPa) | Poisson’s ratio |
|---|---|---|
| Tooth | 1.96 * 104 | 0.30 |
| Periodontal ligament | 0.69 | 0.45 |
| Alveolar bone | 1.37 * 103 | 0.30 |
| Attachments | 12.5 * 103 | 0.36 |
| Clear aligner | 528 | 0.36 |
The FE mesh was divided by the discretization process, and 234,691 nodes and 13,101 linear elements were generated (Fig. 1C). A friction condition was established in contact interfaces between the aligner and tooth crown surface and attachments, with a friction coefficient of μ = 0.217.
Establishment of a coordinate system
The mesial incisal points of the central incisors and mesial cusp tips of the bilateral first molars were used to define the occlusal plane18. The X-axis represents the direction of the coronal plane with the positive direction being towards the mesial surface of the tooth; the Y-axis represents the sagittal plane with the positive direction being towards the lingual surface; and the Z-axis represents the vertical plane with the positive direction being towards the gingival tissue.
Configuration setting
Three retraction protocols were proposed (Fig. 2):
Configuration 1 (A1): retraction of incisors bodily by 0.25 mm along the occlusal plane,
Configuration 2 (A2): 0.2 mm retraction with 0.15 mm intrusion, and
Configuration 3 (A3): 0.1 mm retraction with 0.23 mm intrusion.
Figure 2.

Loading method of the finite element model to simulate incisor retraction with a clear aligner. The incisors were first displaced in the opposite direction of retraction (A). This led to the deformation of the aligner matching the dentition (B). The forces generated by the aligner on each tooth were then calculated and finally loaded back on the corresponding tooth in the reverse direction (C). Three retraction protocols were designed with different amounts of retraction and intrusion with the same total amount of movement of 0.25 mm (A1, A2 and A3). Dashed arrows indicate the vectors of incisor displacement that activate the aligner. Solid arrows indicate the vectors of the designed incisor retraction.
For all three protocols, the distance of movement measured on the tip of the root was 0.25 mm, as recommended by Invisalign19,20.
Loading method
To mimic the action of the aligner on the tooth in the FE model, a new loading method was developed (Fig. 2). In configuration 1, for example, the incisors were intended to be retracted by 0.25 mm (Fig. 2A1). The incisors were first translated labially along the occlusal plane for 0.25 mm (Fig. 2A). This led to the deformation of the aligner fitting on the dentition (Fig. 2B). The forces generated by the aligner on each tooth were then calculated by the software and then loaded back on the corresponding tooth in the reverse direction (Fig. 2C).
Informed consent for study participation was obtained, and the use of the CBCT data was approved by the Ethics Committee of Shanghai Ninth People’s Hospital (SH9H-2018-T63-1). All experiments were approved and performed in accordance with relevant guidelines and regulations.
Results
During incisor en masse retraction, different force systems and behaviours of both anterior and posterior teeth were recorded among the three performed simulations (Figs. 3–5). To facilitate the comparison, the coordinate values under different simulations were unified for each tooth type.
Figure 3.
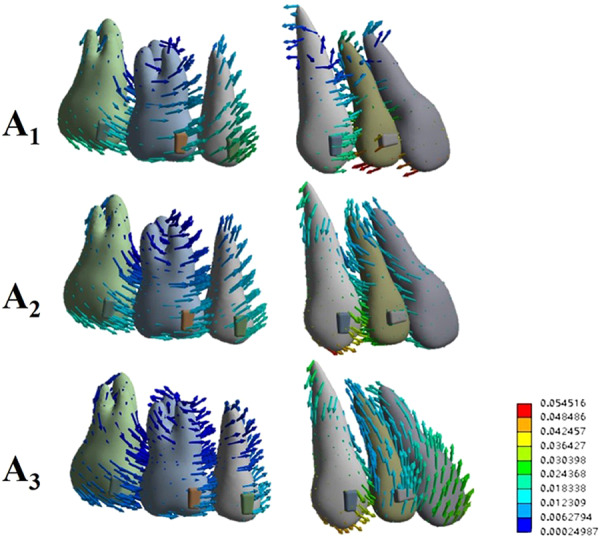
Vector analysis of the overall displacement pattern of the dentition for the three incisor retraction protocols: A1, A2 and A3.
Figure 5.

Stress distribution around the periodontal ligament of each tooth for the three incisor retraction protocols: A1, A2 and A3.
A1: 0.25 mm retraction
Upon this retraction protocol, both central and lateral incisors experienced maximum lingual displacement on incisal edges, while the root apex performed a movement in the labial direction, resulting in uncontrolled lingual tipping movement. In contrast, the canine and posterior teeth exhibited mesial inclination (Fig. 3A1).
