

Abstract
Long bone fractures are rarely seen in newborns. Though the femoral bone is more fragile, occasionally the humeral bone may fracture. Presently described is a rare case of a humeral fracture occurring at birth. A female infant born by vaginal delivery to a 35-year-old multipara woman at the 40th gestational week was hypotonic and in respiratory distress. Resuscitation was performed for 15 minutes. Bilateral Moro reflexes could not be elicited. Radiological evaluation revealed a left humeral diaphysis fracture. Humeral fractures are generally associated with the increase in cesarean deliveries; however, a newborn may also experience trauma during difficult labor and vaginal delivery. Pregnant women should be informed about the potential occurrence of long bone fractures, particularly as a result of necessary obstetric maneuvers performed during a breech delivery. In addition, it should be emphasized that cesarean delivery does not completely eliminate the risk of trauma to the infant.
Keywords: Birth trauma, humerus, newborn
Ahumeral diaphysis fracture in a newborn after a vaginal delivery is rare. Birth traumas, including bone fractures, have been reported in 6.7 to 14 per 1000 live births. Fractures in newborns typically occur due to a narrow maternal pelvis or a breech delivery. Rapid contractions or maneuvers performed during a breech presentation, may lead to fetal injuries. Similarly, an exceptionally large infant, prolonged labor, and fetal head presentation have been reported to possibly be related to fractures. These are the most frequently observed independent risk factors for long bone fractures in both vaginal and cesarean deliveries.[1-3]
Presently described is a case of humeral diaphysis fracture detected in a neonate born by vaginal delivery to a multigravida mother.
Case Report
A female infant was born following a normal, spontaneous vaginal delivery at the 40th gestational week to a 35-year-old gravida 6 mother as her fifth live birth. Her previous pregnancies had been uneventful, and all of the births were spontaneous vaginal deliveries. As a result of a decline in the peak fetal heart rate during labor, the obstetrician applied forced leftward traction on the baby to assist the birth. The infant’s birth weight was 5080 g, length was 46 cm, and head circumference was 37 cm. There was no spontaneous respiration, and the peak heart rate was <100 bpm. The intensive care unit team performed resuscitation for 15 minutes, the infant was intubated, and 2 doses of 0.01mg/kg adrenaline were infused through an umbilical catheter in the delivery room. The umbilical blood gas measurements were pH: 6.9, PCO2: 64 mmHg, bicarbonate: 16 mmol/L, and base excess: -18 mmol/L. Physical examination revealed that the infant was hypotonic and in respiratory distress. Bilateral Moro reflexes could not be elicited. An X-ray indicated a left humeral diaphysis fracture (Fig. 1). Reduction and immobilization of the arm was performed by an orthopedist. Two weeks later, a control X-ray of the left arm revealed complete recovery without any deformity (Fig. 2).
Figure 1.
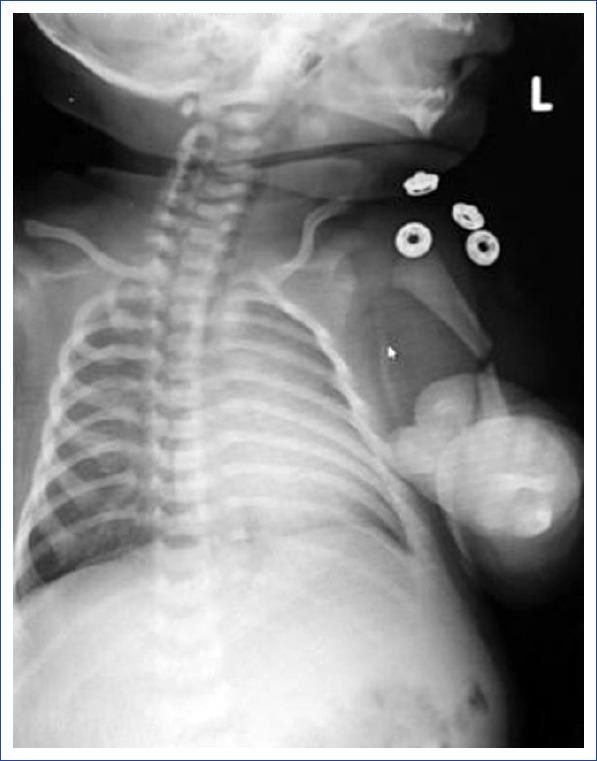
Left humeral diaphysis fracture.
Figure 2.

Left humeral diaphysis fracture.
