

Abstract
Background
Anxiety and depressive disorders can be classified under a bidimensional model, where depression and generalized anxiety disorder are represented by distress and the other anxiety disorders, by fear. The phenotypic structure of this model has been validated, but twin studies only show partial evidence for genetic and environmental distinctions between distress and fear. Moreover, the effects of genetic variants are mostly shared between anxiety and depression, but the genome‐wide genetic distinction between distress and fear remains unexplored. This study aimed to examine the degree of common genetic variation overlap between distress and fear, and their associations with the psychosocial risk factors of loneliness and social isolation.
Methods
We used genome‐wide data from 157,366 individuals in the UK Biobank who answered a mental health questionnaire.
Results
Genetic correlations indicated that depression and generalized anxiety had a substantial genetic overlap, and that they were genetically partially distinct from fear disorders. Associations with loneliness, but not social isolation, showed that loneliness was more strongly associated with both distress disorders than with fear.
Conclusions
Our findings shed light on genetic and environmental mechanisms that are common and unique to distress and fear and contribute to current knowledge on individuals’ susceptibility to anxiety and depression.
Keywords: anxiety, depression, genetics, loneliness, social isolation
1. INTRODUCTION
Anxiety and depressive disorders are the leading mental health problems contributing to the world disability burden (Kessler et al., 2009). Both groups of disorders have heterogeneous symptoms and frequently co‐occur, calling their distinction into question (APA, 2013). One proposed solution to this question is a bidimensional hierarchical structure of distress and fear (Krueger, 1999; Watson, 2005). Preliminary evidence for this model comes from the findings that depression is more often comorbid with generalized anxiety disorder than with other anxiety disorders, and that depression and generalized anxiety share a core component of negative affect symptoms (Mineka, Watson, & Clark, 1998). As a result, depression and generalized anxiety have been characterized as distress disorders. The other anxiety disorders, social anxiety, agoraphobia, specific phobia, and panic disorder have consequently been classified under a fear dimension. The phenotypic structure of this model has been validated at both the symptom and disorder levels (Slade & Watson, 2006; Vollebergh et al., 2001). However, to fully explore this proposed structure, it is necessary to understand the etiological mechanisms underlying both dimensions of distress and fear. One approach to validating this model is to examine the extent to which genetic and environmental factors are shared both within and across these dimensions.
1.1. Genetic structure of distress and fear
Anxiety and depressive disorders are influenced by genetic factors (Craske et al., 2017; Sullivan, Neale, & Kendler, 2000). Previous twin studies showed partial evidence for a genetic structure supporting the distress and fear model (Kendler, Prescott, Myers, & Neale, 2003; Waszczuk, Zavos, Gregory, & Eley, 2014). This support mainly comes from two findings. The first is that generalized anxiety and depression have a substantial genetic overlap, suggesting that distress disorders have a common genetic vulnerability (Kendler, Neale, Kessler, Heath, & Eaves, 1992; Roy, Neale, Pedersen, Mathé, & Kendler, 1995). The second is that disorders across the distress and fear dimensions are partly genetically distinguishable (Kendler et al., 2003; Waszczuk et al., 2014). Therefore, each dimension has specific genetic influences. However, genetic findings from twin studies do not entirely support the distress and fear model. Notably, fear disorders such as panic disorder and agoraphobia share some genetic risk with distress disorders (Hettema, Prescott, Myers, Neale, & Kendler, 2005; Kendler et al., 2003). Also, the genetic links among fear disorders remain unclear, with some studies indicating common genetic influences and others suggesting disorder‐specific genetic effects (Eley, Rijsdijk, Perrin, O'Connor, & Bolton, 2008; Loken, Hettema, Aggen, & Kendler, 2014; Silberg, Rutter, & Eaves, 2001; Waszczuk et al., 2014). In sum, twin studies only partially support the distress and fear model from a genetic perspective.
One limit of twin studies is that they do not identify the specific genetic variants involved. Genome‐wide association studies (GWAS) explore common genetic variation across the whole genome, enabling identification of associations between specific genetic variants and disorders. Studies using this approach are beginning to show that common genetic variants (single‐nucleotide polymorphism; SNP) account for individual differences in depression and anxiety. Findings indicate that SNP‐based heritability of anxiety and depression varies between 0.10 and 0.30 (Howard et al., 2019; Meier et al., 2019; Otowa et al., 2016; Purves et al., 2019; Wray et al., 2018). SNP heritability is one way to show the cumulative contribution of a subset of SNPs to a trait's total heritability (Bulik‐Sullivan, Loh et al., 2015). These recent GWAS also showed that these SNPs were located at various regions on the genome. Therefore, the cumulative effect of these SNPs partially explains individual differences in anxiety and depression. Of more relevance to the current question are findings of genome‐wide genetic correlations showing considerable overlap in genome‐wide SNPs linked to anxiety and depression. Correlation estimates range between 0.60 and 0.80 (Anttila et al., 2018; Meier et al., 2019; Purves et al., 2019). However, these genome‐wide genetic correlations were based on general measures of anxiety and to date, such correlation between generalized anxiety and the fear disorders remain unexplored. Therefore, no study has yet examined common genetic variation with regard to understanding the relationship between distress and fear dimensions.
