

Abstract
Background
Adolescents in the United States account for one-fifth of new HIV cases, and have the highest rate of undiagnosed HIV, with more than half (51%) not knowing their status. It is a crucial public health concern to help equip youth with the information and autonomy to minimize their risk and know their status. Serious videogames are emerging as valuable tools for health and behavior change in adolescents, and have potential to engage this population and increase their use of HIV testing and counseling (HTC). The purpose of this study was to: (I) modify an original serious game targeting risk reduction and HIV prevention developed by the play2PREVENT Lab and create a new serious game that focuses on HTC; (II) evaluate its feasibility and acceptability; (III) pilot-test the assessment measures that are subsequently being used in a large randomized controlled trial.
Methods
Three focus groups with adolescents, aged 14–17 (n=13, mean age =15), informed artwork and storylines for PlayTest! After the game was completed, a pilot test was conducted using a one-group pretest-posttest design to collect data on: (I) participants’ gameplay satisfaction and experience; (II) the validity of the project’s assessments. Twenty-six participants, aged 15–16 were enrolled from a local after-school program. Participants played PlayTest! twice weekly for three weeks. Data were collected on behavior, intentions, knowledge, perceived susceptibility, and attitudes related to HTC at baseline, post-gameplay (three weeks), and follow-up (six weeks).
Results
For the focus groups used in the game development, four major themes emerged: (I) adolescents have strong misperceptions about HTC, including who should get tested and what the test entails; (II) adolescents have incorrect knowledge about how HIV is contracted, spread, and treated; (III) adolescents are supportive of their peers getting tested for HIV, but are not likely to get tested themselves; (IV) while the majority of adolescents know where to get tested for HIV, social stigma, misperceptions around HTC, and fear of having a positive diagnosis keep them from seeking it. For the pilot study, overall, participant experience with the game was highly favorable. The assessments were sensitive enough to capture changes in our target variables: intentions (P=0.037) and knowledge (P=0.025) related to HTC at follow-up.
Conclusions
The PlayTest! game provides promising results regarding using an engaging and evidence-informed videogame intervention to promote HTC in adolescents.
Keywords: Serious game; videogame, adolescents; HIV Testing & Counseling (HTC); behavior change
Introduction
Adolescents in the United States account for one-fifth of new HIV cases, and have the highest rate of undiagnosed HIV, with more than half (51%) not knowing their status (1). Because adolescents are at a particularly high risk of acquiring HIV infection, it is a crucial public health concern to help equip youth with the information and autonomy to minimize their risk and know their status. HIV testing and counseling (HTC) is the critical access point for many HIV prevention interventions; helping to establish early diagnosis and effective care (2). The Centers for Disease Control and Prevention highlights that inadequate sex education is a prevention challenge, with the percentage of U.S. high schools that teach how HIV and other STIs are transmitted ranging from 49-100% across states, and the percentage of U.S. high schools that teach how to access valid and reliable health information, products, and services related to HIV, ranging from 36-100% across states. Stigma and misperception about HIV have also been identified as barriers; with young people having negative perceptions of those who might have HIV and not knowing how HIV is transmitted or treated (3). Additionally, low rates of testing have been identified as another prevention challenge, with only nine percent of U.S. high school students report ever being tested for HIV (3). Therefore, novel approaches are needed to engage this population to give them the knowledge and address behaviors associated with contracting HIV in order to increase their use of HTC.
Serious videogames, videogames developed for a purpose other than solely entertainment (4), are emerging as valuable tools for health and behavior change in adolescents (5) and have the potential to be used to increase HTC rates in adolescents.
The purpose of this study, was to modify an original serious game targeting risk reduction and HIV prevention developed by the play2PREVENT Lab and create a new serious game that focuses on HTC, evaluate its feasibility and acceptability, and pilot-test the assessment measures that are subsequently being used in a large randomized controlled trial.
Methods
Approval for this feasibility study was obtained by the Yale University School of Medicine Human Investigation Committee. This pilot project consisted of multiple components: (I) the development of the videogame PlayTest!; (II) assessment of feasibility and acceptability of the videogame; (III) evaluation of the assessments for a subsequent trial.
