

Abstract
Renal metastases are uncommon in clinical practice, even as autopsy reports much frequent cases în disseminated tumors. Usually multiple and bilateral, they can determine many problems of differential diagnosis in case of solitary renal mass, when a primary kidney neoplasm must be excluded. Main sources are represented by the tumors of the lung, breast, digestive tract, melanomas and lymphomas, but rare cases with other etiology have been reported. Imaging can help to the diagnosis; CT scan, MRI, transabdominal ultrasound and sometimes contrast enhanced ultrasound can be useful. The treatment is individualized by the general status, by other organs involved and by the control of primary tumors; nephrectomy can be made in cases with unsure diagnosis and if primary tumor is controlled.
Keywords: renal metastases, lung tumor, renal carcinoma, contrast enhanced ultrasound
Introduction
Secondary tumors of the kidney are rather uncommon in clinical practice [1], although renal blood flow represents approximately 20% of cardiac output. The incidence in autopsy series is estimated between 2,36-12,6% of patients with metastatic tumors [2], but clinical detected renal metastases have a much lower prevalence. Improvements in oncologic therapy and increased access to imaging techniques (especially CT scan and MRI) were correlated to an increasing number of reported kidney metastases into the literature [2].
Etiology
Renal metastases are originated mainly from lung, breast, digestive organs (especially esophagus, stomach and colon) and melanoma [3,4].
Most patients have no metastasis to the kidney at the moment of the diagnosis (69,5%), and 80% develop metastasis to the other organs during evolution [2], sometimes several years after primary tumor identification or even after removal of the original tumor [5,6,7]. Rarely, renal metastases are discovered prior to primary site tumor [8]. Some cases with solitary metastatic renal mass and multiple metastases were also reported and determine difficulties of differential diagnosis [9,10].
The lung represents the main source for kidney metastasis in most studies; the prevalence of pulmonary tumors as a cause of renal metastasis is estimated at 19,8-23,3% in one study [4] and at 43,7% in another [2].
All pathological types of tumors can be implied [1,2,5,6,7,11,12,13,14,15,16,17,18,19]; in a study 57,6% have squamous cell carcinoma, 28,8% have adenocarcinoma and 5,1% small-cell lung carcinoma [1]. Most cases of lung carcinoma with renal metastases have concomitant metastases located to the liver, bones and adrenal glands. In a series of 146 patients with lung carcinoma, renal metastases represent only 1,4% of total metastases [16]. A rare case of localized mesothelioma with renal metastasis was also described [20].
Digestive tumors represent another possible source of renal metastases. Esophageal carcinoma [21,22,23,24] can metastasize into the lung, liver, bones and adrenal gland [23]. Renal metastases are the 5th place by clinical frequency [21], although one study showed that in autopsy series 12-13% of esophageal carcinomas have renal metastases [23]. Survival is limited in most cases [24]. Gastric carcinoma represents another potential source for renal metastases, with a frequency of 11,1-15,1% of total cases with renal metastases [4]. Colo-rectal tumors [25,26,27] represent 10,6-22,2% of cases with renal metastases [2,4]; metastases into the kidney were found only in 2.7% of autopsy cases, being also associated with unfavorable prognosis [26]. Pancreatic tumors rarely metastasize to the kidney; the route is usually haematogenic but an invasion to the adjacent left kidney is also possible [28]. Hepatocellular carcinoma is exceptionally associated with renal metastasis; in 2012 less than 15 cases were published [29]. In case of solitary renal lesion [30] the main differential diagnosis must be with renal carcinoma with liver metastases. a case of hepatic epithelioid angiomyolipoma with renal metastasis was noted [31] and a case of rupture of renal metastasis from hepatocellular carcinoma was also reported [32].
Renal metastases produced by thyroid tumors are rare. 1,4-6% of differentiated thyroid carcinomas have distant metastases, mainly in bone (43%), lung (40%) and mediastinum (32%). In autopsy series a frequency of 5.9-7.1% was estimated [33]. The prevalence in clinical series varies between 0.47% [34] and 5.3% [2]. Multiple cases were reported into the literature [2,8,9,10,33,34,35,36,37,38,39], usually in cases with extensive multiple site metastases [35].
Follicular carcinoma is the most aggressive, the most frequent sites for metastasis are lung, bone, less frequent brain, liver, skin, kidney and adrenal glands [36]. The main path of dissemination is haematogenic, possibly related to the presence of minor venous and/or lymphatic collaterals between thyroid gland and kidney [36].
Breast carcinoma represents another potential source for renal metastasis, with a prevalence estimated between 5.3% [2] and 12.3% [4].
Genital cancers can represent another source of renal metastasis. Prostate carcinoma is an uncommon cause of renal metastases; only few cases were reported [40,41], and all cases involved left kidney. Cervical carcinoma is exceptionally implied in renal metastasis [42,43,44] in 2017 less than 13 cases were reported.