1.2. Environmental structure of distress and fear
In addition to genetic influences, twin studies have also identified substantial environmental contributions to anxiety and depressive disorders (Eley et al., 2008; Kendler et al., 2003; Loken et al., 2014; Roy et al., 1995; Silberg et al., 2001; Waszczuk et al., 2014). However, in line with genetic findings from twin studies, their findings are equivocal with respect to defining the underlying etiology of the distress and fear model. Furthermore, twin studies did not allow identifying specific aspects of the environment that may contribute to anxiety and depression.
One way to further explore the role of the environment in the structure of distress and fear is to investigate associations with specific types of psychosocial stress. Two factors reflecting psychosocial stress that have recently been associated with several health issues, including anxiety and depression, are loneliness and social isolation (Baselmans et al., 2019; Beutel et al., 2017; Holt‐Lunstad, Smith, Baker, Harris, & Stephenson, 2015; Hyland et al., 2018; Luo, Hawkley, Waite, & Cacioppo, 2012). Loneliness is the subjective feeling of a dissatisfaction with actual and desired social interactions (Ernst & Cacioppo, 1999), and social isolation is the objective lack of social interactions (Coyle & Dugan, 2012). With respect to their role in clarifying the distress and fear model, loneliness may be common to distress disorders since it is associated with both depression and generalized anxiety (Beutel et al., 2017; Hyland et al., 2018). However, loneliness has also been linked to panic attacks (Beutel et al., 2017). Therefore, its role in distinguishing distress from fear is unclear. Furthermore, there is currently conflicting evidence as to whether social isolation is associated with anxiety and depression. Some studies suggest that it is associated with social anxiety and depression (Schwarzbach, Luppa, Forstmeier, König, & Riedel‐Heller, 2014; Teo, Lerrigo, & Rogers, 2013), whereas others found no such association (Coyle & Dugan, 2012; Steptoe, Shankar, Demakakos, & Wardle, 2013). At present, we do not know whether loneliness and social isolation have independent relationships with distress and fear disorders since no study has yet examined and compared their respective associations with all anxiety and depressive disorders.
1.3. Objectives of the study
The aim of this study was to verify the distress and fear model by investigating specific genetic and environmental factors on depression and generalized anxiety disorder (distress), and all other anxiety disorders (fear). The first objective was to examine genome‐wide genetic overlap among distress disorders, and then to see whether this genetic risk was distinct from that on fear disorders. The second objective was to investigate the extent to which associations with loneliness and social isolation supported this hierarchical structure.
2. MATERIALS AND METHODS
2.1. Participants
Participants were from the UK Biobank, a large nation‐wide study documenting general health and illness of more than 500,000 adults aged 40–69 years at recruitment (see Sudlow et al., 2015 for more details on sample and recruitment). This study included a subset of 157,366 participants who completed a mental health follow‐up questionnaire approximately 6–8 years after recruitment (see Davis et al., 2018 for a description of this questionnaire).
2.2. Measurements
2.2.1. Anxiety and depressive disorders
Participants were separated into cases and controls for all disorders.
Disorder diagnoses for depression and generalized anxiety were derived from the definition from Davis et al. (2018). Cases met probable lifetime criteria based on questions from the Composite International Diagnostic Interview short‐form (Kessler, Andrews, Mroczek, Ustun, & Wittchen, 1998). Controls did not meet these criteria and were excluded if they reported taking antidepressant medication.
To assess all other anxiety disorders, participants answered the following question: Have you been diagnosed with one or more of the following mental health problems by a professional, even if you don't have it currently? Fear cases were participants who had been diagnosed with at least one of these disorders: social anxiety, agoraphobia, specific phobia, or panic. This combination allowed us (a) to distinguish the fear disorders from generalized anxiety and (b) to have sufficient statistical power to perform genomic analyses. The number of cases for each fear disorder was not large enough to examine each one separately. When participants did not report any diagnosis and did not report taking antidepressant medication, they were considered controls.
2.2.2. Loneliness and social isolation
Participants were considered lonely if they answered “Yes” to the following question: Do you often feel lonely? They were socially isolated if they were living alone, did not attend a social activity once a week or more often, and/or had friends or family visit them once every few months or less. Both scales were comparable to previously used validated evaluations (e.g., Hughes, Waite, Hawkley, & Cacioppo, 2004; Tanskanen & Anttila, 2016). More details on these measures are provided in the Supplementary material.
2.2.3. Genetic data
Genome‐wide genotyping and imputation for the UK Biobank are described in Bycroft et al. (2018). Quality control procedures were applied to the genetic data and are described in Coleman et al. (2019). SNPs that were genotyped or imputed from the reference panel of the Haplotype Reference Consortium with an INFO score greater than 0.4, and which had a minor allele frequency greater than 0.01 were included in the analyses. Individuals with gender discordant genetic information, unusual missingness, or heterozygosity, or who were up to third‐degree relatives and closer were not included. The final sample included individuals of White Western European ancestry to limit population structure confounding.
2.3. Analytical approach
We first verified the phenotypic structure of the distress and fear model by conducting two sets of correlational analyses in R 3.3.3 (R Core Team, 2017). First, we conducted tetrachoric correlations between depression, generalized anxiety, and fear. Then, disorders were regressed on each other, one at a time, to isolate unique parts of variance (see Table 1 for a description of all phenotypes). We conducted partial correlations using residual phenotypes to examine unique associations between pairs of disorders.