PlayForward (the original game)
PlayForward: Elm City Stories (PlayForward) is an original evidence-informed videogame, that focuses on risk reduction and HIV prevention in youth. PlayForward was designed and developed using a theoretical framework including social learning theory, self-efficacy, prospect theory and message framing, and delay discounting (6,7). In the game, the player uses an Aspirational Avatar (8) to travel through life, facing challenges and exploring how specific choices can impact their short-and long-term goals. The game includes storylines and skill-building opportunities around sex, drugs, alcohol, and positive decision-making, and has up to 16 hours of unique gameplay. PlayForward was evaluated through a large randomized controlled trial (9) and demonstrated efficacy in improving attitudes and knowledge around sexual health (10). The PlayTest! prototype tested in this pilot study was built from the PlayForward game foundation.
Development of PlayTest! (the modified game)
While HIV was incorporated into main storylines and minigames in PlayForward, HTC was not the focus. The development of the modified game, PlayTest!, allowed our team to focus storylines and minigames specifically on HTC, including: risky behaviors associated with increasing the likelihood of acquiring HIV, HIV misperceptions and stigmas, HTC process and confidentiality, and barriers and facilitators to getting tested. We conducted focus groups with adolescents to guide the new content and storylines for PlayTest!.
Focus group discussions
In partnership with one of our local, longstanding afterschool programs, we recruited adolescents to participate in the content development of PlayTest!. Three focus groups with adolescents, aged 14–17 (n=13, mean age =15), informed new artwork and storylines for PlayTest!. Focus groups were conducted by two research team members who have extensive experience with conducting focus groups with adolescents and who had previously worked with groups of adolescents in the afterschool program. The focus groups took place onsite at the participants’ program and included one male-only group, one female-only group, and one mixed gender group, with four to five participants each.
Focus group participants were asked questions such as: “Who should get tested for HIV? What might keep a teen from getting tested? If a teen decided to get tested and the test was positive, what information do you think the doctor should give them? What might keep a teenager from getting tested in the clinic at their school?”.
Evaluation of participants’ gameplay satisfaction and assessments
We conducted a pilot test of PlayTest! using a one-group pretest-posttest design to collect data on: (I) participants’ gameplay satisfaction and experience and (II) the validity of the project’s assessments. Participants played PlayTest! twice weekly for three weeks for a total of approximately six hours of gameplay. We collected data via self-reported assessment questions at baseline, immediately post-gameplay (three weeks) and follow-up (6 weeks). Both qualitative and quantitative data were collected. The after-school program offered the intervention as a part of their curriculum over the course of several weeks, with students being allowed to opt out.
Participants and recruitment
We recruited adolescents from a partner community-based after-school program-that serves over 1000 kids and adolescents per year, with 97% of the participants being racial minorities and 85% receiving free lunch. We sent home information sheets and had parent information sessions during the recruitment phase. Inclusion criteria for the study were adolescents between ages 14–18.
Assessments
Gameplay satisfaction and experience was assessed at three weeks at the end of gameplay with 12 items (e.g., “I enjoyed playing the game”) on a scale from 1 (strongly disagree) to 4 (strongly agree). Each item was analyzed separately using descriptive statistics (11). Three adapted scales were used to explore behaviors, intentions, knowledge, perceived susceptibility, and attitudes. (12-14). Behavior was assessed by asking participants whether they had ever been tested for HIV with response options 1 (yes), 0 (no/decline to answer/ not sure). Intentions to protect one’s self against HIV were assessed with the mean of three items (e.g., “I intend to get tested for HIV in the next month”) rated on a scale ranging from 1 (strongly disagree) to 5 (strongly agree) with higher scores representing healthier intentions. Knowledge was assessed with 25 items with 1 (true) and 0 (false) response options. A sum of the knowledge items was calculated with higher scores representing improved knowledge. Perceived susceptibility was assessed from 1 (big chance) to 4 (no chance) on the item “what do you think your chances are of getting HIV in the next three months?” Attitudes about HIV were assessed with the mean of 5 items following the stem “Imagine you had HIV. Do you think the people you interact with would…” (e.g., “…react positively toward you?”), with response options ranging from 1 (a lot) to 4 (not at all).
Data analysis
Focus groups: for the semi-structured focus groups, a two-person research team comprised of individuals with expertise in videogame interventions, qualitative methods, and health behavior conducted the analysis. Focus groups were recorded and transcribed, and themes were extracted to guide the content, storylines, and dialogue for PlayTest! This information was relayed to our game development partners, who made the appropriate changes to create the new game. Pilot study: Gameplay experience was evaluated through participants responding to 12 items on a scale from 1 (strongly disagree) to 4 (strongly agree) (11). A Cochran’s Q was conducted to determine if the proportion of participants who reported being tested for HIV changed across three time points. For intentions, knowledge, perceived susceptibility, and attitudes one-way repeated measures ANOVAs were conducted to compare scores on across three time points.
