

Abstract
Background
Conflicting and limited high‐quality prospective data are available on the associations between cam morphology and hip and groin symptoms and range of motion (ROM).
Objectives
This cross‐sectional cohort study investigated associations between cam morphology presence, size and duration and symptoms and ROM.
Methods
Academy male football players (n = 49, 17‐24 years) were included. Standardized antero‐posterior pelvic and frog‐leg lateral radiographs were obtained at baseline, 2.5‐ and 5‐year follow‐up. The femoral head‐neck junction was quantified by:
Visual score. Cam morphology (flattening or prominence), large cam (prominence).
Alpha angle. Cam morphology (≥60°), large cam (≥78°).
Cam morphology duration was defined as long (first present at baseline) or short (only from 2.5‐ to 5‐year follow‐up). Current symptoms at 5‐year follow‐up were assessed using a hip and groin pain question and by the “Hip and Groin Outcome Score” (HAGOS). HAGOS scores were categorized into: most symptoms (≥2 domains in lowest interquartile range [IQR]), least symptoms (≥2 domains in highest IQR). Hip ROM was measured by goniometry at 5‐year follow‐up.
Results
Large cam morphology based on visual score was associated with hip and groin pain (23.8% vs. 7.1%, OR: 3.17, CI: [1.15‐8.70], P = .026), but not with HAGOS scores. Cam morphology presence, size, and duration were associated with limited flexion of around 6° and/or 3° to 6° for internal rotation.
Conclusion
Cam morphology presence, size, and duration were associated with limited hip flexion and/or internal rotation, but differences might not exceed the minimal clinical important difference. Whether cam morphology results in symptoms is uncertain.
Keywords: FAI syndrome, femoroacetabular impingement, pain, range of motion
1. INTRODUCTION
Hip and groin symptoms are frequently observed in professional sports and football in particular. The prevalence of hip and groin symptoms in (elite) football is reported as 49% per season, 1 while the incidence varies between 4% and 19%. 2 , 3 One of the causes of hip and groin symptoms in athletes is femoroacetabular impingement (FAI) syndrome. 4 FAI syndrome is defined by a triad of symptoms, clinical signs, and imaging findings. 4
Imaging findings consistent with FAI syndrome include cam and/or pincer morphology. Cam morphology is an extra bone formation on the anterolateral side of the head‐neck junction of the femur which arises during growth. 5 , 6 , 7 , 8 , 9 It can potentially damage intra‐articular structures such as the cartilage and acetabular labrum and might cause symptoms. 10 , 11
Cam morphology prevalence in football players is high. 5 , 6 , 7 , 9 , 12 Although there is an association between cam morphology and hip osteoarthritis (OA), 12 , 13 , 14 , 15 , 16 , 17 the association between cam morphology and symptoms in athletes remains contradictory. Several cross‐sectional studies showed conflicting results. 18 , 19 , 20 , 21 , 22 One available longitudinal case‐control study 23 showed an association between cam morphology and development of hip pain in the general population with a relative risk of 4.3 (95% confidence interval [CI]: 2.3‐7.8). Another prospective cohort study 24 found no association between cam morphology and groin injuries in professional football players. A large cam morphology is associated with a higher risk for developing hip OA 13 and cartilage damage. 25 , 26 , 27 It might therefore hypothetically result in more symptoms and more limited range of motion (ROM). The influence of cam morphology duration on both symptoms and ROM has never been investigated and can only be assessed when information on when cam morphology arises is available.
Therefore, the study aims of this cohort with young academy male football players were to assess the association between the cam morphology presence, size and duration and hip and groin symptoms and ROM within 5‐year follow‐up.
2. METHODS
2.1. Study participants
At baseline, all academy male football players of the Feyenoord Academy aged between 12 and 19 years (n = 141) received an invitational letter of whom 89 finally participated. All 89 baseline participants were invited again to participate at 2.5‐year follow‐up (n = 63 participants) and the 5‐year follow‐up (n = 49 participants) (Figure 1). Inclusion and exclusion criteria were described previously. 5 , 6 The inclusion for the 5‐year follow‐up took place between June 2015 and October 2015. Ethical approval was obtained from the Medical Ethical Committee of the Erasmus Medical Center (Rotterdam, the Netherlands). Each participant gave written consent. For participants under 18 years, written consent was gathered from at least one parent. Participant characteristics, such as age, weight, height (and BMI), football experience, training intensity, and self‐reported hip and/or groin symptoms, were collected (Table 1).
TABLE 1.
Participant characteristics at 5‐year follow‐up
| Number of participants (hips), n | 49 (98) |
|---|---|
| Age, mean ± standard deviation (SD), (range), y | 20.53 ± 2.17 (17‐24) |
| Weight, mean ± SD (range), kg | 73.77 ± 7.87 (57‐91) |
| Height, mean ± SD (range), cm | 180.33 ± 6.63 (165‐190) |
| Body mass index, mean ± SD (range), kg/m2 | 22.65 ± 1.59 (18.5‐27.0) |
| Football experience, mean ± SD (range), y | 14.29 ± 2.58 (9‐19) |
| Training intensity, mean ± SD (range), h/w | 9.30 ± 2.92 (5‐20) |
| Self‐reported hip and/or groin symptoms per hip, n (%) | 14/98 (14.3%) |
|
7 (50%) |
|
7 (50%) |
| HAGOS domain scores, median (IQR, 25th‐75th centile) | |
|
97.50 (92.50‐100.00) |
|
82.14 (73.21‐92.86) |
|
100.00 (95.00‐100.00) |
|
100.00 (87.50‐100.00) |
|
100.00 (87.50‐100.00) |
|
95.00 (80.00‐100.00) |
| Cam morphology based on alpha angle (≥60°) per hip (n = 98), n (%) | 80 (81.6) |
| Cam morphology based on visual score (flattening or prominence) per hip (n = 98), n (%) | 78 (79.6) |
Abbreviations: HAGOS, Hip and Groin Outcome Score; IQR, interquartile range; SD, standard deviation.