Autopsy series estimated a 2.5% [42]. Some cases of renal metastases from uterine leiomyosarcoma, serous carcinoma or from ovarian granulosa cell tumour were also reported [45,46,47].
In patients diagnosed with lymphoma, renal involvement is noted in 34-60% of cases [48] and is represented by multiple, small masses, without capsula. A renal invasion from retroperitoneal disease is noted in 25-30% [48]. Usually there is no mass effect to the vessels or pelvicalyceal system [48]. Melanoma has a prevalence of 14.8% as a source for renal metastases in a study [4].
Several other causes of renal metastases have been reported into the literature, mostly as case reports. Laryngeal tumors [49], salivary or sinonasal adenoid cystic tumors [2,4,50], osteogenic sarcoma [51], chondrosarcoma (probably from lung metastasis, 4-18 years after primary tumor) [52], leiomyosarcoma of the inferior vena cava (probably by renal vessel invasion) [53], neuroblastoma [54], meningeal haemangiopericytoma [55], solitary fibrous tumor [56] have been described as a source for renal metastases. Soft tissue tumors can be a cause of renal metastasis in 5.3% [2] and a case of Merkel cell carcinoma of the skin with renal secondary lesions has been also reported [57]. The cause remains unknown in up to 5.3% [2].
Pathogeny
The mechanism of tumoral metastasis is based by sequential processes of shedding, adhesion, penetration, migration and proliferation of malignant cells originating from a primary malignant tumor [13]; the circulating malignant cells tend to seed in selected organs [13]. The exact mechanism by which various tumors can metastase to the kidney is not precisely known. The lung is especially important because any tumoral cells which detach from primary tumor can go to the arterial circulation and go directly to the kidney. The fact that kidneys are not the main target for metastases in lung tumors suggests that kidneys didn’t have a particular affinity for metastases. Other mechanisms may involve multiple step metastasis when tumoral cells disseminate to the kidney after they invade another organ of tissue (for instance a tumor generates pulmonary metastases and tumoral cells detach from the lung and go to the kidney); this process is known as ”metastasis from metastasis”. Sometimes detached tumoral cells can skip one organ and go directly to another organ. A “seed and soil” hypothesis proposed an organ-preference pattern where some metastases are the product of a favorable interaction between metastatic tumor cells (the “seed”) and their organ microenvironment (the “soil”) [13,58,59].
The detached tumor cells have receptors which bind specifically to the endothelial cells of some organs because of special chemotactic factors (seed) and are attracted preferentially to the target cells (soil). The anatomical particularities of primary site of the tumor are important; the metastasis can be made from primary tumor (lung to the kidney via aorta and kidney arteries), from other secondary site or from lymph nodes.
A particular relation between renal vascularization and another tissue vascularisation can explain some of the renal metastases; minor venous or lymphatic collaterals between thyroid and kidneys have been reported as a possible cause.
Clinical signs
Renal metastases can be unilateral or bilateral, solitary or multifocal [2]. The most frequent symptoms were abdominal or flank pain, hematuria, weight loss, sweats and fever [2,11], but most patients with renal metastases have no specific symptoms [11]. In a series of 64 cases of lung tumors with renal metastases, 50% have hematuria [1].
Imaging
Renal metastases can be diagnosed by transabdominal ultrasound, by CT or IRM [2,11]; sometimes PET-CT [11] or contrast-enhanced ultrasound can be useful. Imaging can usually differentiate between a primary or secondary renal tumor [11]. Sometimes a diffuse enlarged kidney without a clear mass in patients with primary known tumor can suggest renal metastasis [7].
Ultrasound examination may suggest the diagnosis of renal metastases [48]. In case of solid multiple metastases ultrasound can show multiple, usually 1 to 3cm hypoechoic masses, with no capsula, not totally spherical, sometimes wedge-shaped or diffuse renal infiltration. The absence of mass effect to the vessels or pelvicalyceal system is usually noted [48]. The aspect in kidney involvement by lymphoma can be similar, and sometimes renal invasion from retroperitoneal disease is noted [48]. Cases with unilateral or solitary lesions can easily be confounded with renal primary carcinoma. Contrast-Enhanced ultrasound (CEUS) showed in both types of metastases hypo/ isoenhancement in early cortico-medullary phase with early washout. Hypovascular aspect is recorded in more than 80% of renal metastases [48,60].
At CT scan renal metastases are usually multifocal or endophytic [15], isodense or with low attenuation compared with renal parenchyma and only slightly enhancement with contrast [3,11,18], while a solitary lesion, with necrosis or cystic component, with arterial hyperenhancement, well defined margins and renal vein thrombosis suggest primary tumor [18]. Most renal metastases are slightly enhanced [4], more enhanced in venous than in arterial phase [4].
