

Abstract
This analysis extrapolates information from prior studies and experiences to bring PM&R perspective and intervention to the multidisciplinary treatment of COVID-19. The purpose of pulmonary rehabilitation in COVID-19 patients is to improve symptoms of dyspnea, relieve anxiety, reduce complications, minimize disability, preserve function and improve quality of life. Pulmonary rehabilitation during the acute management of COVID-19 should be considered when possible and safe and may include nutrition, airway, posture, clearance technique, oxygen supplementation, breathing exercises, stretching, manual therapy, and physical activity. Given the possibility of long-term disability, outpatient post-hospitalization pulmonary rehabilitation may be considered in all patients hospitalized with COVID-19.
Keywords: Pulmonary Rehabilitation, Inpatient Rehabilitation, Multidisciplinary/Interdisciplinary Rehabilitation, COVID-19
Pulmonary Rehabilitation is a core aspect of medical rehabilitation. The fundamentals tools and interventions of Pulmonary Rehabilitation are extremely important traditional interventions that have an extremely important new role and application in the treatment of COVID-19.
Introduction
This review is written to empower PM&R physicians as many of us are called to assist our colleagues in the fight against COVID-19. The PM&R perspective and Pulmonary Rehabilitation lend unique tools to our medical teams as we work to combat a disease currently without definitive treatment other than supportive care.
These recommendations are extrapolated from studies and experience in patients with COVID-19, pulmonary rehabilitation patients without COVID-19, and from prior SARS/MERS epidemic.1,2 Flexibility and synthesis of heterogeneous and multidisciplinary data and experience across specialties is necessary to address the new and unique rehabilitation challenges that arise from this pandemic. This review serves as a guide and launching point for the ongoing management of functional and comorbid rehabilitative issues related to COVID-19.
Pulmonary rehabilitation’s definition, as adapted from the American Thoracic Society/European Respiratory Society,3 is comprehensive intervention based on a thorough patient assessment followed by patient tailored therapies that include, but are not limited to, exercise training, education, and behavior change, designed to improve the physical condition of people with respiratory disease.
The purpose of pulmonary rehabilitation in COVID-19 patients is to improve symptoms of dyspnea, relieve anxiety, reduce complications, minimize disability, preserve function and improve quality of life.4 Pulmonary rehabilitation should be tailored to each individual patient. In the event that a PM&R physician or a rehabilitation expert is not available, proposed interventions have been listed.
A PubMed search was conducted using a systematic review filter to identify articles that were published since January 2003 to include the SARS outbreak. Reviews were selected from a systematic search for literature containing information related to COVID-19, MERS, and SARS. Five board certified PM&R physicians scoured additional sources including professional blogs and membership forums.
General Principles
Given the shortage of personal protective equipment and high risk of nosocomial spread, rehabilitation should occur through telemedicine with minimal contact. Self-supervised rehabilitation should be initiated using telemedicine.2,8 Prior studies on the use telehealth and home pulmonary rehabilitation programs showed equal outcomes compared with center based programs.5 If direct supervision is needed, full PPE including gloves, mask, and isolation gown should be used in all person-to person interaction. Furthermore, a face shield and or goggles are also recommended if there is risk of infected aerosolized droplets. Current non-invasive ventilatory techniques have a high risk of aerosolization of the SARS-CoV2 virus.10,11 Nosocomial spread amongst healthcare workers is extremely high (approximately 35% of exposed healthcare workers develop disease)9 and the disease has a more severe clinical course in healthcare workers.
Outpatient mild disease management
Mild disease is defined as mild symptoms without pneumonia manifestations on imaging.6 Rehabilitation for mild disease can be managed in the outpatient setting using telemedicine.2 In mild disease, pulmonary rehabilitation may be considered and include education, airway clearance techniques, physical exercise, breathing exercises, activity guidance, and anxiety management.4 Details are summated in Table 1.
Table 1.