Results
Participant characteristics
In the three focus groups with adolescents, aged 14–17 (n=13, mean age=15), that helped to inform the new artwork and storylines for PlayTest!, 84% of adolescents were male; 77% identified as Black, 8% as Hispanic/Latino, 8% as biracial, and 8% as Native American.
Focus group and game modification
Four major themes emerged from the focus groups around HTC: (I) adolescents have strong misperceptions about HTC, including who should get teste and what the test entails; (II) adolescents have incorrect knowledge about how HIV is contracted, spread, and treated; (III) adolescents are supportive of their peers getting tested for HIV, but are not likely to get tested themselves; (IV) while the majority of adolescents know where to get tested for HIV, social stigma, misperceptions around HTC, and fear of having a positive diagnosis keep them from seeking it. These themes shaped the stories, characters, risk scenarios, and behavioral skills taught in the videogame intervention, to create a relatable, relevant gameplay experience for players (Figure 1). For example, in one of the new storylines, a rumor about a classmate going into the school clinic to be tested for HIV, spreads quickly via a group text. The player must navigate how to handle the situation based on the facts they know about privacy in school clinics and the services that school clinics offer (Figures 2,3).
Figure 1.
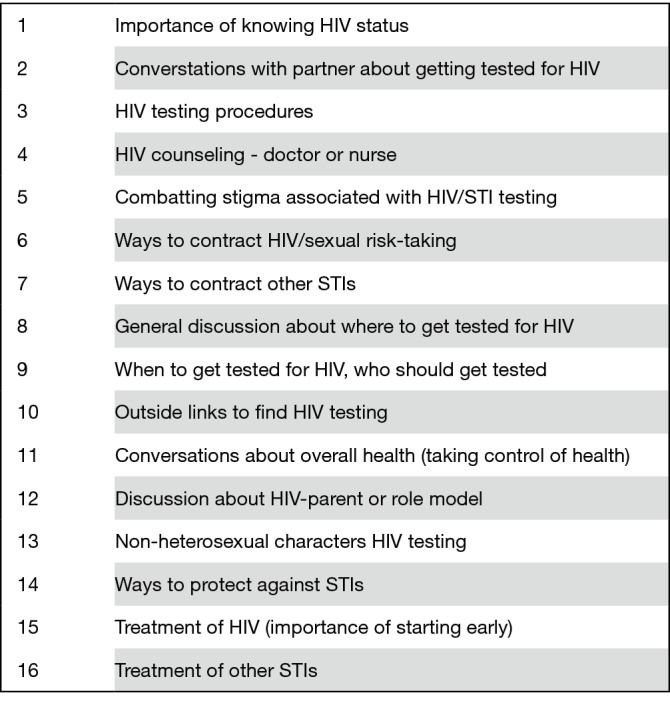
Content for PlayTest!
Figure 2.

Screenshot from PlayTest!
Figure 3.

Screenshot from PlayTest!
The PlayTest! intervention
PlayTest! included six hours of original content focused on myriad topics related to HIV and HTC embedded in eight main storylines and five minigames (Me Power, Know Sense, Priority Sense, Persuasion Power, and People Sense). Me Power encourages students to imagine what kind of future they would like for themselves, so they can better recognize how poor health decisions can impact that future. In Know Sense, players learn accurate information about HIV and HTC. In Priority Sense, the player helps their avatar achieve their goals while balancing the demands of life. In Persuasion Power, players help convince their peers to get tested for HIV and engage in positive health behaviors. In People Sense, the player helps a character decide which of their peers to keep as close friends, based on an individual’s ability to influence their decisions and behaviors. The intervention was comprised of the main storylines, and five levels of each of the minigames (25 minigame levels total).
Pilot study
For the pilot study, of the 26 participants, 15/26 (58%) were girls, 23/26 (88%) were Black and 3/26 (11%) were Hispanic. Participants played the game on average 3.2 hours over three weeks. Twenty-four out of the twenty-six participants (92%) completed at least one game play session, representing some exposure to the intervention. Twenty-one out of the 26 participants (80%) completed their three-week assessments post gameplay. Twenty-one out of the twenty-six participants (80%) completed their six-week follow-up assessment questions.
