

Abstract
The threat of a human pandemic of influenza has prompted the development of national influenza pandemic preparedness plans over the last 4 years. Analyses have been carried out to assess preparedness in Europe, Asia and Africa. We assessed plans to evaluate the national strategic pandemic influenza preparedness in the countries of Latin America.
Published national pandemic influenza preparedness plans from Latin American countries were evaluated against criteria drawn from the World Health Organization checklist. Plans were eligible for inclusion if formally published before 16 November 2007.
Fifteen national plans were identified and retrieved from the 17 Latin American countries surveyed. Latin American countries demonstrated different degrees of preparedness, and that a high level of completeness of plans was correlated to a country's wealth to a certain extent. Plans were judged strong in addressing surveillance requirements, and provided appropriate communication strategies directed to the general public and health care personnel. However, gaps remained, including the organization of health care services’ response; planning and maintenance of essential services; and the provision of containment measures such as the stockpiling of necessary medical supplies including vaccines and antiviral medications. In addition, some inconsistencies and variations which may be important, such as in border control measures and the capacity to contain outbreaks, exist between country plans—issues that could result in confusion in the event of a pandemic. A number of plans remain developmental in nature and, as elsewhere, more emphasis should be placed on strengthening the operability of plans, and in testing them. Whilst taking account of resources constraints, plans should be further developed in a coherent manner with both regional and international imperatives.
Keywords: Pandemic, influenza, Latin America, policy
KEY MESSAGES.
Most Latin American countries now have national strategic pandemic influenza preparedness plans.
Many plans are developmental in nature, although a minority includes more specific and operational guidelines to support pandemic response. Plans should be harnessed to generic preparedness.
Surveillance and communication areas are fairly well addressed while the health care sector and the use of public health interventions, notably related to pharmaceutical interventions, are ill-prepared for pandemic influenza. Contingency planning for essential services is largely absent from plans.
Operational planning needs further strengthening in most plans.
Introduction
The 1997 Hong Kong outbreak of a new strain of highly pathogenic avian influenza in humans reminded us that influenza pandemics have periodically affected humanity. Since then, the new avian influenza strain H5N1 has spread to three continents causing animal outbreaks and has infected more than 300 humans in 14 countries, resulting in high mortality rates (WHO 2008). The World Health Organization (WHO) is coordinating the global response to human cases of H5N1 avian influenza and guiding countries preparing for a pandemic of influenza by publishing guidelines, advice on rapid response and containment, and a checklist for influenza preparedness (WHO 2005a; WHO 2005b).
Currently, the Americas, together with Oceania, are regions that remain free of highly pathogenic avian influenza (HPAI) H5N1. Nevertheless, both North and South America have committed funds to the development of national strategic plans. We evaluate Latin America's plans in order to gain insights into the region's preparedness for pandemic influenza.
Design and data sources
We surveyed 17 Latin American countries (excluding the Caribbean) and evaluated each plan against criteria drawn from a WHO checklist (WHO 2005a). Published plans in the public domain were identified and sourced through the WHO, internet-based searches, and representatives of countries’ ministries of health. Plans were eligible for inclusion if formally published before 16 November 2007, when data collection finished. We evaluated national strategic plans and, where clear links were documented, references or annexes. We evaluated 14 plans in their original language, Spanish, and the Brazilian plan was evaluated in Portuguese and English.
A data extraction tool, based on the WHO checklist for influenza pandemic preparedness, was used (WHO 2005a). It was a modified version of the tool used in previous analyses by our team, which was designed in consultation with pandemic influenza planning experts (Mounier-Jack and Coker 2006; Coker and Mounier-Jack 2006). One hundred and twenty-seven criteria were defined and, for each criterion, plans were scored as either ‘present’ or ‘absent’, thus giving an indication of plans’ completeness. Preparedness plans were scored independently by two researchers, and agreement was arrived at when differences arose.
Countries’ preparedness plans were assessed in their entirety by seven thematic areas (WHO 2005a; WHO 2005b): planning and coordination, surveillance, public health interventions, health system response, maintenance of essential services, communication, and operational capacity.
