

Abstract
Stress is an increasing problem that can result in various psychiatric and somatoform symptoms. Among others, benzodiazepines and valerian preparations are used to treat stress symptoms. The aim of this study was to investigate whether the prescription of a fixed herbal extract combination of valerian, lemon balm, passionflower, and butterbur (Ze 185) changes the prescription pattern of benzodiazepines in hospitalized psychiatric patients. In a retrospective case‐control study, anonymized medical record data from 3,252 psychiatric in‐house patients were analysed over a 3.5‐year period. Cases (n = 1,548) with a prescription of Ze 185 and controls (n = 1,704) were matched by age, gender, hospitalization interval, and main International Classification of Diseases, Version 10 F‐diagnoses. The primary objective was to investigate the effect of Ze 185 on the prescription pattern of benzodiazepines. Secondary objectives investigated the prescriptions of concomitant drugs and effectiveness of the hospital stay. Distribution of drug classes was analysed using the WHO's anatomic‐therapeutic‐chemical code. Data showed that both treatment modalities had a comparable clinical effectiveness but with significantly less prescriptions of benzodiazepines in the Ze 185 group (p = .006). This is of clinical importance because suitable alternatives to benzodiazepines are desirable. To obtain more support for this hypothesis, a dedicated randomized, controlled clinical trial monitoring drug safety is required.
Keywords: anxiety, benzodiazepines, depression, phyto‐anxiolytic, psychiatric disorders, Ze 185
Abbreviations
- AMDP
Association for Methodology and Documentation in Psychiatry
- ATC
Anatomic‐Therapeutic‐Chemical (WHO classification system)
- CGI
Clinical Global Impression
- CIS
Clinical Information System
- GAF
Global Assessment of Functioning
- ICD‐10
International Classification of Diseases, Version 10
- RCT
Randomized Controlled Trial
1. INTRODUCTION
In modern societies, stress is an increasing problem that can result in various somatoform symptoms such as sleep disorders. In a Swiss survey about sleeping habits, sleep quality and the use of sedatives, 2.8% of the respondents reported that they take medication to improve sleep. The most frequently taken sedative drugs were benzodiazepines as well as valerian preparations or benzodiazepine‐like drugs (Tinguely, Landolt, & Cajochen, 2014). Long‐term use of benzodiazepines can pose important adverse effects, which should be considered. These adverse effects include drug dependence, abuse, hangover effects, cognitive and memory impairment, drowsiness, ataxia, motor incoordination, and falls (Gerlach, Maust, Leong, Mavandadi, & Oslin, 2018; Johnson & Streltzer, 2013; Woods, Katz, & Winger, 1992). Especially in elderly, a more than 50% increased risk of hip fractures was found, not to mention consequential costs (Finkle et al., 2011; Johnson & Streltzer, 2013). As a consequence of important identified safety risks, an association between benzodiazepines and an increased risk of mortality was discussed (Agarwal & Landon, 2019; Donnelly, Bracchi, Hewitt, Routledge, & Carter, 2017; Palmaro, Dupouy, & Lapeyre‐Mestre, 2015; Patorno, Glynn, Levin, Lee, & Huybrechts, 2017; Woods et al., 1992). Chronic use of benzodiazepines can lead to tolerance to the pharmacological effects and withdrawal symptoms after discontinuation of the drug. They act not only as sedatives but also have myorelaxant and anxiolytic effects. In addition, recreational use is a relevant complication (Lalive, Rudolph, Luscher, & Tan, 2011).
As stress causes various symptoms, such as anxiety, agitation, nervous tension, and sleep disorders, a single drug might be not the solution for the problem. A suitable way to treat stress‐related symptoms may be the administration of a multicomponent mixture. Herbal medicinal products contain various active ingredients by nature. In the European Union, preparations of Valeriana officinalis L. (Valerianaceae), Melissa officinalis L. (Lamiaceae), and Passiflora incarnata L. (Passifloraceae) are traditionally used for the treatment of nervous tension, the relief of mild symptoms of mental stress, and to aid sleep; either as single extracts or in combination with other herbal extracts (EMA/HMPC, 2013, 2014, 2016). In Switzerland, complementary medicine, including treatment methods with evidence‐based herbal medicine, is well accepted by patients and currently covered by the mandatory basic health insurance, when performed by a certified physician (Klein, Torchetti, Frei‐Erb, & Wolf, 2015). There is one authorized herbal medicinal combination product (Ze 185) that, in addition to the above‐mentioned herbal extracts, contains a dry extract of Petasites hybridus (L.) Gaertn., B. Mey. & Scherb (Asteraceae). P. hybridus is best known for its antispasmodic properties and anti‐inflammatory effect (Anon., 2001). The efficacy and safety of Ze 185 for the treatment of somatoform disorders has been confirmed in a double‐blind, randomized, placebo‐controlled clinical study (Melzer, Schrader, Brattström, Schellenberg, & Saller, 2009). In addition, an open, randomized pilot study of the effect of Ze 185 in comparison with oxazepam was undertaken in patients with psychosomatic and psychovegetative disorders (Schellenberg, Sauer, & Brattström, 2004). Further, in a double‐blind, randomized controlled clinical trial, the reaction to exam anxiety in healthy subjects was studied (Steiner & Opwis, 2000). Recently, the anxiolytic properties of Ze 185 were confirmed in a psychosocial stress paradigm: the Trier social stress test (Meier et al., 2018). These clinical studies show that Ze 185 is a well‐tolerated herbal medicinal product in the respective indications.
The aim of the current retrospective case‐control study was to investigate the effect of Ze 185 on the prescription pattern of benzodiazepines in a population of hospitalized patients with psychiatric and somatoform disorders. Special focus was given to concomitant medications to investigate whether Ze 185 could substitute synthetic drugs.
2. MATERIAL AND METHODS
2.1. Study design and setting
In this single centre retrospective case‐control study, the electronic medical records of anonymized adult in‐patients (age >18 years) were analysed, who were treated at the Clienia private clinic Schlössli in Oetwil am See, Zurich, Switzerland. Patients were hospitalized between January 2, 2010 and May 15, 2013. The clinic is specialized in psychiatric, psychotherapeutic, and psychosomatic treatments. Besides standard therapy, patients are treated with complementary medicine, such as phytotherapy, acupuncture, biofeedback, and hypnosis.