Detailed analysis of anterior tooth displacement showed that both central and lateral incisors had distal crown and mesial root tipping (Fig. 4A1, X-axis). The lingual tipping movement (Y-axis) was accompanied by extrusion on the labial surfaces (Z-axis). Canines exhibited mesial crown tipping, intrusion and minor mesial lingual rotation.
Figure 4.

The displacement pattern of incisors and canines in each direction for the three incisor retraction protocols: A1, A2 and A3.
The maximum stress on the PDL was located at the root apex of the lateral incisor, followed by the cervical area of the lateral and central incisors (Fig. 5A1). For posterior teeth, the mesial cervical area of the 2nd premolar and distal cervical area of the 2nd molar also showed higher stress.
A2: 0.2 mm retraction and 0.15 mm intrusion
The displacements in the crown and root of the central incisor were relatively uniform, indicating bodily movement (Figs. 3A2 and 4A2). The lateral incisors still underwent a lingual tipping movement, albeit less apparent than that in A1. While both incisors showed intrusion movement, more intrusion was noted on lateral incisors. Compared to A1, both incisors displayed less distal crown angulation (X-axis). Canine and posterior teeth also exhibited mesial tipping movements. However, lingual crown tipping and extrusion were noted on canines. The stress on the PDL was now concentrated at the apical area of the canine (Fig. 5A2). The amount of stress on the posterior teeth was decreased when compared to that in A1.
A3: 0.1 mm retraction and 0.23 mm intrusion
The maximum displacement of the central incisor was observed on the crown, showing a labial crown tipping movement, and the intrusion was significant (Figs. 3A3 and 4A3). The movement pattern of the lateral incisor resembled bodily intrusion with minor labial crown tipping. Unlike in A1 or A2, in A3, the incisors exhibited mesial crown tipping on the X-axis (Fig. 4A3). Canines exhibited very similar displacement to that observed in A2, with mesial crown tipping, extrusion and slightly more lingual crown tipping. The stresses on the PDL were also concentrated at the apical area of the canine, while the stresses were smaller and more uniform on incisors and posterior teeth (Fig. 5A3).
The stress distributions on attachments were similar among the three simulations. Higher stresses were concentrated on the gingival surfaces of the lateral incisor and 2nd premolar, mesial surfaces of canines, and distal surfaces of molars (Fig. 6). The maximum stresses were noted on the 2nd premolars for all the simulations. Much lower stresses were observed on the 1st molar attachments, and the lowest were recorded on the 2nd molars. With the increase in intrusion on incisors, the stresses on the gingival surfaces of the attachments on the 1st and 2nd molars increased.
Figure 6.

Stress distribution around the attachments for the three incisor retraction protocols: A1, A2 and A3. Surfaces with higher stresses are illustrated.
Discussion
Despite the growing consumer demand and worldwide use of clear aligners to treat misaligned teeth, several concerns regarding the efficacy of the system in controlling tooth movement remain. The tooth movement achieved upon aligner therapy differs from the tooth movement planned by the virtual setup21. This less predictable movement might be due to the fact that the force-transmission mechanisms of clear aligners are not yet well clarified. In fixed-appliance treatment, the force originating from metal wire and bracket interactions is transmitted to a certain point on the tooth, causing displacement. In contrast, clear aligner therapy outcomes are the result of a predetermined mismatch between the tooth and aligner. The force application point is ever changing, and the direction and amount of the force are very elusive.
Several experimental approaches have been carried out on the biomechanics of possible tooth movement with clear aligners. Compared to displacement measurements and strain gauge measurements, 3D FE analysis has the advantage of taking periodontal tissues into consideration and can calculate the stress, strain and displacement of any part of the tooth and aligner11,22–27. However, most FE studies on clear aligners were limited to a single tooth or a segment of teeth11,22–24,26. In addition, the loading method was conventionally described as moving the assembled aligner directly, which was inconsistent with clinical reality26. In this study, the incisors were first forced in the reverse direction of retraction to activate the aligner. The forces resulting from the deformation of the aligner were then calculated by FE analysis, which were in turn loaded back on the corresponding teeth. The contact interfaces between the aligner and the crown surface and attachments were set to a friction coefficient of 0.2, thus mimicking the mode of action of a shape-mismatched aligner on the dentition. To our knowledge, this is the first time that a clear aligner FE model with intact maxillary dentition and attachments was constructed, and different protocols of tooth movement were analysed. The results showed that the method was practical and reliable.