Results
Fifteen Latin American plans were eligible for inclusion in our analysis (see Table 1 and Boxes 1 and 2). Nicaragua and Panama have developed preparedness plans but these were not publicly available at the time of data collection. The average completeness score of national plans was 48%, ranging from 24% to 69% (see Figures 1, 2 and 3).
Table 1.
Countries surveyed
| Country | Date of publication | No. pages | Source of plan/web reference | Date documents assessed |
|---|---|---|---|---|
| Countries included in the analysis | ||||
| Argentina | Jul 06 | 101 | http://municipios.msal.gov.ar/aviar/ | Oct 07 |
| Brazil | Nov 06 | 218 | http://dtr2001.saude.gov.br/influenza/principal_gripe.htm | Nov 07 |
| Bolivia | Nov 05 | 88 | http://www.sns.gov.bo/caratula/INFLUENZAAVIAR.pdf | Nov 07 |
| Chile | Aug 07 | 163 | http://www.pandemia.cl/ | Aug 07 |
| Colombia | Sep 05 | 21 | http://www.invima.gov.co/Invima/BVSalud/index.html | Aug 07 |
| Costa Rica | Nov 05 | 109 | http://www.col.ops-oms.org/repositorio/vertema.asp?id=67&idrepositorio=1 | Aug 07 |
| Ecuador | Dec 05/ Aug 06 | 82 | http://www.msp.gov.ec/ | Aug 07 |
| El Salvador | May 07 | 130 | Obtained from the Ministry of Health in El Salvador. (http://www.conapreviar.org/) | Nov 07 |
| Guatemala | May 07 | 103 | Obtained from the Ministry of Health Guatemala. Annexes of the plan are pending finalization. | Nov 07 |
| Honduras | Oct 05 | 31 | http://www.col.ops-oms.org/repositorio/vertema.asp?id=43&idrepositorio=1 | Aug 07 |
| Mexico | Dec 06 | 19 + 10 annexes | http://www.dgepi.salud.gob.mx/pandemia/FLU-aviar-PNPRAPI.htm | Aug 07 |
| Paraguay | Mar 06 | 91 | Obtained from Ministry of Health in Paraguay | Aug 07 |
| Peru | Jun 06, Aug 06, Jun 07 | 150 | http://www.minsa.gob.pe/portal/Especiales/aviar/default.asp http://www.oge.sld.pe/aviar/ | Aug 07 |
| Uruguay | Aug 07 | 57 + 11 annexes | http://www.bvsops.org.uy/pdf/influenza.pdf | Aug 07 |
| Venezuela | Jan 06 | 63 | http://www.mpps.gob.ve/ms/modules.php?name=Content&pa=showpage&pid=422 | Aug 07 |
| Countries not included in the analysis | ||||
| Nicaragua | plan exists but not publicly available | |||
| Panama | plan exists but received outside inclusion period | |||
Box 1 Countries included and not included in the analysis.
Included:
Argentina, Brazil, Bolivia, Chile, Colombia, Costa Rica, Ecuador, El Salvador, Guatemala, Honduras, Mexico, Paraguay, Peru, Uruguay, Venezuela
Not included:
Nicaragua, Panama
Box 2 Countries included by sub-regions (PAHO-WHO 2007b).
Southern Cone: Argentina, Chile, Paraguay, Uruguay
Andean Area: Bolivia, Colombia, Ecuador, Peru, Venezuela
Central America: Costa Rica, El Salvador, Guatemala, Honduras
North America: Mexico
Brazil
Figure 1.
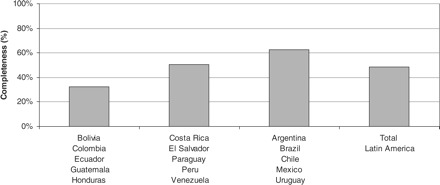
Aggregate completeness scores of preparedness plans by country group
Figure 2.
