

The outbreak of severe pneumonia due to the new SARS‐CoV‐2 has created a world emergency that is putting global public health institutions at high alert. Since the first official paper on January 20 up to now more than 10 000 publications have appeared on PubMed. Surprisingly, no single paper has been dealing with the potential impact of the COVID‐19 on Down syndrome (DS).
As COVID‐19 presents as an acute severe respiratory syndrome and DS is by far the most frequent chromosomal disease with the highest susceptibility to develop respiratory infections and complications, 1 it seems timely to focus on this syndrome during the ongoing pandemic.
DS represents a global problem with more than 5.5 million affected persons, 1:700 cases live births and a 30% increase in the last decades. Likewise, the life expectancy is increasing by the years and quite a number of subjects reach the adult life. 1
The paediatric age in general seems to be less affected by COVID‐19. 2 However, children with DS are especially vulnerable and susceptible to respiratory infections. In addition, they have comorbidities such as immunodeficiency, cardiopathies especially those with surgical valve replacement, obesity, diabetes that have been proven to worsen the outcome of COVID‐19 patients. 3
Presently, there are no official reports on the incidence and evolution of COVID‐19 in DS. The Journal Virtual Revista Sindrome de Down has mentioned cases of COVID‐19 in patients with DS with a variable evolution, from recovery to death. The Trisomy 21 Research Society is evaluating the evolution of the pandemic in patients with DS in order to answer to two main questions: (a) are subjects with DS more susceptible to COVID‐19 infection? (b) are they, once infected, at higher risk for complications than the typical population?
In the absence of an effective vaccine and of specific antiviral drugs, so far, the COVID‐19 treatment remains empiric. Nevertheless, progresses have been made by rationalising the treatment with the combination of drugs to prevent or cure the complications, such as antivirals (remdesivir), anti‐inflammatory (chloroquine, azithromicin) and anticoagulants. 4
At present time, DS undergoes the same control and prevention measures established by the Public Health Services (PHSs) worldwide. The main recommendations consist in social distancing, use of protective facemasks and gloves, frequent washing of hands and disinfection of both hands and environments. Unnecessary exposure should be avoided and non‐authorised persons should stay at home either as prophylaxis or in quarantine. In extreme conditions, the lockdown can be established.
The pandemic scenario raises major worries for families of children with DS for several reasons. In about 40% of the families, one member (mostly parents) had stopped working long before, while others, unless locked‐down, work outside and return home, thus being at potential risk of spreading contagion. On the other hand, lifestyle and rhythms are disrupted by the loss of supports to the families because of the educational and family network isolation and because subjects with DS are usually thriving at school and by visiting relatives, especially grandparents.
Generally speaking, the main lines of recommendations for individuals with DS are practically identical to what is recommended for others, although details may differ from one country to another.
The absence of information about how the disease affects this group of subjects is a limiting factor to further discussing about the specific risk towards COVID‐19.
For that reason, the DS Center of Bambino Gesù Children Hospital has undertaken practical initiatives with special regard to the medical approach of COVID‐19 in vulnerable, medical compromised, immune‐deficient children in general.
The Center had been founded in 2013 and today is following up 763 subjects (gender distribution: 58.9% males; mean age: 7.45 years (SD 5.49, range 0‐21).
A booklet containing exhaustive information about the syndrome had been made available to families and to the Italian Down Syndrome Association (aidp@aipd.it). (http://www.ospedalepediricobambinogesu.it/la‐guida‐alla‐sindrome‐di‐down‐di‐a‐scuola‐di‐salute#.XniOidNKhmA).
By the appearance of the coronavirus infection in Italy, we have predisposed an ad hoc protocol.
The protocol contains instructions related to the importance for children with DS of having earlier access to diagnostic tests and antiviral management, especially in states of immune dysfunction, recurrent pulmonary infections, congenital heart disease and obesity.
With regard to the RT‐PCR test, it is suggested to perform the test on saliva spitted into a sterile bottle instead of on oropharyngeal mucosa brushing. Saliva testing is easy, safe, non‐invasive and equally suitable. 5
A special recommendation to families is that of informing the primary care Doctors and/or the DS Center about suspicious symptoms in order to activate the paths synthesised in a dedicated flow chart (Figure 1). A special alert is addressed to domestic accidents in order to avoid access to Hospital Emergency Departments or unnecessary hospitalisation. The possible admission into an intensive care unit (ICU) becomes a source of special concern.
Figure 1.
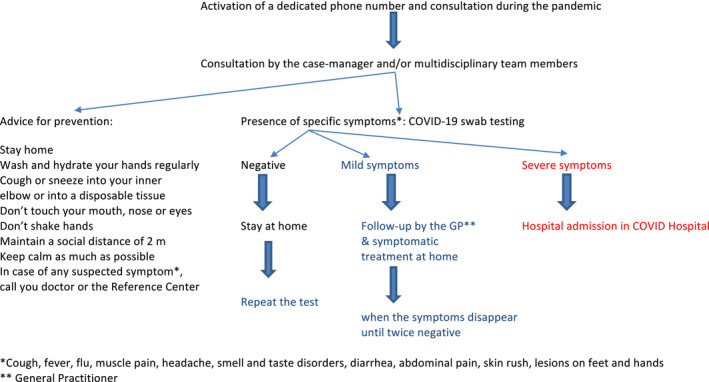
Down syndrome and pandemic COVID‐19 Flow chart: synthesis of the content of the dedicated page at the website of Bambino Gesù Children's Hospital (see text)
Furthermore, the Center, upon request, provides caregivers of children with DS with audio‐visual consultation for any question or as a kind of preliminary triage and stays at disposal of primary care doctors who have received a printed notice as a reminding.
CONFLICT OF INTEREST
None.
REFERENCES
- 1. Valentini D, Di Camillo C, Mirante N, et al. Effects of Pidotimod on recurrent respiratory infections in children with Down syndrome: a retrospective Italian study. Ital J Pediatr. 2020;46:31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Brodin P. Why is COVID‐19 so mild in children? Acta Paediatr. 2020;109:1082‐1083. [DOI] [PubMed] [Google Scholar]
- 3. Siordia JA Jr. Epidemiology and clinical features of COVID‐19: a review of current literature. J Clin Virol. 2020;127:104357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Anonymous . Some drugs for COVID‐19. Med Lett Drugs Ther. 2020;62:49‐50. [PubMed] [Google Scholar]
- 5. Sri Santosh T, Parmar R, Anand H, Srikanth K, Saritha M. A review of salivary diagnostics and its potential implication in detection of COVID‐19. Cureus. 2020;12:e7708. [DOI] [PMC free article] [PubMed] [Google Scholar]