

Abstract
Background:
In December 2018, UNOS approved an allocation scheme based on recipients’ geographic distance from a deceased donor (“acuity circles”). Previous analyses suggested acuity circles (AC) would reduce waitlist mortality overall, but their impact on pediatric subgroups was not considered.
Methods:
We applied Scientific Registry of Transplant Recipients data from 2011-2016 towards the Liver Simulated Allocation Model (LSAM) to compare outcomes by age and illness severity for the UNOS-approved AC and the existing Donor Service Area (DSA)/Region-based allocation schemes. Means from each allocation scheme were compared using matched-pairs t-tests.
Results:
Over a 3-year period, AC allocation is projected to decrease waitlist deaths in infants (39 vs 55; P<0.001), children (32 vs 50; P<0.001), and teenagers (15 vs 25; P<0.001). AC allocation would increase the number of transplants in infants (707 vs 560; P<0.001), children (677 vs 547; P<0.001), and teenagers (404 vs 248; P<0.001). AC allocation led to decreased median PELD/MELD at transplant for infants (29 vs 30; P=0.01), children (26 vs 29; P<0.001), and teenagers (26 vs 31; P<0.001). Additionally, AC allocation would lead to fewer transplants in status 1B in children (97 vs 103; P=0.006) but not infants or teenagers. With AC allocation, 77% of pediatric donor organs would be allocated to pediatric candidates, compared to only 46% in DSA/Region-based allocation (P<0.001).
Conclusion:
AC allocation will likely address disparities for pediatric liver transplant candidates and recipients by increasing transplants and decreasing waitlist mortality. It is more consistent with federally-mandated requirements for organ allocation.
INTRODUCTION
Liver transplantation is a life-saving procedure for individuals with acute liver failure, metabolic deficiencies and end-stage liver disease and other conditions. The demand for liver organs greatly exceeds the available supply, necessitating a system to oversee and coordinate the distribution of deceased-donor organs. In the United States, the principles for organ allocation were outlined by the Institute of Medicine’s “Final Rule,” at the direction of the National Organ Transplant Act of 1984.1,2 The United Network for Organ Sharing (UNOS) is tasked with allocating organs in accordance with these principles: allocation procedures should be clear, equitable, provide utility, and be iteratively monitored and modified so as to maintain public trust. Additionally, the National Organ Transplant Act requires that allocation “recognize the differences in health and in organ transplantation issues between children and adults throughout the system and adopt criteria, policies, and procedures that address the unique healthcare needs of children.”1
Despite the requirement that deceased-donor organs be distributed equitably, disparities in access to these organs persist. First, pediatric candidates are disadvantaged on the waitlist, with nearly half of pediatric deceased-donors organs going to adults.3 This occurs even while waitlist mortality for infants, 20 deaths per 100 patient-years, is higher than for any other age group.4 Additionally, pediatric candidates are disadvantaged on the waitlist as they compete with adults for both pediatric and adult deceased donor organs with an allocation PELD score that underestimates candidate’s 3-month mortality compared to the allocation score for adults on the list.5 Recent attention has focused on geographic disparities in the allocation scheme organized around arbitrary boundaries that form 58 Donor Service Areas (DSA) and 11 Regions, as evidenced by variations in transplant rate and median allocation score at transplant for infants, children and adults.6–8 In response to these geographic disparities, UNOS approved in December 2018 a new allocation scheme that allocates organs based on recipients’ geographic distance from a deceased donor (“acuity circles”) and their allocation score.9 An important aspect of the new allocation policy included a different algorithm that allocated livers from donors under 18 years of age to pediatric candidates on the liver waitlist nationally before adult recipients of lower acuity listed locally. Although previous analyses suggested acuity circles would mitigate geographic disparities and reduce waitlist mortality overall, the policy was not designed specifically to ameliorate disparities for pediatric candidates, nor was the policy’s impact on pediatric subgroups explored in significant detail.10
To better understand the impact of the new UNOS-approved acuity circle allocation on pediatric liver transplant candidates and recipients, we applied the Liver Simulated Allocation Model (LSAM), the computer simulation program utilized by the Scientific Registry of Transplant Recipients (SRTR) and the Organ Procurement and Transplantation Network (OPTN), towards registry data.11 Outcomes under the new acuity circle system were compared with outcomes under the DSA/Region-based allocation scheme by age groups and acuity.