Proposed Content for Mild Disease
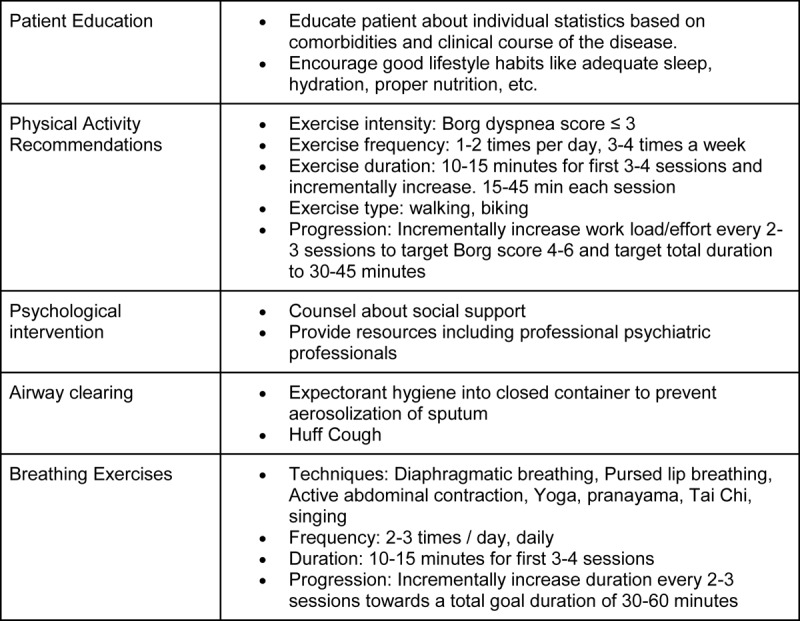
In particular, adequate handling and disposal of corporal fluid should be practiced in home based pulmonary rehabilitation. Patients should be instructed to cover nose and mouth with tissue when coughing or sneezing with the immediately disposal of the tissue. Expectorant hygiene into a closed container should be reinforced to prevent aerosolization of sputum. Hand hygiene with hand washing after having contact with respiratory secretions and contaminated objects/materials should be emphasized.
Patients should be educated on the clinical course of COVID-19 and with individualization based on patient comorbidities.7 The patient, including asymptomatic family members, may be counseled to wear masks;3 Sars-CoV2 has a high transmission rate and a long asymptomatic prodromal phase with a range of 2-14 days and a mean of 3-7 days.8 Mathematical modeling shows that mask use with 50% compliance during a viral outbreak can curb the spread with a 50% decrease in prevalence and 20% decrease in cumulative incidence.3
Breathing exercises may be employed at this stage (Table 1). Diaphragmatic breathing involves coaching the patient to predominantly engage the diaphragm while minimizing the action of accessory muscles.9 Nasal inspiration should be encouraged to facilitate recruitment of the diaphragm and enhance humidification10 Active abdominal muscle contraction should be employed at the end of expiration to increase abdominal pressure and push diaphragm up to a more favorable length-tension.11
Yoga and in particular Viniyoga coordinates breathing with arm lifts or body positioning during the inspiratory or expiratory phase. Pranayama, Tai Chi12, and singing also employ timed breathing techniques.
Acute Inpatient Management
Moderate to severe disease is defined as symptomatic patients with or approaching respiratory distress with respiratory rate> 30 times/minutes, oxygen saturation at rest <93%, or PaO2/FiO2<300 mmHg. These patients require hospitalization and monitoring.6
Pulmonary rehabilitation during acute management of COVID-19 should be considered when possible (Figure 1) and is summarized in Table 2. In acute exacerbation of chronic lung conditions, pulmonary rehabilitation results in moderate to large effects on health-related quality of life and exercise capacity.13 Overall, pulmonary rehab in acute illness appears to be safe with no increased mortality13,14 and can be safely implemented for COVID-19.15
Figure 1.
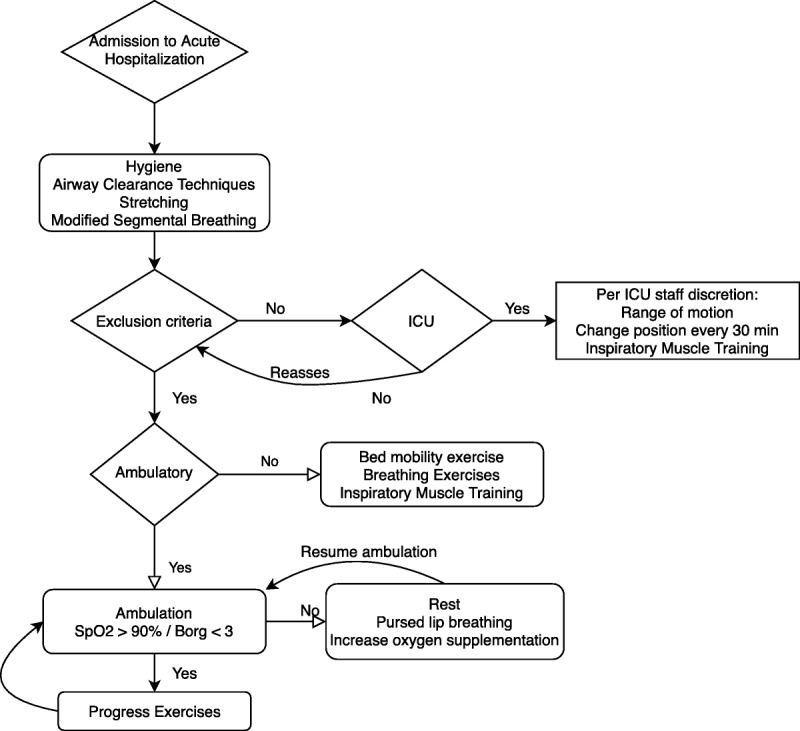
Suggested flowchart for rehabilitation interventions during acute hospitalization
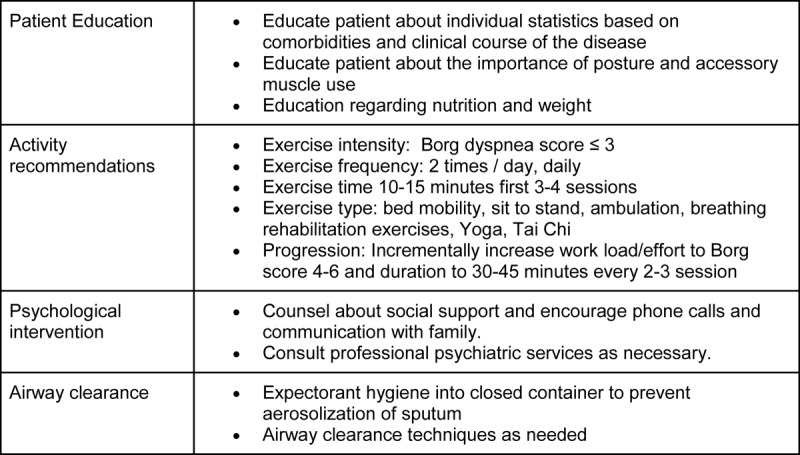
Table 2.
Proposed Acute Management
Early pulmonary rehabilitation and mobilization in the ICU may be approached with cautious consideration and should not occur at the expense of healthcare worker safety.16 SARS-CoV2 aerosolizes during procedures and in ICU environments.17 To preserve personal protective equipment and given the questionable outcome of early mobilization in the ICU,5 early mobilization by additional rehabilitation staff is not recommended in the ICU and may be a consideration by dedicated ICU staff.2 Respiratory muscle weakness from diaphragm proteolysis may occur after prolonged mechanical ventilation18 and inspiratory muscle training may occur during weaning trials with a skilled respiratory therapist.18,19
Initiation of pulmonary rehabilitation in the inpatient setting should occur with safety criteria in mind. Approximately 3% to 5% of otherwise healthy patients can progress within 7 to 14 days of infection to severe or even critical conditions.7 Therefore, initial intensity of exercise should be graded and approached with caution and monitoring. Exclusion criteria include the following: 1. body temperature > 38.0 °C; 2. initial diagnosis time or symptom onset ≤ 3 days; 3. initial onset of dyspnea ≤ 3 days; 4. chest image progression within 24 to 48 hours > 50%; 5. SpO2 ≤ 90%; 6. blood pressure <90/60 mmHg or > 180/90 mmHg;15 7. respiratory rate > 40 times / min; 8. heart rate <40 beats / min or > 120 beat / min; 9. new onset of arrhythmia and myocardial ischemia; 10. altered level of consciousness.