Controlling the movement of incisors at will is a challenge for extraction treatment. In most cases, translation or controlled tipping is preferred for the retraction of upper incisors. In fixed appliances, the moment/force ratios at the bracket are the primary determinant of controlling the tooth movement28,29. It can also be achieved by positioning mini-screws and hooks to adjust the “line of force” related to the centre of resistance of the anterior segment in sliding mechanics30,31. However, the biomechanics of en masse retraction of incisors with clear aligners are not well understood.
Previous studies have reported that clear aligners caused tooth movement mainly by tilting motions and that bodily movement for extraction space closure was less successful1,21. Our present study showed that incisors exhibited uncontrolled tipping and undesired extrusion when bodily retraction was designed (Fig. 3). Thus, similar to fixed appliances, a “bowing effect” would occur during incisor retraction with clear aligners. This might be caused by forces acting below the resistance centres of the four incisors, and the aligner was not rigid enough to hold the teeth vertically. It is thus logical to allow for a certain amount of intrusion during the retraction movement. According to Invisalign, tooth movement is limited within 0.25 mm per stage19,20. Therefore, we designed two retraction and intrusion combinations for incisors, and the total movement amount was 0.25 mm (Fig. 2). On the basis of our FE results, intrusion movement helped generate a force system that approximated the bodily movement of incisors. As the amount of intrusion movement increased, the root movement in the lingual direction became more prominent. However, this tendency declined from the centre to the lateral sides, which produced inconsistent types of movement between the central and lateral incisors. Apart from their different positions in the dental arch, the discrepancy between central and lateral incisors might result from the different anatomical configurations of the crowns.
Anchorage is another major concern during space closing in extraction cases. To maximize the anchorage value of the posterior segment, a protocol of sequential retraction of the canines and incisors was recommended15. Our present study adopted this concept so that 0.5 mm space was created mesial to the canines on the FE model to mimic canine distalization. This gap also increased the aligner surface area around the canine and incisor crowns. Meanwhile, the flexibility of the edentulous span of the aligner distal to the incisor segment was effectively reduced by canine positioning15. In our results, the posterior teeth and canines showed similar mesial tipping movement in the three protocols. With the decrease in the amount of retraction in A2 and A3, less mesial migration of the posterior teeth was observed. However, canines revealed more extrusion displacement when more intrusion was planned on the incisors (Figs. 3 and 4). Higher stresses on canine PDLs were detected (Fig. 5). Based on these results, intraoral elastics could be placed on canines to reinforce anchorage. Taking the vertical movement of canines into consideration, class II elastics should be used for protocol A1, and elastics supported by mini-screws on posterior maxillary bone would be beneficial for protocols A2 and A3.
Auxiliaries such as attachments were mandatory in clear aligner therapy to achieve desired results25,26,32. While some reports pointed out that customized attachments could facilitate complex movements, others failed to find significant differences in the shape and position of attachments on tooth movement16,20,22,26. Most likely, the effect of the attachment would depend on the shape of the tooth. In our present study, only conventional rectangular attachments were used for convenience. Much higher stresses on the PDLs and gingival surfaces of the attachments were detected on lateral incisors (Figs. 5 and 6). These results were in agreement with previous findings that upper lateral incisors commonly come off track during space closure, and horizontal bevelled attachments are recommended for better retention33. Higher stresses were also observed on the gingival surfaces of the attachments on the 1st and 2nd molars when more intrusion was placed on incisors (Fig. 6). This emphasized the significance of the attachments on molars to support incisor intrusion.
Considering all the results obtained through the finite element analysis, it could be stated that the incisors underwent a transition from uncontrolled tipping to gradual root-controlled movement after intrusion displacements were planned. It is worth noting that intrusion was always accompanied by various movement types. Thus, assessment before treatment was indispensable from a clinical perspective. For patients with a deep overbite, more intrusion could not only contribute to improving the occlusion but also lead to good control of root lingual movements. Moreover, the different movement types on incisors draw attention to the clinical aspects of biomechanical analysis, showing that different forces might be loaded on incisors, which should be considered by orthodontists when planning clear aligner therapy.
Our present results were based on the fact that the upper incisors were on normal labiolingual inclination. Calibrating the amount of intrusion and retraction movement in detail according to different inclinations of incisors would help clinicians with treatment planning for individual cases. Although the reliability of finite element analysis must be verified, further studies examining different thicknesses and configurations of the aligners, as well as various attachment designs, should be carried out for a better understanding of clear aligner treatment.
Conclusions
In this study, a unique loading method was developed to mimic the mode of action of clear aligners for anterior en masse retraction in a 3D FE model. The results showed that incorporating intrusion displacement on aligners led to a tendency of lingual root movement for incisor retraction. The discrepancy between the tooth movement displayed in the FE model and the tooth movement planned for incisors reiterated the complexity of the force system in clear aligner therapy.