MATERIALS AND METHODS
Simulation and data source
This study used data from the SRTR. The SRTR data system includes data on all donors, waitlisted candidates, and transplant recipients in the United States, submitted by the members of the OPTN, and has been described elsewhere.12 The Health Resources and Services Administration (HRSA), U.S. Department of Health and Human Services provides oversight to the activities of the OPTN and SRTR contractors. This study was acknowledged by the Institutional Review Board of Johns Hopkins School of Medicine as being exempt from review.
LSAM is the software tool used by the SRTR to perform discrete-event simulation modeling of the United States liver allocation system.11 For this analysis, 10 replications of LSAM were run that included liver transplant candidates and organs offered between July 1, 2011 and June 30, 2016. The simulation time period was 3 years (7/1/2013-6/30/2016). LSAM settings were adjusted so the total number of transplants remained approximately the same under both schemes, as the proposed scheme was not expected to significantly change the number of available transplantable livers. In addition, for a patient whose actual disease progression was censored due to transplant, the disease progression in the absence of a transplant, including death, was imputed with that of a similar patient. Outcomes of interest included: [1] deaths on the liver transplant waitlist, [2] number of transplants, [3] median pediatric end-stage liver disease (PELD; for recipients <12 years old) or model for end-stage liver disease (MELD; for recipients ≥12 years old) score and exception score at transplant, [4] distribution of deceased-donor livers, [5] days on the liver transplant waitlist, [6] travel distance for deceased-donor livers, and [7] posttransplant survival.
Allocation schemes
To test the effects of increasing pediatric priority, we ran replications of LSAM under 2 allocation schemes: (1) acuity circle allocation as approved by OPTN Board in December, 2018,9 and (2) the DSA/Region-based allocation system.13 With acuity circle allocation, the DSA- and Region-based classifications are eliminated. Livers are allocated instead to candidates within 150, 250, or 500 nautical miles (nm) of the donor hospital, and then offered nationally (beyond 500 nm of the donor hospital). Livers are offered first to status 1A and 1B candidates within 500 nm of the donor hospital. Next, livers are offered to candidates with MELD/PELD greater than 37 within 150 nm of the donor hospital, then within 250 nm of the donor hospital, then within 500 nm of the donor hospital. Offers continue in a similar way (to candidates within 150, then 250, and then 500 nm of the donor hospital) to candidates with ranges of MELD/PELD from 33-36, then 29-32, then from 15-28. Livers are then offered nationally to status 1A and 1B candidates, then nationally to MELD/PELD greater than 15 and then finally MELD/PELD less than 15. As in the DSA/Region-based allocation system, livers from deceased donors younger than age 18 will be offered to pediatric candidates prior to adults. The difference with the acuity circle allocation is that pediatric donors will be offered to children nationally before any nonstatus 1A adults. This will give additional priority to pediatric transplant candidates compared to the current distribution system.
Statistical analysis
Across replications, the minimum, mean, and maximum for each outcome were calculated under both allocation schemes. Results were compared with matched paired t-tests. Although multiple-testing adjustments were not formally made in this analysis, we considered P ≤ 0.01 as statistical significance given the multiple tests performed. Results were compared by age group (“infant”: <2 years; “child”: 2-11; “teenager”: 12-17; and “adult”: ≥18) and by illness severity (i.e., Status 1A and 1B). When numerical results are presented in parentheses, they are always presented as “[acuity circle mean] vs [DSA/Region-based mean]” followed by the P-value.
To visualize the effect of allocation scheme on geographic disparity, we calculated for every location in the continental U.S. a weighted average of median allocation scores at transplant, with weights decreasing exponentially in distance to transplant centers. (For a worked example, see Supplemental Digital Content.)