2.2. Radiographs
Three radiographs were obtained during this study by the same standardized radiographic protocol as described previously 5 , 6 ; one supine antero‐posterior pelvic radiograph and a frog‐leg lateral radiograph of each hip.
2.3. Visual scores
The femoral head‐neck junction of all hips was scored qualitatively as normal, flattening, or prominence. 5 , 6 This additional method was used because of alpha angle limitations, especially in hips with an open growth plate. 5 , 7 An experienced musculo‐skeletal radiologist and orthopedic surgeon determined all visual scores simultaneously, and any discrepancies were directly resolved based on consensus. Visual scores were obtained by scoring each hip of all three time points in one session. Visual scores showed a kappa of 0.68 for intra‐observer reliability in the baseline study. 5
2.4. Alpha angle
The alpha angle was automatically calculated on all radiographs, as described by Nötzli et al 28 and was used previously. 5 , 6 In short, the shape of the proximal femur was outlined by a manually positioned anatomical set of points by one observer, by using Statistical Shape Modelling (ASM tool kit, Manchester University, Manchester, UK). The alpha angle was automatically calculated from this point set by using MATLAB v7.1.0 (MathWorks Inc). Intraclass correlation coefficient (ICC) for interobserver reliability was 0.73 (95% confidence interval [CI] 0.56‐0.86). Intra‐observer reliability ICC scores ranged from 0.85 (95% CI 0.49‐0.96) to 0.99 (95% CI 0.93‐1.00). 13 The standard error of measurement (SEM) was 3.45.
2.5. Definition of cam morphology and large cam morphology
The independent variables cam morphology presence and size were analyzed on both the AP view and frog‐leg lateral view at 5‐year follow‐up. The highest score of one of both views was used for analysis. Cam morphology was defined twice, based on the visual score and alpha angle. Cam morphology based on the visual score was defined when either a flattening or prominence was present. Cam morphology based on the alpha angle was defined as alpha angle ≥60°. Large cam morphology based on the visual score was defined as having a prominence. Large cam morphology based on the alpha angle was defined as alpha angle ≥78°. 29
2.6. Cam morphology duration
The third independent variable cam morphology duration was scored dichotomously as “long” or “short” for all radiographs from baseline, 2.5‐year follow‐up, and at 5‐year follow‐up. Long duration was defined as the first presence of cam morphology at baseline and short duration as having cam morphology for the first time at 2.5‐ and/or 5‐year follow‐up.
2.7. Hip and groin pain/symptoms
2.7.1. Questionnaire on hip pain and participant characteristics
Every participant filled out a questionnaire on several participant characteristics at 5‐year follow‐up (Figure 1). This questionnaire contained a question about hip pain: “Do you sometimes have pain in your hips?” A dichotomous answer was possible, “yes” or “no”. When answered positive, the painful side was specified (left, right, and bilateral). They also filled in, if pain occurred during or after sporting activities, or in rest. As this question might include groin pain, we choose “hip and groin pain” as the overall term to define this outcome measure.
2.7.2. Hip and groin outcome score
The “Copenhagen Hip and Groin Outcome Score” (HAGOS) is a valid patient‐reported outcome measure to quantify hip and groin symptomatology. 30 The validated Dutch HAGOS translation was filled out by all participants only at the 5‐year follow‐up (Figure 1). 30 , 31 , 32 This questionnaire obtained information from six domains, specified per person. Each domain is scaled between 0 and 100, with 100 as indicator for no problems, and a lower score for hip and groin symptoms. 32 The football players completed the questionnaires before or on the day at which the radiographs were obtained. All participants were divided into 3 groups based on the level of symptomatology, as described before by Tak et al. 33 The first group is the most symptomatic group in this cohort, defined by at least 2 domains in the lowest interquartile range (IQR) of the HAGOS scores. The group with the least symptomatic participants was defined as having at least 2 domains in the highest IQR of the HAGOS scores. The middle group was the remaining group.
2.8. Hip range of motion
The researcher performing the physical examination was blinded to the outcome of the HAGOS scores and for the radiographs. The same physical examination protocol was used at all time points. 5 , 6 In short, while maintained in neutral rotation, the first resistance/end feel during passive flexion, abduction, adduction, internal rotation and external rotation were measured in supine position and extension in prone position on a flat examination table with a goniometer. Internal and external rotation were measured with 90° of flexion in the hip joint. Stabilization was provided by the free hand of the examiner to the adjacent joints and regions.
2.9. Statistical analysis
The association between cam morphology presence, size and duration at 5‐year follow‐up and hip and groin pain (per hip) and most vs least hip and groin symptoms (based on HAGOS per person) were calculated by means of logistic regression and adjusted for age and body mass index (BMI). The association between cam morphology presence, size and duration at 5‐year follow‐up and ROM was calculated by a linear regression model, adjusted for age and BMI. All per hip regression analyses were performed in a Generalised Estimated Equations (GEE) model. These were all cross‐sectional associations at 5‐year follow‐up. The only longitudinal outcome of this study was the duration of cam morphology which was measured at baseline, 2.5‐year, and 5‐year follow‐up. Absolute rounded ROM averages are presented in Table 5 and 6, with differences observed in the statistical tests presented as estimated mean differences. Differences in baseline characteristics between included participants and dropouts were tested using an independent samples t test. A sensitivity analysis was performed to see if analyzing the HAGOS outcome defined as most symptoms vs middle and least symptoms, gave different results than defining the HAGOS outcome as most vs least symptoms (Table S1). SPSS25.0 (Windows) was used.
TABLE 5.
