

Abstract
Background:
Limited research has examined indicators of electronic cigarette (ECIG) dependence. Researchers have adapted ECIG dependence measures from cigarette smoking dependence measures, but few have examined unique aspects of ECIG dependence. This study used concept mapping, a mixed-methods approach to examine ECIG user-identified indicators of ECIG dependence.
Methods:
In 2019, we recruited current ECIG users (n = 75; 52.9% women; mean age = 33.2, SD = 9.9) from 25 states to complete an online study. Participants completed a brief survey and brainstormed statements (n=216) completing the prompt: “Something specific that makes me think I am addicted to using my electronic cigarette/vaping device is…” After duplicate content was removed, participants sorted the final list of 93 statements by content similarity and rated statements on how true statements were for them (1 – Definitely NOT true to 7 – Definitely true). Multidimensional scaling analysis identified ECIG dependence thematic clusters.
Results:
We identified ten themes: Craving, Negative Affect, Vaping as a Necessity, Therapeutic Effects, Preparedness, Attachment to Device, Impact on Daily Activity, Physical Withdrawal Symptoms, Monetary Cost, and Shame or Embarrassment. Those who had higher ECIG dependence scores and those who reported more frequent ECIG use had higher mean cluster ratings than those with lower ECIG dependence scores and who reported less frequent ECIG use. (ps<05).
Conclusions:
ECIG dependence has similarities to cigarette smoking dependence, but dependence indicators appear to be unique to ECIG use. Health professionals and the public should be aware of ECIG dependence risk and indicators.
Keywords: electronic cigarettes, dependence
1. Introduction
Electronic cigarette (ECIG) use has increased dramatically in recent years. Current ECIG use among U.S. high school students use increased from 1.5% in 2011 to 20.8% in 2018 (Arrazola et al., 2015; Gentzke, 2019; Jamal et al., 2017). Among adults, ECIG use has also increased with 2.8% of all U.S. adults (approximately 6.9 million people) and 5.2% of young adults reporting current ECIG use in 2017 (Wang et al., 2018). Therefore, there are growing concerns about ECIG dependence risk and how best to assess dependence considering potential indictors unique to ECIG use. Cigarette dependence has been well-characterized (Eissenberg, 2004; Glautier, 2004; Health and General, 1988; Henningfield and Fant, 1999; Hughes et al., 1984). Many measures exist to assess cigarette dependence among adults including the Fagerstrom Test of Nicotine Dependence (Heatherton et al., 1991) and the Wisconsin Inventory of Smoking Dependence Motives (Piper et al., 2004). Some research has shown that ECIGs may be associated with less abuse liability than combustible cigarettes (Barnes et al., 2017; McPherson et al., 2016; Vansickel et al., 2012). However, many ECIGs also deliver nicotine, with some that can deliver similar amounts of nicotine or more compared to a cigarette (Hiler et al., 2017; Wagener et al., 2017; Ramôa et al., 2016). Given the evidence that ECIG use has the potential to produce dependence, there is a need to measure ECIG dependence including potentially unique domains that cigarette smoking dependence measures may fail to identify.
Scales to measure ECIG dependence include the Penn State E-cigarette Dependence Index (Foulds et al., 2015) and the E-cigarette Dependence Scale (Morean et al., 2018). However, these scales were created by modifying or adapting cigarette smoking dependence scales and therefore may omit important aspects of ECIG dependence. There may be indicators of dependence for cigarette smoking that may not apply or translate well to ECIG dependence. For example, while one indicator of cigarette smoking dependence may be difficulty in abstaining from smoking where smoking is prohibited. However, ECIG users may find fewer restrictions (either self-imposed or from regulatory policies) regarding where ECIGs are prohibited. Therefore, an item examining difficulty abstaining where ECIG use is prohibited may perform poorly in assessing ECIG dependence. Additionally, because some ECIG characteristics (such as “flavors, vape clouds, contexts where ECIGs are used, and device customizability”) that may contribute to ECIG dependence are different from cigarettes (Bold et al., 2018), existing measures may not fully capture all aspects of ECIG dependence. As a result, ECIG users may engage in some behaviors that are indicative of dependence (such as concealing use indoors) that would not likely be performed by cigarette smokers. Indeed, others have noted that dependence on different products must be assessed differently given that ECIGs have characteristics unique from cigarettes (e.g., availability of flavors, less odor, etc.; Fagerström and Eissenberg, 2012). A better understanding of these unique ECIG dependence indicators may aid clinicians in treatment efforts for ECIG users who want to reduce their ECIG use and to inform future scale development. Thus, there is a need to examine if there are other indicators of dependence among ECIG users. This study’s purpose was to examine ECIG user-identified indicators of ECIG dependence by using concept mapping (Rosas and Kane, 2012), a validated mixed-method participatory approach.