Table 1.
Phenotype variables
| Initial phenotypes | Residual phenotypes a | ||
|---|---|---|---|
| Depression | Depression‐(GAD) | Depression‐(fear) | Depression‐(GAD + fear) |
| GAD | GAD‐(depression) | GAD‐(fear) | GAD‐(Depression + fear) |
| Fear | Fear‐(GAD) | Fear‐(depression) | Fear‐(GAD + depression) |
Abbreviation: GAD, generalized anxiety disorder.
Outcome‐(covariate[s]).
Examining the genetic structure of distress and fear requires information about the individual effects of each SNP on a trait, and these effects are obtained by conducting a GWAS. Therefore, preliminary to main analyses, we conducted GWAS with BGENIE version 1.2 for all disorder phenotypes presented in Table 1, controlling for age, sex, six genetic principal components for European samples, and factors representing variability in initial assessment center and genotyping batch (Bycroft et al., 2017). GWAS results were not interpreted and were used for the following genetic correlation analyses (summary statistics of GWAS are available at https://phenviz.navigome.com/downloads). With GWAS results, we estimated (a) SNP heritability to document the contribution of common genetic variation to each disorder and (b) genetic correlations between disorders (Bulik‐Sullivan, Finucane et al., 2015; Bulik‐Sullivan, Loh et al., 2015). We conducted genetic correlations with the initial and residual phenotypes that were used for full and partial phenotypic correlations. We also conducted genetic correlations between loneliness, social isolation, and disorders (see Figures S1 and S2).
Finally, to investigate the environmental structure of distress and fear disorders, we examined their full and partial phenotypic correlations with loneliness and social isolation. Here, partial correlations allowed examining the extent to which controlling for one disorder affected the association between another disorder and one psychosocial factor.
3. RESULTS
3.1. Phenotype description
The number of cases and controls for each phenotype is provided in Table 2. Loneliness and social isolation were evaluated in the full sample of the UK Biobank, unlike anxiety and depressive disorders that were measured with the Mental Health Questionnaire on a subset of the sample. This explains why there were more participants for loneliness and social isolation.
Table 2.
Distributions of disorders
| Depression | Generalized anxiety | Fear | Loneliness | Social isolation | |
|---|---|---|---|---|---|
| Cases | 44,357 | 11,111 | 11,425 | 88,430 | 15,530 |
| Controls | 88,650 | 96,821 | 114,853 | 389,807 | 487,409 |
| Cases/cases + controls | 0.33 | 0.10 | 0.09 | 0.18 | 0.03 |
| Total number of subjects | 133,007 | 107,932 | 126,278 | 478,237 | 502,939 |
3.2. Phenotypic structure of distress and fear
Full and partial correlations were used to examine phenotypic associations among disorders (see Table 3). Full correlations partially supported the distress and fear structure. However, the phenotypic structure of distress and fear emerged more clearly when reviewing partial correlations. Differences between correlations were tested with a two‐sample Z test after performing a Fisher r‐to‐z transformation. All partial correlations were statistically different from each other, and from their corresponding full correlation. These associations provide preliminary evidence for the phenotypic distinction between distress and fear dimensions.
Table 3.
Phenotypic correlations between disorders
| Generalized anxiety | Depression | Fear | |
|---|---|---|---|
| Generalized anxiety | – | 0.872 (0.868–0.878) | 0.723 (0.715–0.733) |
| Depression | 0.561 (0.557–0.566) | – | 0.510 (0.500–0.522) |
| Fear | 0.268 (0.262–0.274) | 0.056 (0.050–0.063) | – |
Note: Full correlations are presented in the right part of the table above the diagonal. Partial correlations, which controlled for the other phenotype, are bottom left of the diagonal. All correlations are statistically significant, p < .001. 95% confidence intervals are presented in parentheses and were bootstrapped for tetrachoric correlations.
3.3. Genetic structure of distress and fear
Table 4 presents SNP heritability estimates for all variables. Liability scale estimates were based on sample prevalence under the assumption of accurate sampling. Sensitivity analyses were conducted, with population prevalence 10% higher or lower than sample prevalence. Heritability for psychosocial factors were included because we tested their genetic correlations with the disorders, and these correlations are best understood in the context of their individual SNP heritability (see the Supplementary material).
Table 4.
SNP heritability estimates
| Phenotype | Observed h 2 | h 2 converted to liability scale | ||
|---|---|---|---|---|
| Population prevalence = sample prevalence | Population prevalence = sample prevalence + 10% | Population prevalence = sample Prevalence − 10% | ||
| Generalized anxiety | 0.058 (0.006) | 0.215 (0.022) | 0.224 (0.023) | 0.205 (0.021) |
| Depression | 0.070 (0.006) | 0.124 (0.010) | 0.128 (0.010) | 0.121 (0.010) |
| Fear | 0.028 (0.004) | 0.103 (0.015) | 0.107 (0.015) | 0.098 (0.014) |
| Loneliness | 0.036 (0.002) | 0.078 (0.004) | 0.081 (0.004) | 0.075 (0.004) |
| Social isolation | 0.007 (0.004) | 0.042 (0.025) | 0.045 (0.026) | 0.043 (0.025) |
Note: Standard errors are presented in parentheses. All heritability estimates are statistically significant, p < .001.