Physical exercise is a core component of pulmonary rehabilitation and may start with bed mobility in the very deconditioned patient to walking in the ambulatory patient.3 Rehabilitation intervention should target SpO2 > 90% with titration of supplemental oxygen to maintain target saturation.3,4,7 Pause in activity should occur if SpO2 drops below target or Borg scale dyspnea score > 3 with consideration of breathing technique like pursed lip breathing with resumption of exercise intervention once SpO2 reaches target.7,20
Pursed lips breathing is performed by a nasal inspiration followed by expiratory blowing against pursed lips to decrease airway collapse, reduce respiratory rate and dynamic hyperinflation during exercise training with the aim of an overall increase endurance.20 Oxygen supplementation has also been successfully used during exercise training to help unload the respiratory muscles.2,7
Pulmonary rehabilitation or breathing exercises should be stopped if SpO2 does not recover and the patient is unable to maintain Borg scale dyspnea score <4, with rest and oxygen supplementation. Rehabilitation exercises should also stop for chest pain, palpations, and dizziness. The Borg Scale is a validated and easy to use tool for patients to self-monitor respiratory effort with a close correlation between the magnitude of respiratory effort and the intensity of dyspnea.21
Active cycle of breathing techniques utilizes combinations and cycles of airway clearance techniques to ventilate obstructed lung segements.22 No specific technique has found to be superior to over others and should be based on training and expertise.23 Autogenic drainage is a common technique that utilizes a combination of the maneuvers to mobilize and centralize secretions with short breaths to collect secretions in peripheral airway, followed by normal breaths to collect secretions into the intermediate airway, and deep breaths and huff cough to expel secretions.24
Application of airway clearance techniques can significantly reduce the need for ventilatory support, days of mechanical ventilation and hospitalization.10 Airway clearance techniques aim to help airway clearance by mobilizing mucus in a cephalad direction from the peripheral to upper airway, promoting the recruitment of lung volume, and eliminating mucus by cough or forced expectoration.6 Physical exercise is a cornerstone of pulmonary rehabilitation and has been shown to facilitate airway clearance.8 In acute phases, early mobilization and physical exercise are preferred and more effective than mucus clearance techniques, and mucus clearance techniques should not be used alone or take precedence over physical movement.9
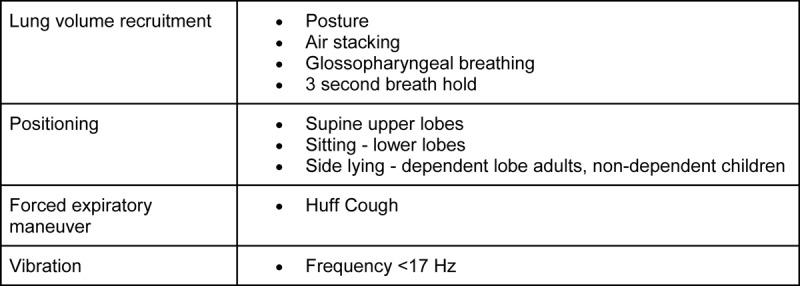
Lung volume recruitment maneuvers include air stacking and glottis holding. Air stacking involves delivery of air via Ambu bag25. Glossopharyngeal breathing is a form of positive pressure breathing technique that can be used to assist failing respiratory muscles and increase tidal volumes. It involves successive inhale of boluses of air and pushing them into the lungs.26 The 3-second breath hold is a method of ventilating obstructed lung segments. A pause for 3 seconds allows for Pendelluft flow where air moves from unobstructed regions to the obstructed regions of the lung.27