RESULTS
Deaths on the liver transplant waitlist
Acuity circle allocation is projected to lead to fewer deaths than DSA/Region-based allocation over a 3-year period for infants (39 vs 55; P < 0.001), children (32 vs 50; P = 0.003) and teenagers (15 vs 25; P < 0.001; Table 1). In addition, acuity circle allocation would decrease the number of waitlist deaths for adults (4109 vs 4392; P < 0.001). Acuity circle allocation is projected to lead to fewer deaths for Status 1B infants (12 vs 16; P = 0.007) and children (4 vs 7; P < 0.001) but have no impact on status 1B teenagers (1 vs 1; P = 0.7). While there would be no change in the number of Status 1A deaths for any pediatric age group, there would be fewer Status 1A deaths for adults with acuity circle allocation (11 vs 27; P < 0.001).
Table 1:
Number of deaths on the liver transplant waitlist by age using acuity circles (AC) and DSA/Region-based (DSA) allocation schemes for all candidates and those with Status 1A and 1B exception. Data represent mean (minimum, maximum).
| Overall | Status 1A | Status 1B | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Age group | AC* | DSA** | P | AC | DSA | P | AC | DSA | P |
| Infant | 39 (32, 52) | 55 (46, 68) | <0.001 | 2 (0, 4) | 2 (0, 5) | 0.5 | 12 (6, 17) | 16 (10, 20) | 0.007 |
| Child | 32 (23, 41) | 50 (38, 56) | <0.001 | 3 (0, 6) | 4 (0, 10) | 0.2 | 4 (2, 5) | 7 (4, 10) | <0.001 |
| Teenager | 15 (11, 22) | 25 (20, 32) | <0.001 | 1 (0, 2) | 2 (0, 4) | 0.02 | 1 (0,3) | 1 (0, 2) | 0.7 |
| Adult | 4109 (3949, 4214) | 4392 (4235, 4458) | <0.001 | 11 (6, 19) | 27 (15, 34) | <0.001 | -- | -- | -- |
Number of transplants
Acuity circle allocation is projected to increase the number of transplants compared to DSA/Region-based allocation performed in infants (707 vs 560; P < 0.001), children (677 vs 547; P < 0.001) and teenagers (404 vs 248; P < 0.001; Table S1). In contrast, the number of transplants would decrease for adults under acuity circle allocation (16 508 vs 16 963; P < 0.001). By construction with LSAM, the total (adult plus pediatric) number of transplants would not change significantly (18 295 vs 18 319; P = 0.4).
Median PELD/MELD score and exception at transplant
For patients transplanted with priority based on their PELD/MELD score, the median allocation score at transplant is projected to decrease under acuity circle allocation for infants (29 vs 30; P = 0.01), children (26 vs 29; P < 0.001) and teenagers (26 vs 31; P < 0.001; Table 2). In contrast, the median allocation score at transplant for adults would increase (32 vs 30; P < 0.001). While geographic variability in median allocation score at transplant would decrease for adult (Figure 1a and 1b) and pediatric candidates (Figure 1c and 1d), greater variability would persist for pediatric candidates compared to adults. The number of pediatric candidates transplanted as Status 1B would be roughly similar under both allocation schemes for all pediatric groups. There would be a small decrease in Status 1B transplants for children if acuity circles allocation were adopted (97 vs 103; P = 0.006) whereas the difference cannot be distinguished from zero for infants (115 vs 117; P = 0.4) and teenagers (23 vs 27; P = 0.02). The number of candidates transplanted as Status 1A would increase for all age groups including infants (83 vs 75; P = 0.004), children (90 vs 80; P < 0.001), teenagers (75 vs 60; P < 0.001), and adults (758 vs 643; P < 0.001).
