

Background: Statins reduce cardiovascular morbidity and mortality, but adherence is suboptimal. We hypothesised that adherence to statins determines survival in patients with peripheral artery disease (PAD).
Methods and results: Single centre observational study with 691 symptomatic PAD patients admitted to a tertiary university centre between 2010 and 2017. Mortality was evaluated over a mean follow-up of 50 ± 26 months. Statin adherence and LDL cholesterol (LDL-C) target attainment was related to total mortality.
Initially, 73% of the patients were on statins with an increase in statin use to 81% (p<0.0001) at follow-up. Statin dosage, normalised to simvastatin 40 mg, increased from 50 to 58 mg/day (p<0.0001), paralleled by a mean decrease of LDL-C from 97 to 82 mg/dl (p<0.0001). The proportion of patients on a high-intensity statin treatment increased over time from 38 to 62% (p<0.0001).
Patients never receiving statins had a higher mortality rate (34%) compared to patients on statins (20%) or having newly received a statin (15%; p<0.01). Moreover, patients on intensified statin medication had the lowest mortality (10%), whereas patients who terminated statin medication or reduced the statin dosage had a higher mortality rate (33% and 43%, respectively; p<0.05).
Figure 1.
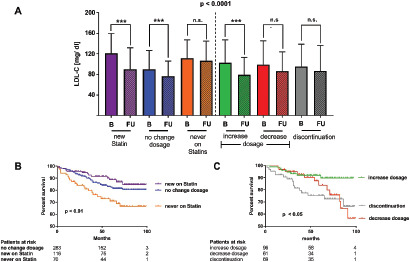
Conclusion: Statin treatment, particularly high-intensity therapy, reduces mortality in symptomatic PAD. Patients benefit even from de novo statin therapy, whereas dose reduction or statin discontinuation have deleterious effects. A strategy of intensive and sustained statin therapy is worthwhile.