Abbreviation: SNP, single‐nucleotide polymorphism.
Genetic correlations are presented in Table 5 and indicated that all disorders were all genetically correlated. Partial correlations showed a pattern of associations that, again, partially supported the distress and fear distinction. Depression and generalized anxiety remained strongly genetically correlated after controlling for fear, and their respective genetic association with fear was reduced after controlling for generalized anxiety (for depression) or depression (for generalized anxiety). Yet, despite being slightly attenuated, the genetic correlation between generalized anxiety and fear remained strong after controlling for depression, therefore not entirely distinguishing fear from distress disorders. Finally, analyses using the block‐jackknife method, a resampling technique used to estimate standard errors (Bulik‐Sullivan, Finucane et al., 2015; Quenouille, 1956; Tukey, 1958) showed that none of these genetic correlations were statistically different.
Table 5.
Genetic correlations between disorders
| Generalized anxiety | Depression | Fear | |
|---|---|---|---|
| Generalized anxiety | – | 0.816 (0.050) | 0.718 (0.076) |
| Depression | 0.798 (0.059) | – | 0.679 (0.069) |
| Fear | 0.632 (0.191) | 0.335 (0.264) | – |
Note: Full correlations are presented in the right part of the table above the diagonal. Partial correlations, which controlled for the other phenotype, are bottom left of the diagonal. All correlations are statistically significant, p < .001. Standard errors are presented in parentheses.
3.4. Environmental structure of distress and fear
Full and partial correlations between disorders and psychosocial variables are presented in Figures 1 and 2. Loneliness was moderately correlated with generalized anxiety (r = .25) and depression (r = .26), and only weakly with fear (r = .11). In contrast, associations with social isolation were very weak (r < .02) and did not allow distinguishing distress disorders from fear. Again, differences between correlations were tested with a two‐sample Z test after a Fisher r‐to‐z transformation, but none of them were statistically different.
Figure 1.
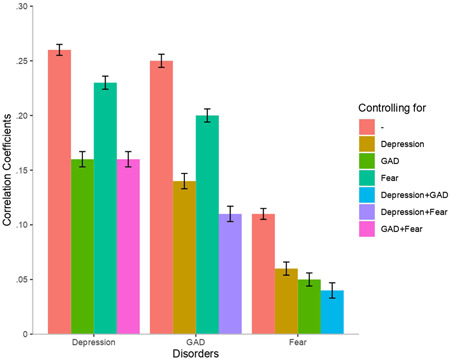
Phenotypic correlations between loneliness and disorders. 95% confidence intervals are presented as error bars. GAD, generalized anxiety disorder
Figure 2.
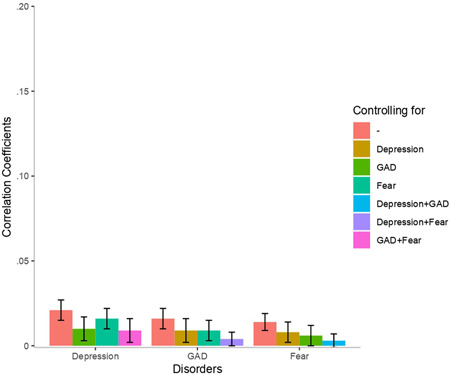
Phenotypic correlations between social isolation and disorders. 95% confidence intervals are presented as error bars. GAD, generalized anxiety disorder
Partial correlations showed that the association between loneliness and depression was marginally more attenuated when controlling for generalized anxiety than when controlling for fear. Similarly, the association between loneliness and generalized anxiety was more strongly attenuated when controlling for depression than when controlling for fear, suggesting that depression and generalized anxiety shared more variance with loneliness than did depression and fear. Partial correlations between loneliness and fear were weak. Partial correlations between loneliness and the unique variance of each disorder (controlling for the other two disorders) revealed stronger associations with depression and generalized anxiety than with fear. Overall, partial correlations indicate that the two distress disorders shared more variance with loneliness than either one of the distress disorder and fear. We conducted genetic correlations between disorders and psychosocial variables to document the role of SNPs in these associations (see Figures S1 and S2).
4. DISCUSSION
The aim of this study was to examine the role of specific genetic and psychosocial factors in validating the distress and fear classification for anxiety and depressive disorders. Using data from the UK Biobank, we provide preliminary evidence that this hierarchical structure is supported through genome‐wide genetic associations and phenotypic relationships with loneliness.