2.2. Ethical approval
According to Swiss law, at the time of the investigation, an ethical approval by the responsible local ethics committee of the Canton of Zurich was not necessary for the retrospective analysis of anonymized patient data (KEK, 2010).
2.3. Drug of interest
Ze 185 (Relaxane®) was prescribed as film‐coated tablets, which contain the fixed combination of four dry extracts: 90 mg of a 90% (w/w) ethanolic extract of P. hybridus (L.) Gaertn., B. Mey. & Scherb roots (DER 7–14:1); 90 mg of a 45% (w/w) methanolic extract of V. officinalis L. roots (DER 4–6:1); 90 mg of a 50% (w/w) ethanolic extract of P. incarnata L. herb (DER 3–6:1); 60 mg of a 20% (w/w) ethanolic extract of M. officinalis L. leaves (DER 2.5–3.9:1; Fingerprint analysis see Figure 3). The fixed herbal drug combination is manufactured by Zeller Medical AG (CH‐8590 Romanshorn, Switzerland) and has been registered and marketed in Switzerland since 1970 for the treatment of nervousness, nervous tension, agitation, and exam anxiety. These ailments can, amongst others, lead to the following symptoms: spasmodic gastrointestinal complaints, increased irritability, occasional trouble falling asleep, and sleeping through the night. The recommended dose is one film‐coated tablet three times daily.
Figure 3.
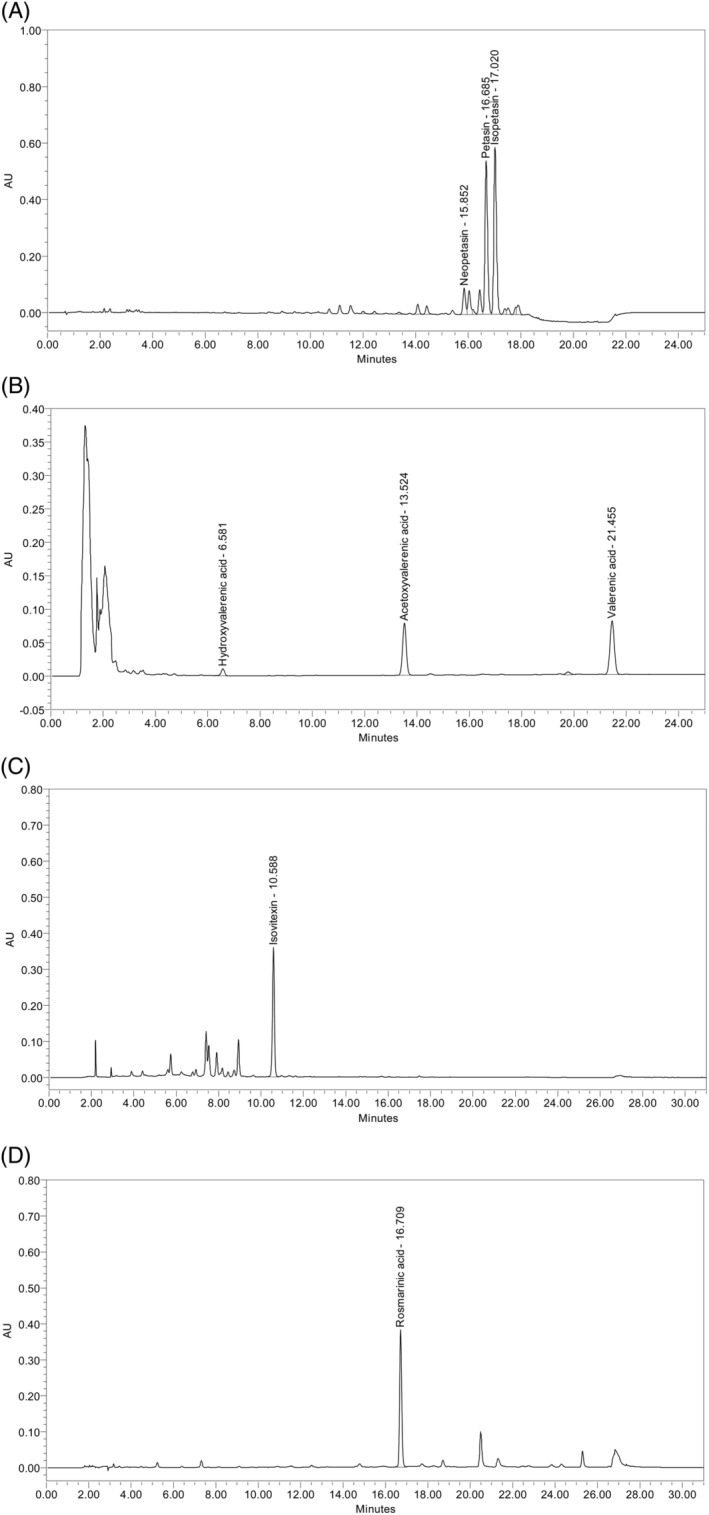
(a) High‐performance liquid chromatography (HPLC) fingerprint of P. hybridus dry extract performed with reversed phase HPLC (HPLC Waters H‐Class with PDA); stationary phase: C‐18 column (1.8 μm); mobile phase: gradient using acetonitrile, methanol and 0.1% solution of formic acid in water; UV‐detection at 243 nm. (b) HPLC fingerprint of valerian dry extract performed with reversed phase HPLC (HPLC 1100 Series Agilent); stationary phase: C‐18 column (5 μm); mobile phase: gradient using acetonitrile and 5 g/L solution of phosphoric acid in water; UV‐detection at 220 nm. (c) HPLC fingerprint of Passion flower dry extract performed with reversed phase HPLC (HPLC 1100 series Agilent); stationary phase: C‐18 column (3 μm) containing a C‐18 precolumn; mobile phase: gradient using 0.05 M phosphoric acid in water and acetonitrile; UV‐detection at 336 nm. (d) HPLC fingerprint of Melissa dry extract performed with reversed phase HPLC (HPLC 1100 series Agilent); stationary phase: C‐18 column (3 μm) containing a C‐18 precolumn; mobile phase: gradient using (A) 0.05 M phosphoric acid in water and acetonitrile; UV‐detection at 300 nm
2.4. Patient inclusion
Patients from all wards of the psychiatric clinic were included in the study. Therefore, cases and controls were selected for analysis by automatic identification from medical records using the Clinical Information System (CIS). Complete anonymization of the patient data was guaranteed for the analysis.