Table 2:
Median PELD/MELD score at transplant using acuity circles (AC) and DSA/Region-based (DSA) allocation schemes for all candidates and number of individuals transplanted with Status 1A and 1B exception. Data represent mean (minimum, maximum).
| Median PELD/MELD at transplant | Number of Status 1A transplants | Number of Status 1B transplants | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Age group | AC* | DSA** | P | AC | DSA | P | AC | DSA | P |
| Infant | 29 (28, 30) | 30 (30, 31) | 0.01 | 83 (69, 95) | 75 (67, 83) | 0.004 | 115 (94, 130) | 117 (100, 131) | 0.4 |
| Child | 26 (24, 28) | 29 (28, 30) | <0.001 | 90 (76, 103) | 80 (67, 92) | <0.001 | 97 (88, 108) | 103 (92, 114) | 0.006 |
| Teenager | 26 (25, 27) | 31 (30, 32) | <0.001 | 75 (62, 88) | 60 (51, 69) | <0.001 | 23 (17, 29) | 27 (18, 36) | 0.02 |
| Adult | 32 (32, 33) | 30 (29, 30) | <0.001 | 758 (704, 795) | 643 (593, 697) | <0.001 | -- | -- | -- |
Figure 1:
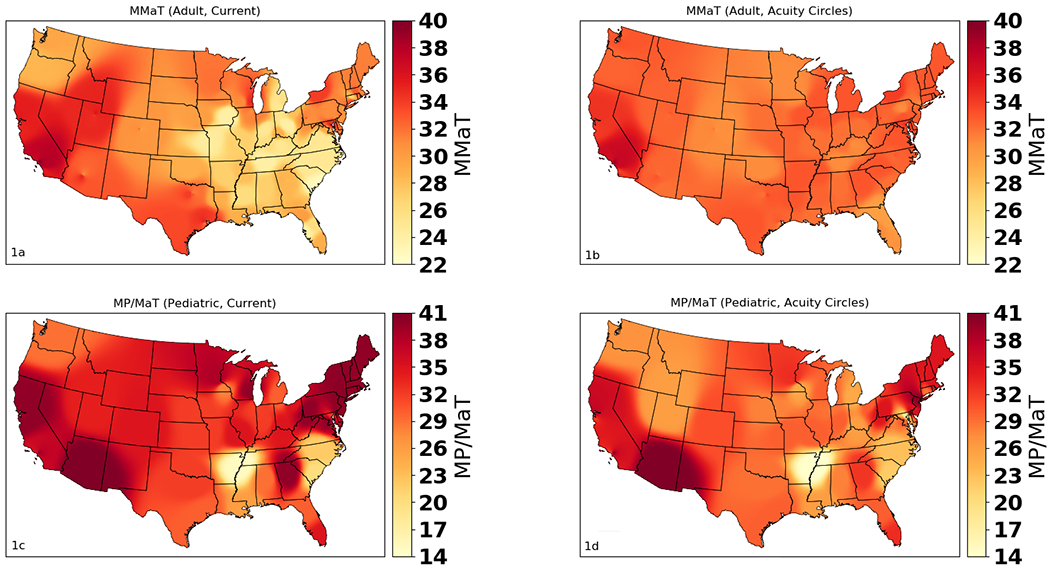
Distribution of Median MELD at Transplant (MMaT) or Median PELD/MELD at Transplant (MP/MaT) for (a) adults under the current DSA/Region-based system, (b) adults under proposed acuity circles, (c) pediatric candidates under the current DSA/Region-based system, and (d) pediatric candidates under proposed acuity circles
Distribution of deceased-donor livers
Acuity circle allocation is projected to increase the overall percentage of pediatric deceased-donor organs being transplanted into pediatric candidates (77% vs 46%; P < 0.001) with an increase observed in infants (15% vs 13%; P=0.002), children (24% vs 17%; P < 0.001) and more than doubling for teenagers (38% vs 15%; P < 0.001).
Days on the liver transplant waitlist
Median days on the waitlist is projected to decrease for infants (29 vs 42; P < 0.001), children (45 vs 70; P < 0.001) and teenagers (45 vs 57; P = 0.004; Table S2). In addition, median days on the waitlist would decrease for adults under acuity circle allocation (84 vs 89; P < 0.001).
Travel distance for deceased-donor livers
Using acuity circle allocation, the median transport distance in nautical miles is projected to increase for all age groups including infants (403 vs 236; P < 0.001), children (395 vs 231; P < 0.001), teenagers (359 vs 125; P < 0.001) and adults (215 vs 92; P < 0.001; Table S3).