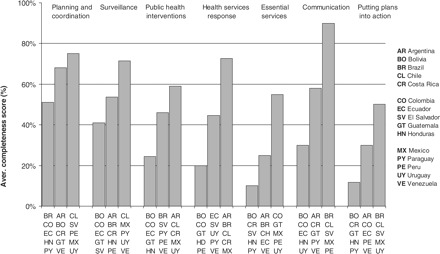
Completeness of preparedness plans by country group and thematic area. *Completeness score (%) is obtained by the number of criteria met by a country (with regards to a specific theme) divided by the number of criteria that evaluates that theme
Figure 3.
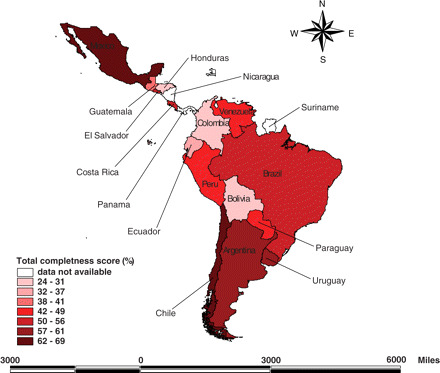
Completeness scores of preparedness plans by country
Seven countries scored 50% or more for overall completeness, whilst four countries scored 40% or less. Countries that scored less than 40% had developmental plans or preliminary versions which were incomplete. These plans focused on specific topics, such as planning and coordination, and surveillance systems. Overall, planning and coordination, surveillance, and communication themes were better developed than public health interventions, health services response and maintenance of essential services.
We found correlations between completeness scores and Gross Domestic Product (GDP) per capita (correlation coefficient = 0.69) and an inverse correlation with the proportion of the population living under the international poverty level (r = –0.65) (see Table 2 for details of GDP for the 15 countries).
Table 2.
Countries population and GDP per capita
| Population (*1000) | GDP (US$PPP) | |
|---|---|---|
| Lower middle income economies | ||
| Bolivia | 9354 | $3100 |
| Colombia | 46 279 | $8600 |
| Ecuador | 13 419 | $4500 |
| El Salvador | 6857 | $4900 |
| Guatemala | 12 911 | $5000 |
| Honduras | 7362 | $3100 |
| Paraguay | 6301 | $4800 |
| Peru | 28 380 | $6600 |
| Upper middle income economies | ||
| Argentina | 39 134 | $15 200 |
| Brazil | 188 883 | $8800 |
| Chile | 16 465 | $12 500 |
| Costa Rica | 4399 | $12 500 |
| Mexico | 108 327 | $10 700 |
| Uruguay | 3487 | $10 900 |
| Venezuela | 27 216 | $7200 |
Latin America has a total of approximately 518 774 millions of people and the average GPD is $7893 (CIA 2007).
Planning and coordination scored an average of 64%. All countries in the study had established a national committee to respond to pandemic influenza led by the Ministry of Health, in most countries in association with the Ministry of Animal Husbandry (in 14 plans). These countries stated that beyond WHO Pandemic Influenza Phase 3, communication between Ministries of Health and Ministry of Animal Husbandry would be strengthened. Thirteen countries organized their plan according to WHO pandemic influenza phases; among them Brazil, Bolivia, Mexico and Peru had developed specific sub-groupings of national phases, in line with WHO Pandemic Influenza phases.
Seven countries (Bolivia, Colombia, Costa Rica, El Salvador, Guatemala, Honduras and Peru) had made some estimate of the cost of planning and implementing their plans. Only Peru and Honduras had identified funding resources. Bolivia and Guatemala acknowledged that full implementation would not be possible unless external financial support is granted.
Thirteen countries have highlighted the need to update their legal framework to accommodate some critical public health measures. Only Chile and Mexico made explicit reference to addressing ethics and human rights principles during the response to a pandemic influenza. These issues include the enforcement of quarantine and compulsory vaccination.
Collaboration with the regional office of WHO for the Americas, the Pan American Health Organization (PAHO), was noted in 14 plans. This mainly involved notification to the WHO Global Influenza Surveillance Network, and participation in cross-regional pandemic influenza related workshops organized by PAHO (PAHO-WHO 2007a). Twelve countries referred to the need to comply with the WHO International Health Regulations.