Acknowledgements
This work was supported by Natural Science Foundation of Shanghai (19ZR1429600).
Author contributions
T.J. drafted the work and was responsible for the acquisition of the data for the work. R.Y.W., J.K.W., and H.H.W. organized and analysed the data for the work. Professor G.H.T. made substantial contributions to the concept of the work and finally approved of the version to be published.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
These authors contributed equally: Ting Jiang and Rui Ying Wu.
References
- 1.Rossini G, Parrini S, Castroflorio T, Deregibus A, Debernardi CL. Efficacy of clear aligners in controlling orthodontic tooth movement: A systematic review. Angle Orthod. 2015;85:881–889. doi: 10.2319/061614-436.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Joffe L. Invisalign®: early experiences. J. Orthod. 2003;30:348–352. doi: 10.1093/ortho/30.4.348. [DOI] [PubMed] [Google Scholar]
- 3.Zawawi KH. Orthodontic treatment of a mandibular incisor extraction case with Invisalign. Case Rep. Dent. 2014;2014:657657. doi: 10.1155/2014/657657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Honn M, Goz G. A premolar extraction case using the Invisalign system. J. Orofac. Orthop. 2006;67:385–394. doi: 10.1007/s00056-006-0609-6. [DOI] [PubMed] [Google Scholar]
- 5.Womack WR. Four-premolar extraction treatment with Invisalign. J. Clin. Orthod. 2006;40:493–500. [PubMed] [Google Scholar]
- 6.Choi NC, Park YC, Jo YM, Lee KJ. Combined use of miniscrews and clear appliances for the treatment of bialveolar protrusion without conventional brackets. Am. J. Orthod. Dentofac. Orthop. 2009;135:671–681. doi: 10.1016/j.ajodo.2006.12.025. [DOI] [PubMed] [Google Scholar]
- 7.Bowman SJ. Improving the predictability of clear aligners. Semin. Orthod. 2017;23:65–75. doi: 10.1053/j.sodo.2016.10.005. [DOI] [Google Scholar]
- 8.Vardimon AD, Robbins D, Brosh T. In-vivo von Mises strains during Invisalign treatment. Am. J. Orthod. Dentofac. Orthop. 2010;138:399–409. doi: 10.1016/j.ajodo.2008.11.027. [DOI] [PubMed] [Google Scholar]
- 9.Simon M, Keilig L, Schwarze J, Jung BA, Bourauel C. Forces and moments generated by removable thermoplastic aligners: incisor torque, premolar derotation, and molar distalization. Am. J. Orthod. Dentofac. Orthop. 2014;145:728–736. doi: 10.1016/j.ajodo.2014.03.015. [DOI] [PubMed] [Google Scholar]
- 10.Bowman SJ, et al. Creative adjuncts for clear aligners, part 3: Extraction and interdisciplinary treatment. J. Clin. Orthod. 2015;49:249–262. [PubMed] [Google Scholar]
- 11.Geramy A, Shahroudi AS. Fixed versus Removable Appliance for Palatal Expansion; A 3D Analysis Using the Finite Element Method. J. Dent. 2014;11:75–84. [PMC free article] [PubMed] [Google Scholar]
- 12.Hedayati Z, Shomali M. Maxillary anterior en masse retraction using different antero-posterior position of mini screw: a 3D finite element study. Prog. Orthod. 2016;17(2016):31. doi: 10.1186/s40510-016-0143-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ellis E, McNamara JA. Cephalometric evaluation of incisor position. Angle Orthod. 1986;56:324–344. doi: 10.1043/0003-3219(1986)056<0324:CEOIP>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 14.Wang CY, et al. Tension-compression viscoelastic behaviors of the periodontal ligament. J. Formos. Med. Assoc. 2012;111:471–481. doi: 10.1016/j.jfma.2011.06.009. [DOI] [PubMed] [Google Scholar]
- 15.Samoto H, Vlaskalic V. A customized staging procedure to improve the predictability of space closure with sequential aligners. J. Clin. Orthod. 2014;48:359–367. [PubMed] [Google Scholar]
- 16.Comba B, Parriini S, Rossini G, Castroflorio T, Deregibus A. A Three-Dimensional Finite Element Analysis of Upper-Canine Distalization with Clear Aligners, Composite Attachments, and Class II Elastics. J. Clin. Orthod. 2017;51:24–28. [PubMed] [Google Scholar]
- 17.Ramalho A, Vale Antunes P. Reciprocating wear test of dental composites against human teeth and glass. Wear. 2007;263:1095–1104. doi: 10.1016/j.wear.2007.01.086. [DOI] [Google Scholar]