Posttransplant survival
The proportion of transplant recipients surviving 1 year after transplant is not projected to change under acuity circle allocation for infants (86% vs 85%; P = 0.06) and children (89% vs 88%; P = 0.1) but would increase very slightly for teenagers (89% vs 87%; P = 0.01).
DISCUSSION
This LSAM analysis demonstrates that the approved acuity circle allocation is likely to improve outcomes for pediatric liver transplant candidates of all age groups, by decreasing waitlist mortality and increasing number of transplants. It would significantly increase the percentage of pediatric donor livers that are transplanted into pediatric candidates, from less than 50% to more than 75%. Acuity circle allocation also leads to pediatric candidates being transplanted at lower PELD/MELD scores and with fewer children as Status 1B, suggesting that pediatric candidates would be transplanted earlier and before their illness severity progressed to more life-threatening levels. All age groups had shorter waitlist times. Despite the benefits of acuity circle allocation, it is important to note that geographic disparities for pediatric candidates would continue to persist, and likely exceed variability in adults, suggesting the former are more susceptible to center/regional variations in donor availability, listing practices and use of technical-variant or marginal grafts.
Currently, pediatric candidates less than 1 year of age at listing experience the highest waitlist mortality for any age group. Specifically, the recent SRTR report indicates that this group has a waitlist mortality of 20 deaths per 100 patient-years, compared to 13 deaths per 100 patient-years for all adults, and is even higher than for elderly (i.e., over 65 years) candidates (18 deaths per 100 patient-years).4 This suggests a life-threatening disadvantage for these young candidates in accessing deceased-donor livers within our current allocation system. Furthermore, an analysis of the 90-day waitlist mortality for pediatric candidates on the liver transplant waitlist suggested that the current PELD score underestimates the actual risk of death by 17%, putting pediatric candidates at a disadvantage compared to adults.5
Although it has been widely reported and discussed that our current allocation system falls short of its Final Rule and NOTA’s requirements, and despite several attempts by UNOS committees to make the system more equitable, little progress has been made in abating this disparity. For example, a 2015 white paper entitled “The Ethical Principles of Pediatric Organ Allocation” by the Pediatrics and Ethics Committees of UNOS delineated 4 key principles that support the prioritization of pediatric candidates and include: (1) the prudential allocation of healthcare resources over the lifespan of the individual; (2) the fair innings principle; (3) the “maximin principle;” and (4) utility.14 Despite these foundational principles being defined and often implemented in other global communities, no substantial changes have been made to the U.S. allocation system in the intervening years.15 Our analysis highlights that acuity circle allocation would “recognize differences in health and in organ transplantation between children and adults” and incorporate “procedures that address the unique health care needs of children” more appropriately than the current system. It would reduce mortality and likely morbidity for infants, children, and teenagers—without increasing mortality for adult candidates.
An additional important outcome of acuity circle allocation is a substantial increase in the percentage of pediatric deceased-donor livers that are transplanted into pediatric candidates instead of adults. This can be attributed to an allocation policy created with the intention to prioritize pediatric waitlist candidates for pediatric deceased donor livers. While the DSA/Region-based allocation system attempts to direct pediatric deceased-donor organs towards pediatric candidates, Hsu et al. reported—and this is supported by our LSAM simulation—that nearly half of these organs are transplanted into adults. A quarter of pediatric donor livers are never offered to any pediatric candidate.3 This disparity occurs because, in many instances, there is not a pediatric candidate within the DSA/Region with sufficient priority to be allocated the organ. However, our simulation demonstrates that there are likely pediatric candidates within a feasible distance from the donor hospital that would benefit from these pediatric organs.
While the broader sharing under acuity circle allocation would likely increase pediatric deceased-donor organs available for pediatric candidates, it does not prioritize national sharing of organs for the sickest individuals. We recently proposed a scheme, SharePeds, that prioritized national sharing of these organs within the existing DSA/Region-based framework for high acuity pediatric candidates that demonstrated superior outcomes relative to the traditional allocation scheme.16 Continued exploration of the impact of prioritizing national sharing for this population is critical to optimize equity and disparity reduction in the system.
