

Abstract
Burst wave lithotripsy (BWL) is a new non-invasive method for stone comminution using bursts of sub-megahertz ultrasound. A porcine model of urolithiasis and techniques to implement BWL treatment has been developed to evaluate its effectiveness and acute safety. Six human calcium oxalate monohydrate stones (6–7 mm) were hydrated, weighed, and surgically implanted into the kidneys of three pigs. Transcutaneous stone treatments were performed with a BWL transducer coupled to the skin via an external water bath. Stone targeting and treatment monitoring were performed with a co-aligned ultrasound imaging probe. Treatment exposures were applied in three 10-minute intervals for each stone. If sustained cavitation in the parenchyma was observed by ultrasound imaging feedback, treatment was paused and the pressure amplitude was decreased for the remaining time. Peak negative focal pressures between 6.5 and 7 MPa were applied for all treatments. After treatment, stone fragments were removed from the kidneys. At least 50% of each stone was reduced to <2 mm fragments. 100% of four stones were reduced to <4 mm fragments. Magnetic resonance imaging showed minimal injury to the functional renal volume. This study demonstrated that BWL could be used to effectively fragment kidney stones with minimal injury.
1. INTRODUCTION
Burst wave lithotripsy (BWL) is an experimental technology to noninvasively fragment kidney stones with bursts of focused ultrasound. BWL applies multicycle sinusoidal bursts of ultrasound instead of relying on shock waves with a single compression/tension cycle1. Successful fragmentation of natural and artificial stones using BWL has been demonstrated in vitro, with the ability to control the fragment size2, producing fragments small enough to potentially pass spontaneously and asymptomatically through the urinary tract. In a previous study applying a range of BWL exposures to porcine kidneys, it was demonstrated that renal injury correlates well with the onset of sustained cavitation in the renal parenchyma3. A subset of exposure parameters was identified from the previous study that caused minimal functional renal injury, but successfully fragmented stones in vitro. In the present study, an animal model was developed and used to assess the effectiveness of BWL treatment and potential renal injury.
2. METHODS
All protocols and procedures were approved by the University of Washington’s Institutional Animal Care and Use Committee. A 6–7 mm hydrated human kidney stone, with a primary composition of calcium oxalate monohydrate (COM), was surgically implanted in each kidney of three pigs via a small ureteral incision made in the proximal ureter. A burst wave lithotripsy ultrasound transducer with an inline ultrasound imaging probe was coupled by a small water bath placed on the flank, and the focus was aligned with the stone. Each stone was exposed to burst wave lithotripsy at 6.5 – 7 MPa (350 kHz, 10 Hz PRF and 0.057% duty factor) focal pressure for 30 minutes under real-time image guidance in 10 minute sets. One stone was not treated due to the poor acoustic window. After treatment, the kidneys were removed for injury analysis by gross, Magnetic Resonance Imaging (MRI) and histological assessment. Evaluation of hemorrhagic injury by MRI was performed as reported previously3. An expert in shock wave lithotripsy kidney injury performed a blinded examination of the slides. Stone fragments were retrieved from the kidney to determine the fraction of stone mass comminuted to pieces <2 or <4 mm.
3. RESULTS
Over the 5 treatments, an average 87% or 92% of the mass was comminuted to fragments <2 mm or <4 mm respectively (Figure 1a). In 3 of the 5 experiments, the stone was completely disintegrated. Many smaller fragments in the range of ~1–2 mm were recovered (Figure 2b). No indications of damage to the skin overlying the treatment site or intervening tissues were observed upon inspection. No bleeding or other injury was observed on the capsular surfaces of any of the 5 treated kidneys. Gross examination of the collecting space of the kidneys revealed minor petechial hemorrhagic injury to the urothelium immediately surrounding the area containing a majority of the stone fragments in each kidney (Figure 2a). Evaluation by MRI did not detect hemorrhagic injury to the functional renal volume. Histology showed damage to the mucosa of the collecting space in the vicinity of the stone (Figure 2b) with damage ranging from sloughing of the epithelium with small focal hemorrhagic spots to larger hemorrhagic regions extending through the full thickness of the lamina propria. This damage was limited to the immediate area of the stones and similar to the width of the ultrasound focus and stone (~1 cm diameter).