Gameplay experience
Overall, participant experience with the game was highly favorable (Table 1). Eighty-five percent enjoyed playing the game, 83% felt connected to the characters, 88% reported they would make decisions in life as they made them in the game, and 89% felt responsible for the choices they made in the game.
Table 1. Player gameplay experience.
| Item | M (SD) | % agree |
|---|---|---|
| I would play this game again | 2.60 (1.10) | 65 |
| I was frustrated with this game | 2.05 (0.62) | 21 |
| I would make decisions in life like I made them in the game | 3.12 (0.93) | 88 |
| I liked the way the game looked | 3.11 (0.76) | 89 |
| I felt connected to other characters in the game | 3.08 (0.90) | 83 |
| I felt connected to my character in the game | 2.86 (0.95) | 79 |
| I felt responsible for the choices I made in the game | 3.06 (0.87) | 89 |
| I enjoyed playing the game | 2.95 (0.83) | 85 |
| The game was challenging | 2.65 (0.86) | 53 |
| I would tell my friends to play the game | 3.00 (0.71) | 88 |
Evaluation of assessments
The assessments used in the pilot study were sensitive enough to capture changes in our target variables: intentions (P=0.037) and knowledge (P=0.025) related to HTC at follow-up. For intentions, there was a significant effect for time (P=0.037), for knowledge, there was a significant effect for time (P=0.025). For perceived susceptibility to HIV, assessment measures showed no significant change (P=0.390). For attitudes, assessment measures showed no significant change in attitude toward HIV testing over time (P=0.323) (Table 2).
Table 2. Evaluation of assessment validity.
| Scores baseline, mean (SD) | Scores (post-gameplay, 3 weeks), mean (SD) | Scores (follow-up, 6 weeks), mean (SD) | Number of participants tested for HIV (baseline) | Number of participants tested for HIV (post-gameplay, 3 weeks) | Number of participants tested for HIV (follow-up, 6 weeks) | P value | |
|---|---|---|---|---|---|---|---|
| Intentions | 2.81 (0.89) | 3.28 (0.92) | 3.15 (0.81) | – | – | – | 0.037 |
| Knowledge | 17.44 (4.30) | 21.13 (3.83) | 21.13(2.85) | – | – | 0.025 | |
| Perceived Susceptibility | 0.06 (0.24) | 0.22 (0.55) | 0.11 (0.32) | – | – | – | 0.390 |
| Attitudes | 2.18 (0.77) | 2.30 (0 .60) | 2.19 (0.58) | – | – | – | 0.323 |
| Behavior | – | – | – | 0 | 0 | 2 | 0.135 |
Discussion
Novel methods to promote and increase HIV testing rates in adolescents are needed. For this project we created a serious game that focuses on HTC through feedback from focus groups with adolescents and evaluated the game’s feasibility and acceptability through players’ gameplay satisfaction and experience. Analysis of our qualitative data regarding the participants’ gameplay experience highlights that a majority of the participants found the game to be enjoyable and relatable.
The findings regarding the feasibility and acceptability of the game are very important. Studies have shown that player enjoyment of a game increases engagement with the subject matter (15); ultimately affecting the acquisition and use of knowledge and skills (16). The large number of participants that enjoyed and felt connected to PlayTest! underscores its success in connecting with its target audience and providing a novel and enjoyable platform to learn about HTC and potentially change behavior.
Although various programs exist to teach adolescents in the U.S. about HIV, education about promoting HIV testing is sorely lacking. A videogame has an advantage over conventional methods, by not only delivering knowledge to the player, but also allowing students to practice skills and behaviors in the context of the game that are associated with HTC. For example, in the game PlayTest!, the player practices having a conversation with a medical professional at their school’s health center about the process of getting tested for HIV. Ideally, being able to practice these skills and behaviors in the game will translate into positive real-life health behaviors. There is evidence that individuals who gain new knowledge and are able to practice new behavioral skills in a virtual environment are more likely to use these new skills in real life (17-20).
Most HTC interventions for adolescents have only measured an intention to be tested and not actual testing (21); therefore partnering with schools that have school-based health centers to be able to track students who play PlayTest! is another step that we have implemented as we have started the subsequent large randomized controlled trial; providing concrete data on HTC rates. Additionally, this game intervention could be useful for addressing common misperceptions about HIV and HTC that have been identified as a barrier to testing in adolescents (22) and could be used in a classroom setting as a part of a health class curriculum to help provide knowledge around HTC.