Association between cam morphology based on visual score and range of motion at 5‐year follow‐up (n = hips)
| Range of motion | Normal (n = 18) | Flattening (n = 38) | Prominence (n = 42) | Cam, P (degrees) a | Large cam, P (degrees) b |
|---|---|---|---|---|---|
| Flexion | 121° ± 8 | 116° ± 6 | 116° ± 7 | .001 (6°) | .30 (2°) |
| Abduction | 43° ± 6 | 41° ± 4 | 42° ± 5 | .40 (1°) | .71 (0°) |
| Adduction | 26° ± 6 | 27° ± 6 | 27° ± 6 | .80 (0°) | .90 (0°) |
| Internal rotation | 28° ± 10 | 26° ± 6 | 24° ± 8 | .12 (3°) | .033 (3°) |
| External rotation | 36° ± 6 | 34° ± 5 | 34° ± 7 | .17 (2°) | .84 (0°) |
| Extension | 22° ± 4 | 23° ± 5 | 22° ± 5 | .06 (1°) | .58 (1°) |
Values are expressed as mean ± standard deviation.
Cam morphology vs having no cam morphology. Difference between groups is also presented in degrees range of motion.
Large cam morphology vs having no large cam morphology. Difference between groups is also presented as the estimated mean difference in degrees range of motion.
Bolded P‐values indicate a statistically significant difference.
TABLE 6.
Association between cam morphology based on alpha angle (AA) and range of motion at 5‐year follow‐up (n = hips)
| Range of motion | AA < 60° (n = 20) | AA 60°‐78° (n = 53) | AA ≥ 78° (n = 25) | Cam (P) a | Large cam (P) b |
|---|---|---|---|---|---|
| Flexion | 122 ± 9 | 117 ± 6 | 113 ± 7 | .032 (5°) | .049 (3°) |
| Abduction | 44 ± 5 | 41 ± 5 | 42 ± 5 | .18 (2°) | .42 (1°) |
| Adduction | 26 ± 5 | 27 ± 5 | 26 ± 6 | .99 (0°) | .48 (1°) |
| Internal rotation | 30 ± 9 | 26 ± 7 | 21 ± 7 | .005 (4°) | .05 (3°) |
| External rotation | 35 ± 6 | 34 ± 6 | 33 ± 7 | .55 (1°) | .28 (2°) |
| Extension | 23 ± 5 | 23 ± 5 | 20 ± 4 | .25 (1°) | .11 (1°) |
Values are expressed as mean ± standard deviation.
Cam morphology vs having no cam morphology. Difference between groups is also presentsed in degrees range of motion.
Large cam morphology vs having no large cam morphology. Difference between groups is also presented as the estimated mean difference in degrees range of motion.
Bolded P‐values indicate a statistically significant difference.
3. RESULTS
3.1. Participant characteristics
Demographic data of the participants are summarized in Table 1. The mean follow‐up time was 5.3 ± 0.1 years (range 5.0‐5.6 years). Of the 89 baseline participants (12‐19 years old), 49 (55%) participated at 5‐year follow‐up. No differences in baseline demographic data between these 49 participants and 40 dropouts were observed, Table 2. 9 Participants dropped out for various reasons: 24 rejected the invitation, 11 were unreachable, 4 lived abroad, and 1 person accepted the invitation but did not appear during the allocated time‐slot. All 49 included participants still played football at the time of the 5‐year follow‐up study. Of those, 28 (57%) were still active in a first or second team of a professional football club. All other 21 football players (43%) played football at an amateur level. Cam morphology prevalence was 82% (80 of 98 hips) based on visual score and 80% (78 of 98 hips) based on the alpha angle.
TABLE 2.
Demographic baseline data of 5‐year follow‐up participants compared to dropouts a
| Participant characteristics |
Baseline (n = 49) 5‐year follow‐up participants |
Baseline (n = 40) 5‐year follow‐up dropouts |
P |
|---|---|---|---|
| Age, y | 15.20 ± 2.13 | 15.25 ± 1.77 | .88 |
| Weight, kg | 58.54 ± 14.71 | 60.43 ± 12.60 b | .37 |
| Height, cm | 169.35 ± 13.16 | 171.47 ± 10.67 b | .25 |
| Body mass index, kg/m2 | 20.01 ± 2.32 | 20.29 ± 2.17 b | .42 |
| Football experience, y | 8.84 ± 2.65 | 9.13 ± 2.40 b | .45 |
| Training intensity, h/w | 7.87 ± 1.57 | 8.08 ± 2.00 b | .45 |
| Prevalence of cam, symptoms, and ROM | |||
| Cam morphology prevalence (VS/AA), % | |||
|
48.0 | 62.5 | .05 |
|
48.0 | 50.0 | .80 |
| Hip and groin pain, % per hip | 20.4 | 13.2 | .20 |
| Range of motion | |||
| |||
|
123.88 ± 6.54 | 123.87 ± 6.64 | .99 |
|
125.92 ± 8.05 | 123.45 ± 8.84 | .05 |
| |||
|
41.92 ± 10.26 | 39.83 ± 9.40 | .16 |
|
41.22 ± 7.78 | 38.60 ± 8.25 | .031 |
| |||
|
30.80 ± 3.95 | 28.80 ± 5.21 | .005 |
|
30.06 ± 5.27 | 28.55 ± 5.64 | .07 |
| |||
|
27.57 ± 8.15 | 26.33 ± 8.36 | .32 |
|
23.71 ± 7.39 | 22.75 ± 9.40 | .46 |
| |||
|
40.35 ± 8.82 | 35.50 ± 9.06 | <.001 |
|
37.22 ± 9.45 | 34.23 ± 8.74 | .031 |
| |||
|
14.89 ± 2.39 | 14.31 ± 3.22 | .19 |
|
15.03 ± 2.53 | 14.56 ± 2.89 | .26 |
Abbreviations: AA, alpha angle; ROM, range of motion; VS, visual score.