Cases: All patients were included in the analysis, if they were treated with any dose of Ze 185 on at least 1 day during their inpatient visit between January 2, 2010 and May 15, 2013. Controls: The control population without Ze 185 treatment was defined based on matching age (±5 years), gender, hospitalisation during the same interval (±6 months), and main International Classification of Diseases, Version 10 (ICD‐10) F‐diagnosis at the end of the clinical visit.
2.5. Study variables
The primary objective of the retrospective data analysis was to investigate the effect of Ze 185 on the prescription pattern of benzodiazepines in hospitalized patients with psychiatric disorders. The prescription pattern was investigated stratified by various primary F‐diagnoses according to ICD‐10 (WHO, 1992) at the end of the hospital stay.
The secondary objectives were to investigate (a) the effect of Ze 185 on the prescription pattern of other concomitantly prescribed drugs and (b) the effectiveness of the hospital stay in comparison with patients without Ze 185 treatment. This effectiveness was evaluated based on the Clinical Global Impression (CGI) score (Guy, 1976), the Global Assessment of Functioning (GAF) score (Hall, 1995), and selective symptoms of the “Association for Methodology and Documentation in Psychiatry” (AMDP) system (AMDP, 1982; AMDP‐CIPS, 1990). In the CGI score, higher values correspond to a condition with stronger severity and lower values to less severity. In the GAF score, lower value counts correspond to a less severe disease and higher values to a stronger severity. In the AMDP system, 140 items are counted to provide a psychopathological diagnosis. The single items of the AMDP system were scored on a 4‐point scale (0 = not at all, 1 = mild, 2 = moderate, and 3 = severe). For this retrospective data analysis, 11 items of the AMDP system were selected for detailed analysis. Four items from the category mental diagnosis (item 65 “anxious”; item 69 “restless”; item 82 “agitated”; item 83 “motor restlessness”) and seven items from the category somatic diagnosis (item 101 “initial insomnia”; item 102 “middle insomnia”; item 106 “decreased appetite”; item 119 “palpitations”; item 122 “sweating”; item 126 “diffuse pressure in head”; item 127 “back pain”) were chosen for further analysis.
The distribution of the drug classes was analysed using the WHO's anatomic‐therapeutic‐chemical classification system code with focus on medication with psychotropic activity.
As for safety, no data were reported in the CIS. Therefore, safety and tolerability of the patients' medication could not be evaluated.
2.6. Database structure
For the descriptive data analysis, medical records from the CIS were extracted to an Excel file. The information scientist of the clinic extracted and anonymized all patient data. For the anonymization, the patient information number was used by the information scientist to create a pseudo patient information number. Thus, a complete anonymization of the patient data was guaranteed for the data analyst.
2.7. Statistical analysis
Descriptive statistical analysis and all statistical tests used were performed using IBM SPSS Statistics for Windows, Version 21.0 (IBM Corp., Armonk, New York). The t test was used for normally distributed variables; otherwise, the Wilcoxon rank sum test was used. For the comparison of categorical variables, the Chi‐squared test was used. The default summary statistics for quantitative and ordinal variables were the number of observations (n), mean, standard deviation (SD), or median, as appropriate. For qualitative variables, the number and frequency of subjects with non‐missing data (n, %) per category were presented.
2.8. Study performance
This retrospective analysis was performed according to the checklist for observational studies (Strengthening the Reporting of Observational Studies in Epidemiology, STROBE; von Elm et al., 2007).
3. RESULTS
A total of 3,252 patients were included in the retrospective data analysis. Of these, 1,548 cases were treated with Ze 185, and 1,704 matched controls received regular medical treatment without Ze 185. Demographic characteristics are described in Table 1. A distribution of the patients' ages at entry is shown in Figure 1. In both groups, age and gender were equally distributed. The duration of the hospital stay was on average (mean ± SD) numerically comparable (n = 1,548 cases: 38.9 ± 29.6, range 1 to 205 days and n = 1,704 controls: 33.6 ± 29.4 days, range 1 to 185 days) but significantly different between the groups (p < .001).
Table 1.
Demographic characteristics
| Parameter | Casesa (n = 1,548) | Controlsb (n = 1,704) | Total (n = 3,252) | p‐value |
|---|---|---|---|---|
| Age (years), mean ± SD (median) | 45.4 ± 18.1 (44.0) | 44.6 ± 18.1 (43.0) | 45.2 ± 18.1 (43.0) | .390 |
| Sex (male/female) | 585/963 | 694/1010 | 1279/1973 | .087 |
| Duration of hospital stay (days), mean ± SD (median) | 38.9 ± 29.6 (33.0) | 33.6 ± 29.4 (26.0) | 36.1 ± 29.6 (29.0) | <.001 |
Receiving at least one prescription of Ze 185.
Receiving no prescription of Ze 185, matched to cases.
Figure 1.

Demographic distribution of patient's age at entry. Slight bimodal distribution of age could be observed (normal distribution is given for reference) [Colour figure can be viewed at wileyonlinelibrary.com]
3.1. F‐diagnoses
For the detailed analysis of F‐diagnoses, focus was on the primary F‐diagnoses according to ICD‐10 at the end of hospital stay (Figure 2). In the main categories of ICD‐10, the most frequent primary diagnosis was F3 “mood [affective] disorders” (cases n = 796; controls n = 866). The most frequent subcategories were F32 “depressive episodes” (cases n = 319; controls n = 357) and F33 “recurrent depressive disorders” (cases n = 424; controls n = 449). The second most frequent primary diagnosis was F1 “mental and behavioural disorders due to psychoactive substance use” (cases n = 278; controls n = 275). These patients were mainly diagnosed with the subcategory F10 “use of alcohol” (cases n = 134; controls n = 165). These categories were equally distributed between the groups. The results showed a statistically significant difference between the groups for the primary diagnoses F2 “schizophrenia, schizotypal and delusional disorders” (cases n = 101; controls n = 181; p < .001) and F4 “neurotic, stress‐related and somatoform disorders” (cases n = 185; controls n = 163; p = .028).