Forced expiration maneuvers like the huff cough can be used to propel secretions. A huff cough is performed with an open glottis where equal pressure point dynamic compression of the airways creates an increase in the linear velocity of the expiratory airflow and propels secretions. Initiating a forced expiration at a low lung volume shifts the equal pressure point to the periphery and small airways. A forced expiration from a high lung volume will move the equal pressure point centrally towards the large central airway.28
Posture plays an important role in respiratory function12 and patients can be encouraged to engage in erect head and neck positioning during respiratory treatment and at all times when possible. External vibration if available may be applied with oscillation frequencies less than 17 Hz to improve mucociliary clearance.24
Positioning is effective, simple, and easy to accomplish.29 Positioning may be preferable over other techniques like postural drainage given the pathophysiology of COVID-19 and the observed V/Q mismatch.29,30 31 Sitting and standing are the preferred positions in non-critically ill patients to maximize lung function including FVC, increase lung compliance and elastic recoil, and shift mediastinal structures, and provide mechanical advantage in forced expiration.13,14,32
Targeted positioning may be used to enhance ventilation, perfusion, oxygenation and mobilization of secretions in specific lung regions of consolidations through gravity.21 Perfusion is greater to the dependent lung segments in all positions.33 Preferential ventilation changes based on position. Two minutes in each position while engaging in breathing exercises may be sufficient to ventilate/perfuse targeted lung segments.33
Anecdotal evidence in hospitals suggesting prone positioning during acute care of COVID-19 patient has been beneficial. If possible, we recommend time in all positions including side-lying, upright, supine, and prone and guided by imaging findings when possible. Targeted positions may be determined by the location of consolidations seen on imaging or found on examination.7
In the upright position, ventilation preferentially occurs in the mid and lower lobes with perfusion greatest in the lower lobes.34 Patients may rest in a supine position occasionally to aid in DLCO. DLCO increases in the supine position in healthy subjects.35 Supine position also preferentially ventilates the upper lobes.34
In adults side-lying position preferentially ventilates the dependent lung by maximizing the length-tension ratio in the dependent hemi-diaphragm and negative pleural pressure.36 In young children <12-years-old side-lying position preferentially ventilates the nondependent lung and closing of airway in depend regions. Side-lying may be a good position during administration of inhaled drug with improved deposition by 13% to the dependent upper lobe.33
Prone positioning for 2 minutes duration may aid in ventilation to dorsal lung through reduction in lung compression by the heart in the semi-prone position due to ventral displacement of the heart24 with increases in end-expiratory transpulmonary pressure and expiratory reserve volume,25 more homogenous lung inflation from dorsal to ventral and improvement in oxygenation.26 Prone positioning has been used in the ICU to improve gas exchange in ARDS and improve Pa/FiO2 in patients on mechanical ventilation and reduces cardiovascular comorbidities.37
Patients may be encouraged to engage in routine stretching three times a day. Stretching has been shown to increase compliance by as much as 50mL. Stretches should include neck, upper chest, pectoralis major, lateral chest stretches38 and flexion and extension to mobilize the facet joints. The dorsal chest wall has been shown to be less compliant in patients with ARDS.39