Values are expressed as mean ± standard deviation.
Data of n = 38 are presented, due to missing data.
Bolded P‐values indicate a statistically significant difference.
3.2. Cam morphology and hip and groin pain
Nine players (18.4%) reported hip and groin pain (5 bilateral and 4 unilateral). Of these 14 hips, 10 hips were painful at one occasion and 4 at two occasions; 1 hip both during sports and at rest and 3 hips directly after sports and at rest. In total, 4 hips were painful during sports, 6 hips directly after sports, and 8 hips at rest.
Of 80 hips with cam morphology based on visual score, 11 hips (13.8%) had hip and groin pain compared to 3 of 18 hips (16.7%) without cam (OR: 0.51, CI: [0.15‐1.69]). Of 78 hips with cam morphology based on alpha angle, 9 hips (11.5%) had hip and groin pain, compared to 5 of 20 hips (25.0%) without cam (OR: 0.42, CI: [0.13‐1.32]). Of the 42 hips with large cam morphology based on visual score, 10 hips (23.8%) had hip and groin pain compared to 4 of 56 hips (7.1%) without large cam (OR: 3.17, CI: [1.15‐8.70], P = .026). Of 25 hips with large cam morphology based on alpha angle, 4 hips (16.0%) had hip and groin pain compared to 10 of 73 hips (13.7%) without large cam (OR: 1.21, CI: [0.60‐2.43]) (Table 3).
TABLE 3.
Association between cam morphology based on both visual score (VS) and alpha angle (AA) and symptoms at 5‐year follow‐up
| HAGOS questionnaire (per person) | Normal | Flattening | Prominence | AA < 60° | AA 60°‐78° | AA ≥ 78° | Cam, P a (VS/AA) | Large cam, P b (VS/AA) |
|---|---|---|---|---|---|---|---|---|
| Most symptoms | 2/4 (50.0%) | 3/16 (18.8%) | 7/25 (28.0%) | 3/5 (60.0%) | 5/22 (22.7%) | 4/18 (22.2%) | .21/.14 | .88/.95 |
| Least symptoms | 2/4 (50.0%) | 13/16 (81.3%) | 18/25 (72.0%) | 2/5 (40.0%) | 17/22 (77.3%) | 14/18 (77.8%) | ||
| Hip and groin pain (per hip) | ||||||||
|
3/18 (16.7%) | 1/38 (2.6%) | 10/42 (23.8%) | 5/20 (25.0%) | 5/53 (9.4%) | 4/25 (16.0%) | .27/.14 | .026/.60 |
Cam morphology vs having no cam morphology. For associations between cam morphology presence and size and HAGOS, “most vs least symptoms” is used.
Large cam morphology vs having no large cam morphology.
Bolded P‐values indicate a statistically significant difference.
Of 47 hips with long cam morphology duration based on visual score, 7 hips (14.9%) had hip and groin pain compared to 4 of the 33 hips (12.1%) with short cam duration (OR: 1.99, CI: [0.19‐21.19]). Long cam morphology duration defined by the alpha angle, resulted in 6 of 47 hips (12.8%) with hip and groin pain, compared to 3 of 31 hips (9.7%) with short cam duration (OR: 1.63, CI: [0.24‐10.93]).
3.3. Cam morphology and hip and groin symptoms
Hip and Groin Outcome scores were not normally distributed. The median and IQRs of all 6 HAGOS domains of this cohort are presented in Table 1 . An overview of the distribution of the HAGOS domains per HAGOS group (most, middle, and least symptoms) in this cohort is presented in Table 4. The group with most symptoms consisted of 12 of 49 football players (25%), the group with the least symptoms consisted of 33 football players (67%) and the middle group consisted of 4 football players (8%).
TABLE 4.
Spreading of all 6 HAGOS domain medians for the 3 different HAGOS groups at 5‐year follow‐up a
| HAGOS group b | Persons | Pain | Symptoms | Function in DL | S&R | PA | QoL |
|---|---|---|---|---|---|---|---|
| Most symptoms | 12 | 87.50 (80.63‐94.38) | 66.07 (58.04‐76.79) | 90.00 (85.00‐95.00) | 82.81 (67.97‐84.38) | 81.25 (75.00‐100.00) | 70.00 (61.25‐80.00) |
| Middle | 4 | 96.25 (93.13‐99.38) | 80.36 (67.86‐82.14) | 100.00 (96.25‐100.00) | 92.19 (81.25‐96.09) | 87.50 (78.13‐87.50) | 85.00 (68.75‐97.50) |
| Least symptoms | 33 | 100.00 (95.00‐100.00) | 89.29 (82.14‐96.43) | 100.00 (100.00‐100.00) | 100.00 (100.00‐100.00) | 100.00 (100.00‐100.00) | 100.00 (90.00‐100.00) |
Abbreviations: DL, daily living; PA, physical activities; QoL, quality of life; S&R, sports & recreation.
Values are expressed as median (IQR, 25th‐75th centile).
Most symptoms are defined by at least 2 domains in the lowest interquartile range (IQR), least symptoms by at least 2 domains in the highest IQR and the middle group is the remaining group.
In the group with cam morphology based on visual score, 10 of 41 persons (24.4%) were classified into the group with most symptoms. In the group without cam, most symptoms were observed in 2 of 4 persons (50.0%) (OR: 0.24, CI: [0.03‐2.20]). In the group with cam morphology based on alpha angle, 9 of 40 persons (22.5%) were classified into the group with most symptoms. In the group without cam, most symptoms were observed in 3 of 5 persons (60.0%) (OR: 0.22, CI: [0.03‐1.67]). Large cam morphology based on visual score was observed in 25 persons (51.0%), and 7 of them (28.0%) were classified in the group with most symptoms. In the group without large cam, most symptoms were observed in 5 of 20 persons (25.0%) (OR: 1.12, CI: [0.28‐4.46]). Large cam morphology based on alpha angle was observed in 18 persons (36.7%), and 4 of them (22.2%) were classified into the group with most symptoms. In the group without large cam, most symptoms were observed in 8 of 27 persons (29.6%) (OR: 0.95, CI: [0.21‐4.30]) (Table 3).