One limitation of our analysis is that LSAM cannot predict how increased allocation of deceased-donor organs to pediatric candidates would increase split liver transplantation—and the potential for more deceased donor organs being transplanted into 2 recipients. Many grafts allocated for pediatric candidates are split because they are larger than needed for that candidate. There is growing recognition that outcomes following split liver transplantation are similar to whole deceased-donor grafts.17–20 Several studies have identified that these grafts are insufficiently used, and would likely have positive effects in transplant rates and mortality.21,22 It is conceivable then that increased splitting would occur under the acuity circles scheme, and would subsequently yield grafts for adult recipients in the majority of instances. A second limitation of LSAM is that it cannot model changes in behavior, such as a center’s decision to accept/decline an offer, which may change over different allocation schemes.
Acuity circle allocation scheme would represent an important step towards eliminating disparities faced by infants, children and teenagers in need of a liver transplant. After implementation, it will be important to empirically verify that this scheme does accomplish disparity reduction as projected, and to continue to investigate and address persistent disparities for pediatric candidates to optimize outcomes for these vulnerable children. Likewise, the impact of acuity circles on geographic variability in allocation for pediatric candidates should continue to be evaluated to make sure significant disparities don’t persist. Ongoing work will be necessary to ensure that the youngest and most vulnerable candidates do not continue to die on the waitlist at high rates, and that any liver allocation policies moving forward must incorporate prioritizing pediatric recipients listed nationally for livers from pediatric donors.
Supplementary Material
Acknowledgments
Disclosure and sources of funding: The authors declare no conflicts of interest. This work was supported by the Society for Pediatric Liver Transplantation, Agency for Healthcare Research and Quality (Dr. Mogul, K08 HS023876), and the National Institutes of Health (Dr. Perito, K23 DK0990253; Dr. Gentry R01 DK111233). The interpretation and reporting of these data are the responsibility of the author(s) and in no way should be seen as an official policy of or interpretation by the Organ Procurement and Transplantation Network or the U.S. Government. The content is the responsibility of the authors alone and does not necessarily reflect the views or policies of the NIH or the Department of Health and Human Services, nor does mention of trade names, commercial products, or organizations imply endorsement by the U.S. Government.
REFERENCES
- 1.National Organ Transplant Act. Pub L No. 98–507, 98 STAT. 2339. 1984. Available at https://www.govinfo.gov/content/pkg/STATUTE-98/pdf/STATUTE-98-Pg2339.pdf Accessed July 3, 2019.
- 2.Institute of Medicine, Committee on Organ Procurement and Transplantation Policy, Division of Health Sciences Policy. Organ Procurement and Transplantation: Assessing Current Policies and the Potential Impact of the DHHS Final Rule. Washington DC: National Academies Press; 1999. 10.17226/9628. [DOI] [PubMed] [Google Scholar]
- 3.Hsu EK, Shaffer ML, Gao L, et al. Analysis of liver offers to pediatric candidates on the transplant wait list. Gastroenterology. 2017;153(4):988–995. doi: 10.1053/j.gastro.2017.06.053 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kim WR, Lake JR, Smith JM, et al. OPTN/SRTR 2017 annual data report: liver. Am J Transplant. 2019;19 Suppl 2:184–283. doi: 10.1111/ajt.15276 [DOI] [PubMed] [Google Scholar]