Furthermore, because adapted assessment scales were used in this project, it was important to test the validity of the assessment questions that are now being used in a subsequent large randomized controlled trial. The assessment measures were sensitive enough to capture changes in our target variables of intentions and knowledge in a small sample and a pattern of means that trended in the right direction for susceptibility. These findings highlight the validity of the measures, and this pilot study gives us confidence in the measures we have proceeded with in the randomized controlled trial.
This study has several limitations. Videogames are engaging and provide a novel way to connect with adolescents whose lives are immersed in technology, however there are challenges to engage adolescents in any intervention. Our pilot study allowed us to collect real world data and demonstrate the acceptability and feasibility of this intervention. Our goal for this pilot study was to have the participants receive a significant amount of exposure to the intervention. We created six hours of game content specifically focused on HTC; however, play times varied across students (some students played six hours of the game in three hours) and the number of hours played is not necessarily associated with how far they progressed in the game or the amount of exposure they had to the content. Our previous study examining the relationship between gameplay and impact demonstrated that how a student plays the game (quality), and not the amount of time they play the game (quantity) is a better indicator of the effect of the intervention (23). Furthermore, in the context of the pilot study, students were not required to play a certain amount of time, nor were they mandated to attend their after-school program daily. Notably, participants received compensation to answer the assessment questions at the various time points, but not for playing the game.
The sample size for this pilot study is another limitation. The small sample size and the use of a one-group pretest-posttest design with no control group limits our ability to validate that documented changes are due solely to the PlayTest! intervention. Additionally, this study was completed in a structured urban after-school setting, which may also affect its generalizability. Future work includes further modifying elements of the game to ensure that it effectively addresses perceived susceptibility and attitudes with the goal of seeing increases in these areas and evaluating the game with a considerably larger number of adolescents in a range of settings with longer follow-up periods.
Another limitation of the pilot study, is that only 15 and 16 years old participated, although it was created for a wider age range of adolescents. However, because we work with after-school programs for our studies, the after-school program felt that the content in the videogame was most appropriate for their 15–16 years old attendees. As a result, the pilot study was offered as a part of the after-school curriculum for the 15–16 years old groups that aligned with a healthy decision—making unit that they were starting. But this does highlight how after-school programs and schools might be able to incorporate this unique intervention into their already structured programs.
Conclusions
Despite these limitations, the PlayTest! game provides promising results regarding, using an engaging and evidence-informed videogame intervention to promote HTC in adolescents in a format that is acceptable and feasible to them. The goal for the PlayTest! game intervention is that it will build on the engagement and reach that technology-based interventions offer while effectively addressing the very concerning high rates of HIV and low rates of HTC in adolescents. It meets adolescents where they are and provides them with an intervention that resonates with them and has the potential to impact health promotion behaviors.
Acknowledgments
We would like to thank Erica Miller and Milana Bochkur-Dratver for their valuable contributions to this project.
Funding: We would like to acknowledge and thank our funder, the National Institute of Child Health and Development.
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Open Access Statement: This is an Open Access article distributed in accordance with the Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License (CC BY-NC-ND 4.0), which permits the non-commercial replication and distribution of the article with the strict proviso that no changes or edits are made and the original work is properly cited (including links to both the formal publication through the relevant DOI and the license). See: https://creativecommons.org/licenses/by-nc-nd/4.0/.
Footnotes
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/mhealth.2020.01.05). The authors have no conflicts of interest to declare.
References
- 1.Centers for Disease Control and Prevention. Diagnoses of HIV infection in the United States and dependent areas, 2017. HIV Surveillance Report 2018;29.