Long cam morphology duration defined by the visual score, resulted in 9 of 27 persons (33.3%) in the group with most symptoms. Short cam duration was observed in 1 of 14 persons (7.1%) in the group with most symptoms (OR: 12.92, CI: [0.88‐188.93], P = .062). Long cam morphology duration defined by the alpha angle resulted in 8 of 29 persons (27.6%) in the group with most symptoms. Short cam duration was observed in 1 of 11 persons (9.1%) in the group with most symptoms (OR: 4.27, CI: [0.40‐45.52]).
3.4. Cam morphology and range of motion
The average flexion was lower in hips with cam morphology than in hips without cam based on visual score (116° ± 6° vs 121° ± 8°, P = .001) and alpha angle (116° ± 6° vs 122° ± 9°, P = .032) (Tables 5 and 6). Lower average internal rotation was observed in hips with cam morphology based on alpha angle, compared to hips without cam (24° ± 7° vs 30° ± 9°, P = .005) (Table 6). The average internal rotation in hips with large cam morphology based on visual score was lower than in hips without large cam (24 ± 8° vs 27° ± 7°, P = .033) (Table 5). Limited flexion was observed in hips with large cam morphology based on alpha angle, compared to hips without large cam (113° ± 7° vs 118° ± 7°, P = .049) (Table 6). Lower flexion was observed in hips with cam morphology based on alpha angle for at least 5 years (long duration), than hips with cam for 2.5 years or less (short duration) (115° ± 6° vs 116° ± 7°, P = .016).
4. DISCUSSION
The relationship between cam morphology and hip and groin symptoms is inconsistent. A large cam morphology based on the visual score in young male academy football players showed an association with hip and groin pain, but not with more hip and groin symptoms as defined by the HAGOS score. A longer cam morphology duration was not significantly associated with more hip and groin symptoms. Cam morphology presence and size were associated with limited flexion and internal rotation, whereas a longer cam morphology duration was only associated with limited flexion.
4.1. Cam morphology and hip and groin pain/symptoms
Large cam morphology was significantly associated with hip and groin pain, but not with the HAGOS scores. Other cross‐sectional studies on this association showed conflicting results. Mayes et al 22 did not find an association between cam morphology and with HAGOS scores < 100 in ballet dancers. Anderson et al, 19 who investigated 547 individuals (1081 hips, mean age 67 years), did not find a significant association between cam morphology and the “modified Harris Hip Scores” or “Hip Outcome Scores.” Also, no association between cam morphology and self‐reported hip pain was found by Gosvig et al 20 who studied 3202 participants from the general population. A longitudinal study by Mosler et al 24 could not identify an association between cam morphology and groin injuries in professional athletes.
However, other studies did show an association between cam morphology and hip and groin symptoms. A longitudinal study by Khanna et al 23 focused on the development of hip pain at 4.4‐year follow‐up in 170 asymptomatic volunteers (mean age 29.5 years) at baseline. Seven of 14 (50.0%) painful hips had cam morphology compared with 37 of 318 (11.6%) painless hips at follow‐up (RR: 4.3, P = .0002). Other cross‐sectional studies also found an association. Larson et al 21 studied 125 National Football League prospects and observed a significantly higher cam morphology prevalence in the symptomatic group (P = .009). Allen et al 18 demonstrated a significant association between higher alpha angles in painful hips (mean 69.9°) than in asymptomatic hips (mean 63.1°). In a retrospective study of 334 patients, a significant association between hip symptoms and increased alpha angles (P < .001) was observed as well. 34
An explanation for the absence of association between cam morphology (flattening or prominence and/or alpha angle ≥60°) and symptoms within 5‐year follow‐up could be that only larger cam morphology can cause rapid intra‐articular damage. This is in line with the higher risk of developing hip OA when cam morphology is bigger. 12 , 29 No association between cam morphology and HAGOS scores was observed in this study. HAGOS scores in the group classified as most symptoms in this cohort were ranging between 66.07 and 90.00, indicating that symptoms were mild. Also, the HAGOS score is a score per person rather than per hip, which might dilute the association in the presence of unilateral cam morphology. Also, the HAGOS questionnaire captures hip and groin symptoms and not only hip‐related pain, as other entities of groin pain might be more prevalent in football players than pain arising from the hip joint. Another explanation could be that participants were young. Cam morphology arises from 12 to 14 years old 5 , 6 , 7 , 8 , 9 , 35 and continues to grow thereafter until growth plate closure. During 5‐year follow‐up, participants were aged 20.5 years (17‐24 years) on average. Therefore, the cam morphology duration might have been too short to create hip damage and symptoms. This is supported by our findings that 33.3% of the group with long cam morphology duration based on visual score was classified in the most symptoms group, compared to 7.1% in the short duration group. Although not statistically significant (P = .06), future studies on the relationship between cam morphology and symptoms should also take into account the duration of cam morphology. It could also be that football players are not keen to report about their (hip and groin) complaints as they may be afraid of losing their place on the pitch. Finally, the pathway from having cam morphology into developing the clinical entity of FAI syndrome and thus pain is complex and also involves the amount of femoral and acetabular version, soft‐tissue structures, activities which a person undertakes and many other person‐specific factors. Obviously, it can also be that the presence of cam morphology itself is not associated with symptoms or reduced range of motion, as cam morphology is also highly prevalent in asymptomatic populations. 11
4.2. Cam morphology and range of motion
Significant associations between cam morphology presence and limited flexion and internal rotation were observed and influenced by cam morphology size. A longer cam morphology duration only negatively influenced the amount of flexion. Our findings partly correspond with current available literature. Audenaert et al 36 observed a significantly lower range of internal rotation in the cam morphology group (based on CT) vs a group without cam morphology. In collegiate football players, Kapron et al 37 found a significant association between alpha angle and limited internal rotation. Mosler et al 38 screened 426 male professional football players in Qatar for 2 consecutive seasons and observed that asymptomatic hips with cam morphology and large cam morphology were associated with lower internal rotation. Interestingly, a systematic review of Freke et al 39 did only find limited and conflicting evidence on the association of cam morphology and limited ROM in symptomatic patients. However, ROM in symptomatic hips might also be influenced by pain rather than cam morphology only. 33 In the current study, the average differences between hips with and without cam morphology were around 6° for flexion and 3°‐6° for internal rotation. This raises questions on whether these differences are clinically relevant.