- 5.Chang CH, Bryce CL, Shneider BL, et al. Accuracy of the pediatric end-stage liver disease score in estimating pretransplant mortality among pediatric liver transplant candidates. JAMA Pediatr. 2018;172(11):1070–1077. doi: 10.1001/jamapediatrics.2018.2541 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Yeh H, Smoot E, Schoenfeld DA, et al. Geographic inequity in access to livers for transplantation. Transplantation. 2011;91(4):479–486. doi: 10.1097/TP.0b013e3182066275 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bowring MG, Zhou S, Chow EKH, et al. Geographic disparity in deceased-donor liver transplant rates following Share 35. Transplantation. 2019;103(10):2113–2120. doi: 10.1097/TP.0000000000002643 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gentry SE, Massie AB, Cheek SW, et al. Addressing geographic disparities in liver transplantation through redistricting. Am J Transplant. 2013;13(8):2052–2058. doi: 10.1111/ajt.12301 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.OPTN/UNOS Liver and Intestine Transplantation Committee. Liver and Intestine Distribution Using Distance from Donor Hospital. Bethesda, MD: National Institutes of Health; 2018. Available at https://optn.transplant.hrsa.gov/media/2766/liver_boardreport_201812.pdf Accessed July 3, 2019. [Google Scholar]
- 10.Weaver T, Schladt D, Pyke J, et al. Analysis Report: Data Request on Circle Based Allocation. Minneapolis, MN: Scientific Registry of Transplant Recipients; 2018. Available at https://optn.transplant.hrsa.gov/media/2640/li2018_01_analysis-report_20180924.pdf Accessed July 3, 2019. [Google Scholar]
- 11.Thompson D, Waisanen L, Wolfe R, et al. Simulating the allocation of organs for transplantation. Health Care Manag Sci. 2004;7(4):331–338. [DOI] [PubMed] [Google Scholar]
- 12.Massie AB, Kucirka LM, Segev, DL. Big data in organ transplantation: registries and administrative claims. Am J Transplant. 2014;14(8):1723–1730. doi: 10.1111/ajt.12777 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.OPTN: Organ Procurement and Transplantation Network. OPTN Policies. Bethesda, MD: National Institutes of Health; 2019. Available at https://optn.transplant.hrsa.gov/media/1200/optn_policies.pdf#nameddest=Policy_09 Accessed July 3, 2019. [Google Scholar]
- 14.OPTN: Organ Procurement and Transplantation Network. Ethics: Ethical principles of pediatric organ allocation. Available at https://optn.transplant.hrsa.gov/resources/ethics/ Accessed July 9, 2019.
- 15.Hsu EK, Mazariegos GV. Global lessons in graft type and pediatric liver allocation: a path toward improving outcomes and eliminating wait-list mortality. Liver Transpl. 2017;23(1):86–95. doi: 10.1002/lt.24646 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Perito ER, Mogul DB, VanDerwerken D, et al. The impact of increased allocation priority for children awaiting liver transplant: a liver simulated allocation model (LSAM) analysis. J Pediatr Gastroenterol Nutr. 2019;68(4):472–479. doi: 10.1097/MPG.0000000000002287 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Mogul DB, Luo X, Bowring MG, et al. Fifteen-year trends in pediatric liver transplants: split, whole deceased, and living donor grafts. J Pediatr. 2018;196:148–153.e2. doi: 10.1016/j.jpeds.2017.11.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sasaki K, Firl DJ, McVey JC, et al. Elevated risk of split-liver grafts in adult liver transplantation: statistical artifact or nature of the beast? Liver Transpl. 2019;25(5):741–751. doi: 10.1002/lt.25409 [DOI] [PubMed] [Google Scholar]
- 19.Ge J, Lai JC. Split-liver allocation: an underused opportunity to expand access to liver transplantation. Liver Transpl. 2019;25(5):690–691. doi: 10.1002/lt.25458 [DOI] [PubMed] [Google Scholar]
- 20.Kim HB, Vakili K. To split or not to split? That is no longer the question. J Pediatr. 2018;196:12–13. doi: 10.1016/j.jpeds.2017.12.019 [DOI] [PubMed] [Google Scholar]
- 21.Perito ER, Roll G, Dodge JL, et al. Split liver transplantation and pediatric waitlist mortality in the United States: potential for improvement. Transplantation. 2019;103(3):552–557. doi: 10.1097/TP.0000000000002249 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Valentino PL, Emre S, Geliang G, et al. Frequency of whole-organ in lieu of split-liver transplantation over the last decade: children experienced increased wait time and death. Am J Transplant. 2019;19(11):3114–3123. doi: 10.1111/ajt.15481 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.