Figure 2.
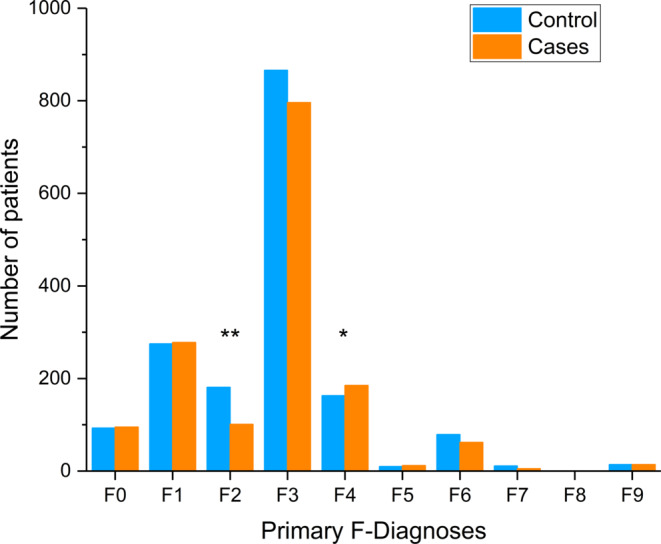
Distribution of primary F‐diagnoses according to International Classification of Diseases, Version 10. Number of patients within a group at the end of the hospital stay. Cases, n = 1,548: receiving at least one prescription of Ze 185, controls, n = 1,704: receiving no prescription of Ze 185, matched to cases; F0: Organic, including symptomatic, mental disorders; F1: Mental and behavioral disorders due to psychoactive substance use; F2: Schizophrenia, schizotypal, and delusional disorders; F3: Mood (affective) disorders; F4: Neurotic, stress‐related and somatoform disorders; F5: Behavioral syndromes associated with physiological disturbances and physical factors; F6: Disorders of adult personality and behavior; F7: Mental retardation; F8: Disorders of psychological development; F9: Behavioral and emotional disorders with onset usually occurring in childhood and adolescence, unspecified mental disorder. *p = .028, **p < .001 (Chi‐squared test) [Colour figure can be viewed at wileyonlinelibrary.com]
3.2. Symptom severity and effectiveness
At baseline, controls showed a numerically comparable (6.07 ± 0.72 vs. 6.02 ± 0.67, respectively) but significantly (p < .022) higher CGI score (=more severe symptoms) compared with cases. No significant differences between groups were observed for the GAF score. A significant treatment effect was seen in both groups (p < .001, each) in both the CGI and GAF scores at the end of hospital stay. However, numerically comparable (60.0 ± 15.3 vs. 61.2 ± 15.6, respectively) but significantly (p = .034) lower scores (=more severe symptoms) were seen for the GAF score in controls versus cases.
To evaluate the effectiveness of the hospital stay, the CGI score, GAF score, and selected items of the AMDP system were analysed. At the end of therapy, the CGI score was similar in both groups (cases 3.36 ± 0.91, n = 1,421; controls 3.40 ± 0.95, n = 1,551; p = .289) and showed a significant improvement in comparison with the beginning of the therapy (p < .001) in both groups.
The GAF score (mean ± SD) was similar in both groups at the beginning of the therapy (cases 48.4 ± 12.1, n = 1,488; controls 47.6 ± 12.5, n = 1,623; p = .088). At the end of therapy, cases and controls were statistically different but numerically comparable (cases 61.2 ± 15.6, n = 1,466; controls 60.0 ± 15.3, n = 1,623; p = .034). Importantly, in both groups, there was a significant improvement from baseline to the end of therapy (p < .001).
At the beginning of the therapy, selected items of the AMDP system (mean ± SD) were partially different between the groups. The item 65 “anxious”, item 69 “restless” and item 119 “palpitations” were significantly higher for cases (anxious: 0.85 ± 0.94, n = 1,065, p = .008; restless: 0.96 ± 0.96, n = 1,054, p = .011; palpitations: 0.19 ± 0.45, n = 903, p = .032) than for controls (anxious: 0.75 ± 0.94, n = 1,268; restless: 0.86 ± 0.96, n = 1,273; palpitations: 0.14 ± 0.45, n = 1,056). Furthermore, cases (agitated: 0.16 ± 0.61, n = 1,063) were significantly less agitated (item 82) than the controls (agitated: 0.22 ± 0.61, n = 1,281; p = .020). No significant differences were found between cases and controls at the beginning of the therapy for item 83: “motor restlessness” (cases 0.32 ± 0.71, n = 1,063; controls 0.33 ± 0.71, n = 1,281; p = .853); item 101: “initial insomnia” (cases 1.11 ± 0.99, n = 936; controls 1.03 ± 0.99, n = 1,086; p = .078), item 102: “middle insomnia” (cases 1.17 ± 1.02, n = 934; controls 1.10 ± 1.02, n = 1,088; p = .155); item 106: “decreased appetite” (cases 0.81 ± 0.97, n = 929; controls 0.78 ± 0.97, n = 1,080; p = .520); item 122: “sweating” (cases 0.13 ± 0.49, n = 897; controls 0.15 ± 0.49, n = 1,052; p = .399); item 126: “diffuse pressure in head” (cases 0.20 ± 0.59, n = 905; controls 0.23 ± 0.59, n = 1,061; p = .153); and item 127: “back pain” (cases 0.25 ± 0.71, n = 911; controls 0.28 ± 0.71, n = 1,066; p = .278).
