

Short abstract
See related Reply
To the Editors:We read the Letter from China by Guan and Zhong regarding coronavirus disease 2019 (COVID‐19) with immense interest, as it provided novel insight into this catastrophic pandemic. 1 COVID‐19 hotspots until February 2020 were East‐Asian cities including Wuhan (China) and Yokohama (Japan) where the cruise ship Diamond Princess harboured. The mortality rate in Asia‐Pacific countries increased at a slower rate until mid‐April compared to some Euro‐American countries. 2 Notably, COVID‐19 high‐burden countries in Western Europe and North America, such as Italy, Belgium, the Netherlands, the United States, Spain, France, the United Kingdom and Switzerland, do not currently recommend universal Bacillus Calmette–Guérin (BCG) vaccination because tuberculosis is not highly prevalent. 3 BCG induces trained immunity (innate immune memory) by non‐specific cross‐protection against non‐tuberculous pathogens. 4 Therefore, some researchers believe that people vaccinated with BCG have some immune protection to severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2). Nevertheless, other researchers counter that this association can be explained by confounding factors including the abundant medical resources of the COVID‐19 high‐burden countries. To reduce this confounding effect, we compared population‐based mortality from COVID‐19 using data of only World Bank‐defined high‐income countries. 2 , 5
The high‐income countries and regions were classified into two groups based on national policies regarding universal BCG vaccination 3 : ‘Currently Recommended Countries (CRC)’ and ‘Currently Not Recommended Countries (CNRC)’. CNRC were further divided into ‘Never Recommended Countries’ and ‘Previously Recommended Countries’ 3 (Fig. 1).
Figure 1.
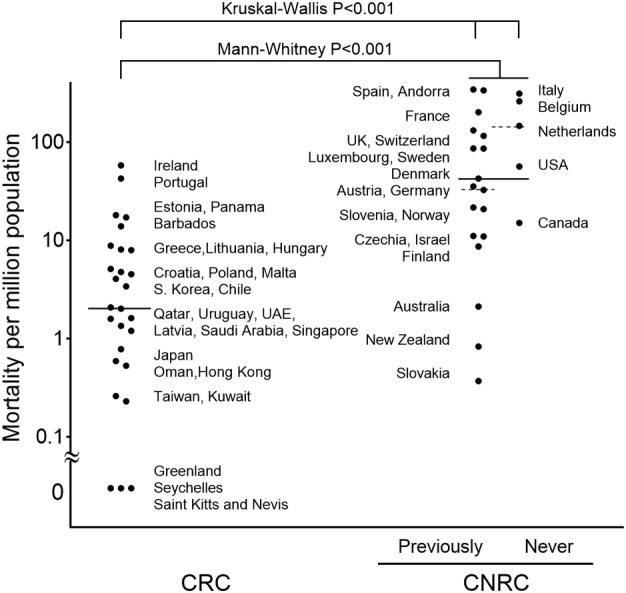
Mortality differences between Currently Recommended Countries (CRC) and Currently Not Recommended Countries (CNRC). Country‐level median values were calculated regardless of population size. Mann–Whitney test was used for two‐group comparison and the Kruskal–Wallis test was used for three‐group comparison. Previously, Previously Recommended Countries; Never, Never Recommended Countries; solid bar, median mortality among CRC and CNRC; broken bar, median mortality among Previously Recommended countries and Never Recommended countries.
We analysed mortality data from 27 CRC and 23 CNRC. All CRC provide the first BCG shot at birth except for Greece (6 years), Malta (school age) and Barbados (5–6 years). Median mortality per one million population for CRC was significantly lower than that for CNRC (2.1 (interquartile range (IQR): 0.7–8.0) vs 42.6 (IQR: 13.1–139.3), Mann–Whitney P < 0.001; Fig. 1). Mortality rates significantly differed between the three groups (Kruskal–Wallis P < 0.001; Fig. 1). The highest median mortality of 146.5 (IQR: 56.6–260.5) was found in the Never Recommended Countries, followed by 34.0 (IQR: 11.0–108.4) in the Previously Recommended Countries and 2.1 (IQR: 0.7–8.0) in the CRC.
Guan and Zhong called for active prevention measures to combat the current global pandemic. 1 National policies for paediatric universal BCG vaccination possibly contribute to reducing COVID‐19‐related mortality. We expect that ongoing randomized trials will confirm the role of BCG vaccination in preventing COVID‐19‐related death.
REFERENCES
- 1. Guan WJ, Zhong NS. Letter from China. Respirology 2020; 25: 657–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Worldometer . Worldmeter COVID‐19 coronavirus pandemic. [Accessed 10 Apr 2020.] Available from URL: https://www.worldometers.info/coronavirus/
- 3. The BCG Atlas Team . The BCG World Atlas, 2nd edn. [Accessed 10 Apr 2020.] Available from URL: [http://www.bcgatlas.org/
- 4. Netea MG, Joosten LA, Latz E, Mills KH, Natoli G, Stunnenberg HG, O'Neill LA, Xavier RJ. Trained immunity: a program of innate immune memory in health and disease. Science 2016; 352: aaf1098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. The World Bank . World Bank Country and Lending Groups. [Accessed 10 Apr 2020.] Available from URL: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups
Ebina‐Shibuya R, Horita N, Namkoong H, Kaneko T. National policies for paediatric universal BCG vaccination were associated with decreased mortality due to COVID‐19. Respirology. 2020;25:898–899. 10.1111/resp.13885