First, we found that genome‐wide genetic correlations partially supported the distress and fear model. Our results add to previous twin studies showing strong genetic correlations between depression and generalized anxiety by suggesting that this genetic association is in part accounted for by common genetic variants (Kendler et al., 1992; Roy et al., 1995). This finding provides preliminary evidence that the genetic correlation between broadly measured anxiety and depression from a recent genome‐wide study may be due to a genetic overlap between depression and generalized anxiety specifically, and not between depression and fear disorders (Anttila et al., 2018). Second, in agreement with the distinction of distress and fear disorders, we found no genetic relationship between depression and fear after controlling for general anxiety. This finding is inconsistent with twin study findings showing a genetic link between panic disorder (a fear disorder), and depression (Kendler et al., 2003). Had we tested this association between specific fear disorder and depression, we may have found similar results. However, statistical power was not sufficient to perform genetic correlations with each fear disorder separately. Finally, we found that distress and fear were not entirely distinguishable on the basis of their genetic structure since there was a genetic association between generalized anxiety and fear, independently from depression. This genetic association may be explained by a common genetic vulnerability for symptoms characterizing all anxiety disorders, for instance, excessive worry or fear about the future, which are not a core feature of depression (APA, 2013; Kessler et al., 1998). Nevertheless, at the phenotypic level, generalized anxiety and fear were only moderately associated when controlling for depression and their genetic association has to be interpreted within the scope of this moderate phenotypic association.
Next, we found that the distress and fear structure was also supported to some extent by phenotypic relationships with loneliness. Depression and generalized anxiety showed moderate associations with loneliness, while fear was only weakly correlated with loneliness. This finding provides additional evidence for a shared distress dimension and for a distinction between distress and fear disorders. It is consistent with previous studies showing that lonely individuals are more likely to have depression or generalized anxiety and adds to the current literature by indicating that loneliness may not be as strongly linked to fear disorders (Beutel et al., 2017; Hyland et al., 2018). This partial distinction with fear may be explained by the fact that loneliness is a negative feeling reflecting a subjective dissatisfaction about one's social relationships (Ernst & Cacioppo, 1999), and that negative affect could be a component more associated with distress than with fear (Gamez, Watson, & Doebbeling, 2007; Mineka et al., 1998). Moreover, it is possible that the phenotypic association between loneliness and distress disorders is driven by common genetic influences. We conducted genetic correlations between loneliness and all disorders and found that, indeed, loneliness was genetically associated with depression and generalized anxiety, respectively (see Figure S1). Future studies should examine whether SNPs associated with loneliness are shared across both distress disorders.
In contrast with loneliness, social isolation was not phenotypically correlated with any disorder. This may be explained by the fact that isolated anxious or depressed individuals are likely to refrain from seeking treatment (Mojtabai, Olfson, & Mechanic, 2002). Therefore, it is possible that isolated individuals who may have received a diagnosis had they consulted a professional have been ignored. Furthermore, some individuals do not mind living alone and prefer solitary hobbies rather than group activities (Cacioppo, Cacioppo, Capitanio, & Cole, 2015). These individuals may be satisfied with their social life and for them, social isolation may not be a risk factor for anxiety or depression. Nevertheless, our findings contribute to a debate as to whether social isolation is a risk factor for anxiety and depression. While our results are inconsistent with evidence suggesting a link between social isolation and anxiety and depression (Schwarzbach et al., 2014; Teo et al., 2013), they are coherent with other studies showing that only loneliness, and not social isolation, is a risk factor for poor mental health (Coyle & Dugan, 2012; Steptoe et al., 2013).
The strengths of this study are the large population‐based sample of the UK Biobank, the genome‐wide genetic data, and the evaluations of specific anxiety disorders and psychosocial factors. These evaluations allowed differentiating generalized anxiety from the other anxiety disorders and loneliness from social isolation. However, our study bears some limits. First, we were unable to examine fear disorders separately to have sufficient statistical power to perform genomic analyses. Second, evaluations of depression and generalized anxiety were likely to be more accurate than the single‐item measure for fear disorders. However, measures were based on available data in the UK Biobank and allowed us to have specific measures of all anxiety disorders. Third, this study was observational and did not allow inference on the direction of association between psychosocial factors and the disorders. It is possible that loneliness is a consequence of the disorders rather than a risk factor or that a gene‐environment correlation is at play (see the Supplementary material). Future research should examine this question within a longitudinal perspective. Fourth, it is possible that we found strong genetic correlations because both genetic and phenotypic data came from the same sample. Future research should aim at replicating these findings across different samples. Finally, participants of the UK Biobank are on average healthier and more likely to live in less socioeconomically deprived areas than the general UK population (Fry et al., 2017) and only individuals from European ancestry were included in genetic analyses. This limits the generalization of results to the general population and to individuals of other ancestry.
5. CONCLUSION
This study provides preliminary evidence supporting the distress and fear classification of anxiety and depression. Above and beyond symptom and diagnostic characteristics, findings revealed that measured genetic variants and loneliness may accurately distinguish distress from fear. There is still a need to further clarify the etiological architecture of the distress and fear model, but our study contributes to the current state of knowledge on potential mechanisms underlying this structure.
CONFLICT OF INTERESTS
The authors declare that there are no conflict of interests.
Supporting information
Supporting information
ACKNOWLEDGMENTS
This study has been conducted using the UK Biobank Resource, under the application 18177. We acknowledge the work of the scientists involved in the creation of the UK Biobank and we thank all the participants who have generously agreed to share their life experiences. This study represents independent research part funded by the NIHR Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King's College London. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health and Social Care. High performance computing facilities were funded with capital equipment grants from the GSTT Charity (TR130505) and Maudsley Charity (980). The work of T. C. Eley is funded by a program grant from the UK Medical Research Council (MR/M021475/1). The work of G. Morneau‐Vaillancourt is supported by a Doctoral Research Scholarship from the Fonds de recherche du Québec ‐ Société et Culture and by the Quebec Network on Suicide, Mood Disorders and Related Disorders. C. Rayner is supported by a grant from Foundation Peters to T. C. Eley and G. Breen. The work of K. L. Purves is supported by a grant from the Alexander Von Humboldt Foundation and by the UK medical Research Council (MR/M021475/1). The work of R. Cheesman is supported by an ESRC studentship.