2. Methods
2.1. Overview
This study was approved by the East Carolina University and Medical Center Institutional Review Board. This study used concept mapping, an approach that incorporates multiple steps including development of a focus prompt, brainstorming, sorting, rating, representation, data analysis, and interpretation (described further below). Briefly, participants responded to a prompt to brainstorm statements related to ECIG dependence and then sorted and rated these statements. Data from the participant sorting task were used to create a visual representation (i.e., a cluster map) of thematic clusters related to ECIG dependence. This method is ideally suited for identifying new domains of ECIG dependence because analyses yield a visual representation of thematic clusters, similar to an exploratory factor analysis, but do not require large sample sizes.
2.2. Participants
In 2019, we recruited adult current (past-30 day) ECIG users to participate in a study by posting advertisements on Craigslist websites in 12 states under the “et cetera” classified pages. We chose Craigslist markets by randomly selecting three states from each of the U.S. census regions (Northeast, Midwest, South, West; as in Soule et al., 2017a, 2017b). Respondents completed an online survey that included questions about demographics, ECIG use, and other tobacco use. Eligible participants were required to be over the age of 18 and be current (i.e., past-30 day) ECIG users who self-reported being “addicted to vaping/using electronic cigarettes,” expecting those who self-identified as being addicted to ECIG use would be most likely to be able to report indicators of addiction. Because the most common pattern of ECIG use among adults is “dual use” (i.e., users of ECIGs and cigarettes; Rodu & Plurphanswat, 2018), we included ECIG users who also reported current cigarette smoking in addition to exclusive ECIG users. Importantly, as noted in the focus prompt, participants were asked to identify indicators of dependence related to their ECIG use only, not cigarettes or other products. We used the word “addiction” because we felt this term is more universally understood than “dependence.” We invited 162 eligible individuals to complete the study and 75 participated (response rate = 46.3%).
2.3. Measures
Participants completed questions assessing tobacco use including age of first use, first product used, lifetime cigarette use (i.e., more than 100 lifetime cigarettes), tobacco products currently used, quantity and frequency of ECIG use, ECIG device and liquid characteristics, the four-item E-Cigarette Dependence Scale (Morean et al., 2018) questionnaire, and demographic questions.
2.4. Concept Mapping Procedures
To identify ECIG dependence themes, we used concept mapping (Trochim, 1989), a mixed-method participatory approach that has been used previously to examine ECIG use including reasons for use (Soule et al., 2016b), positive outcome expectancies (Soule et al., 2017a), and adverse effects (Soule et al., 2016a) and utilizes three participant tasks (brainstorming, sorting, and rating) described below.
2.5. Brainstorming
After completing tobacco use and demographic questions, participants completed the brainstorming task in which they provided statements that completed a prompt developed by the research team: “Something specific that makes me think I am addicted to using my electronic cigarette/vaping device is…” Participants completed this task individually, but all statements generated by participants were visible in a list to subsequent participants. We encouraged participants to provide several statements that completed the prompt and to review the statements provided previously to avoid duplication of content. We reviewed the statement list continuously and closed the brainstorming task after saturation was reached (i.e., additional participants no longer added statements with unique content). Participants generated 216 statements. Seventy-five participants completed brainstorming and received a $10 e-gift card.
2.6. Sorting
Five researchers reviewed independently the statements generated in the brainstorming task to remove statements. Statements that represented duplicate or redundant content (e.g., “First thing I reach for in the morning when I wake up” and “I wake up and I grab it”) or were unrelated to the focus prompt (e.g., “Feen [sic] to smoke hookah when I drink”) were candidates for removal. If three or more reviewers identified a statement as redundant or unrelated to the focus prompt, the statement was removed. Among duplicate content statements, the statements that were most complete (i.e., fully described a single idea) and were least complex (i.e., contained fewer words) were retained. Statement review and removal resulted in a final list of 93 statements. References to ECIGs in statements were changed to “vape/e-cigarette” in the final statement list for consistency.