- 2.World Health Organization. HIV and adolescents: Guidance for HIV testing and counselling and care for adolescents living with HIV: recommendations for a public health approach and considerations for policy-makers and managers 2013. [PubMed]
- 3.Centers for Disease Control and Prevention. HIV and Youth 2018. (Accessed June 27, 2019). Available online: https://www.cdc.gov/hiv/group/age/youth/index.html
- 4.Clark CA. Serious games. New York: Viking, 1970. doi: 10.1177/000276427001400113. [DOI] [Google Scholar]
- 5.Primack BA, Carroll MV, McNamara M, et al. Role of video games in improving health-related outcomes: a systematic review. Am J Prev Med 2012;42:630-8. 10.1016/j.amepre.2012.02.023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Duncan LR, Hieftje KD, Culyba S, et al. Game playbooks: tools to guide multidisciplinary teams in developing videogame-based behavior change interventions. Transl Behav Med 2014;4:108-16. 10.1007/s13142-013-0246-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Camenga DR, Hieftje KD, Fiellin LE, et al. The use of message framing to promote sexual risk reduction in young adolescents: a pilot exploratory study. Health Education Research 2014;29:360-6. 10.1093/her/cyt156 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hieftje K, Duncan LR, Fiellin LE. Novel methods to collect meaningful data from adolescents for the development of health interventions. Health Promotion Practice 2014;15:714-22. 10.1177/1524839914521211 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Fiellin LE, Kyriakides TC, Hieftje KD, et al. The design and implementation of a randomized controlled trial of a risk reduction and human immunodeficiency virus prevention videogame intervention in minority adolescents: PlayForward: Elm City Stories. Clin Trials 2016;13:400-8. 10.1177/1740774516637871 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Fiellin LE, Hieftje KD, Pendergrass TM, et al. Videogame Intervention for Sexual Risk Reduction in Minority Adolescents: A Randomized Clinical Trial. J Med Internet Res 2017;19:e314. 10.2196/jmir.8148 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hieftje KD, Pendergrass TM, Montanaro E, et al. “But do they like it?” Participant satisfaction and gameplay experience of a public health videogame intervention in adolescents 2018 IEEE 6th International Conference on Serious Games and Applications for Health (SeGAH). doi: 10.1109/SeGAH.2018.8401349. [DOI] [Google Scholar]
- 12.Kalichman SC, Picciano JF, Roffman RA. Motivation to reduce HIV risk behaviors in the context of the information, motivation and behavioral skills (IMB) model of HIV prevention. Journal of Health Psychology 2008;13:680-9. 10.1177/1359105307082456 [DOI] [PubMed] [Google Scholar]
- 13.Kann L, McManus T, Harris WA, et al. Youth Risk Behavior Surveillance - United States, 2015. MMWR Surveill Summ 2016;65:1-174. [DOI] [PubMed] [Google Scholar]
- 14.Addis Z, Yalew A, Shiferaw Y, et al. Knowledge, attitude and practice towards voluntary counseling and testing among university students in North West Ethiopia: a cross sectional study. BMC Public Health 2013;13:714. 10.1186/1471-2458-13-714 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Iten N, Petko D. Learning with serious games: Is fun playing the game a predictor of learning success? Br J Educ Technol 2016;47:151-63. 10.1111/bjet.12226 [DOI] [Google Scholar]
- 16.Ritterfeld U, Weber R. Video games for entertainment and education. In Vorderer P, Bryant J. editors. Playing video games: Motives, responses, and consequences. 2006:399-413. [Google Scholar]
- 17.Bainbridge W. The scientific research potential of virtual worlds. Science 2007;317:472-6. 10.1126/science.1146930 [DOI] [PubMed] [Google Scholar]
- 18.Hubal R, Kizakevich P, Furberg R. Synthetic characters in health-related applications. Advanced Computational Intelligence Paradigms in Healthcare-2. Springer, 2007:5-26. [Google Scholar]
- 19.Johnson WL, Beal CR. Iterative Evaluation of a Large-Scale, Intelligent Game for Language Learning. AIED. 2005:290-7. [Google Scholar]
- 20.Schwebel DC, Gaines J, Severson J. Validation of virtual reality as a tool to understand and prevent child pedestrian injury. Accid Anal Prev 2008;40:1394-400. 10.1016/j.aap.2008.03.005 [DOI] [PubMed] [Google Scholar]
- 21.Albarracín D, Gillette JC, Earl AN, et al. A test of major assumptions about behavior change: a comprehensive look at the effects of passive and active HIV-prevention interventions since the beginning of the epidemic. Psychol Bull 2005;131:856-97. 10.1037/0033-2909.131.6.856 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Peralta L, Deeds BG, Hipszer S, et al. Barriers and facilitators to adolescent HIV testing. AIDS Patient Care STDS 2007;21:400-8. 10.1089/apc.2006.0112 [DOI] [PubMed] [Google Scholar]
- 23.Montanaro E, Fiellin LE, Fakhouri T, et al. Using videogame apps to assess gains in adolescents’ substance use knowledge: new opportunities for evaluating intervention exposure and content mastery. J Med Internet Res 2015;17:e245. 10.2196/jmir.4377 [DOI] [PMC free article] [PubMed] [Google Scholar]