Not all growth plates were closed (93.9%) at 5‐year follow‐up. This means that hips with open growth plates might still have the potential to develop cam morphology or increase to a large cam morphology. 9 This can possibly cause more severe impingement, and therefore result in more symptoms and limited ROM in the future.
4.3. Limitations
Some limitations in this study have to be acknowledged. During 5‐year follow‐up, 40 participants (44.9%) were lost to follow‐up. Although there were no differences in baseline characteristics between participants and dropouts, it has bias, as it resulted in a relatively small sample size. Due to the small sample size and low proportion of hips without cam morphology, the resulting findings have wide confidence intervals. Of the included 49 participants, 42.9% played football at an amateur level, with lower intensity and training hours per week. This could have resulted in lower cam morphology prevalence 12 , 35 and might have influenced symptoms. 40 A possible limitation of the patient characteristics questionnaire is that it cannot be excluded that the question “Do you sometimes have pain in your hips?” also included patients with groin symptoms and made no distinction between long standing and acute hip and groin symptoms. However, large cam morphology based on the alpha angle was associated with hip and groin pain based on this question, which indicates that type II errors are not likely. As the HAGOS‐domain scores were not normally distributed and as the median scores in 3 out of 6 domains are having the maximum score of 100, a ceiling effect cannot be ruled out.
By using radiographs, the prevalence of cam morphology might have been underestimated as compared to cross‐sectional imaging such as magnetic resonance imaging (MRI) or computed tomography (CT). However, by using two radiographic views (AP and frog‐leg lateral), as recommended by the Warwick Agreement, 4 the risk of false‐negative measurements was minimalized.
4.4. Range of motion
The ROM was obtained before or after training, which could have resulted in different outcomes. Range of motion measurement by goniometry could result in measurement errors and can give an overestimation of the ROM. 41 Beside this limitation, range of motion is an acceptable and reliable measurement method for longitudinal studies in FAI syndrome patients. The reliability of range of motion testing of the hip is described in literature as good to excellent by Prather et al. 42
5. CONCLUSION
Data of this cohort study suggest that the presence, size, and duration of a bony cam morphology have a direct but small effect on the range of motion. Symptoms might develop in some football players with large cam morphology or several years after cam morphology development. A larger prospective cohort is needed to further elucidate these findings.
6. PERSPECTIVES
Our study showed that large cam morphology is only associated with hip and groin symptoms but not with HAGOS scores. The presence, size, and duration of cam morphology are associated with limited flexion and/or internal rotation, although the clinical relevance of these differences is questionable. This suggests that a bony cam morphology has a direct but small effect on the range of motion and symptoms which might develop in some players several years after cam morphology has developed. More factors are involved in the complex pathway between cam morphology and developing the clinical entity of FAI syndrome with symptoms and limited function, such as femoral and acetabular orientation, soft‐tissue condition (eg, labrum, cartilage, ligamentum teres), activity level, and many other person‐specific factors. This needs further investigation in a larger cohort.
7.
FIGURE 1.
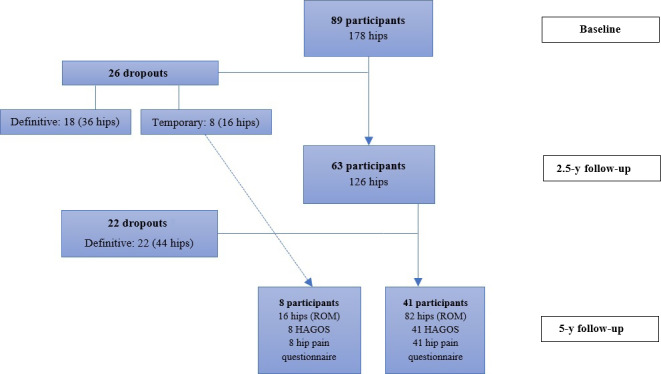
Flowchart of all analysed HAGOS questionnaires, hip pain questionnaires and ROM at all time‐points
Supporting information
Table S1
ACKNOWLEDGEMENTS
We want to thank Raymond van Meenen, Rob Kurvers, Marcel de Geus, and other staff members of Feyenoord Football Academy for their collaboration in this study. This study would not have been possible without its participants and their families, to whom we offer our sincerest gratitude. The authors declare that they have no conflicts of interest.