Discussion
Long bone fractures are frequently associated with maneuvers performed during vaginal deliveries of babies with a breech presentation. However, emergency cesarean deliveries have a greater risk for long bone fractures compared with vaginal deliveries. Premature birth, malpresentation, malposition, and multiple pregnancy may predispose to long bone fracture.[4] Long bone fractures are also associated with neonatal osteoporosis.[5] In addition, pathological fractures may be related to osteogenesis imperfecta, rickets, or child abuse.[6] The incidence of long bone injuries has been reported as 0.23 to 4 per 1000 live births.[4, 7, 8] The incidence of humeral fracture has been reported as 0.05 per 1000 live births.[5, 7, 8] Spontaneous delivery of our case included head presentation; however, obstetric maneuvers were required during labor as a result of a decrease in the fetal heart rate. Even with such maneuvers, the life of the baby cannot always be saved.[5] The results of 1 case series indicated that more fractures occurred during cesarean delivery, which was thought to be safer than vaginal delivery. The authors concluded that there is a greater risk of long bone fracture in emergency cesarean delivery.[7]
Diagnosis of humeral diaphysis fracture can easily be made with an X-ray. The greater difficulty is to diagnose epiphyseal dislocation.[9] Diagnosis may require ultrasound, magnetic resonance imaging, or even arthrography.[7] In this case, diagnosis was made with X-ray imaging.
In emergency cesarean deliveries, and when forced maneuvers are required in either vaginal or cesarean deliveries, fetal injuries, including long bone fractures, may occur. Fortunately, humeral fractures frequently heal without any deformity after simple immobilization.[5] In our case, the humeral fracture healed successfully after application of an orthopedic brace for 2 weeks.
In conclusion, long bone fractures are among the most unwanted complications of birth. Cesarean delivery does not eliminate the possibility of long bone fracture. Before the birth, families should be informed that necessary obstetric maneuvers may result in a bone fracture. Finally, examination and detection of trauma and injuries in newborns at an early stage after birth is very important in order to prevent later unwanted outcomes.
Disclosures
Informed consent: Written informed consent was obtained from the patient for the publication of the case report and the accompanying images.
Peer-review: Externally peer-reviewed.
Conflict of Interest: None declared.
Authorship contributions: Concept – S.H.; Design – S.H.; Supervision – E.C.; Materials – K.Y.; Data collection &/or processing – S.H., K.Y.; Analysis and/or interpretation – S.H., E.C.; Literature search – K.Y.; Writing – S.H., K.Y.; Critical review – E.C.
References
- 1.Bulbul A, Sozeri S, Selalmaz M, Uslu S, Nuhoglu A. The incidence and associated of the birth trauma in the newborns. risk factors. J Turgut Ozal Med Cent. 2013;20:327–30. [Google Scholar]
- 2.Awari BH, Al-Habdan I, Sadat-Ali M, Al-Mulhim A. Birth associated trauma. Saudi Med J. 2003;24:672–4. [PubMed] [Google Scholar]
- 3.Barrientos G, Cervera P, Navascués J, Sánchez R, Romero R, Pérez-Sheriff V, et al. Obstetric trauma. A current problem?Cir Pediatr. 2000;13:150–2. [PubMed] [Google Scholar]
- 4.Kaya B, Daglar K, Kirbas A, Tüten A. Humerus Diaphysis Fracture in a Newborn during Vaginal Breech Delivery. Case Rep Obstet Gynecol. 2015;2015:489108. doi: 10.1155/2015/489108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sherr-Lurie N, Bialik GM, Ganel A, Schindler A, Givon U. Fractures of the humerus in the neonatal period. Isr Med Assoc J. 2011;13:363–5. [PubMed] [Google Scholar]
- 6.Dias E. Bilateral humerus fracture following birth trauma. J Clin Neonatol. 2012;1:44–5. doi: 10.4103/2249-4847.92230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Basha A, Amarin Z, Abu-Hassan F. Birth-associated long-bone fractures. Int J Gynaecol Obstet. 2013;123:127–30. doi: 10.1016/j.ijgo.2013.05.013. [DOI] [PubMed] [Google Scholar]
- 8.Al-Habdan I. Birth-related fractures of long bones. Indian J Pediatr. 2003;70:959–60. doi: 10.1007/BF02723819. [DOI] [PubMed] [Google Scholar]
- 9.Husain SN, King EC, Young JL, Sarwark JF. Remodeling of birth fractures of the humeral diaphysis. J Pediatr Orthop. 2008;28:10–3. doi: 10.1097/BPO.0b013e3181558c67. [DOI] [PubMed] [Google Scholar]