- 18.Sushma K, Rajendra BH, Praveenkumar SM. An assessment of curve of spee in healthy human permanent dentitions: a cross sectional analytical study in a group of young indian population. J. Clin. Diagn. Res. 2017;11:ZC53–ZC57. doi: 10.7860/JCDR/2017/22839.9184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kravitz ND, Kusnoto B, Begole E, Obrez A, Agran B. How well does Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with Invisalign. Am. J. Orthod. Dentofac. Orthop. 2009;135:27–35. doi: 10.1016/j.ajodo.2007.05.018. [DOI] [PubMed] [Google Scholar]
- 20.Goto M, Yanagisawa W, Kimura H, Inou N, Maki K. A method for evaluation of the effects of attachments in aligner-type orthodontic appliance: Three-dimensional finite element analysis. Orthodontic Waves. 2017;76:207–214. doi: 10.1016/j.odw.2017.09.001. [DOI] [Google Scholar]
- 21.Zhang XJ, et al. Integrated three-dimensional digital assessment of accuracy of anterior tooth movement using clear aligners. Korean J. Orthod. 2015;45:275–281. doi: 10.4041/kjod.2015.45.6.275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hahn W, et al. Torquing an upper central incisor with aligners–acting forces and biomechanical principles. Eur. J. Orthod. 2010;32:607–613. doi: 10.1093/ejo/cjq007. [DOI] [PubMed] [Google Scholar]
- 23.Hahn W, et al. Influence of thermoplastic appliances’ thickness on the magnitude of force delivered to a maxillary central incisor during tipping. Am. J. Orthod. Dentofac. Orthop. 2009;136:e1–7. doi: 10.1016/S0889-5406(09)00737-9. [DOI] [PubMed] [Google Scholar]
- 24.Hahn W, et al. Initial forces and moments delivered by removable thermoplastic appliances during rotation of an upper central incisor. Angle Orthod. 2010;80:239–246. doi: 10.2319/033009-181.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Cortona A, Rossini G, Parrini S, Deregibus A, Castroflorio T. Clear aligner orthodontic therapy of rotated mandibular round-shaped teeth: A finite element study. Angle Orthod. 2020;90:247–254. doi: 10.2319/020719-86.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Gomez JP, Peña FM, Martínez V, Giraldo DC, Cardona CI. Initial force systems during bodily tooth movement with plastic aligners and composite attachments: A three-dimensional finite element analysis. Angle Orthod. 2015;85:454–460. doi: 10.2319/050714-330.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kohda N, et al. Effects of mechanical properties of thermoplastic materials on the initial force of thermoplastic appliances. Angle Orthod. 2013;83:476–483. doi: 10.2319/052512-432.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Tanne K, Koenig HA, Burstone CJ. Moment to force ratios and the center of rotation. Am. J. Orthod. Dentofac. Orthop. 1988;94:426–431. doi: 10.1016/0889-5406(88)90133-3. [DOI] [PubMed] [Google Scholar]
- 29.Kusy RP, Tulloch JF. Analysis of moment/force ratios in the mechanics of tooth movement. Am. J. Orthod. Dentofac. Orthop. 1986;90:127–131. doi: 10.1016/0889-5406(86)90044-2. [DOI] [PubMed] [Google Scholar]
- 30.Lee KJ, et al. Displacement pattern of the maxillary arch depending on miniscrew position in sliding mechanics. Am. J. Orthod. Dentofac. Orthop. 2011;140:224–232. doi: 10.1016/j.ajodo.2010.05.020. [DOI] [PubMed] [Google Scholar]
- 31.Tominaga J, et al. Effect of bracket slot and archwire dimensions on anterior tooth movement during space closure in sliding mechanics: A 3 dimensional finite element study. Am. J. Orthod. Dentofac. Orthop. 2014;146:166–174. doi: 10.1016/j.ajodo.2014.04.016. [DOI] [PubMed] [Google Scholar]
- 32.Barone S, Paoli A, Razionale AV, Savignano R. Computational design and engineering of polymeric orthodontic aligners. Int. J. Numer. Method. Biomed. Eng. 2017;2017:e2839. doi: 10.1002/cnm.2839. [DOI] [PubMed] [Google Scholar]
- 33.Bowman SJ, et al. Creative adjuncts for clear aligners, part 2: Intrusion, rotation, and extrusion. J. Clin. Orthod. 2015;49:162–172. [PubMed] [Google Scholar]