At the end of treatment, three items were significantly different when comparing cases and controls: item 101 “initial insomnia” (cases 0.41 ± 0.64, n = 824; controls 0.35 ± 0.59, n = 893, p = .046), item 102 “middle insomnia” (cases 0.40 ± 0.67, n = 825; controls 0.34 ± 0.60, n = 892, p = .026), and item 119 “palpitations” (cases 0.08 ± 0.29 n = 799; controls 0.05 ± 0.25, n = 878, p = .014). No significant differences were found between cases and controls at the end of the therapy for item 65 “anxious” (cases 0.49 ± 0.74, n = 935; controls 0.44 ± 0.67, n = 1,027, p = .086), item 69 “restless” (cases 0.52 ± 0.73, n = 933; controls 0.50 ± 0.72, n = 1,023; p = .582), item 82 “agitated” (cases 0.10 ± 0.39, n = 935; controls 0.11 ± 0.40, n = 1,028; p = .609), item 83 “motor restlessness” (cases 0.16 ± 0.47, n = 935; controls 0.17 ± 0.49, n = 1,029; p = .671), item 106 “decreased appetite” (cases 0.18 ± 0.48, n = 812; controls 0.21 ± 0.52, n = 888; p = .177), item 122 “sweating” (cases 0.08 ± 0.34, n = 801; controls 0.06 ± 0.30, n = 878; p = .275), item 126 “diffuse pressure in head” (cases 0.09 ± 0.32, n = 798; controls 0.10 ± 0.36, n = 880; p = .758), and item 127 “back pain” (cases 0.12 ± 0.42, n = 798; controls 0.16 ± 0.52, n = 881; p = .105).
Importantly, in both treatment groups, each AMDP‐item improved significantly from baseline to the end of treatment (p < .001).
3.3. Concomitant medication
Cases and controls received a plethora of concomitant medications. Therefore, the population was analysed for differences between the groups. Based on the indication of Ze 185, special focus was put on medications with psychotropic activity. The numbers of prescriptions of anxiolytics (especially benzodiazepines), hypnotics/sedatives, and antidepressants were significantly different between cases and controls (Table 2).
Table 2.
Overview of prescribed medication in “cases” with Ze 185 and “controls” by ATC code in the drug class N, Nervous system
| Drug class by ATC code | Cases Ze 185 (n = 1,548) | Controls (n = 1,704) | Total (n = 3,252) | p‐value |
|---|---|---|---|---|
| N02: Analgesics | 571 | 593 | 1,164 | .215 |
| N02A: Opioids | 60 | 104 | 164 | .004 |
| N02B: Other analgesics and antipyretics | 530 | 533 | 1,063 | .072 |
| N02C: Antimigraine preparations | 29 | 27 | 56 | .527 |
| N03: Antiepileptics | 248 | 289 | 537 | .471 |
| N03A: Antiepileptics | 248 | 289 | 537 | .471 |
| N04: Anti‐Parkinson drugs | 71 | 97 | 168 | .155 |
| N04A: Anticholinergic agents | 60 | 79 | 139 | .284 |
| N04B: Dopaminergic agents | 11 | 20 | 31 | .175 |
| N05: Psycholeptics | 1,548 | 1,452 | 3,000 | <.001 |
| N05A: Antipsychotics | 900 | 1,035 | 1935 | .131 |
| N05B: Anxiolytics | 655 | 809 | 1,464 | .003 |
| N05BA: Benzodiazepine derivatives | 655 | 808 | 1,463 | .003 |
| N05C: Hypnotics and sedatives | 940 | 603 | 1,543 | <.001 |
| N05CA: Barbiturates, plain | 0 | 0 | 0 | NA |
| N05CB: Barbiturates, combination | 0 | 0 | 0 | NA |
| N05CC: Aldehydes and derivatives | 10 | 23 | 33 | .046 |
| N05CD: Benzodiazepine derivatives | 9 | 5 | 14 | .210 |
| N05 CE: Piperidinedione derivatives | 0 | 0 | 0 | NA |
| N05CF: Benzodiazepine related drugs | 133 | 174 | 304 | .115 |
| N05CH: Melatonin receptor agonists | 0 | 0 | 0 | NA |
| N05CM: Other hypnotics and sedatives | 60 | 71 | 131 | .674 |
| N05CP: Herbal hypnotics and sedatives | 0 | 0 | 0 | NA |
| N05CX: Hypnotics and sedatives, combination excl. Barbiturates | 1,548 | 415 | 1963 | <.001 |
| N05CX99: Valerian/hops extract (Ze 91019) | 784 | 444 | 1,228 | <.001 |
|
N05BA or N05CD benzodiazepine derivatives (total benzodiazepine) |
661 | 809 | 1,470 | .006 |
| N06: Psychoanaleptics | 1,160 | 1,150 | 2,310 | <.001 |
| N06A: Antidepressants | 1,135 | 1,114 | 2,249 | <.001 |
| N06AA: Non‐selective monoamine reuptake inhibitors | 122 | 131 | 253 | .837 |
| N06AA06: Trimipramin | 63 | 63 | 126 | .582 |
| N06AB: Selective serotonin reuptake inhibitors | 496 | 439 | 935 | <.001 |
| N06AF: Monoamine oxidase inhibitors, non‐selective | 0 | 0 | 0 | NA |
| N06AG: Monoamine oxidase A inhibitors | 4 | 4 | 4 | .892 |
| N06AX: Other antidepressants | 778 | 772 | 1,550 | .005 |
| N06AX05: Trazodone | 353 | 320 | 673 | .005 |
| N06AX11: Mirtazapine | 190 | 173 | 363 | .055 |
| N06AX25: Hypericum | 50 | 29 | 79 | .005 |
Note: Only drug classes or individual active substances for the most relevant medications with a high prevalence in patients with psychiatric disorders are depicted.
Abbreviations: ATC, anatomic‐therapeutic‐chemical; NA = not applicable.