van Klij P, Ginai AZ, Heijboer MP, Verhaar JAN, Waarsing JH, Agricola R. The relationship between cam morphology and hip and groin symptoms and signs in young male football players. Scand J Med Sci Sports. 2020;30:1221–1231. 10.1111/sms.13660
REFERENCES
- 1. Thorborg K, Rathleff MS, Petersen P, Branci S, Holmich P. Prevalence and severity of hip and groin pain in sub‐elite male football: a cross‐sectional cohort study of 695 players. Scand J Med Sci Sports. 2017;27(1):107‐114. [DOI] [PubMed] [Google Scholar]
- 2. Walden M, Hagglund M, Ekstrand J. The epidemiology of groin injury in senior football: a systematic review of prospective studies. Br J Sports Med. 2015;49(12):792‐797. [DOI] [PubMed] [Google Scholar]
- 3. Werner J, Hagglund M, Walden M, Ekstrand J. UEFA injury study: a prospective study of hip and groin injuries in professional football over seven consecutive seasons. Br J Sports Med. 2009;43(13):1036‐1040. [DOI] [PubMed] [Google Scholar]
- 4. Griffin DR, Dickenson EJ, O'Donnell J, et al. The Warwick Agreement on femoroacetabular impingement syndrome (FAI syndrome): an international consensus statement. Br J Sports Med. 2016;50(19):1169‐1176. [DOI] [PubMed] [Google Scholar]
- 5. Agricola R, Bessems JH, Ginai AZ, et al. The development of Cam‐type deformity in adolescent and young male soccer players. Am J Sports Med. 2012;40(5):1099‐1106. [DOI] [PubMed] [Google Scholar]
- 6. Agricola R, Heijboer MP, Ginai AZ, et al. A cam deformity is gradually acquired during skeletal maturation in adolescent and young male soccer players: a prospective study with minimum 2‐year follow‐up. Am J Sports Med. 2014;42(4):798‐806. [DOI] [PubMed] [Google Scholar]
- 7. Palmer A, Fernquest S, Gimpel M, et al. Physical activity during adolescence and the development of cam morphology: a cross‐sectional cohort study of 210 individuals. Br J Sports Med. 2018;52(9):601‐610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Siebenrock KA, Ferner F, Noble PC, Santore RF, Werlen S, Mamisch TC. The cam‐type deformity of the proximal femur arises in childhood in response to vigorous sporting activity. Clin Orthop Relat Res. 2011;469(11):3229‐3240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. van Klij P, Heijboer MP, Ginai AZ, Verhaar JAN, Waarsing JH, Agricola R. Cam morphology in young male football players mostly develops before proximal femoral growth plate closure: a prospective study with 5‐yearfollow‐up. Br J Sports Med. 2018;53(9):532‐538. [DOI] [PubMed] [Google Scholar]
- 10. Beck M, Kalhor M, Leunig M, Ganz R. Hip morphology influences the pattern of damage to the acetabular cartilage: femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br. 2005;87(7):1012‐1018. [DOI] [PubMed] [Google Scholar]
- 11. Heerey JJ, Kemp JL, Mosler AB, et al. What is the prevalence of imaging‐defined intra‐articular hip pathologies in people with and without pain? A systematic review and meta‐analysis. Br J Sports Med. 2018;52(9):581‐593. [DOI] [PubMed] [Google Scholar]
- 12. van Klij P, Heerey J, Waarsing JH, Agricola R. The prevalence of cam and pincer morphology and its association with development of hip osteoarthritis. J Orthop Sports Phys Ther. 2018;48(4):230‐238. [DOI] [PubMed] [Google Scholar]
- 13. Agricola R, Heijboer MP, Bierma‐Zeinstra SM, Verhaar JA, Weinans H, Waarsing JH. Cam impingement causes osteoarthritis of the hip: a nationwide prospective cohort study (CHECK). Ann Rheum Dis. 2013;72(6):918‐923. [DOI] [PubMed] [Google Scholar]
- 14. Nelson AE, Stiller JL, Shi XA, et al. Measures of hip morphology are related to development of worsening radiographic hip osteoarthritis over 6 to 13 year follow‐up: the Johnston County Osteoarthritis Project. Osteoarthritis Cartilage. 2016;24(3):443‐450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Nicholls AS, Kiran A, Pollard TC, et al. The association between hip morphology parameters and nineteen‐year risk of end‐stage osteoarthritis of the hip: a nested case‐control study. Arthritis Rheum. 2011;63(11):3392‐3400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Saberi Hosnijeh F, Zuiderwijk ME, Versteeg M, et al. Cam deformity and acetabular dysplasia as risk factors for hip osteoarthritis. Arthritis Rheumatol. 2017;69(1):86‐93. [DOI] [PubMed] [Google Scholar]
- 17. Thomas GE, Palmer AJ, Batra RN, et al. Subclinical deformities of the hip are significant predictors of radiographic osteoarthritis and joint replacement in women. A 20 year longitudinal cohort study. Osteoarthritis Cartilage. 2014;22(10):1504‐1510. [DOI] [PubMed] [Google Scholar]
- 18. Allen D, Beaule PE, Ramadan O, Doucette S. Prevalence of associated deformities and hip pain in patients with cam‐type femoroacetabular impingement. J Bone Joint Surg Br. 2009;91(5):589‐594. [DOI] [PubMed] [Google Scholar]
- 19. Anderson LA, Anderson MB, Kapron A, et al. The 2015 Frank Stinchfield Award: radiographic abnormalities common in senior athletes with well‐functioning hips but not associated with osteoarthritis. Clin Orthop Relat Res. 2016;474(2):342‐352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Gosvig KK, Jacobsen S, Sonne‐Holm S, Gebuhr P. The prevalence of cam‐type deformity of the hip joint: a survey of 4151 subjects of the Copenhagen Osteoarthritis Study. Acta Radiol. 2008;49(4):436‐441. [DOI] [PubMed] [Google Scholar]
