

Maia Dorsett.

In medicine, we examine our errors closely. Since the publication of To Err Is Human by the Institute of Medicine at the end of the past century, patient safety and quality are priorities (1). One core principle is that we cannot improve care if we do not examine our errors and use them to change our processes. Errors are destined to be repeated, and risk to patients further magnified when we do not learn from mistakes.
The past few months have tragically left us with ample opportunities to improve. The coronavirus disease 2019 (COVID-19) pandemic has amplified preexisting deficiencies and inequities of our healthcare system. U.S. healthcare is incentivized to react to sickness rather than proactively focus on health maintenance. As an emergency physician, I witness the impact of this approach daily. Far more money and effort are expended on minimally impactful interventions than addressing social determinants of health such as housing, food security, and safety from violence. Collectively, these have a greater impact on healthcare outcomes than any pill. Procedures to manage illness are well compensated, but public health systems to improve population health are underfunded and understaffed. On any given day, emergency departments (EDs) operate near or over capacity. A lack of inpatient beds forces EDs to hold admitted patients until space is available. ED care is then shunted to suboptimal conditions, leaving us to care for patients in waiting rooms, chairs, and hallways (2). Such reactionary systems fail spectacularly in the face of time-sensitive emergencies, because they lack the plasticity to respond quickly (3). Our healthcare and public health systems have faltered in the face of the COVID-19 pandemic. The question remains, will we learn from our mistakes?
COVID-19 is a slow-moving mass casualty incident (MCI). An MCI occurs when the available local resources, such as personnel and equipment, are overwhelmed by the number and severity of casualties. We typically think of MCIs as abbreviated, geographically bounded events—a building collapse, a terrorist attack, a school shooting, but COVID-19 is a slow-moving tidal wave. Defining this pandemic as an MCI is key, because, regardless of the type of hazard or degree of effect, common principles and structure exist to guide the emergency management of these events (4). There are four phases of the emergency management cycle that can be applied to analyze and guide our pandemic response (Fig. 1) (5, 6).
Fig. 1. Emergency management cycle.
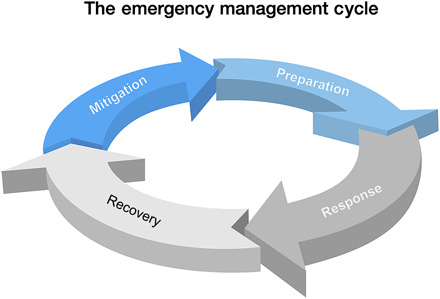
(i) Mitigation. Mitigation refers to efforts to reduce the effect of an MCI before the event. This applies to events that can be announced, such as the COVID-19 pandemic. In the case of COVID-19, a significant lag time occurred between first reported cases and development of community spread within the United States. Examples of COVID-19 mitigation include early travel and gathering restrictions, expanded testing, and increased public health activities including contact tracing.
(ii) Preparation. Preparedness activities are necessary when mitigation measures have not or cannot prevent a disaster. In this phase, governments and organizations devise and enact plans to minimize the damage and save the maximum number of lives. For COVID-19, this includes stockpiling of resources, including personal protective equipment (PPE), ventilators, testing equipment, and supplies. It also involves development and testing of plans to increase hospital capacity such as conversion of nontraditional units into intensive care units (ICUs) and existing agreements between healthcare entities to load-balance patients within the healthcare system. Inadequate preparation for this pandemic fostered a sense of betrayal for healthcare professionals. For instance, the U.S. Centers for Disease Control and Prevention’s rapid de-escalation of its recommendations for use of PPE was widely felt to be more a response to lack of resources than to a finding that providers were at less risk. Healthcare professionals serving in all sectors, from Emergency Medical Services to hospital personnel, have become infected in significant numbers (7–9).
(iii) Response. Response activities occur during and immediately following a disaster. The primary objective is to assist victims and reduce secondary damage. This includes activation and notification of key organizations and personnel, organization of command, and implementing resource allocation strategies to save as many lives as possible. Examples during the COVID-19 pandemic include lockdowns and social distancing, resource distribution of ventilators and personnel, alteration in Emergency Medical Services protocols to move patients to alternate destinations, and utilization of telehealth to provide assessment and care while minimizing patient movement and exposure of healthcare personnel. When demand exceeds available resources, response may include implementation of Crisis Standards of Care, where care standards shift away from day-to-day conventional standards, allocating healthcare resources (such as ventilators, ICU beds, or even initiation of resuscitation) to save as many lives as possible. Since the need to implement altered standards depends on existing resources, a system that normally operates near or over capacity is more likely to cross the Crisis Standard threshold.
COVID-19 is an ICU disease. While most patients do well, a significant proportion require prolonged mechanical ventilation. Although understanding of this novel disease is evolving daily, with many unknowns and experimental treatments ongoing, there are a few things we do know: patients requiring invasive ventilation will do better when cared for by specialists trained in intensive care (10). In places where systems have been overwhelmed and healthcare professionals with a wide range of training have been drafted to care for these patients, finding ways to expand oversight by critical care–trained physicians, such as using telemedicine services, is critical to improving survival for those who are most critically ill (11).
The response phase also requires monitoring for unintended consequences and modifying appropriately. Early on, there was a concerted effort to discourage ED use for non-emergent conditions to improve ED capacity and decrease opportunities for exposure within the ED. This initiative, while successful, has had worrisome consequences. With the exceptions of EDs in outbreak epicenters, which were overwhelmed for weeks, those in the rest of the country are now seeing record-low numbers of patients. Emergency physicians are wondering where all the patients with heart attacks, strokes, and sepsis are (12). The answer likely lies in the increased incidence of out-of-hospital cardiac arrest, which partly reflects patients remaining at home for fear of contracting COVID-19 at the hospital.