Significantly less cases than controls received prescriptions of benzodiazepines (cases n = 661, controls n = 809; p = .006). The number of patients with prescribed hypnotics/sedatives was significantly higher for cases than controls (cases n = 940, controls n = 603; p < .001). In the group of hypnotics/sedatives, the main differences were seen for a specific valerian/hops extract (Ze 91019). Significantly more cases than controls received a prescription of this fixed extract combination (cases n = 784, controls n = 444; p < .001). The number of patients receiving antidepressant prescriptions was also significantly increased among cases compared with controls (cases n = 1,135, controls n = 1,114; p < .001). Of these, 496 cases and 439 controls received a prescription of selective serotonin reuptake inhibitors (p < .001). Significantly more cases than controls received prescriptions of other antidepressants (cases n = 778, controls n = 772; p = .005) including Hypericum extract (cases n = 50, controls n = 29; p = .005).
4. DISCUSSION
The number of prescriptions of benzodiazepines has considerably increased over the past decades (Agarwal & Landon, 2019; Kaufmann, Spira, Alexander, Rutkow, & Mojtabai, 2016; Verthein, Buth, Holzbach, Neumann‐Runde, & Martens, 2019). This development is giving cause for concern because of the increased risk of related adverse drug reactions posing a significant public health problem (Del Giorno, Ceschi, & Gabutti, 2017). It was concluded that understanding and addressing prescription patterns may help curb the growing use of benzodiazepines (Agarwal & Landon, 2019).
This retrospective case‐control study investigated, among other aspects, the prescriptions and use of benzodiazepines in 3,252 psychiatric patients. Our data showed that both treatment modalities for cases and controls had a comparable clinical effectiveness as indicated by CGI, GAF, and AMDP scores. Cases received significantly less prescriptions of benzodiazepine (p = .006) but, on the other hand, more prescriptions of hypnotics (in particular valerian/hops extract).
The demographic characteristics were similar in cases and controls. Due to the high number of patients in the case and control groups, there were small differences, which turned out to be statistically significant (e.g., for duration of hospital stay and baseline CGI score). However, these differences are probably clinically irrelevant.
In both groups, the hospital stay and the associated treatment modalities were comparably effective. This is shown by the CGI and GAF scores and selected items of the AMDP system improving significantly and comparably by the end of hospital stay. Due to the database structure of the CIS, safety relevant data could not be surveyed. Because no suspected adverse drug reactions related to the intake of Ze 185 in the period of the study were reported to the pharmacovigilance department of the marketing authorization holder of Ze 185, it may be assumed that no relevant adverse drug reactions occurred.
Most primary diagnoses were equally distributed among study subjects. However, the F2‐diagnosis (“schizophrenia, schizotypal and delusional disorders”) was statistically more prevalent in the control group. The F4‐diagnosis (“neurotic, stress‐related and somatoform disorders”) was more often diagnosed in cases. Ze 185 is not indicated in schizophrenia and associated disorders but instead for the treatment of symptoms of stress‐related and somatoform disorders. This reflects the current medicinal use of Ze 185, and thus, the data are compatible with the authorized indication. In both groups, only a limited number of patients were diagnosed. A larger number of patients would allow more definite conclusions to be drawn.
Most patients had a primary F3‐diagnosis such as F32 (“depressive episodes”) and F33 (“recurrent depressive disorders”). Depression is often associated with anxiety and somatoform disorders. This is also reflected in the study population as the second most frequent diagnosis belonged to the category F4 “neurotic, stress‐related and somatoform disorders”. Ze 185 is effective in the treatment of depression and anxiety in patients with somatoform disorders (Melzer et al., 2009). As approved by the Swiss Agency for Therapeutic Products (Swissmedic), Ze 185 is indicated for the treatment of the following complaints: nervousness, tension, restlessness, and exam anxiety, leading to symptoms such as spasmodic gastrointestinal complaints, increased irritability, occasional trouble falling asleep, and sleeping through the night. Similar symptoms such as “reduced concentration,” “disturbed sleep,” and “somatic symptoms such as agitation” are also described in the F32‐ and F33‐diagnoses. Therefore, the prescription pattern of Ze 185 reflected the authorized indication very well.
In addition to Ze 185, cases received prescriptions of other concomitant medications for the treatment of their symptoms. Focussing on psychoactive drugs influencing the nervous system, a difference in the number of prescriptions of benzodiazepines, hypnotics, and antidepressants was found. Because less patients received concomitant prescriptions of benzodiazepines among the cases compared with controls, this may suggest that Ze 185 could be a viable option to substitute benzodiazepines in patients suffering from depression and anxiety symptoms. However, to substantiate this hypothesis, a direct comparison study between benzodiazepines and Ze 185 would be necessary.
More cases than controls received prescriptions of hypnotics and antidepressants. The most frequently prescribed hypnotic was a specific valerian/hops extract. Selective serotonin reuptake inhibitors or other antidepressants, including St. John's wort, were also more often prescribed for cases. It seemed that cases being prescribed Ze 185 also had an overall higher rate of prescription for other herbal medicinal drugs. This may partially reflect the good tolerability profile and sufficient efficacy of these drugs. On the other hand, personal preferences of the patients and/or the prescribing physicians could not be excluded.
4.1. Strengths and limitations
Randomized, controlled clinical trials (RCT) are regarded as providing the highest evidence of proving treatment effects in evidence‐based medicine. These studies possess a high internal validity as the investigator controls for all possible confounding effects. Observational studies (cross‐sectional or case‐control studies), however, have a higher external validity, because data are observed unbiased by protocol restrictions (Carlson & Morrison, 2009). As Vandenbroucke (Vandenbroucke, 2011) pointed out in an editorial, there are four meta‐analyses contrasting RCTs and observational studies of treatments that found no large differences between the study types (Benson & Hartz, 2000; Concato, Shah, & Horwitz, 2000; Ioannidis et al., 2001; MacLehose et al., 2000).
