

Abstract
Patient: Female, 45-year-old
Final Diagnosis: Hypothyroidism
Symptoms: Dysarthria • dyspnea
Medication:—
Clinical Procedure: Pericardial drainage
Specialty: Cardiology
Objective:
Rare disease
Background:
Thyroid function is closely related to the cardiovascular system. Pericardial effusion is a well-known complication of hypothyroidism. It is common for massive pericardial effusion to progress to tamponed heart with hypotension, but not high blood pressure.
Case Report:
A 46-year-old woman presented to the hospital with dysarthria and left-side weakness of the upper limb which had started 30 minutes before her arrival at the hospital. The patient showed hypertensive emergency (213/124 mmHg) with intracerebral hemorrhage. Further evaluation for high blood pressure and transthoracic echocardiography demonstrated the presence of a large amount of pericardial effusion, and urgent pericardiocentesis was performed. The laboratory examination showed elevated thyroid-stimulating hormone and decreased free thyroxine level, leading to a diagnosis of primary hypothyroidism. The administration of current medications was maintained, including thyroid hormone replacement and anti-hypertensive drugs.
Conclusions:
A rare case of profound hypothyroidism presenting with hypertensive crisis and massive pericardial effusion is described in this report.
MeSH Keywords: Cardiac Tamponade; Hypertension, Malignant; Hypothyroidism
Background
Hypothyroidism can affect any organ system, including the digestive, cardiovascular, dermatological, endocrine, hematological, musculoskeletal, psychiatric, renal, or pulmonary systems. The most common cardiovascular symptoms of hypothyroidism are bradycardia, diastolic hypertension, narrowed pulse pressure, and attenuated activity in the precordial examination. The incidence of pericardial effusion due to hypothyroidism ranges from 3% to 37%, and this condition is most commonly observed in patients with severe hypothyroidism [1–8]. The discriminating feature of massive pericardial effusion caused by hypothyroidism is an absence of sinus tachycardia. Tachycardia is commonly observed in cases of pericardial effusion with early tamponed physiology due to other causes [2,9]. Additionally, pericardial effusion and nonpitting edema (myxedema) can occur in patients with severe, long-standing hypothyroidism [9,10]. There are few reports of massive pericardial effusion and hypertensive emergency with cerebral hemorrhage caused by profound hypothyroidism [2,3,11,12].
Case Report
A 46-year-old woman presented to our hospital emergency room with dysarthria and left-side weakness of the upper limb. These symptoms had started 30 minutes before her arrival at the hospital. She did not have any past medical histories. Initial vital signs were: blood pressure, 213/124 mmHg; body temperature, 36.3°C; heart rate, 60 bpm; and respiratory rate, 20 bpm. The patient appeared to have a puffy face and generalized edema. No jugular venous distension was observed, and cardiac murmur was not auscultated. Neurological examination revealed dysarthria and left upper-limb weakness of motor grade 1–2. Neuroimaging was immediately carried out; non-contrast brain computed tomography revealed intracranial hemorrhage at the right basal ganglia, right thalamus, and right periventricular white matter (Figure 1). The patient was admitted to the Neurosurgical Department and was treated as a hypertensive crisis with intracranial hemorrhage.
Figure 1.
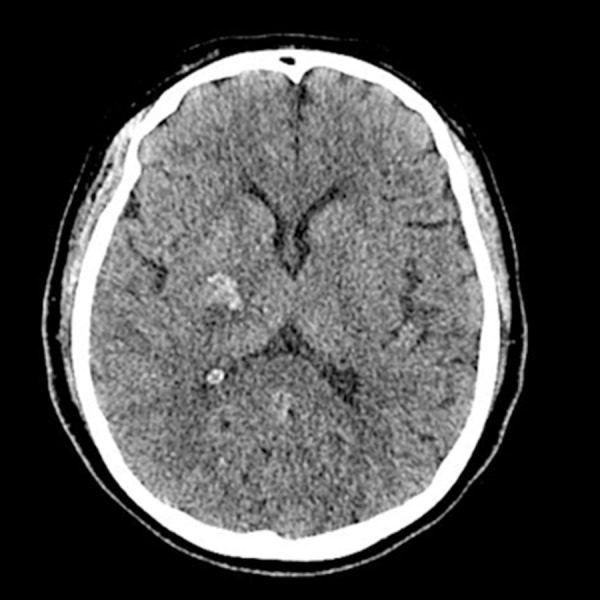
Non-contrast brain computed tomography showing intracranial hemorrhage on the right basal ganglia, right thalamus, and right periventricular white matter.