We invited participants who completed the brainstorming task to complete the sorting and rating tasks. For the sorting task, participants organized all statements into “piles” of similar content. We instructed participants that there could not be a single pile containing all statements, piles could not be organized based on any other criteria than content similarity (e.g., true/false, does not apply to me, not important, etc.), and there could not be an “other” or miscellaneous pile. Participants completed the sorting task individually and received a $25 e-gift card. To verify participant sorting validity, each completed sorting activity was reviewed by the study team to determine if instructions were followed. While we did not have a specific set of pre-determined categories to reference and recognizing that many participants may group the statements differently, we reviewed participants’ categories to verify that there was some organization to the statement that followed the outlined instructions. Of the 41 participants who completed the sorting activity, 37 participants had verified sorts that followed instructions that were included in the representation analysis (below). A pooled study analysis indicates that model fit does not improve significantly beyond 40 sorting participants (Rosas and Kane, 2012).
2.7. Rating
After completing the sorting task, participants completed the rating task. These participants were the same participants who completed the sorting task that were recruited from the original participants who completed the brainstorming task: participants rated each statement based on the instructions: “Please rate each of the following statements in the range indicated below (1 – Definitely NOT true for me to 7 – Definitely true for me) based on how true each statement is for you.” Research staff reviewed participant ratings to determine validity (i.e., ensured variability in statement ratings and that participants had not provided repeated rating values for most of the statements). All 45 participants’ rating activities were verified and participants received a $10 e-gift card.
2.8. Representation
We used nonmetric multidimensional scaling (MDS) to generate a visual representation of the sorting data. A 93 x 93 matrix of similarities was created to identify the number of times each statement was sorted into the same pile by aggregating all participants’ sorting data. Using an algorithm (Kruskal and Wish, 1978), each statement was assigned a two-dimensional space coordinate (x,y) to create a “point map.” Points that are closer together represent statements that were sorted together by more participants (i.e., relate to more similar content) while points that are farther apart represent statements that were sorted together by fewer participants (i.e., relate to less similar content). The stress value, which measures the degree to which distances between points on the cluster map are discrepant from values in the matrix of similarities, ranges from 0 to 1 and is an indicator of goodness of fit of the final MDS representation. Lower values represent less discrepancies and better model fit. The stress value for this analysis was 0.28, similar to the average stress values reported in a pooled analysis of CM studies (Rosas and Kane, 2012) indicating good model fit.
2.9. Analysis and interpretation
We identified clusters of statements relating to ECIG dependence themes using hierarchical cluster analysis. Using an algorithm (Ward, 1963), non-overlapping clusters were identified by grouping statements together that minimized the distances between statements within a cluster. A “cluster map” (Figure 1) was created by enclosing points within clusters with polygon-shaped boundaries. Subsequent models were generated by using the same algorithm to add an additional cluster by dividing one cluster from the previous model into two clusters. We used this procedure until a final model was reached using interpretability (i.e., each cluster relates a single idea) and parsimony (i.e., simpler model/fewer clusters preferred) as indicators of good model fit through group discussion among the research team. Thus, the final model was both data driven and qualitatively assessed by the research team to meet the aforementioned criteria of interpretability and parsimony. We assigned names to the clusters that summarized the theme of the statement content within each cluster. We calculated mean cluster ratings by averaging all participant ratings of each statement within a cluster. We compared mean cluster ratings between sample subgroups based on participant demographics and tobacco use (gender, education, cigarette smoking status, flavor use, and mean E-Cigarette Dependence Scale score) using independent samples t-tests with an alpha level of 0.05.
Figure 1.