18F-FDG PET features of metastatic renal tumors are rarely reported: high uptake in [4], the main difficulty is related to the physiological excretion of radiotracer through urinary tract, which may interfere with tumor imaging [18].
The sensitivity and specificity of 18F-FDG PECT-CT in detecting renal tumors are 60% and 100% respectively [18]. 131-I-Whole Body Scan can help in cases associated with thyroid carcinomas [35,38].
Urine analysis can show hematuria but this is not a mandatory sign. Percutaneous biopsy of renal mass can help to the diagnosis [20], and immunohistochemistry is useful in difficult cases [17].
Differential diagnosis
The differential diagnosis of renal masses includes renal cell carcinoma, transitional cell carcinoma of renal pelvis, squamous cell carcinoma of the kidney, renal lymphomas and sarcomas and secondary tumors [20]. The presence of a renal mass in a patient with known malignancy doesn’t suggest always a secondary tumor. A study published by Patel et al [61] who used CT scan for the diagnosis has showed that in 36 cases of renal masses in patients with other primary malignancy 21 were metastases and 15 were synchronous renal carcinomas. The enhancement pattern at CT examination (hypo or hyperenhancement) was similar, but renal metastases have more frequently an solid endophytic appearance and were multiple or bilateral. Biopsy can be useful is case of doubt and nephrectomy can be recommended for both diagnostic and therapeutic reasons in selected cases. Kidney was the eighth site of metastasis by frequency [61].
Treatment
No clear guideline is available for management of renal secondary tumors [11,15]; chemotherapy guided to the primary tumor can be useful, although results are usually poor [3]; nephrectomy can be made in unilateral cases with no other metastases [3] when primary tumor is also controlled) [15]; stereotactic body radiation has been suggested in some cases associated with non-small cell lung carcinoma [11,15,19]. Factors related to favorable outcome are control of the primary site, good performance status, metachronous lesions and longer disease-free interval [1].
Case report
We present a case of a 50th year old woman who was admitted in our clinic for upper dysphagia, nausea, cough and weight loss of over 44 pounds in the last 6 months. At clinical examination we noted a severe malnutrition, no palpable lymph nodes, digital clubbing and pain at the palpation of the upper abdomen. No urinary complains were recorded.
Abdominal ultrasound reveals multiple, round, hypoechoic nodules with a maximum diameter located to the renal parenchyma with bilateral involvement (Figure 1), three hypoechoic nodules located inside the spleen (Figure 2) and multiple abdominal lymph nodes in the upper abdomen. No liver abnormalities were noted. A contrast examination with Sonovue was performed and showed no enhancement for renal and splenic nodules during arterial, venous and late phase which was suggestive for metastatic renal and splenic lesions (Figure 3 and 4).
Figure 1.
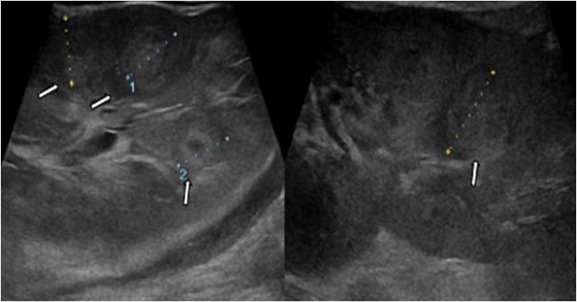
Ultrasound detected multiple hypoechogenic, round shaped, inhomogeneous renal mass (white arrow)
Figure 2.
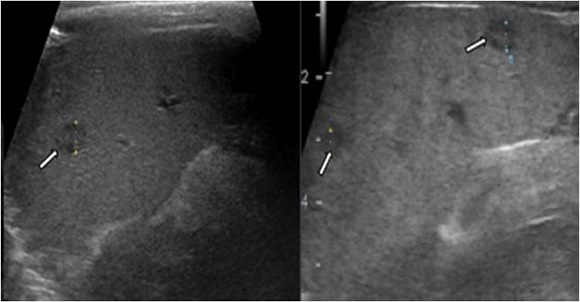
Grey scale sonography demonstrates multiple oval shaped, hypoechogenic and inhomogeneous lesions in the spleen (spleen metastases)
Figure 3.
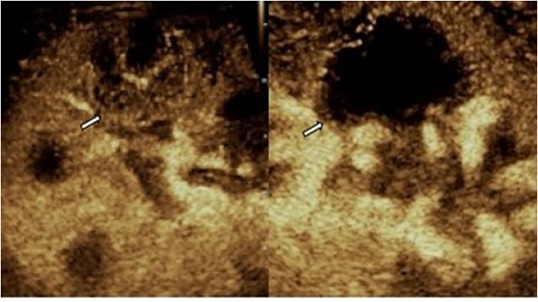
On CEUS scan in the corticomedullary phase, the renal lesion presents a slightly inhomogeneous enhancement with several necrotic areas. b. In venous phase, the lesion reveals no enhancement
Figure 4.