Operational cooperation of national governments with neighbouring countries was poorly addressed. Even if 10 plans mentioned that coordination and collaboration would be needed with neighbouring countries, only three plans addressed the need to coordinate animal surveillance systems with those of neighbouring countries.
The average completeness score for surveillance in Latin America was 55%. All analysed plans reported having surveillance systems for seasonal influenza. These systems have been established during the last 7–10 years and they showed different levels of development: 14 countries gave detailed information on their sentinel surveillance systems, and some, such as Costa Rica, noted they are still planning to increase the number of sentinel posts. Plans from Paraguay and Guatemala mentioned the lack of budget and human resources to expand their surveillance capabilities. Thirteen plans noted the existence of at least one laboratory able to obtain routine influenza diagnostic typing and, when sub-typing was not available, countries planned to secure further testing through the Regional Reference Laboratory (CDC, Atlanta, US). Brazil planned to create cross-border links between national laboratories of both human and animal surveillance. In-country cooperation between animal and human surveillance networks was reported in 13 plans with varying levels of detail.
We found that only nine plans mentioned having outbreak investigation capacity, and some highlighted that investigation teams were often experienced in other disease outbreaks in the region.
The average completeness score for public health interventions for the region was 43%. The disparity between sub-regions was more pronounced than in the previous two themes, with Southern Cone countries scoring the highest (58%) and those from the Andean Region the lowest (29%). Triggers to activate the implementation of public health interventions before and during the epidemic were unclear in many plans. Interventions included those targeted at limiting the spread of the disease internationally (border control was envisaged in 12 countries and entry screening in two plans); reducing its spread nationally (quarantine was anticipated in 12 plans, closure of schools in eight plans); and reducing individuals’ risk of infection (personal hygiene measures were noted in nine plans, and use of masks for the general population in three plans) (Bell 2006). According to 15 plans analysed, only seven included an option for early containment of pandemic influenza. PAHO has, subsequent to the publication of those plans, supported member states with training and the creation of rapid response teams (PAHO-WHO 2007a).
Fourteen plans described a pandemic vaccine strategy, albeit with very limited details, and 10 defined priority groups for vaccination. Costa Rica was the only country that had estimated the size of its priority groups eligible for pandemic vaccination. Strategic measures targeting distribution (in seven plans) and storage (in five plans) of vaccines were poorly addressed by countries; only Brazil, El Salvador, Mexico and Uruguay provided specific details. Nevertheless, most countries acknowledged that they are unlikely to obtain enough vaccine to serve the whole of the population.
Countries addressed antiviral drug strategy very poorly. All plans acknowledged it was unlikely that antiviral medication would be available during the pandemic to all who needed it. Only four plans—Argentina, Chile, Costa Rica and Uruguay—had defined priority groups for the use of antivirals for treatment. In these four plans, the first priority group was either essential personnel (including health care workers) or individuals hospitalized. Other priority groups were those individuals over 65 years old, or children. Seven countries—Argentina, Chile, Guatemala, Mexico, Peru, Uruguay and Venezuela—defined priority groups for the use of antivirals for prophylaxis, primarily targeting essential personnel, notably health personnel, and close contacts of pandemic cases, in the early stages of a pandemic.
The average completeness score for health services response was 46%. In general, it was unclear how the health sector would respond to a sudden increase in individuals seeking health care over a prolonged period of time. For instance, a triage system was only considered in five plans. Mexico and Chile scored the highest in the above theme, both with 82%. Mexico plans to set up hospitals and CAA (centres for attention and isolation) to manage the increased number of individuals seeking health care in the event of a pandemic. In terms of organization of care, referral hospitals have been identified in most countries, while a majority of strategies focus on increasing self-assessment and self-care for influenza and preparing a response at community level. Five countries—Argentina, Chile, Costa Rica, Mexico and Uruguay—indicate that their response would involve the private health sector.