Morneau‐Vaillancourt G, Coleman JRI, Purves KL, et al. The genetic and environmental hierarchical structure of anxiety and depression in the UK Biobank. Depress Anxiety. 2020;37:512–520. 10.1002/da.22991
Contributor Information
Gerome Breen, Email: gerome.breen@kcl.ac.uk.
Thalia C. Eley, Email: thalia.eley@kcl.ac.uk.
DATA AVAILABILITY STATEMENT
The data (GWAS summary statistics) that support the findings of this study are openly available at https://phenviz.navigome.com/downloads.
REFERENCES
- Anttila, V. , Bulik‐Sullivan, B. , Finucane, H. K. , Walters, R. K. , Bras, J. , Duncan, L. , … Murray, R. (2018). Analysis of shared heritability in common disorders of the brain. Science, 360, eaap8757 10.1126/science.aap8757 [DOI] [PMC free article] [PubMed] [Google Scholar]
- American Psychiatric Association (2013). Diagnostic and statistical manual of mental disorders (5). Washington, DC: American Psychiatric Association. [Google Scholar]
- Baselmans, B. M. L. , van de Weijer, M. P. , Abdellaoui, A. , Vink, J. M. , Hottenga, J. J. , Willemsen, G. , … Bartels, M. (2019). A genetic investigation of the well‐being spectrum. Behavior Genetics, 49, 286–297. 10.1007/s10519-019-09951-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beutel, M. E. , Klein, E. M. , Brähler, E. , Reiner, I. , Jünger, C. , Michal, M. , … Tibubos, A. N. (2017). Loneliness in the general population: Prevalence, determinants and relations to mental health. BMC Psychiatry, 17, 97 10.1186/s12888-017-1262-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bulik‐Sullivan, B. , Finucane, H. K. , Anttila, V. , Gusev, A. , Day, F. R. , Loh, P.‐R. , … Neale, B. M. (2015). An atlas of genetic correlations across human diseases and traits. Nature Genetics, 47, 1236–1241. 10.1038/ng.3406 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bulik‐Sullivan, B. , Loh, P.‐R. , Finucane, H. K. , Ripke, S. , Yang, J. , Patterson, N. , … Neale, B. M. (2015). LD Score regression distinguishes confounding from polygenicity in genome‐wide association studies. Nature Genetics, 47, 291–295. 10.1038/ng.3211 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bycroft, C. , Freeman, C. , Petkova, D. , Band, G. , Elliott, L. T. , Sharp, K. , … Marchini, J. (2017). Genome‐wide genetic data on ~500 000 UK Biobank participants. BioRxiv, 10.1101/166298 [DOI] [Google Scholar]
- Bycroft, C. , Freeman, C. , Petkova, D. , Band, G. , Elliott, L. T. , Sharp, K. , … Marchini, J. (2018). The UK Biobank resource with deep phenotyping and genomic data. Nature, 562, 203–209. 10.1038/s41586-018-0579-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cacioppo, J. T. , Cacioppo, S. , Capitanio, J. P. , & Cole, S. W. (2015). The neuroendocrinology of social isolation. Annual Review of Psychology, 66, 733–767. 10.1146/annurev-psych-010814-015240 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coleman, J. R. I. , Peyrot, W. J. , Purves, K. L. , Davis, K. A. S. , Rayner, C. , Choi, S. W. , … Breen, G. (2019). Genome‐wide gene‐environment analyses of major depressive disorder and reported lifetime traumatic experiences in UK Biobank. BioRxiv, 10.1101/247353 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coyle, C. E. , & Dugan, E. (2012). Social isolation, loneliness and health among older adults. Journal of Aging and Health, 24, 1346–1363. 10.1177/0898264312460275 [DOI] [PubMed] [Google Scholar]
- Craske, M. G. , Stein, M. B. , Eley, T. C. , Milad, M. R. , Holmes, A. , Rapee, R. M. , & Wittchen, H.‐U. (2017). Anxiety disorders. Nature Reviews Disease Primers, 3, 17024 10.1038/nrdp.2017.24 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davis, K. A. S. , Coleman, J. R. I. , Adams, M. , Allen, N. , Breen, G. , Cullen, B. , … Hotopf, M. (2018). Mental health in UK Biobank: Development, implementation and results from an online questionnaire completed by 157,366 participants. BJPsych Open, 4, 83–90. 10.1192/bjo.2018.12 [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- Eley, T. C. , Rijsdijk, F. V. , Perrin, S. , O'Connor, T. G. , & Bolton, D. (2008). A multivariate genetic analysis of specific phobia, separation anxiety and social phobia in early childhood. Journal of Abnormal Child Psychology, 36, 839–848. 10.1007/s10802-008-9216-x [DOI] [PubMed] [Google Scholar]
- Ernst, J. M. , & Cacioppo, J. T. (1999). Lonely hearts: Psychological perspectives on loneliness. Applied and Preventive Psychology, 8, 1–22. 10.1016/S0962-1849(99)80008-0 [DOI] [Google Scholar]