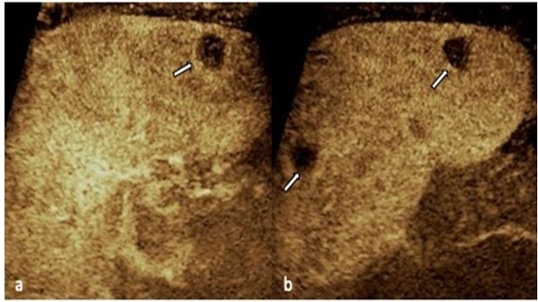
CEUS shows hypoenhancement of the lesion during the arterial phase. b. Asecond lesion can be seen in the parenchymal phase; both masses demonstrate washout appearance
CT scan showed a large, heterogenous mediastino-pulmonary mass, with encasement of aortic arch and descendent aorta, left pulmonary artery and left principal bronchia and compression of the esophagus and trachea (Figure 5). Two nodules inside the left pulmon, 18 and 8mm diameter were also noted. Multiple, bilateral, hypodense postcontrast nodules were seen in kidney and 3 nodules with a diameter of 22, 6 and 7mm respectively were noted inside the spleen (Figure 6). Bilateral suprarenal metastases were also recorded and multiple celiac, perigastric and para-aortic lymph nodes were also seen (Figure 7 and 8).
Figure 5.
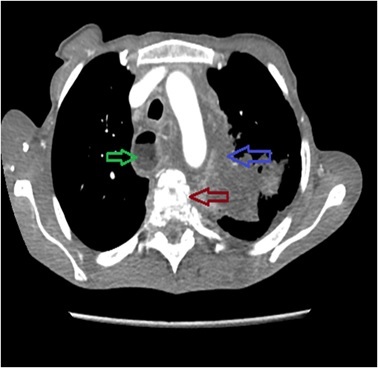
CT after contrast: mediastino-pulmonary mass (blue arrow), esophageal dilation (green arrow), osteolysis of vertebral body T5
Figure 6.
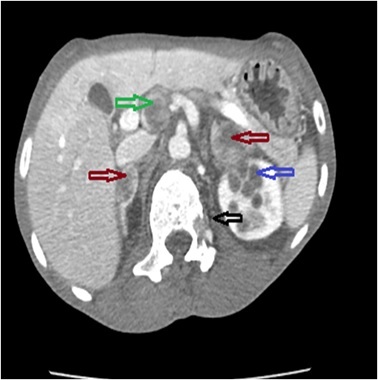
CT after contrast: hypoenhanced metastasis of adrenal glands (red arrow), kidney (blue arrow), lymph nodes (green arrow), osteolysis L1 (dark arrow)
Figure 7.
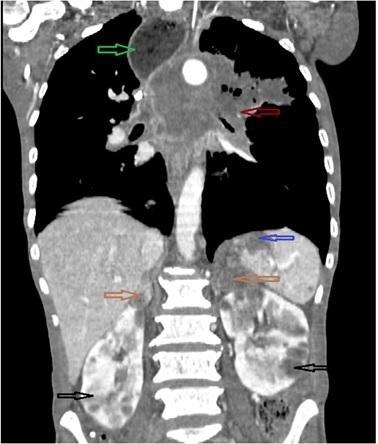
Reconstruction CT 3D in coronal plane, after contrast-heterogenous mediastino-pulmonary mass, with encasement of middle and posterior mediastinum, with important mass effect to esophagus (much enlarged); hypoenhanced metastases located to the spleen adrenal glands and both kidneys
Figure 8.
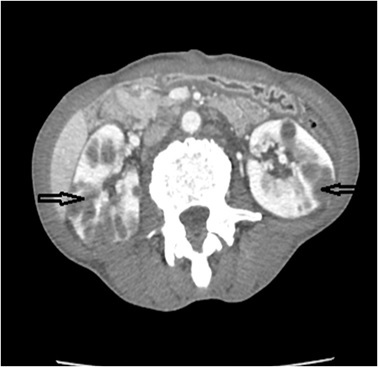
CT after contrast: bilateral, hypoenhanced metastasis of kidney (dark arrow)
The urine examination showed no abnormalities.
The patient refused esophagoscopy for esophageal wall evaluation and also bronchoscopy for evaluation of mediastino-pulmonary mass and requested discharge from the hospital because of rapid deterioration of general status.
We interpreted the case as a pulmonary tumor with mediastinal invasion and metastases to the kidneys, adrenal glands (bilateral), spleen and abdominal lymphnodes.
We could not confirm the results by pathology, as upper endoscopy and bronchoscopy were both rejected by the patient because of the altered general status.
Conclusions
Renal metastases are rarely seen in medical practice, cases manifested as solitary renal mass must be differentiated from primary renal carcinoma.