(iv) Recovery. This is the last but equally crucial phase. While technically recovery follows response, preparing for recovery begins as soon as an incident starts. Recovery from this pandemic will focus on how to reopen our society and economy. The key to successful recovery with minimal health impact will be testing capacity and availability of trained public health professionals to assess contacts, manage new cases, and determine whether return to response mode is warranted. It also includes measures such as vaccine development. We must cycle back to mitigation before reopening. Premature reopening only invites recurrent disaster.
While attention usually focuses on the response phase, emergency management requires a balanced approach with attention and funding for each phase. By design, a well-organized and robust public health and emergency preparedness system may appear as an overreaction. This is because carefully planned and executed preventive interventions can minimize the degree of tragedy before lives are lost, rather than rushed reactionary band-aids once the system is overwhelmed. The fence around the swimming pool does not draw the same attention as the resuscitation of a toddler who fell in, but by every measure, the fence is the far better of the two options.
Many aspects of life will never be the same after this pandemic. However, there are some aspects that we hope do not return to “normal.” Great innovations and shifts have been made, particularly in the area of matching resources to patient needs. Telehealth has expanded to provide continued care, match patient needs with destination when they access the 911 system, and provide follow-up care upon discharge from the hospital. Emergency medical services is now recognized as a frontline healthcare provider, has become interconnected with telehealth, and will be reimbursed for patient transport to non-ED destinations that are more appropriate. Hospitals have adjusted schedules for profitable elective procedures to increase the capacity to care for patients with emergency conditions and for potential surges. Our healthcare system is beginning to value and assure a proactive approach rather than a reactive one.
Emergency management is a cycle, and we must now use the recovery phase to analyze the strengths and deficiencies of our response to begin the mitigation and planning phases for the next, unplanned hazard. We can hope that our collective memory is long, not short.
REFERENCES AND NOTES
- 1.L. T. Kohn, J. Corrigan, M. S. Donaldson, To Err Is Human: Building a Safer Health System (National Academy Press, 2000); http://site.ebrary.com/id/10038653. [PubMed]
- 2.McKenna P., Heslin S. M., Viccellio P., Mallon W. K., Hernandez C., Morley E. J., Emergency department and hospital crowding: Causes, consequences, and cures. Clin. Exp. Emerg. Med. 6, 189–195 (2019). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mareiniss D. P., The impending storm: COVID-19, pandemics and our overwhelmed emergency departments. Am. J. Emerg. Med. S0735675720301753 (2020). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Coccolini F., Sartelli M., Kluger Y., Pikoulis E., Karamagioli E., Moore E. E., Biffl W. L., Peitzman A., Hecker A., Chirica M., Damaskos D., Ordonez C., Vega F., Fraga G. P., Chiarugi M., Di Saverio S., Kirkpatrick A. W., Abu-Zidan F., Mefire A. C., Leppaniemi A., Khokha V., Sakakushev B., Catena R., Coimbra R., Ansaloni L., Corbella D., Catena F., COVID-19 the showdown for mass casualty preparedness and management: The Cassandra syndrome. World J. Emerg. Surg. 15, 26 (2020). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.National Governors’ Association, Center for Policy Research, in Comprehensive Emergency Management: A Governor’s Guide (NGA State Emergency Management Series, National Governorsy Research, i, 1979).
- 6.Macintyre A. G., Barbera J. A., Brewster P., Health care emergency management: Establishing the science of managing mass casualty and mass effect incidents. Disaster Med. Public Health Prep. 3, S52–S58 (2009). [DOI] [PubMed] [Google Scholar]
- 7.A. Watkins, “Last week one paramedic was infected. Now over 150 are in quarantine,” New York Times, 20 March 2020; www.nytimes.com/2020/03/20/nyregion/coronavirus-nyc-emergency-response.html.
- 8.J. Greene, “More than 2,000 workers at Henry Ford Health, Beaumont affected by COVID-19,” Modern Healthcare, 6 April 2020; www.modernhealthcare.com/hospital-systems/more-2000-workers-henry-ford-health-beaumont-affected-covid-19.
- 9.CDC COVID-19 Response Team , Characteristics of health care personnel with COVID-19—United States, February 12–April 9, 2020. MMWR Morb. Mortal. Wkly. Rep. 69, 477–481 (2020). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Pronovost P. J., Angus D. C., Dorman T., Robinson K. A., Dremsizov T. T., Young T. L., Physician staffing patterns and clinical outcomes in critically Ill patients: A systematic review. JAMA 288, 2151–2162 (2002). [DOI] [PubMed] [Google Scholar]
- 11.Young L. B., Chan P. S., Lu X., Nallamothu B. K., Sasson C., Cram P. M., Impact of telemedicine intensive care unit coverage on patient outcomes: A systematic review and meta-analysis. Arch. Intern. Med. 171, 498–506 (2011). [DOI] [PubMed] [Google Scholar]
- 12.W. Feuer, “Doctors worry the coronavirus is keeping patients away from US hospitals as ER visits drop: ‘Heart attacks don’t stop’,” CNBC, 14 April 2020; www.cnbc.com/2020/04/14/doctors-worry-the-coronavirus-is-keeping-patients-away-from-us-hospitals-as-er-visits-drop-heart-attacks-dont-stop.html.