Osteopathic manipulation, if appropriate, may be helpful and should address autonomics, lymph drainage, and rib cage mobility.30 The patient may also engage in modified segmental breathing where the patient applies pressure to their own thoracic cage to resist respiratory excursion in one area of the thoracic cavity and to facilitate the expansion of adjacent regions of the thoracic cavity that may have decreased ventilation and mobility.40
Education regarding proper nutrition is particularly important in COVID-19 as studies from Western countries are showing that obesity to be a significant risk factor for severity of disease with at least ⅔ of ICU patients having overweight BMI.41 In obesity, lung function is also impaired.42
The same strategies may be applied to patients recovering from ICU level care. In these patients, a focus on breathing exercises (Table 3) and bed mobility may be the initial intervention given the deconditioning that occurs in ICU. Bed mobility exercises include ankle pumps, sliding legs into flexion/extension, over-head arm stretches, sit-to-stand at bedside. In addition, respiratory muscle weakness from diaphragm proteolysis may be suspected in those patients with prolonged mechanical ventilation.18 Inspiratory and expiratory muscle training can be implemented in these patients starting with incentive spirometry and progressing to inspiratory muscle training devices if available.18,19
Table 3.
Airway Clearance Techniques
Post-Acute Rehabilitation
Appropriateness for inpatient acute rehabilitation should be individualized to the patient and the facility with ongoing AAPM&R guidance.2,43 Outpatient post-hospitalization pulmonary rehabilitation may be considered in all patients hospitalized with COVID-19.44 Patient selection criteria will have to be developed in the coming months after the pandemic. Quadriceps weakness and impaired exercise capacity may be predictors of good candidates for pulmonary rehabilitation.45 Occupational and physical therapy may also be considered in those with residual functional deficits associated with prolonged hospitalization.
Routine monitoring with chest x-ray and PFT may be considered in the outpatient setting particularly within 6 months of infection and for severe and critical patients. Pulmonary fibrosis may occur in COVID-19. In SARS-CoV in 2003, pulmonary fibrosis was seen to develop in 45% of patients (diagnosed by X-ray and CT scan) 1 month after infection, 30-36% 3-6 months after infection,46 and 28% 1 year after infection.46 After SARS-CoV infection, severity of fibrosis and disability correlated with the severity and duration of illness.47,48 Improvement in lung function in SARS-CoV patients plateaued at 6 months with continued disability particularly in DLCO 2 years after infection.49
Pulmonary rehabilitation in the post-acute period may work towards improvement in exercise capacity. In patients with interstitial lung disease, exertional desaturation is a key feature and is often more severe than that seen in other pulmonary conditions.50 Interstitial lung disease is associated with reduced ventilatory capacity and tissue oxygenation with premature onset of metabolic acidosis with dyspnea and lower limb discomfort/fatigue during submaximal exercise.22,51 Pulmonary hypertension also be present and decrease exercise capacity.52 Supplemental oxygen may be needed to facilitate oxygenation of tissue and enhance exercise capacity with target SpO2 from 85 to 90%.44
Conclusion
PM&R physicians and rehabilitation may play a pivotal role in restoring function and limiting disability this pandemic. PM&R interventions and Pulmonary Rehabilitation give us additional tools in the fight against COVID-19 and may include nutrition, airway, posture, clearance technique, oxygen supplementation, breathing exercises, stretching, manual therapy, and physical activity. In the months to years following this pandemic, the burden of disease may be large and PM&R will play a crucial role in the rehabilitation of patients with disability in relation to COVID-19.