Electrocardiography showed a normal sinus rhythm (Figure 2A) and chest radiograph revealed the presence of the “water bottle” sign, indicating a large cardiomegaly (Figure 2B). Transthoracic echocardiography revealed a circumferential large amount of pericardial effusion, with compression of the right ventricle and right atrium; the maximal thickness was about 30 mm on the posterior side of the ventricular wall, and left ventricular systolic function was preserved (Figure 3).
Figure 2.

(A) Electrocardiogram showing normal sinus rhythm. (B) Chest X-ray showing the “water bottle” sign, indicating a large cardiomegaly.
Figure 3.

Pre-pericardiocentesis echocardiographic findings. Transthoracic echocardiography showed a circumferential large amount of pericardial effusion (maximal thickness, about 30 mm at the posterior side of the ventricular wall) with slight compression of the right atrium and right ventricle. Left ventricular systolic function was preserved. (A) A large amount of pericardial effusion was observed on the parasternal long-axis view and parasternal short-axis views. (B) A large amount of pericardial effusion was also observed in various apical views.
On the initial laboratory finding, the patient’s hemoglobin level was 7.0 g/dL, indicating normocytic normochromic anemia.
Anisocytosis was observed in the blood smear morphology, and reticulocyte level was normal (1.15%). Total cholesterol and triglyceride levels were high, at 204 and 339 mg/dL, respectively. Other laboratory findings, such as platelet and leukocyte count, renal function, serum electrolytes, and liver function, were unremarkable.
Controlling blood pressure using appropriate drugs was considered to prevent worsening of neurological symptoms or examination and additional hemorrhage due to excessively high blood pressure almost 220, under the absolutely close monitoring of blood pressure. Blood pressure was abruptly decreased by the injection of intravenous low-dose perdipine, which then caused her condition to worsen, resulting in reduced awareness and shortness of breath. In addition, according to the European Society of Cardiology statement [13], a total score of 7 points was confirmed in this patient, consisting of hypothyroidism (–1), dyspnea (1), rapid worsening of symptom (2), cardiomegaly on chest X-ray (1), circumferential pericardial effusion >2 cm in diastole (3), and swinging heart (1). Due to these sudden aggravated symptoms and the indicated score, echocardiography-guided urgent pericardiocentesis was immediately performed through an apical approach.
A 1100 cc volume of straw-colored fluid was drained, a sample of which was sent for analysis. After pericardiocentesis, the fluctuation in blood pressure disappeared, but the high blood pressure remained at 160–170 mmHg.
No malignant cells, bacteria on infectious culture, or mycobacterium (assessed by acid-fast bacilli stain) were detected in the pericardial effusion. Serology tests were negative, including antinuclear antibodies, human immunodeficiency virus, anti-neutrophil cytoplasmic antibodies, anticardiolipin antibodies, and various tumor markers. Thyroid hormone tests revealed elevated thyroid-stimulating hormone (TSH) of >100 mU/mL (normal range: 0.27–4.20 mU/mL) and considerably decreased free thyroxine (T4) of <0.08 ng/dL (normal range: 0.74–1.80 ng/dL) and triiodothyronine (T3) of <0.20 ng/mL (normal range: 0.80–2.00 ng/mL). The anti-microsomal antibody (anti-thyroid peroxidase antibody) level was <9 (normal level: <34 U/mL) and the anti-thyroglobulin antibody level was high, at 320 U/mL (normal level: <115 U/mL).
The administration of current medications was maintained, including Synthroid (oral thyroid hormone replacement) and anti-hypertensive drugs. Synthroid was initially prescribed at a dose of 0.15 mg, and the anti-hypertensive drug olmesartan was administered at 40 mg and combined with amlodipine 5 mg.
The neurological symptoms improved gradually with rehabilitation. Six-month follow-up resulted in lowering the dosage of anti-hypertensive drug due to normalization of thyroid hormone level, and the symptoms of hypothyroidism had also disappeared. Thyroid hormone levels were improved: the TSH level was 0.64 uIU/mL and the free T4 level was 1.88 ng/dL. Subsequent follow-up echocardiography showed no evidence of pericardial effusion, and a definite concentric left ventricular hypertrophy was observed (Figure 4).
Figure 4.

Post-pericardiocentesis echocardiographic findings. (A) Pericardial effusion was not observed on the parasternal long-axis view or parasternal short-axis views. Definite concentric left ventricular hypertrophy was detected on the parasternal long-axis view. (B) Pericardial effusion was not observed on various apical views. (C) The mitral valve inflow velocity in terms of E and A velocity and mitral annulus tissue Doppler velocity as e’ and a’ velocities were clearly detected after pericardiocentesis.
Discussion
The hypertensive emergency with intracranial hemorrhage was the one of the clinical features of hypertensive crisis in this patient, and was associated with uncontrolled high blood pressure. The large amount of pericardial effusion was accompanied by profound hypothyroidism. This condition is contradictory when combined with large amount of pericardial effusion and hypertensive emergency. In contrast to previous reported cases [14–16], our patient initially presented with hypertensive emergency despite the base condition of massive pericardial effusion. Hypertensive emergency in combination with a large amount of pericardial effusion is uncommon.