The strength of this retrospective, case‐control study is the availability of a large sample (number of patients) and the possibility of investigating prescription patterns as it occurs in routine clinical care, therefore, providing real world evidence. The hospital has a defined public service mandate from the Canton Zurich (Zurich County, 250,000 inhabitants) and covers all levels of psychiatric diagnoses and care. Limitations are, of course, the different treatment durations and the polypharmacy of the patients. However, the polypharmacy also provided the basis for the detailed analysis of concomitant medication. Patient data from only one clinic were analysed. Characteristics of cases and controls were slightly different at baseline. Differences in the number of cases and controls between baseline and end of therapy in CGI, GAF, and AMDP items are due to missing data, which is a general limitation of retrospective studies (real world data) (Katkade, Sanders, & Zou, 2018). A multicentre study would have provided a broader picture. Therefore, with regard to effectiveness, only hypotheses on the therapeutic setting can be generated. There might be a confounding bias due to the patients' and/or physicians' preferences regarding the uses of benzodiazepines or herbal drugs that influenced the prescription pattern. Neither a causal relationship between Ze 185 and the reduction of benzodiazepine prescriptions nor a better tolerability could be inferred, due to the CIS database lacking detailed adverse event monitoring.
5. CONCLUSION
The broad indication of Ze 185 covers the treatment of stress‐related complaints, such as nervousness, nervous tension, agitation, and anxiousness. Patients with these symptoms are often treated with benzodiazepines. The data in the present retrospective case‐control study have certain limitations but provide some evidence that a treatment modality including Ze 185 could reduce the need for benzodiazepines. This is of general clinical interest and relevance as benzodiazepines are under ongoing discussion due to their problematic safety profile. However, to obtain a solid answer for this hypothesis, a dedicated randomized, controlled clinical trial closely monitoring drug safety is needed.
CONFLICT OF INTEREST
MK and KS were employees of the Clienia Private Clinic Schlössli. SN, CB, CZ, and JD are/were employees of Max Zeller Söhne AG and supported the analysis of the data and the preparation of manuscript on the basis of mutual scientific agreement with MK and KS. As such, the employees confirm no bias to the publication.
AUTHOR CONTRIBUTIONS
MK was involved in supervision, study design, data interpretation, and manuscript preparation. KS contributed to data collection and analysis. SN and CB were involved in the manuscript preparation and data interpretation. JD and CZ contributed to study design, data analysis, manuscript preparation, and revision.
ACKNOWLEDGMENT
This study was conducted as investigator‐initiated research. There was no funding by the manufacturers of the investigated herbal medicinal products or other mentioned central nervous system drugs.
Keck ME, Nicolussi S, Spura K, Blohm C, Zahner C, Drewe J. Effect of the fixed combination of valerian, lemon balm, passionflower, and butterbur extracts (Ze 185) on the prescription pattern of benzodiazepines in hospitalized psychiatric patients—A retrospective case‐control investigation. Phytotherapy Research. 2020;34:1436–1445. 10.1002/ptr.6618
REFERENCES
- Agarwal, S. D. , & Landon, B. E. (2019). Patterns in outpatient benzodiazepine prescribing in the United States. JAMA Network Open, 2(1), e187399 10.1001/jamanetworkopen.2018.7399 [DOI] [PMC free article] [PubMed] [Google Scholar]
- AMDP . (1982). The AMDP‐system. Manual for the assessment and documentation of psychopathology. Arbeitsgemeinschaft für Methodik und Dokumentation in der Psychiatrie [AMDP] Berlin: Springer. [Google Scholar]
- AMDP‐CIPS . (1990). Rating scales for psychiatry. European Edition. Weinheim: Beltz Test GmbH.
- Anon. (2001). Monograph. Petasites hybridus . Alternative Medicine Review, 6(2), 207–209. [PubMed] [Google Scholar]
- Benson, K. , & Hartz, A. J. (2000). A comparison of observational studies and randomized, controlled trials. The New England Journal of Medicine, 342(25), 1878–1886. 10.1056/NEJM200006223422506 [DOI] [PubMed] [Google Scholar]
- Carlson, M. D. , & Morrison, R. S. (2009). Study design, precision, and validity in observational studies. Journal of Palliative Medicine, 12(1), 77–82. 10.1089/jpm.2008.9690 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Concato, J. , Shah, N. , & Horwitz, R. I. (2000). Randomized, controlled trials, observational studies, and the hierarchy of research designs. The New England Journal of Medicine, 342(25), 1887–1892. 10.1056/NEJM200006223422507 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Del Giorno, R. , Ceschi, A. , & Gabutti, L. (2017). Benzodiazepines in elderly patients: The dark side of a magic pill. Revue Médicale Suisse, 13(547), 282–284. [PubMed] [Google Scholar]
- Donnelly, K. , Bracchi, R. , Hewitt, J. , Routledge, P. A. , & Carter, B. (2017). Benzodiazepines, Z‐drugs and the risk of hip fracture: A systematic review and meta‐analysis. PLoS One, 12(4), e0174730 10.1371/journal.pone.0174730 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EMA/HMPC . (2013). Community herbal monograph on Melissa officinalis L., folium. EMA/HMPC/196745/2012.
- EMA/HMPC . (2014). Community herbal monograph on Passiflora incarnata L., herba. EMA/HMPC/669740/2013.