The main sources for renal metastases are tumors of the lung, breast, digestive tract, melanomas and lymphomas.
Diagnosis is based by the imaging exams (CT scan, MRI, ultrasound); contrast enhanced ultrasound can be useful for the diagnosis.
The treatment is the same as for primary tumor; nephrectomy can be an option in selected cases.
Acknowledgements
Larisa Daniela Sandulescu has a contribution equal to the first and the last author as principal author.
Financial interest
None
Conflict of interests
None to declare.
References
- 1.Tomita M, Ayabe T, Chosa E, Nakamura K. Isolated Renal Metastasis from Non-Small-Cell Lung Cancer: Report of 2 Cases. Case Rep Surg. 2015;2015:357481–357481. doi: 10.1155/2015/357481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Zhou C, Urbauer DL, Fellman BM, Tamboli P, Zhang M, Matin SF, Wood CG, Karam JA. Metastases to the kidney: a comprehensive analysis of 151 patients from a tertiary referral centre. BJU Int. 2016;117(5):775–782. doi: 10.1111/bju.13194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Adamy A, Von Bodman C, Ghoneim T, Favaretto RL, Bernstein M, Russo P. Solitary, isolated metastatic disease to the kidney: Memorial Sloan-Kettering Cancer Center experience. BJU Int. 2011;108(3):338–342. doi: 10.1111/j.1464-410X.2010.09771.x. [DOI] [PubMed] [Google Scholar]
- 4.Qiu DS, Xu LY, Hu XY. Imaging appearance of a singular metastatic adenoid cystic carcinoma of the right kidney: A case report and literature review. Oncol Lett. 2014;8(6):2669–2671. doi: 10.3892/ol.2014.2546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mulamalla K, Truskinovsky AM, Dudek AZ. Pulmonary blastoma with renal metastasis responds to sorafenib. J Thorac Oncol. 2007;2(4):344–347. doi: 10.1097/01.JTO.0000263719.76944.0a. [DOI] [PubMed] [Google Scholar]
- 6.Uemura M, Hirai T, Inoue H, Kanno N, Nishimura K, Mizutani S, Miyoshi S, Yoshida K, Kawano K, Matsumura A. Renal metastasis originating from pulmonary carcinoma: a case report. Hinyokika Kiyo. 2001;47(7):489–492. [PubMed] [Google Scholar]
- 7.Srisung W, Mankongpaisarnrung C, Warraich I, Sotello D, Yarbrough S, Laski M. Carcinoma of the lungs causing enlarged kidneys. Proc (Bayl Univ Med Cent) 2015;28(2):221–223. doi: 10.1080/08998280.2015.11929235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gao Y, Deng W, Chen Y, Fan Y, Guo Z. Renal metastases as the initial presentation of papillary thyroid carcinoma: A case report and literature review. Mol Clin Oncol. 2017;6(6):821–824. doi: 10.3892/mco.2017.1243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gezer E, Selek A, Tarkun İ, Cantürk Z, Çetinarslan B. Papillary thyroid carcinoma presenting as a primary renal tumor with multiple pulmonary and bone metastases: a case report. J Med Case Rep. 2019;13(1):95–95. doi: 10.1186/s13256-019-2025-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Nair LM, Anila KR, Sreekumar A, Pradeep VM. Renal metastasis from papillary carcinoma thyroid detected by whole body iodine scan: A case report and review of the literature. Indian J Nucl Med. 2016;31(3):232–234. doi: 10.4103/0972-3919.183618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Numan L, Asif S, Abughanimeh OK. Isolated Renal Metastasis from Primary Lung Squamous Cell Carcinoma with Synchronous Small Cell Lung Cancer. Cureus. 2019;11(6):e4891–e4891. doi: 10.7759/cureus.4891. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Fujii Y, Masuda M, Hirokawa M, Matsushita K, Hasegawa H. Bilateral renal metastases of lung adenoid cystic carcinom. Hinyokika Kiyo. 1991;37(10):1307–1311. [PubMed] [Google Scholar]
- 13.Cai J, Liang G, Cai Z, Yang T, Li S, Yang J. Isolated renal metastasis from squamous cell lung cancer. Multidiscip Respir Med. 2013;8(1):2–2. doi: 10.1186/2049-6958-8-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Shimizu Y, Iguchi T, Nitta Y, Machida Y, Kuratsukuri K, Kawashima H, Nakatani T. A Case of Pulmonary Pleomorphic Carcinoma With Renal Metastasis. Urol Case Rep. 2014;2(6):179–180. doi: 10.1016/j.eucr.2014.07.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Wang J, Wang L, Long L, Tao Q, Xu F, Luo F. Solitary renal metastasis from squamous cell carcinoma of the lung: A case report. Medicine (Baltimore) 2019;98(5):e14310–e14310. doi: 10.1097/MD.0000000000014310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Akduman B, Altun R, Yesilli C, Yenidunya S, Ozdemir H, Mungan NA. Symptomatic renal metastasis 5 years after the management of a squamous cell carcinoma of the lung. Int J Urol. 2004;11(6):421–423. doi: 10.1111/j.1442-2042.2004.00810.x. [DOI] [PubMed] [Google Scholar]