Massive pericardial effusion almost to the point of cardiac tamponade is a rare complication of hypothyroidism. The identification of cardiac tamponade is difficult in this situation, as hypothyroidism may be mistaken for cardiac failure due to the symptoms of tachycardia, increased venous pressure, lower-limb edema, and increased cardiac size. In addition, typical signs of tamponade (hypotension, distant heart sounds, and increased jugular vein pressure) may be absent in patients with hypothyroidism [17]. In the present case, normal heart rate, rather than typical sinus tachycardia, was observed.
In hypothyroidism, pericardial fluid accumulates slowly, which allows the pericardium to accommodate the increased fluid volume by stretching, thus avoiding a significant rise in pericardial pressure. It is likely that increased albumin capillary leakage and impairment of lymphatic drainage resulted in significant accumulation of fluid over time, leading to tamponade [18,19].
Cardiac tamponade is defined as a state in which the heart is compressed due to fluid accumulation and increased intrapericardial pressure, resulting in cardiogenic shock and circulatory collapse [20]. Abnormal thyroid hormone function can cause an imbalance of the alpha- and beta-adrenergic receptors through changes in the synthesis and regulation of these receptors, leading to increased systemic vascular resistance. Moreover, hypothyroidism can cause water retention, resulting in increased preload [20,21]. Hypothyroidism is frequently associated with diastolic hypertension, as in the present case, in which hypertensive hypothyroidism occurred with systolic blood pressure of 213 mmHg and diastolic blood pressure of 124 mmHg.
Our patient lacked clinical signs of cardiac tamponade; nevertheless, a large amount of pericardial effusion with moderate respiratory distress and worsening dyspnea appears to be an appropriate indication for pericardiocentesis.
Echocardiography remains the most important test for the diagnosis of pericardial effusion, as this examination can facilitate evaluation of effusion size and enable the detection of changes in the amount of pericardial fluid after therapy through follow-up examinations [22]. Thyroid hormone replacement therapy leads to compete regression of pericardial effusion, and echocardiographic abnormalities are usually reversible in the hypothyroid heart. Chamber dilatation, reduced myocardial contractility, increased myocardial thickness, and enlargement of the left ventricular volume have also been described in early studies [18].
Testing of TSH levels for patients with acute pericarditis and various degrees of pericardial effusion is endorsed by the 2015 European Society of Cardiology Guidelines for the diagnosis and management of pericardial disease [23]. Routine evaluation of massive pericardial effusion (excluding common causes such as tuberculosis, malignancies, infections, and connective tissue disorders) should include thyroid function tests, even if there are no other signs or symptoms suggestive of hypothyroidism.
Conclusions
Massive pericardial effusion occurring in combination with severe hypothyroidism and myxedema is rare, even more so when accompanied by severe systemic hypertension [11,12,19,24]. The present case demonstrates an atypical presentation of cerebral hemorrhage as a hypertensive emergency associated with profound hypothyroidism with massive pericardial effusion. Management of large pericardial effusion can be effective as an invasive procedure with pericardiocentesis, even when based on the cause of other medical conditions.
Footnotes
Conflict of interest
None.