- Fry, A. , Littlejohns, T. J. , Sudlow, C. , Doherty, N. , Adamska, L. , Sprosen, T. , Collins, R. , & Allen, N. E. (2017). Comparison of sociodemographic and health‐related characteristics of UK Biobank participants with those of the general population. American Journal of Epidemiology, 186, 1026–1034. 10.1093/aje/kwx246 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gamez, W. , Watson, D. , & Doebbeling, B. N. (2007). Abnormal personality and the mood and anxiety disorders: Implications for structural models of anxiety and depression. Journal of Anxiety Disorders, 21, 526–539. 10.1016/j.janxdis.2006.08.003 [DOI] [PubMed] [Google Scholar]
- Hettema, J. M. , Prescott, C. A. , Myers, J. M. , Neale, M. C. , & Kendler, K. S. (2005). The structure of genetic and environmental risk factors for anxiety disorders in men and women. Archives of General Psychiatry, 62, 182–189. 10.1001/archpsyc.62.2.182 [DOI] [PubMed] [Google Scholar]
- Holt‐Lunstad, J. , Smith, T. B. , Baker, M. , Harris, T. , & Stephenson, D. (2015). Loneliness and social isolation as risk factors for mortality. Perspectives on Psychological Science, 10, 227–237. 10.1177/1745691614568352 [DOI] [PubMed] [Google Scholar]
- Howard, D. M. , Adams, M. J. , Clarke, T.‐K. , Hafferty, J. D. , Gibson, J. , Shirali, M. , … McIntosh, A. M. (2019). Genome‐wide meta‐analysis of depression identifies 102 independent variants and highlights the importance of the prefrontal brain regions. Nature Neuroscience, 22, 343–352. 10.1038/s41593-018-0326-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hughes, M. E. , Waite, L. J. , Hawkley, L. C. , & Cacioppo, J. T. (2004). A short scale for measuring loneliness in large surveys. Research on Aging, 26, 655–672. 10.1177/0164027504268574 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hyland, P. , Shevlin, M. , Cloitre, M. , Karatzias, T. , Vallières, F. , McGinty, G. , … Power, J. M. (2018). Quality not quantity: Loneliness subtypes, psychological trauma, and mental health in the US adult population. Social Psychiatry and Psychiatric Epidemiology, 3, 10.1007/s00127-018-1597-8 [DOI] [PubMed] [Google Scholar]
- Kendler, K. S. , Neale, M. C. , Kessler, R. C. , Heath, A. C. , & Eaves, L. J. (1992). Major depression and generalized anxiety disorder. Same genes, (partly) different environments? Archives of General Psychiatry, 49, 716–722. [DOI] [PubMed] [Google Scholar]
- Kendler, K. S. , Prescott, C. A. , Myers, J. , & Neale, M. C. (2003). The structure of genetic and environmental risk factors for common psychiatric and substance use disorders in men and women. Archives of General Psychiatry, 60, 929–937. 10.1001/archpsyc.60.9.929 [DOI] [PubMed] [Google Scholar]
- Kessler, R. C. , Aguilar‐Gaxiola, S. , Alonso, J. , Chatterji, S. , Lee, S. , Ormel, J. , … Wang, P. S. (2009). The global burden of mental disorders: An update from the WHO World Mental Health (WMH) Surveys. Epidemiologia e Psichiatria Sociale, 18, 23–33. 10.1017/S1121189X00001421 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kessler, R. C. , Andrews, G. , Mroczek, D. , Ustun, B. , & Wittchen, H. ‐U. (1998). The World Health Organization Composite International Diagnostic Interview short‐form (CIDI‐SF). International Journal of Methods in Psychiatric Research, 7, 171–185. 10.1002/mpr.47 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krueger, R. F. (1999). The structure of common mental disorders. Archives of General Psychiatry, 56, 921–926. 10.1001/archpsyc.56.10.921 [DOI] [PubMed] [Google Scholar]
- Loken, E. K. , Hettema, J. M. , Aggen, S. H. , & Kendler, K. S. (2014). The structure of genetic and environmental risk factors for fears and phobias. Psychological Medicine, 44, 2375–2384. 10.1017/S0033291713003012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luo, Y. , Hawkley, L. C. , Waite, L. J. , & Cacioppo, J. T. (2012). Loneliness, health, and mortality in old age: A national longitudinal study. Social Science & Medicine, 74, 907–914. 10.1016/j.socscimed.2011.11.028 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meier, S. M. , Trontti, K. , Purves, K. L. , Als, T. D. , Grove, J. , Laine, M. , … Mors, O. (2019). Genetic variants associated with anxiety and stress‐related disorders: A genome‐wide association study and mouse‐model study. JAMA Psychiatry, 76, 924–932. 10.1001/jamapsychiatry.2019.1119 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mineka, S. , Watson, D. , & Clark, L. A. (1998). Comorbidity of anxiety and unipolar mood disorders. Annual Review of Psychology, 49, 377–412. [DOI] [PubMed] [Google Scholar]
- Mojtabai, R. , Olfson, M. , & Mechanic, D. (2002). Perceived need and help‐seeking in adults with mood, anxiety, or substance use disorders. Archives of General Psychiatry, 59, 77–84. 10.1001/archpsyc.59.1.77 [DOI] [PubMed] [Google Scholar]