Guidelines for the control of infection in health care settings were present in 11 plans, and 13 had planned for the provision of protective equipment for health care workers. Sources of additional health care workers were identified in five plans. Of note, Costa Rica developed a detailed operational guideline for health care personnel on how to use personal protective equipment, and Peru had a central stockpile of 10 000 units of personal protective equipment.
Little attention was paid to the preparedness efforts of essential services outside the health care sector. Only six plans showed some evidence that continuity of essential services would be addressed during the pandemic. Only nine plans identified an agency in charge of the national response.
Communication strategies are relatively well elaborated by the majority of countries, with an average completeness score of 59%. These strategies target three main audiences: government officials, health care professionals and the general public.
We also assessed plans’ operational capacity. The average completeness score was 31%. The availability of regional or local plans or instructions for regional or local authorities were, in general, poorly developed, with only seven plans mentioning the presence of detailed instructions to local authorities. Peru and Venezuela referred to regional plans for pandemic preparedness, and Chile, Uruguay, Mexico, Bolivia and El Salvador reported that detailed instructions to the regions had been issued.
Most plans did not mention whether simulations had been carried out in the country; this despite widespread acknowledgement of the necessity of conducting simulations to test preparedness. References to simulations in six countries were found in their pandemic influenza websites or from representatives of Ministries of Health. Simulations have been conducted to test the national plan (Argentina) or the response capacity of the health sector (Chile). Mexico carried out a simulation ‘Escudo centinela’ in February 2007 in several Mexican cities. In El Salvador, a local simulation was conducted in February 2007 and the country was preparing to hold a pandemic exercise at the airport in early 2008. Of note, Colombia and Uruguay made reference to exercises carried out in conjunction with delegations from PAHO (Uruguay Ministry of Health and Ministry of Agriculture 2007).
The training and education of health care workers was mentioned in six plans. Training is anticipated to be carried out through protocols or awareness and capacity building campaigns designed for this specific group.
Specific containment measures such as pre-purchase agreements for the purchase of pandemic vaccine and the stockpiling of antivirals were poorly covered overall. Three plans reported having a stockpile of antiviral medication: Argentina and Mexico each had a national stockpile as part of their rapid response strategy, while the Brazilian dedicated website for pandemic influenza preparedness mentioned that the country had secured an initial stockpile to cover 5% of the population (WHO 2006a).
Discussion
This study is, to our knowledge, the first analysis of national strategic pandemic preparedness plans in the Latin America region. It adds to a body of research we have conducted in Europe (Mounier-Jack and Coker 2006; Mounier-Jack et al. 2007), Asia (Coker and Mounier-Jack 2006) and Africa (Ortu et al. 2008). Previous analyses have shown that planning for an influenza pandemic requires continued efforts to harness and expand existing resources and to test and enhance plans. Latin America includes a variety of lower-middle-income and upper-middle-income countries with wide variation in social and political conditions, within which the different preparedness plans have been developed. Between November 2005 and November 2007, most countries published national strategic plans, and many countries and international agencies (such as PAHO) have made considerable efforts to support planning through regional workshops.
Our study demonstrates that Latin American national plans have a number of strengths. Resources have been invested in enhancing surveillance systems for influenza and developing communication strategies directed to the general public and health care personnel. Yet, strategic differences between countries exist, notably in the level of preparation for outbreak early containment; and national strategy on border control measures. This highlights the need to promote exchanges between countries and to improve consistency in pandemic response planning.
Our analysis also shows varying degrees of preparedness amongst countries. Plans highlight that in low-resource settings, external funding is needed to ensure that sustainable levels of preparedness can be achieved. One challenging issue will be how pandemic influenza preparedness can be harnessed to generic preparedness for other public health crises, thus avoiding duplication and incoherence in planning.
The ability of different health systems to respond to emergencies varies considerably, especially in low-income settings where infrastructure is fragile, resources limited and current capacity insufficient. However, the region needs to ensure that early detection and optimal response to an epidemic are planned and can be delivered. As part of this strengthening, in 2007 PAHO supported country members in developing and training rapid response teams for the eventuality of an influenza pandemic (PAHO-WHO 2007a).