References:
- 1.Hardisty CA, Naik DR, Munro DS. Pericardial effusion in hypothyroidism. Clin Endocrinol (Oxf) 1980;13(4):349–54. doi: 10.1111/j.1365-2265.1980.tb03395.x. [DOI] [PubMed] [Google Scholar]
- 2.Kabadi UM, Kumar SP. Pericardial effusion in primary hypothyroidism. Am Heart J. 1990;120(6 Pt 1):1393–95. doi: 10.1016/0002-8703(90)90253-t. [DOI] [PubMed] [Google Scholar]
- 3.Kerber RE, Sherman B. Echocardiographic evaluation of pericardial effusion in myxedema. Incidence and biochemical and clinical correlations. Circulation. 1975;52(5):823–27. doi: 10.1161/01.cir.52.5.823. [DOI] [PubMed] [Google Scholar]
- 4.Yamanaka S, Kumon Y, Matsumura Y, et al. Link between pericardial effusion and attenuation of QRS voltage in patients with hypothyroidism. Cardiology. 2010;116(1):32–36. doi: 10.1159/000313464. [DOI] [PubMed] [Google Scholar]
- 5.Chahine J, Ala CK, Gentry JL, et al. Pericardial diseases in patients with hypothyroidism. Heart. 2019;105(13):1027–33. doi: 10.1136/heartjnl-2018-314528. [DOI] [PubMed] [Google Scholar]
- 6.Leonardi A, Penta L, Cofini M, et al. Pericardial effusion as a presenting symptom of hashimoto thyroiditis: A case report. Int J Environ Res Public Health. 2017;14(12):E1576. doi: 10.3390/ijerph14121576. pii: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Schmitt W, Roque D, Germano A. Massive pericardial effusion caused by hypothyroidism. Clin Case Rep. 2018;6(4):766–67. doi: 10.1002/ccr3.1447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ates I, Kaplan M, Yilmaz N. Newly diagnosed primary hypothyroidism applicant with massive pericardial effusion and acute renal failure. Endocr Regul. 2016;50(1):24–26. doi: 10.1515/enr-2016-0005. [DOI] [PubMed] [Google Scholar]
- 9.Klein I, Danzi S. Thyroid disease and the heart. Circulation. 2007;116(15):1725–35. doi: 10.1161/CIRCULATIONAHA.106.678326. [DOI] [PubMed] [Google Scholar]
- 10.Danzi S, Klein I. Thyroid abnormalities in heart failure. Heart Fail Clin. 2020;16(1):1–9. doi: 10.1016/j.hfc.2019.08.002. [DOI] [PubMed] [Google Scholar]
- 11.Machado C, Bhasin S, Nona W, Steinman RT. Hypothyroid cardiac tamponade presenting with severe systemic hypertension. Clin Cardiol. 1993;16(6):513–16. doi: 10.1002/clc.4960160612. [DOI] [PubMed] [Google Scholar]
- 12.Chou SL, Chern CH, How CK, et al. A rare case of massive pericardial effusion secondary to hypothyroidism. J Emerg Med. 2005;28(3):293–96. doi: 10.1016/j.jemermed.2004.11.017. [DOI] [PubMed] [Google Scholar]
- 13.Ristic AD, Imazio M, Adler Y, et al. Triage strategy for urgent management of cardiac tamponade: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2014;35(34):2279–84. doi: 10.1093/eurheartj/ehu217. [DOI] [PubMed] [Google Scholar]
- 14.Papakonstantinou PE, Gourniezakis N, Skiadas C, et al. Massive pericardial effusion without cardiac tamponade due to subclinical hypothyroidism (Hashimoto’s disease) Rural Remote Health. 2018;18(2):4384. doi: 10.22605/RRH4384. [DOI] [PubMed] [Google Scholar]
- 15.Fadel BM, Galzerano D, Pergola V, Di Salvo G. Massive pericardial effusion without cardiac tamponade. Eur Heart J. 2016;37(33):2612. doi: 10.1093/eurheartj/ehw076. [DOI] [PubMed] [Google Scholar]
- 16.Omura Y, Ugi S, Sugimoto T, et al. Massive pericardial effusion secondary to Hashimoto’s disease. Eur J Intern Med. 2007;18(5):438–40. doi: 10.1016/j.ejim.2007.05.001. [DOI] [PubMed] [Google Scholar]
- 17.Wang JL, Hsieh MJ, Lee CH, et al. Hypothyroid cardiac tamponade: Clinical features, electrocardiography, pericardial fluid and management. Am J Med Sci. 2010;340(4):276–81. doi: 10.1097/MAJ.0b013e3181e664c6. [DOI] [PubMed] [Google Scholar]
- 18.Sinha A, Yeruva SL, Kumar R, Curry BH. Early cardiac tamponade in a patient with postsurgical hypothyroidism. Case Rep Cardiol. 2015;2015:310350. doi: 10.1155/2015/310350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Manolis AS, Varriale P, Ostrowski RM. Hypothyroid cardiac tamponade. Arch Intern Med. 1987;147(6):1167–69. [PubMed] [Google Scholar]
- 20.Spodick DH. Acute cardiac tamponade. N Engl J Med. 2003;349(7):684–90. doi: 10.1056/NEJMra022643. [DOI] [PubMed] [Google Scholar]
- 21.Fletcher AK, Weetman AP. Hypertension and hypothyroidism. J Hum Hypertens. 1998;12(2):79–82. doi: 10.1038/sj.jhh.1000574. [DOI] [PubMed] [Google Scholar]
- 22.Pepi M, Muratori M. Echocardiography in the diagnosis and management of pericardial disease. J Cardiovasc Med (Hagerstown) 2006;7(7):533–44. doi: 10.2459/01.JCM.0000234772.73454.57. [DOI] [PubMed] [Google Scholar]
- 23.Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS) Eur Heart J. 2015;36(42):2921–64. doi: 10.1093/eurheartj/ehv318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Agarwal A, Chowdhury N, Mathur A, et al. Pericardial effusion with cardiac tamponade as a form of presentation of primary hypothyroidism. J Assoc Physicians India. 2016;64(12):98–100. [PubMed] [Google Scholar]