Footnotes
Author Disclosures: None
References:
- 1.Janssens J-P, Chappuis-Gisin É, Maragkoudakis C, et al. : [Pulmonary rehabilitation in respiratory disorders other than COPD : an individualized approach]. Rev Med Suisse. 2018;14:2054–2057. [PubMed] [Google Scholar]
- 2.Lim PA, Ng YS, Tay BK. Impact of a viral respiratory epidemic on the practice of medicine and rehabilitation: severe acute respiratory syndrome. Arch Phys Med Rehabil. 2004;85:1365–1370. doi: 10.1016/j.apmr.2004.01.022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Spruit MA, Singh SJ, Garvey C, et al. :. An Official American Thoracic Society/European Respiratory Society Statement: Key Concepts and Advances in Pulmonary Rehabilitation. Am J Respir Crit Care Med. 2013;188:e13–e64. doi: 10.1164/rccm.201309-1634ST [DOI] [PubMed] [Google Scholar]
- 4.Chinese Association of Rehabilitation Medicine, Respiratory rehabilitation committee of Chinese Association of Rehabilitation Medicine, Cardiopulmonary rehabilitation Group of Chinese Society of Physicai Medicine and Rehabilitation [Recommendations for respiratory rehabilitation of COVID-19 in adult]. Zhonghua Jie He He Hu Xi Za Zhi. 2020;43:E029. doi: 10.3760/cma.j.cn112147-20200228-00206 [DOI] [PubMed] [Google Scholar]
- 5.Alison JA, McKeough ZJ, Johnston K, et al. :. Australian and New Zealand Pulmonary Rehabilitation Guidelines. Respirology. 2017;22:800–819. doi: 10.1111/resp.13025 [DOI] [PubMed] [Google Scholar]
- 6.Lin L, Li TS. [Interpretation of “Guidelines for the Diagnosis and Treatment of Novel Coronavirus (2019-nCoV) Infection by the National Health Commission (Trial Version 5)”]. Zhonghua Yi Xue Za Zhi. 2020;100:E001. doi: 10.3760/cma.j.issn.0376-2491.2020.0001 [DOI] [PubMed] [Google Scholar]
- 7.Rodriguez-Morales AJ, Cardona-Ospina JA, Gutiérrez-Ocampo E, et al. :. Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel Med Infect Dis. March 2020:101623. doi: 10.1016/j.tmaid.2020.101623 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Guo Y-R, Cao Q-D, Hong Z-S, et al. :. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak – an update on the status. Military Med Res. 2020;7:11. doi: 10.1186/s40779-020-00240-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gosselink R. Breathing techniques in patients with chronic obstructive pulmonary disease (COPD). Chron Respir Dis. 2004;1:163–172. doi: 10.1191/1479972304cd020rs [DOI] [PubMed] [Google Scholar]
- 10.Elad D, Wolf M, Keck T. Air-conditioning in the human nasal cavity. Respir Physiol Neurobiol. 2008;163(1-3):121–127. doi: 10.1016/j.resp.2008.05.002 [DOI] [PubMed] [Google Scholar]
- 11.Casciari RJ, Fairshter RD, Harrison A, Morrison JT, Blackburn C, Wilson AF. Effects of breathing retraining in patients with chronic obstructive pulmonary disease. Chest. 1981;79:393–398. doi: 10.1378/chest.79.4.393 [DOI] [PubMed] [Google Scholar]
- 12.Ngai SPC, Jones AYM, Tam WWS. Tai Chi for chronic obstructive pulmonary disease (COPD). Cochrane Database Syst Rev. 2016;(6):CD009953. doi: 10.1002/14651858.CD009953.pub2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Jones SE, Barker RE, Nolan CM, Patel S, Maddocks M, Man WDC. Pulmonary rehabilitation in patients with an acute exacerbation of chronic obstructive pulmonary disease. J Thorac Dis. 2018;10(S12):S1390–S1399. doi: 10.21037/jtd.2018.03.18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Puhan MA, Gimeno-Santos E, Cates CJ, Troosters T. Pulmonary rehabilitation following exacerbations of chronic obstructive pulmonary disease. Cochrane Airways Group, ed. Cochrane Database of Systematic Reviews. December 2016. doi: 10.1002/14651858.CD005305.pub4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Yang F, Liu N, Hu JY, et al. : [Pulmonary rehabilitation guidelines in the principle of 4S for patients infected with 2019 novel coronavirus (2019-nCoV)]. Zhonghua Jie He He Hu Xi Za Zhi. 2020;43:180–182. doi: 10.3760/cma.j.issn.1001-0939.2020.03.007 [DOI] [PubMed] [Google Scholar]