- EMA/HMPC . (2016). European Union herbal monograph on Valeriana officinalis L., radix EMA/HMPC/150848/2015 Corr
- Finkle, W. D. , Der, J. S. , Greenland, S. , Adams, J. L. , Ridgeway, G. , Blaschke, T. , … VanRiper, K. B. (2011). Risk of fractures requiring hospitalization after an initial prescription for zolpidem, alprazolam, lorazepam, or diazepam in older adults. Journal of the American Geriatrics Society, 59(10), 1883–1890. 10.1111/j.1532-5415.2011.03591.x [DOI] [PubMed] [Google Scholar]
- Gerlach, L. B. , Maust, D. T. , Leong, S. H. , Mavandadi, S. , & Oslin, D. W. (2018). Factors associated with long‐term benzodiazepine use among older adults. JAMA Internal Medicine, 178(11), 1560–1562. 10.1001/jamainternmed.2018.2413 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guy, W. (1976). ECDEU assessment manual for psychopharmacology—Revised (DHHS Publ No. ADM 91‐338), U.S Department of Health and Human Services; Rockville, MD. [Google Scholar]
- Hall, R. C. (1995). Global assessment of functioning. A modified scale. Psychosomatics, 36(3), 267–275. 10.1016/S0033-3182(95)71666-8 [DOI] [PubMed] [Google Scholar]
- Ioannidis, J. P. , Haidich, A. B. , Pappa, M. , Pantazis, N. , Kokori, S. I. , Tektonidou, M. G. , … Lau, J. (2001). Comparison of evidence of treatment effects in randomized and nonrandomized studies. JAMA, 286(7), 821–830. 10.1001/jama.286.7.821 [DOI] [PubMed] [Google Scholar]
- Johnson, B. , & Streltzer, J. (2013). Risks associated with long‐term benzodiazepine use. American Family Physician, 88(4), 224–226. [PubMed] [Google Scholar]
- Katkade, V. B. , Sanders, K. N. , & Zou, K. H. (2018). Real world data: An opportunity to supplement existing evidence for the use of long‐established medicines in health care decision making. Journal of Multidisciplinary Healthcare, 11, 295–304. 10.2147/JMDH.S160029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaufmann, C. N. , Spira, A. P. , Alexander, G. C. , Rutkow, L. , & Mojtabai, R. (2016). Trends in prescribing of sedative‐hypnotic medications in the USA: 1993‐2010. Pharmacoepidemiology and Drug Safety, 25(6), 637–645. 10.1002/pds.3951 [DOI] [PMC free article] [PubMed] [Google Scholar]
- KEK . (2010). [Guideline for the submission of research applications of the cantonal ethics committee of Zürich]. Wegleitung für die Einreichung eines Forschungsgesuches an die Kantonale Ethikkommission Zürich (Version 01.072010): Kantonale Ethik‐Kommission Zürich (KEK).
- Klein, S. D. , Torchetti, L. , Frei‐Erb, M. , & Wolf, U. (2015). Usage of complementary medicine in Switzerland: Results of the Swiss health survey 2012 and development since 2007. PLoS One, 10(10), e0141985 10.1371/journal.pone.0141985 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lalive, A. L. , Rudolph, U. , Luscher, C. , & Tan, K. R. (2011). Is there a way to curb benzodiazepine addiction? Swiss Medical Weekly, 141, w13277 10.4414/smw.2011.13277 [DOI] [PubMed] [Google Scholar]
- MacLehose, R. R. , Reeves, B. C. , Harvey, I. M. , Sheldon, T. A. , Russell, I. T. , & Black, A. M. (2000). A systematic review of comparisons of effect sizes derived from randomised and non‐randomised studies. Health Technology Assessment, 4(34), 1–154. 10.3310/hta4340 [DOI] [PubMed] [Google Scholar]
- Meier, S. , Haschke, M. , Zahner, C. , Kruttschnitt, E. , Drewe, J. , Liakoni, E. , … Gaab, J. (2018). Effects of a fixed herbal drug combination (Ze 185) to an experimental acute stress setting in healthy men—An explorative randomized placebo‐controlled double‐blind study. Phytomedicine, 39, 85–92. 10.1016/j.phymed.2017.12.005 [DOI] [PubMed] [Google Scholar]
- Melzer, J. , Schrader, E. , Brattstrom, A. , Schellenberg, R. , & Saller, R. (2009). Fixed herbal drug combination with and without butterbur (Ze 185) for the treatment of patients with somatoform disorders: Randomized, placebo‐controlled pharmaco‐clinical trial. Phytotherapy Research, 23(9), 1303–1308. 10.1002/ptr.2771 [DOI] [PubMed] [Google Scholar]
- Palmaro, A. , Dupouy, J. , & Lapeyre‐Mestre, M. (2015). Benzodiazepines and risk of death: Results from two large cohort studies in France and UK. European Neuropsychopharmacology, 25(10), 1566–1577. 10.1016/j.euroneuro.2015.07.006 [DOI] [PubMed] [Google Scholar]
- Patorno, E. , Glynn, R. J. , Levin, R. , Lee, M. P. , & Huybrechts, K. F. (2017). Benzodiazepines and risk of all cause mortality in adults: Cohort study. BMJ, 358, j2941 10.1136/bmj.j2941 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schellenberg, R. , Sauer, S. , & Brattström, A. (2004). Vegetable daytranquilizer Ze 185* and oxazepam in the clinical and neurophysiological comparison by patients with psychovegetative complaint. Zeitschrift für Phytotherapie, 25, 289–295. [Google Scholar]
- Steiner, G. , & Opwis, K. (2000). Wirkung von Relax auf Angst und kognitive Leistungsfähigkeit Eine plazebokontrollierte Doppelblindstudie. Ars Medici, 25/26, 1564–1567. [Google Scholar]
- Tinguely, G. , Landolt, H. P. , & Cajochen, C. (2014). Sleep habits, sleep quality and sleep medicine use of the Swiss population result. Therapeutische Umschau, 71(11), 637–646. 10.1024/0040-5930/a000604 [DOI] [PubMed] [Google Scholar]
- Vandenbroucke, J. P. (2011). Why do the results of randomised and observational studies differ? BMJ, 343, d7020 10.1136/bmj.d7020 [DOI] [PubMed] [Google Scholar]
- Verthein, U. , Buth, S. , Holzbach, R. , Neumann‐Runde, E. , & Martens, M. S. (2019). Benzodiazepines and Z‐drugs—Analyses of ambulatory prescriptions from 2006 to 2015. Benzodiazepine und Z‐substanzen—Analyse der kassenärztlichen Verschreibungen von 2006 bis 2015. Psychiatrische Praxis, 46(7), 399–405. 10.1055/a-0961-2371 [DOI] [PubMed] [Google Scholar]
- von Elm, E. , Altman, D. G. , Egger, M. , Pocock, S. J. , Gotzsche, P. C. , Vandenbroucke, J. P. , & Initiative, S. (2007). Strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ, 335(7624), 806–808. 10.1136/bmj.39335.541782.AD [DOI] [PMC free article] [PubMed] [Google Scholar]
- WHO . (1992). ICD‐10: International statistical classification of diseases and related health problems (10th ed.). Geneva: World Health Organisation. [Google Scholar]
- Woods, J. H. , Katz, J. L. , & Winger, G. (1992). Benzodiazepines: Use, abuse, and consequences. Pharmacol Rev, 44(2), 151–347. [PubMed] [Google Scholar]