- 17.Ter Avest MJ, Schook RM, Koudstaal LG, Grünberg K, Paul MA, Smit EF, Postmus PE. Benefit of a second opinion for lung cancer: no metastasis to the kidney but a synchronous primary renal neoplasm. Case Rep Oncol. 2014;7(1):122–125. doi: 10.1159/000359996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Aras M, Dede F, Ones T, Inanır S, Erdil TY, Turoğlu HT. Is The Value of FDG PET/CT In Evaluating Renal Metastasis Underestimated? A Case Report And Review of The Literature. Mol Imaging Radionucl Ther. 2013;22(3):109–112. doi: 10.4274/Mirt.130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Zardawi SJ, Li BT, Zauderer MG, Wang JW, Atmore BB, Barnes TA, Pavlakis N, Mathur MN, Clarke S. Localized malignant pleural mesothelioma with renal metastasis. Oxf Med Case Reports. 2015;2015(1):170–172. doi: 10.1093/omcr/omu064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Lim DH, Im YH, Ji SH, Park BB, Oh MJ, Lee J, Park KW, Lee SH, Park JO, Kim K, Kim WS, Jung CW, Park YS, Kang WK, Lee MH, Kim K, Shim YM, Park K. Esophageal squamous cell carcinoma recurring as a solitary renal mass. Cancer Res Treat. 2004;36(4):271–274. doi: 10.4143/crt.2004.36.4.271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Verma V, Simone CB. Stereotactic body radiation therapy for metastases to the kidney in patients with non-small cell lung cancer: a new treatment paradigm for durable palliation. Ann Palliat Med. 2017;6(2):96–103. doi: 10.21037/apm.2017.03.06. [DOI] [PubMed] [Google Scholar]
- 22.Matsushita Y, Katoh T, Isurugi K, Obara W, Suzuki T, Tamura T, Tanji S, Fujioka T. Metastatic renal tumor originating from esophageal carcinoma: a case report. Hinyokika Kiyo. 1998;44(8):591–594. [PubMed] [Google Scholar]
- 23.Chang KP, Huang CP, Chang H. Solitary renal metastasis of esophageal squamous cell carcinoma mimicking primary renal neoplasm-A case report and literature review. Biomedicine (Taipei) 2016;6(1):35–39. doi: 10.7603/s40681-016-0006-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Sun Y, Yu X, Zhang Y. Renal metastasis after esophagectomy of esophageal squamous cell carcinoma: a case report and literature review. World J Surg Oncol. 2014;12:165–165. doi: 10.1186/1477-7819-12-165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Dormeus S, Hernández EA, Nicolazzi M, Barba JF, Algarra R, Tienza A, Pascual JI, Berián JM, Zudaire JJ. Ureteroiliac fistula secondary to radiotherapy in a patient with single renal metastasis of colon adenocarcinoma. Can Urol Assoc J. 2013;7(1-2):E146–149. doi: 10.5489/cuaj.259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Dagnoni C, Granero LC, Rovere RK. Sigmoid adenocarcinoma with renal metastasis. Clin Pract. 2011;1(4):187–188. doi: 10.4081/cp.2011.e88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Sánchez-Ortiz RF, Madsen LT, Bermejo CE, Wen S, Shen Y, Swanson DA, Wood CG. A renal mass in the setting of a nonrenal malignancy: When is a renal tumor biopsy appropriate. Cancer. 2004;101(10):2195–2201. doi: 10.1002/cncr.20638. [DOI] [PubMed] [Google Scholar]
- 28.Malkoç E, Aktaş Z, Kara K, Haholu A. Renal metastasis from pancreatic adenocarcinoma: a rare case along with literature review. Turk J Urol. 2015;41(2):93–95. doi: 10.5152/tud.2015.54280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Ong KW, Joseph B, Gyomber DV, Bolton DM, Lawrentschuk N. Nephrectomy for a renal metastasis of undiagnosed hepatocellular carcinoma arising from an orthotopic liver transplant undertaken for cryptogenic cirrhosis. Korean J Urol. 2013;54(10):715–717. doi: 10.4111/kju.2013.54.10.715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Fukushima M, Isoyama E, Sakaridani N, Sanematsu H, Kadowaki H, Hirakawa S, Miyagawa I. Renal metastasis originating from liver cancer. Nihon Hinyokika Gakkai Zasshi. 1996;87(3):710–713. doi: 10.5980/jpnjurol1989.87.710. [DOI] [PubMed] [Google Scholar]