- 16.Liu W, Mu X, Wang X, Zhang P, Zhao L, Li Q. Effects of comprehensive pulmonary rehabilitation therapy on pulmonary functions and blood gas indexes of patients with severe pneumonia. Exp Ther Med. July 2018. doi: 10.3892/etm.2018.6396 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Wax RS, Christian MD. Practical recommendations for critical care and anesthesiology teams caring for novel coronavirus (2019-nCoV) patients. Can J Anaesth. February 2020. doi: 10.1007/s12630-020-01591-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bissett B, Gosselink R, van Haren FMP. Respiratory Muscle Rehabilitation in Patients with Prolonged Mechanical Ventilation: A Targeted Approach. Crit Care. 2020;24:103. doi: 10.1186/s13054-020-2783-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Paiva DN, Assmann LB, Bordin DF, et al. :. Inspiratory muscle training with threshold or incentive spirometry: Which is the most effective? Revista Portuguesa de Pneumologia (English Edition). 2015;21:76–81. doi: 10.1016/j.rppnen.2014.05.005 [DOI] [PubMed] [Google Scholar]
- 20.Mayer AF, Karloh M, Dos Santos K, de Araujo CLP, Gulart AA. Effects of acute use of pursed-lips breathing during exercise in patients with COPD: a systematic review and meta-analysis. Physiotherapy. 2018;104:9–17. doi: 10.1016/j.physio.2017.08.007 [DOI] [PubMed] [Google Scholar]
- 21.Cullen DL, Rodak B. Clinical utility of measures of breathlessness. Respir Care. 2002;47:986–993. [PubMed] [Google Scholar]
- 22.McKoy NA, Saldanha IJ, Odelola OA, Robinson KA. Active cycle of breathing technique for cystic fibrosis. Cochrane Database Syst Rev. 2012;12:CD007862. doi: 10.1002/14651858.CD007862.pub3 [DOI] [PubMed] [Google Scholar]
- 23.Wilson LM, Morrison L, Robinson KA. Airway clearance techniques for cystic fibrosis: an overview of Cochrane systematic reviews. Cochrane Database Syst Rev. 2019;1:CD011231. doi: 10.1002/14651858.CD011231.pub2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.McCormack P, Burnham P, Southern KW. Autogenic drainage for airway clearance in cystic fibrosis. Cochrane Database Syst Rev. 2017;10:CD009595. doi: 10.1002/14651858.CD009595.pub2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kang SW, Bach JR. Maximum insufflation capacity: vital capacity and cough flows in neuromuscular disease. Am J Phys Med Rehabil. 2000;79:222–227. doi: 10.1097/00002060-200005000-00002 [DOI] [PubMed] [Google Scholar]
- 26.Maltais F. Glossopharyngeal breathing. Am J Respir Crit Care Med. 2011;184:381. doi: 10.1164/rccm.201012-2031IM [DOI] [PubMed] [Google Scholar]
- 27.Crawford AB, Cotton DJ, Paiva M, Engel LA. Effect of airway closure on ventilation distribution. J Appl Physiol. 1989;66:2511–2515. doi: 10.1152/jappl.1989.66.6.2511 [DOI] [PubMed] [Google Scholar]
- 28.McIlwaine M, Bradley J, Elborn JS, Moran F. Personalising airway clearance in chronic lung disease. Eur Respir Rev. 2017;26:160086. doi: 10.1183/16000617.0086-2016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Fink JB. Positioning versus postural drainage. Respir Care. 2002;47:769–777. [PubMed] [Google Scholar]
- 30.Tang X, Du R, Wang R, et al. :. Comparison of Hospitalized Patients with Acute Respiratory Distress Syndrome Caused by COVID-19 and H1N1. Chest. March 2020:S0012369220305584. doi: 10.1016/j.chest.2020.03.032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Gattinoni L, Coppola S, Cressoni M, Busana M, Chiumello D. Covid-19 Does Not Lead to a “Typical” Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med. March 2020. doi: 10.1164/rccm.202003-0817LE [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Manning F, Dean E, Ross J, Abboud RT. Effects of side lying on lung function in older individuals. Phys Ther. 1999;79:456–466. [PubMed] [Google Scholar]
- 33.Dentice RL, Elkins MR, Dwyer GM, Bye PTP. The use of an alternate side lying positioning strategy during inhalation therapy does not prolong nebulisation time in adults with Cystic Fibrosis: a randomised crossover trial. BMC Pulm Med. 2018;18:3. doi: 10.1186/s12890-017-0568-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Bailey DL, Farrow CE, Lau EM. V/Q SPECT-Normal Values for Lobar Function and Comparison With CT Volumes. Semin Nucl Med. 2019;49:58–61. doi: 10.1053/j.semnuclmed.2018.10.008 [DOI] [PubMed] [Google Scholar]