Our survey shows that preparedness levels for both vaccination and antiviral drugs are poor. Access to pandemic vaccine is expressed as a concern in plans. Currently only Brazil has production capacity for influenza vaccines, with the Instituto Butantan in Sao Paulo able to produce approximately 20 millions trivalent doses/year (WHO 2006b). Both Mexico and Brazil were granted new funds from the WHO's influenza vaccine technology transfer programme (part of the Global Action Plan), in August and May 2007 respectively, to upgrade their technology to produce influenza vaccines, resulting in increased regional vaccine production capacity (WHO 2007).
While 10 plans mentioned cooperation and collaboration with neighbouring countries, the plans did not demonstrate clear operational cooperation in areas such as border control management, surveillance and early containment mechanisms. Only Brazil's plan has identified specific resources for border management, including the training of border personnel and the provision of medical supplies, outlining the need for interoperability with neighbouring countries’ plans. Latin American countries surveyed demonstrated limited planning of essential services outside the health sector, in line with what has been observed elsewhere (Coker and Mounier-Jack 2006; UN System Influenza Coordinator and World Bank 2007; Ortu et al. 2008). Such gaps would severely impact the regional resilience to a pandemic. In addition, there are specific concerns regarding the maintenance of the global supply chain during a pandemic (Luke and Rodrigue 2008), on which Latin American countries have a strong bearing, with many workers originating from this region and the Panama Canal being critical to supply chains. Greater regional and sub-regional cooperation may be needed to strengthen coordination of strategies between neighbouring countries and to ensure that policies are coherent.
Our assessment of pandemic preparedness of the Latin American region is consistent with previous evaluations carried out in other regions such as Africa (Ortu et al. 2008), Europe (Mounier-Jack and Coker 2006; Mounier-Jack et al. 2007) and Asia Pacific (Coker and Mounier-Jack 2006). Even if comparison among regions is difficult due to the disparity of countries in each of them, similar strengths and gaps may be highlighted. For instance, all regions boast a strong focus on communication and awareness-raising, whereas most provide limited operational guidance to preparedness, notably in relation to essential services. We also observe disparities in the preparedness of affluent nations and lower-income nations. In plans of resource-poor countries of Latin America, Africa and Asia, surveillance of both animal and human systems has received most attention in recent years, and operational response, notably of the health system, remains often developmental in nature.
There were a number of limitations to our study. The fluidity of the environment means that plans are being drafted and constantly modified. Our analysis offers only a snapshot in time. Another limitation concerns the difference between evaluating country plans and determining countries’ preparedness for an influenza pandemic. The completeness of national preparedness plans might be an important indicator of a country's preparedness, but plans are only one element. Finally, given the nature of plans, and the variations in language and format, any determination of criterion inclusion is, by necessity, somewhat subjective.
Our analysis of countries’ preparedness plans describes, therefore, a partial but important assessment of preparedness. Plans reflect not only strategic and tactical policy choices that are made by governments, but also their ability to involve and coordinate a broad range of relevant parties, which may be an important element in the success of the operational response.
Although the American continent has not had, to date, any cases of highly pathogenic avian influenza (H5N1) either in the avian or human populations, growing global concern has led most Latin American countries to develop strategic plans to respond to an influenza pandemic. Our analysis shows that gaps exist, however, including in the organization of health care services’ response, planning and maintenance of essential services, and the provision of containment measures such as stockpiling of necessary medical goods including vaccines and antiviral medications. In addition, some inconsistencies and variation that may be potentially important exist between country plans—issues that could result in confusion in the event of a pandemic. Furthermore, as is a feature of many strategic plans elsewhere in the world, the operability of strategic plans is a challenge across the region. Further emphasis of preparedness in Latin America should be placed on strengthening the operability of strategic plans.
Funding
This research was undertaken through an unrestricted educational grant from Hoffmann-La Roche.
Role of the funding source
The sponsors of the study had no role in study design, data collection, data analysis, data interpretation, or writing the report. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Acknowledgements
We thank the experts and representatives of ministries who offered their insights and sourced public documents.