- 21. Larson CM, Sikka RS, Sardelli MC, et al. Increasing alpha angle is predictive of athletic‐related "hip" and "groin" pain in collegiate National Football League prospects. Arthroscopy. 2013;29(3):405‐410. [DOI] [PubMed] [Google Scholar]
- 22. Mayes S, Ferris AR, Smith P, Garnham A, Cook J. Bony morphology of the hip in professional ballet dancers compared to athletes. Eur Radiol. 2017;27(7):3042‐3049. [DOI] [PubMed] [Google Scholar]
- 23. Khanna V, Caragianis A, Diprimio G, Rakhra K, Beaule PE. Incidence of hip pain in a prospective cohort of asymptomatic volunteers: is the cam deformity a risk factor for hip pain? Am J Sports Med. 2014;42(4):793‐797. [DOI] [PubMed] [Google Scholar]
- 24. Mosler AB, Weir A, Serner A, et al. Musculoskeletal screening tests and bony hip morphology cannot identify male professional soccer players at risk of groin injuries: a 2‐year prospective cohort study. Am J Sports Med. 2018;46(6):1294‐1305. [DOI] [PubMed] [Google Scholar]
- 25. Beaule PE, Hynes K, Parker G, Kemp KA. Can the alpha angle assessment of cam impingement predict acetabular cartilage delamination? Clin Orthop Relat Res. 2012;470(12):3361‐3367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Johnston TL, Schenker ML, Briggs KK, Philippon MJ. Relationship between offset angle alpha and hip chondral injury in femoroacetabular impingement. Arthroscopy. 2008;24(6):669‐675. [DOI] [PubMed] [Google Scholar]
- 27. Pollard TC, McNally EG, Wilson DC, et al. Localized cartilage assessment with three‐dimensional dGEMRIC in asymptomatic hips with normal morphology and cam deformity. J Bone Joint Surg Am. 2010;92(15):2557‐2569. [DOI] [PubMed] [Google Scholar]
- 28. Notzli HP, Wyss TF, Stoecklin CH, Schmid MR, Treiber K, Hodler J. The contour of the femoral head‐neck junction as a predictor for the risk of anterior impingement. J Bone Joint Surg Br. 2002;84(4):556‐560. [DOI] [PubMed] [Google Scholar]
- 29. Agricola R, Waarsing JH, Thomas GE, et al. Cam impingement: defining the presence of a cam deformity by the alpha angle: data from the CHECK cohort and Chingford cohort. Osteoarthritis Cartilage. 2014;22(2):218‐225. [DOI] [PubMed] [Google Scholar]
- 30. Thorborg K, Holmich P, Christensen R, Petersen J, Roos EM. The Copenhagen Hip and Groin Outcome Score (HAGOS): development and validation according to the COSMIN checklist. Br J Sports Med. 2011;45(6):478‐491. [DOI] [PubMed] [Google Scholar]
- 31. Tak I, Tijssen M, Schamp T, et al. The Dutch hip and groin outcome score: cross‐cultural adaptation and validation according to the COSMIN checklist. J Orthop Sports Phys Ther. 2018;48(4):299‐306. [DOI] [PubMed] [Google Scholar]
- 32. Thorborg K, Branci S, Stensbirk F, Jensen J, Holmich P. Copenhagen hip and groin outcome score (HAGOS) in male soccer: reference values for hip and groin injury‐free players. Br J Sports Med. 2014;48(7):557‐559. [DOI] [PubMed] [Google Scholar]
- 33. Tak I, Glasgow P, Langhout R, Weir A, Kerkhoffs G, Agricola R. Hip range of motion is lower in professional soccer players with hip and groin symptoms or previous injuries, independent of cam deformities. Am J Sports Med. 2016;44(3):682‐688. [DOI] [PubMed] [Google Scholar]
- 34. Guler O, Isyar M, Karatas D, Ormeci T, Cerci H, Mahirogullari M. A retrospective analysis on the correlation between hip pain, physical examination findings, and alpha angle on MR images. J Orthop Surg Res. 2016;11(1):140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Tak I, Weir A, Langhout R, et al. The relationship between the frequency of football practice during skeletal growth and the presence of a cam deformity in adult elite football players. Br J Sports Med. 2015;49(9):630‐634. [DOI] [PubMed] [Google Scholar]
- 36. Audenaert EA, Peeters I, Vigneron L, Baelde N, Pattyn C. Hip morphological characteristics and range of internal rotation in femoroacetabular impingement. Am J Sports Med. 2012;40(6):1329‐1336. [DOI] [PubMed] [Google Scholar]
- 37. Kapron AL, Anderson AE, Peters CL, et al. Hip internal rotation is correlated to radiographic findings of cam femoroacetabular impingement in collegiate football players. Arthroscopy. 2012;28(11):1661‐1670. [DOI] [PubMed] [Google Scholar]
- 38. Mosler AB, Agricola R, Thorborg K, et al. Is bony hip morphology associated with range of motion and strength in asymptomatic male soccer players? J Orthop Sports Phys Ther. 2018;48(4):250‐259. [DOI] [PubMed] [Google Scholar]
- 39. Freke MD, Kemp J, Svege I, Risberg MA, Semciw A, Crossley KM. Physical impairments in symptomatic femoroacetabular impingement: a systematic review of the evidence. Br J Sports Med. 2016;50(19):1180. [DOI] [PubMed] [Google Scholar]
- 40. Herrero H, Salinero JJ, Del Coso J. Injuries among Spanish male amateur soccer players: a retrospective population study. Am J Sports Med. 2014;42(1):78‐85. [DOI] [PubMed] [Google Scholar]
- 41. Nussbaumer S, Leunig M, Glatthorn JF, Stauffacher S, Gerber H, Maffiuletti NA. Validity and test‐retest reliability of manual goniometers for measuring passive hip range of motion in femoroacetabular impingement patients. BMC Musculoskelet Disord. 2010;11:194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Prather H, Harris‐Hayes M, Hunt DM, Steger‐May K, Mathew V, Clohisy JC. Reliability and agreement of hip range of motion and provocative physical examination tests in asymptomatic volunteers. PM R. 2010;2(10):888‐895. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1