Figure 1:
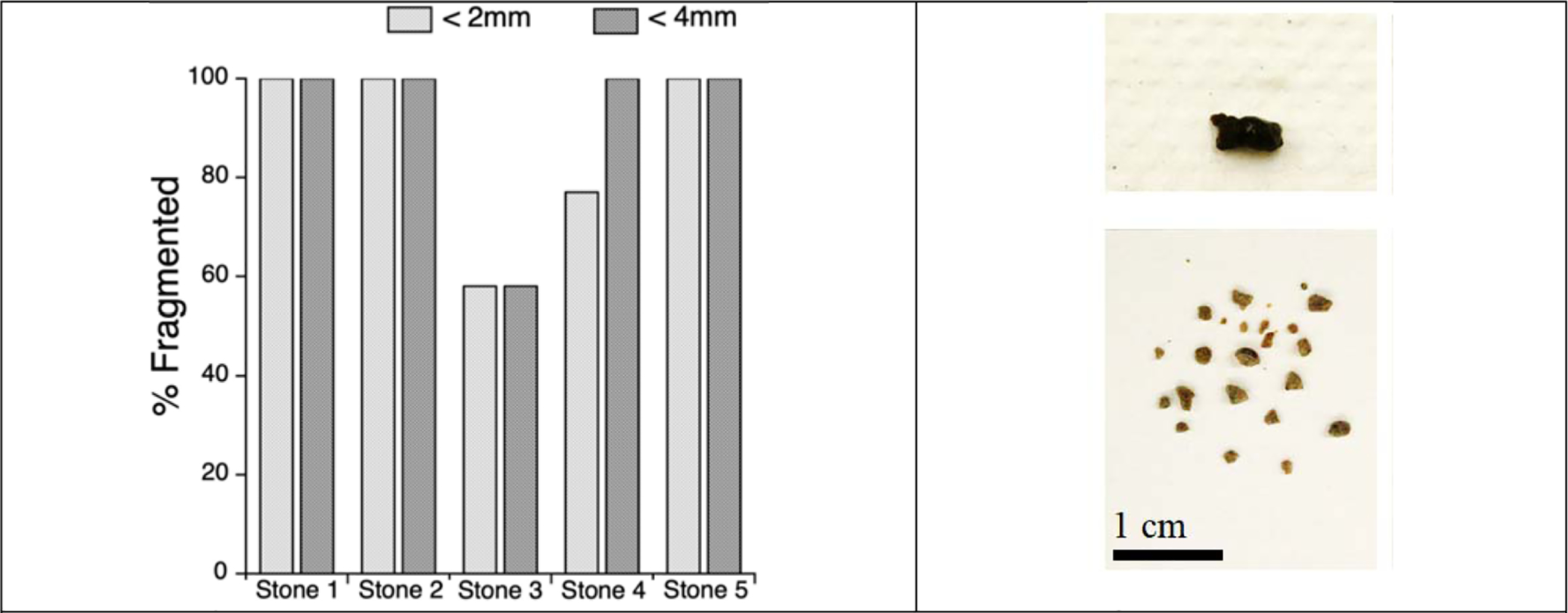
a) Bar chart showing the percent fragmentation of each treated stone to <2 and <4 mm. b) example of stone before treatment (top) and after treatment (bottom)
Figure 2:
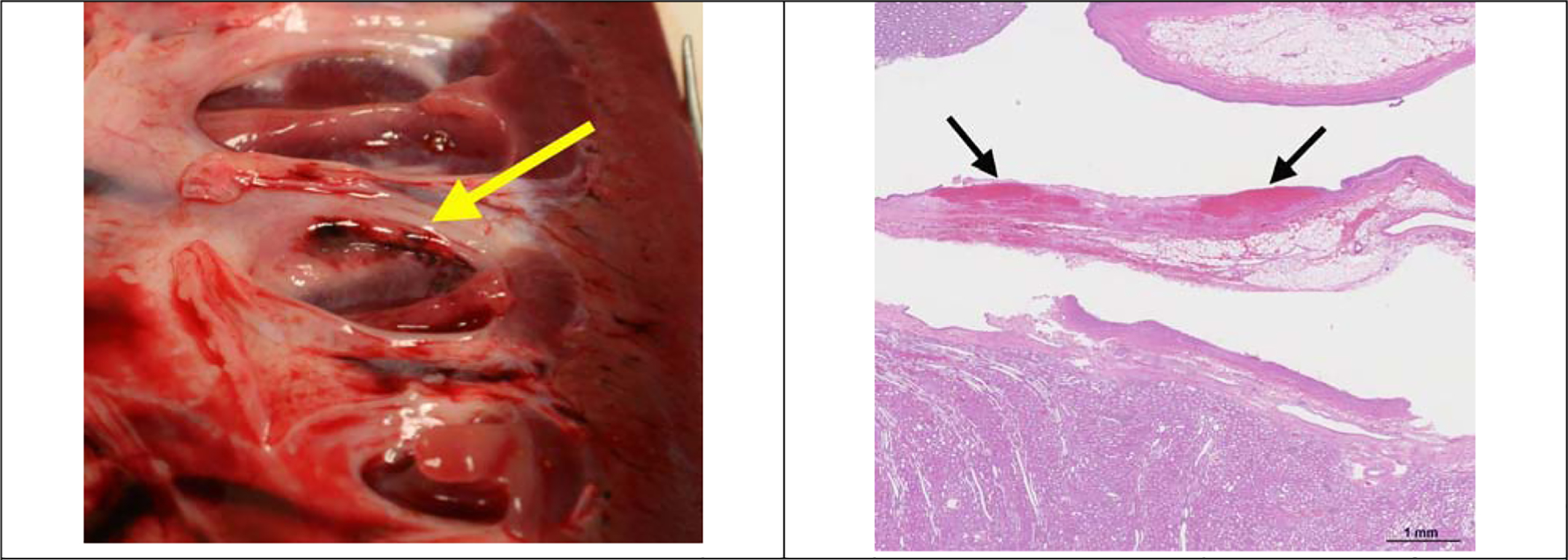
a) A freshly excised kidney exposed to 30-minute BWL treatment, showing petechial injury to the urothelium (yellow arrow) in the vicinity of the stone fragments. b) Histological section showing kidney section stained with hematoxylin and eosin. Focal mucosal injury and bleeding is observed in the location of treatment (arrows), extending to the lamina propria of the wall but not into the renal parenchyma.
4. CONCLUSION
We developed and implemented an animal model to perform clinical simulation of BWL to noninvasively fragment kidney stones. The results indicate that BWL can consistently produce stone fragments small enough to spontaneously pass. In addition, these data suggest such exposures produce minimal injury to the kidney and urinary tract.
ACKNOWLEDGMENTS
We acknowledge funding support from NIH through NIDDK P01 DK043881 and K01 DK104854. We thank our many co-workers not listed as authors on this paper.
REFERENCES
- 1.Cleveland RO, McAteer JA: Physics of Shock-Wave Lithotripsy Smith’s Textbook of Endourology: Wiley-Blackwell, pp. 527–558, 2012 [Google Scholar]
- 2.Maxwell AD, Cunitz BW, Kreider W et al. : Fragmentation of urinary calculi in vitro by burst wave lithotripsy. J Urol, 193: 338, 2015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.May PC, Kreider W, Maxwell AD et al. : Detection and Evaluation of Renal Injury in Burst Wave Lithotripsy Using Ultrasound and Magnetic Resonance Imaging. J Endourol, 31: 786, 2017 [DOI] [PMC free article] [PubMed] [Google Scholar]