References
- Bell DM. Non-pharmaceutical interventions for pandemic influenza, national and community measures. Emerging Infectious Diseases. 2006;12:88–94. doi: 10.3201/eid1201.051371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- CIA. The World Factbook: Field listing – GDP – per capita (PPP) 2007. Central Intelligence Agency; 2007. [Google Scholar]
- Coker R, Mounier-Jack S. Pandemic influenza preparedness in the Asia-Pacific region. The Lancet. 2006;368:886–9. doi: 10.1016/S0140-6736(06)69209-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luke TC, Rodrigue JP. Protecting public health and global freight transportation systems during an influenza pandemic. American Journal of Disaster Medicine. 2008;3:99–107. [PubMed] [Google Scholar]
- Mounier-Jack S, Coker RJ. How prepared is Europe for pandemic influenza? Analysis of national plans. The Lancet. 2006;367:1405–11. doi: 10.1016/S0140-6736(06)68511-5. [DOI] [PubMed] [Google Scholar]
- Mounier-Jack S, Jas R, Coker R. Progress and shortcomings in European national strategic plans for pandemic influenza. Bulletin of the World Health Organization. 2007;85:923–9. doi: 10.2471/BLT.06.039834. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ortu G, Mounier-Jack S, Coker R. Pandemic influenza preparedness in Africa is a profound challenge for an already distressed region: analysis of national preparedness plans. Health Policy and Planning. 2008;23:161–9. doi: 10.1093/heapol/czn004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- PAHO-WHO. Avian flu and pandemic influenza: Progress report. July 2007. 27th Pan American Sanitary Conference, 59th Session of the Regional Committee; 1–5 October 2007; Washington DC, USA. 2007. [accessed August 2007]. Online at: http://www.ops-oms.org/English/GOV/CSP/csp27-08-e.pdf. [Google Scholar]
- PAHO-WHO. [accessed January 2008];Health situation in the Americas: Basic indicators 2007. 2007 Online at: http://www.paho.org/english/dd/ais/coredata.htm.
- UN System Influenza Coordinator and World Bank. Third global progress report, December 2007. New York and Washington, DC: UNSIC and World Bank; 2007. Responses to avian influenza and state of pandemic readiness. [Google Scholar]
- Uruguay Ministry of Health and Ministry of Agriculture. [accessed August 2007];Plan nacional integrado ante pandemia de influenza, Uruguay 2007. 2007 Online at: http://www.bvsops.org.uy/pdf/influenza.pdf.
- WHO. [accessed August 2007];Checklist for influenza pandemic preparedness planning. WHO/CDS/CSR/GIP/2005.4. 2005 Online at: http://www.who.int/csr/resources/publications/influenza/WHO_CDS_CSR_GIP_2005_4/en/index.html.
- WHO. [accessed July 2007];Global influenza preparedness plan. The role of WHO and recommendations for national measures before and during pandemics. WHO/CDS/CSR/GIP/2005.5. 2005 Online at: http://www.who.int/csr/resources/publications/influenza/WHO_CDS_CSR_GIP_2005_5/en/index.html.
- WHO. [accessed July 2007];Cumulative number of confirmed human cases of avian influenza A/(H5N1) reported to WHO. 2006 Online at: http://www.who.int/csr/disease/avian_influenza/country/cases_table_2006_04_12/en/index.html.
- WHO. Global pandemic influenza action plan to increase vaccine supply. Presentation at the Global Vaccine Research Forum 2006. 2006 Online at: http://www.who.int/vaccine_research/about/gvrf/Costa_presentation.pdf.
- WHO. Meeting with international partners on influenza vaccine technology transfer to developing country vaccine manufacturers. 29–30 October 2007, Bangkok, Thailand. 2007 Online at: http://www.who.int/vaccine_research/diseases/influenza/Report_IVR%20Meeting_BKK%2029-30%20Oct%202007_Final.pdf.
- WHO. [accessed 20 May 2008];Cumulative number of confirmed human cases of avian influenza A/(H5N1) reported to WHO. 2008 Online at: http://www.who.int/csr/disease/avian_influenza/country/cases_table_2008_04_30/en/index.html.