- Otowa, T. , Hek, K. , Lee, M. , Byrne, E. M. , Mirza, S. S. , Nivard, M. G. , … Hettema, J. M. (2016). Meta‐analysis of genome‐wide association studies of anxiety disorders. Molecular Psychiatry, 21, 1391–1399. 10.1038/mp.2015.197 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Purves, K. L. , Coleman, J. R. I. , Meier, S. , Rayner, C. , Davis, K. A. S. , Cheesman, R. , … Eley, T. C. (2019). A major role for common genetic variation in anxiety disorders. Molecular Psychiatry, 10.1038/s41380-019-0559-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quenouille, M. H. (1956). Notes on bias in estimation. Biometrika, 43, 353–360. 10.1093/biomet/43.4-4.353 [DOI] [Google Scholar]
- R Core Team (2017). R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria: Retrieved from https://www.R‐project.org/ [Google Scholar]
- Roy, M.‐A. , Neale, M. C. , Pedersen, N. L. , Mathé, A. A. , & Kendler, K. S. (1995). A twin study of generalized anxiety disorder and major depression. Psychological Medicine, 25, 1037–1049. 10.1017/S0033291700037533 [DOI] [PubMed] [Google Scholar]
- Schwarzbach, M. , Luppa, M. , Forstmeier, S. , König, H. H. , & Riedel‐Heller, S. G. (2014). Social relations and depression in late life—A systematic review. International Journal of Geriatric Psychiatry, 29, 1–21. 10.1002/gps.3971 [DOI] [PubMed] [Google Scholar]
- Silberg, J. L. , Rutter, M. , & Eaves, L. (2001). Genetic and environmental influences on the temporal association between earlier anxiety and later depression in girls. Biological Psychiatry, 49, 1040–1049. 10.1016/S0006-3223(01)01161-1 [DOI] [PubMed] [Google Scholar]
- Slade, T. , & Watson, D. (2006). The structure of common DSM‐IV and ICD‐10 mental disorders in the Australian general population. Psychological Medicine, 36, 1593–1600. 10.1017/S0033291706008452. [DOI] [PubMed] [Google Scholar]
- Steptoe, A. , Shankar, A. , Demakakos, P. , & Wardle, J. (2013). Social isolation, loneliness, and all‐cause mortality in older men and women. Proceedings of the National Academy of Sciences, 110, 5797–5801. 10.1073/pnas.1219686110 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sudlow, C. , Gallacher, J. , Allen, N. , Beral, V. , Burton, P. , Danesh, J. , … Collins, R. (2015). UK Biobank: An open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS Medicine, 12, e1001779 10.1371/journal.pmed.1001779 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sullivan, P. F. , Neale, M. C. , & Kendler, K. S. (2000). Genetic epidemiology of major depression: Review and meta‐analysis. American Journal of Psychiatry, 157, 1552–1562. 10.1176/appi.ajp.157.10.1552 [DOI] [PubMed] [Google Scholar]
- Tanskanen, J. , & Anttila, T. (2016). A prospective study of social isolation, loneliness, and mortality in Finland. American Journal of Public Health, 106, 2042–2048. 10.2105/AJPH.2016.303431 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Teo, A. R. , Lerrigo, R. , & Rogers, M. A. M. (2013). The role of social isolation in social anxiety disorder: A systematic review and meta‐analysis. Journal of Anxiety Disorders, 27, 353–364. 10.1016/j.janxdis.2013.03.010 [DOI] [PubMed] [Google Scholar]
- Tukey, J. W. (1958). Bias and confidence in not‐quite large samples. Annals of Mathematical Statistics, 29, 614–623. [Google Scholar]
- Vollebergh, W. A. M. , Iedema, J. , Bijl, R. V. , de Graaf, R. , Smit, F. , & Ormel, J. (2001). The structure and stability of common mental disorders. Archives of General Psychiatry, 58, 597–603. 10.1001/archpsyc.58.6.597 [DOI] [PubMed] [Google Scholar]
- Waszczuk, M. A. , Zavos, H. M. S. , Gregory, A. M. , & Eley, T. C. (2014). The phenotypic and genetic structure of depression and anxiety disorder symptoms in childhood, adolescence, and young adulthood. JAMA Psychiatry, 71, 905–916. 10.1001/jamapsychiatry.2014.655 [DOI] [PubMed] [Google Scholar]
- Watson, D. (2005). Rethinking the mood and anxiety disorders: A quantitative hierarchical model for DSM‐V. Journal of Abnormal Psychology, 114, 522–536. 10.1037/0021-843X.114.4.522 [DOI] [PubMed] [Google Scholar]
- Wray, N. R. , Ripke, S. , Mattheisen, M. , Trzaskowski, M. , Byrne, E. M. , Abdellaoui, A. , … Bacanu, S. A. (2018). Genome‐wide association analyses identify 44 risk variants and refine the genetic architecture of major depression. Nature genetics, 50, 668–681. 10.1038/s41588-018-0090-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting information
Data Availability Statement
The data (GWAS summary statistics) that support the findings of this study are openly available at https://phenviz.navigome.com/downloads.