- 31.Marcuzzi A, Haider EA, Salmi ISA. Hepatic epithelioid angiomyolipoma with renal metastasis: radiologic-pathologic correlation. Radiol Case Rep. 2018;13(4):829–833. doi: 10.1016/j.radcr.2018.05.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Kinoshita O, Ichijo Y, Yoneda M, Ikai A, Yamashita T. Spontaneous Rupture of Renal Metastasis from Hepatocellular Carcinoma. Case Rep Surg. 2017;2017:8607061–8607061. doi: 10.1155/2017/8607061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Cheon M, Choi JY, Kim HK, Chung JH, Ko YH, Kim YE, Choi D, Lee KH, Kim BT. Renal Metastasis from Follicular Thyroid Carcinoma Diagnosed by I-131 Whole-body Scan Mimicking Renal Cell Carcinoma on Contrast-Enhanced Computed Tomography. Nucl Med Mol Imaging. 2011;45(1):72–75. doi: 10.1007/s13139-010-0067-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Yamazaki H, Kishida T, Noguchi G, Iwasaki H, Suganuma N, Masudo K, Nakayama H, Yamashita T, Yamanaka T, Sugawara Y, Matsubara Y, Kohagura K, Rino Y, Masuda M. Nephrectomy for Metastatic Kidney Tumor in Patients with Differentiated Thyroid Cancer: A Report of Two Cases. Case Rep Endocrinol. 2018;2018:7842792–7842792. doi: 10.1155/2018/7842792. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Claimon A, Suh M, Cheon GJ, Lee DS, Kim EE, Chung JK. Bilateral Renal Metastasis of Hürthle Cell Thyroid Cancer with Discordant Uptake Between I-131 Sodium Iodide and F-18 FDG. Nucl Med Mol Imaging. 2017;51(3):256–260. doi: 10.1007/s13139-016-0462-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Cochetti G, Puxeddu E, Zingaro MD, D'Amico F, Cottini E, Barillaro F, Mearini E. Laparoscopic partial nephrectomy of thyroid cancer metastasis: case report and review of the literature. Onco Targets Ther. 2013;6:355–360. doi: 10.2147/OTT.S37402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Nath V, Baliga M, Lewin J, Souza F, Akhtar I. Follicular Thyroid Carcinoma Metastatic to the Kidney: Report of a Case with Cytohistologic Correlation. Case Rep Pathol. 2015;2015:701413–701413. doi: 10.1155/2015/701413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Kulkarni P, Rekha PS, Prabhu M, Venkataramarao SH, Raju N, Chandrasekhar NH, Kannan S. Renal Metastasis and Dual ((18)F-Fluorodeoxyglucose and (131)I) Avid Skeletal Metastasis in a Patient with Papillary Thyroid Cancer. Indian J Nucl Med. 2017;32(1):50–53. doi: 10.4103/0972-3919.198482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Abe K, Hasegawa T, Onodera S, Oishi Y, Suzuki M. Renal metastasis of thyroid carcinoma. Int J Urol. 2002;9(11):656–658. doi: 10.1046/j.1442-2042.2002.00537.x. [DOI] [PubMed] [Google Scholar]
- 40.Ibinaiye PO, Mbibu H, Shehu SM, David SO, Samaila MO. Renal metastasis from prostate adenocarcinoma: a potential diagnostic pitfall. Ann Afr Med. 2012;11(4):230–233. doi: 10.4103/1596-3519.102854. [DOI] [PubMed] [Google Scholar]
- 41.Kurtul N, Resim S, Koçarslan S. Giant renal metastasis from prostate cancer mimicking renal cell carcinoma. Turk J Urol. 2018;44(4):367–369. doi: 10.5152/tud.2017.39225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Bazine A, Zniber HO, Ghaouti M, Bazine A, Baydada A, Sifat H. An Uncommon Case of Renal Metastasis from Cervical Cancer. Cureus. 2017;9(12):e1941–e1941. doi: 10.7759/cureus.1941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Fan G, Xie YU, Pei X, Lei J, Ye M, Zeng G, Li F, Xiong Y, Han W. Renal metastasis from cervical carcinoma presenting as a renal cyst: A case report. Oncol Lett. 2015;10(5):2761–2764. doi: 10.3892/ol.2015.3690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Kulkarni MM, Khandeparkar SG, Joshi AR, Kothikar V. A rare case of renal metastasis from squamous cell carcinoma of the cervix. J Midlife Health. 2016;7(2):94–96. doi: 10.4103/0976-7800.185330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Burns EM, Rosoff JS, Brooks SA, Picard MM, Smith MT, Picard JC. Renal metastasis of an ovarian granulosa cell tumour inducing growth of a cystic nephroma. BMJ Case Rep. 2013;2013(pii):bcr2013200010. doi: 10.1136/bcr-2013-200010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Bajic P, Gange WS, Blackwell RH, Shah AS, Biemer J, Picken MM, Gorbonos A. A Case of Renal Metastasis of Uterine Leiomyosarcoma. Cureus. 