- 35.Katz S, Arish N, Rokach A, Zaltzman Y, Marcus E-L. The effect of body position on pulmonary function: a systematic review. BMC Pulm Med. 2018;18:159. doi: 10.1186/s12890-018-0723-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Bhuyan U, Peters AM, Gordon I, Davies H, Helms P. Effects of posture on the distribution of pulmonary ventilation and perfusion in children and adults. Thorax. 1989;44:480–484. doi: 10.1136/thx.44.6.480 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Guérin C, Reignier J, Richard J-C, et al. :. Prone Positioning in Severe Acute Respiratory Distress Syndrome. N Engl J Med. 2013;368:2159–2168. doi: 10.1056/NEJMoa1214103 [DOI] [PubMed] [Google Scholar]
- 38.Rattes C, Campos SL, Morais C, et al. :. Respiratory muscles stretching acutely increases expansion in hemiparetic chest wall. Respiratory Physiology & Neurobiology. 2018;254:16–22. doi: 10.1016/j.resp.2018.03.015 [DOI] [PubMed] [Google Scholar]
- 39.Pelosi P, D’Andrea L, Vitale G, Pesenti A, Gattinoni L. Vertical gradient of regional lung inflation in adult respiratory distress syndrome. Am J Respir Crit Care Med. 1994;149:8–13. doi: 10.1164/ajrccm.149.1.8111603 [DOI] [PubMed] [Google Scholar]
- 40.Harmony WN. Segmental breathing. Phys Ther Rev. 1956;36:106–107. doi: 10.1093/ptj/36.2.106 [DOI] [PubMed] [Google Scholar]
- 41.Intensive Care National Audit & Research Centre. ICNARC Report on COVID-19 in Critical Care. Intensive Care National Audit & Research Centre; 2020. [Google Scholar]
- 42.Chlif M, Temfemo A, Keochkerian D, Choquet D, Chaouachi A, Ahmaidi S. Advanced Mechanical Ventilatory Constraints During Incremental Exercise in Class III Obese Male Subjects. Respir Care. 2015;60:549–560. doi: 10.4187/respcare.03206 [DOI] [PubMed] [Google Scholar]
- 43.AAPM&R Board of Governors AAPM&R Position Statement on the Necessity and Preservation of Personal Protective Equipment. AAPM&R Position Statement on the Necessity and Preservation of Personal Protective Equipment. https://www.aapmr.org/news-publications/member-news/member-news-details/2020/03/30/aapm-r-position-statement-on-the-necessity-and-preservation-of-personal-protective-equipment#.XoYsMSWqIgQ.email. Published March 30, 2020.
- 44.Dowman L, Hill CJ, Holland AE. Pulmonary rehabilitation for interstitial lung disease. Cochrane Database Syst Rev. 2014;(10):CD006322. doi: 10.1002/14651858.CD006322.pub3 [DOI] [PubMed] [Google Scholar]
- 45.Burtin C, Saey D, Saglam M, et al. :. Effectiveness of exercise training in patients with COPD: the role of muscle fatigue. Eur Respir J. 2012;40:338–344. doi: 10.1183/09031936.00111811 [DOI] [PubMed] [Google Scholar]
- 46.Hui DS, Joynt GM, Wong KT, et al. :. Impact of severe acute respiratory syndrome (SARS) on pulmonary function, functional capacity and quality of life in a cohort of survivors. Thorax. 2005;60:401–409. doi: 10.1136/thx.2004.030205 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Xie L, Liu Y, Xiao Y, et al. :. Follow-up Study on Pulmonary Function and Lung Radiographic Changes in Rehabilitating Severe Acute Respiratory Syndrome Patients After Discharge. Chest. 2005;127:2119–2124. doi: 10.1378/chest.127.6.2119 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Venkataraman T, Frieman MB. The role of epidermal growth factor receptor (EGFR) signaling in SARS coronavirus-induced pulmonary fibrosis. Antiviral Res. 2017;143:142–150. doi: 10.1016/j.antiviral.2017.03.022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Ngai JC, Ko FW, Ng SS, To K-W, Tong M, Hui DS. The long-term impact of severe acute respiratory syndrome on pulmonary function, exercise capacity and health status. Respirology. 2010;15:543–550. doi: 10.1111/j.1440-1843.2010.01720.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Jenkins S, Čečins N. Six-minute walk test: observed adverse events and oxygen desaturation in a large cohort of patients with chronic lung disease. Intern Med J. 2011;41:416–422. doi: 10.1111/j.1445-5994.2010.02169.x [DOI] [PubMed] [Google Scholar]
- 51.Vogiatzis I, Zakynthinos S. Factors limiting exercise tolerance in chronic lung diseases. Compr Physiol. 2012;2:1779–1817. doi: 10.1002/cphy.c110015 [DOI] [PubMed] [Google Scholar]
- 52.Boutou AK, Pitsiou GG, Trigonis I, et al. :. Exercise capacity in idiopathic pulmonary fibrosis: the effect of pulmonary hypertension. Respirology. 2011;16:451–458. doi: 10.1111/j.1440-1843.2010.01909.x [DOI] [PubMed] [Google Scholar]