2017;9(7):e1470–e1470. doi: 10.7759/cureus.1470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Cochrane E, Menzies A, Sweeney K, Burke W. Synchronous renal and para-aortic metastasis in a uterine serous carcinoma: A case review and clinical considerations. Gynecol Oncol Rep. 2019;28:12–14. doi: 10.1016/j.gore.2019.01.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Sparchez Z, Radu P, Sparchez M, Crisan N, Kacso G, Petrut B. Contrast enhanced ultrasound of renal masses. A reappraisal of EFSUMB recommendations and possible emerging applications. Med Ultrason. 2015;17(2):219–226. doi: 10.11152/mu.2013.2066.172.fsum. [DOI] [PubMed] [Google Scholar]
- 49.Del Vecchio S, Ellis R, Gallagher K, Ng KL, Ma L, Strutton G, Wood S. A Rare Case of Solitary Kidney Metastasis Following Primary Laryngeal Squamous Cell Carcinoma. J Kidney Cancer VHL. 2017;4(2):6–9. doi: 10.15586/jkcvhl.2017.68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Shah D, Shah D. Sinonasal Adenoid Cystic Carcinoma with Rare Renal Metastasis on Fluorodeoxyglucose Positron Emission Tomography Scan: A Case Report and Literature Review. Indian J Nucl Med. 2018;33(1):52–54. doi: 10.4103/ijnm.IJNM_104_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Kajikawa T, Ishikura K, Banya Y, Fujioka T, Kubo T. Renal metastasis from osteogenic sarcoma: report of a case. Nihon Hinyokika Gakkai Zasshi. 1993;84(9):1694–1697. doi: 10.5980/jpnjurol1989.84.1694. [DOI] [PubMed] [Google Scholar]
- 52.Sekito S, Kato M, Nishikawa K, Yoshio Y, Kanai M, Kanda H, Arima K, Sugimura Y. Successfully Treated Lung and Renal Metastases from Primary Chondrosarcoma of the Scapula with Radiofrequency Ablation and Surgical Resection. Case Rep Oncol Med. 2019;2019:6475356–6475356. doi: 10.1155/2019/6475356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Chan G, Kroczak T, Drachenberg D. Leiomyosarcoma of the inferior vena cava with renal metastasis: An unusual case and diagnostic challenge. Can Urol Assoc J. 2014;8(9-10):358–360. doi: 10.5489/cuaj.2119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Yoshikawa T, Tanizawa A, Suzuki K, Ikeda K, Nomura E, Maeda Y, Tanaka N, Yamada K, Sakai Y, Imamura Y, Ohshima Y. High-Risk Neuroblastoma with Metastases to Bilateral Kidneys at Diagnosis. Case Rep Pediatr. 2017;2017:5375091–5375091. doi: 10.1155/2017/5375091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Campobasso D, Ferretti S, Pilato FP, Frattini A. Giant bilateral renal metastases from a meningeal hemangiopericytoma. J Cancer Res Ther. 2018;14(6):1434–1436. doi: 10.4103/0973-1482.187340. [DOI] [PubMed] [Google Scholar]
- 56.Demirer Z, Zor M, Kurt B, Bozkurt Y, Yildirim I. Bilateral renal metastasis of an inguinal malignant solitary fibrous tumor, 9 years after primary surgical treatment. Med Princ Pract. 2012;21(6):585–587. doi: 10.1159/000339923. [DOI] [PubMed] [Google Scholar]
- 57.Medhi S, Purandare NC, Dua SG, Gujral S. Bilateral renal metastases in a case of Merkel cell carcinoma. J Cancer Res Ther. 2010;6(3):353–355. doi: 10.4103/0973-1482.73365. [DOI] [PubMed] [Google Scholar]
- 58.Langley RR, Fidler IJ. The seed and soil hypothesis revisited--the role of tumor-stroma interactions in metastasis to different organs. Int J Cancer. 2011;128(11):2527–2535. doi: 10.1002/ijc.26031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Psaila B, Lyden D. The metastatic niche: adapting the foreign soil. Nat Rev Cancer. 2009;9(4):285–293. doi: 10.1038/nrc2621. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Ignee A, Straub B, Schuessler G, Dietrich CF. Contrast enhanced ultrasound of renal masses. World J Radiol. 2010;2(1):15–31. doi: 10.4329/wjr.v2.i1.15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Patel U, Ramachandran N, Halls J, Parthipun A, Slide C. Synchronous renal masses in patients with a nonrenal malignancy: incidence of metastasis to the kidney versus primary renal neoplasia and differentiating features on CT. AJR Am J Roentgenol. 2011;197(4):W680–W686. doi: 10.2214/AJR.11.6518. [DOI] [PubMed] [Google Scholar]