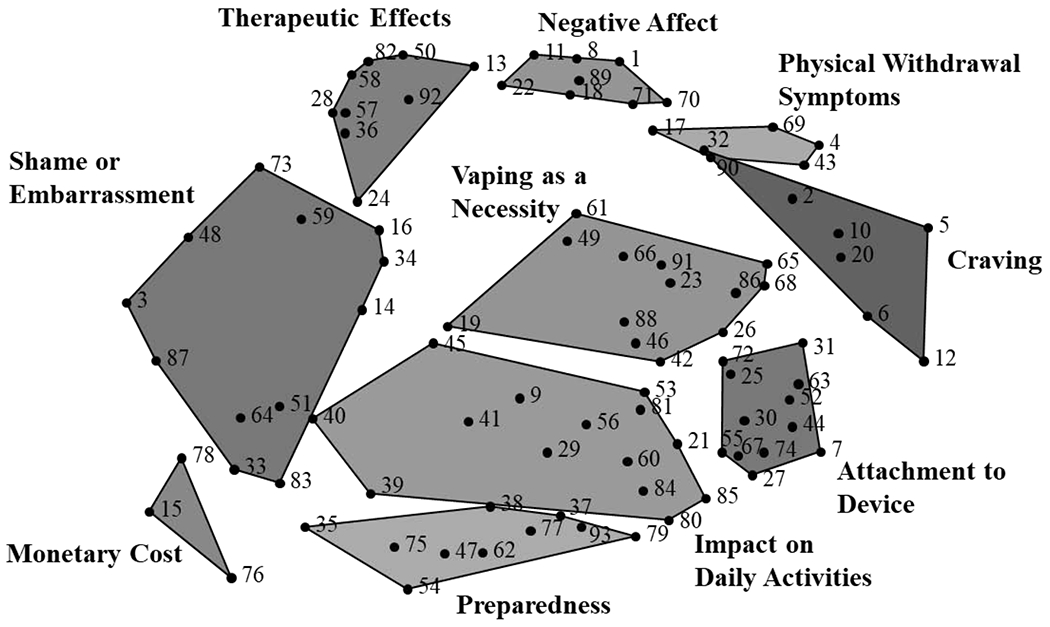
Concept map displaying 10 clusters ECIG user-identified statements describing indicators of ECIG addiction. Numbered points on the map that are closer to one another represent statements of more similar content whereas points on the map that are further apart represent statements of less similar content. Point numbers correspond to statements displayed in Table 2.
3. Results
3.1. Participant characteristics
Table 1 displays sample characteristics. Approximately half (52.9%) of participants were women. Most participants were white (84.3%), non-Hispanic (82.9%), had an average age of 33.2 (SD = 9.9), and 40% had a bachelor’s degree or higher. Most (84.3%) had smoked 100 or more cigarettes in their lifetime and around half (47.1%) were dual users of ECIGs and cigarettes. Nearly three quarters used ECIGs every day and 71.0% had been using ECIGs regularly for more than a year. Mean E-Cigarette Dependence Scale score was 2.5 (SD = 0.83) out of a possible 4.
Table 1.
Sample demographics and ECIG/tobacco use characteristics.
| Characteristic | N | % |
|---|---|---|
| Age (M, SD) | 33.2, 9.9 | |
| Sex | ||
| Female | 37 | 52.9 |
| Male | 31 | 44.3 |
| Transgender or other | 2 | 2.8 |
| Ethnicity | ||
| Hispanic/Latino(a) | 12 | 17.1 |
| Race | ||
| American Indian/Alaskan Native | 1 | 1.4 |
| Asian | 2 | 2.9 |
| Native Hawaiian/Pacific Islander | 1 | 1.4 |
| Black/African American | 3 | 4.3 |
| White/European American | 59 | 84.3 |
| More than one race | 4 | 5.7 |
| Education | ||
| High School diploma or GED | 12 | 17.2 |
| Some college credit, but less than 1 year | 8 | 11.4 |
| 1 or more years of college, no degree | 14 | 20.0 |
| Associate’s degree | 8 | 11.4 |
| Bachelor’s degree | 20 | 28.6 |
| Higher than a bachelor’s degree | 8 | 11.4 |
| Regular ECIG use history1 | ||
| 0-3 months | 5 | 7.3 |
| 4-6 months | 6 | 8.7 |
| 7-12 months | 9 | 13.0 |
| Between 1-2 years | 25 | 36.2 |
| More than 2 years | 24 | 34.8 |
| ECIG frequency | ||
| At least once per day | 10 | 14.3 |
| Every once in a while throughout the day | 9 | 12.9 |
| Fairly frequently throughout the day | 32 | 45.7 |
| Almost always throughout most of the day | 19 | 27.1 |
| Regular ECIG device | ||
| Prefilled disposable/Cig-alike | 7 | 10.0 |
| E-hookah | 2 | 2.9 |
| Vape pen/eGo style device | 9 | 12.9 |
| Rebuildable/Mechanical Mod or Box Mod | 19 | 27.1 |
| E-cigar | 2 | 2.9 |
| Pod mod such as JUUL | 31 | 44.3 |
| ECIG liquid nicotine concentration2 | ||
| 1-4 mg/ml | 18 | 25.7 |
| 5-10 mg/ml | 20 | 28.6 |
| 11-20 mg/ml | 20 | 28.6 |
| 20+ mg/ml | 10 | 14.3 |
| Don’t know | 2 | 2.9 |
| ECIG liquid flavor preference | ||
| Menthol or mint | 19 | 27.1 |
| Tobacco | 16 | 22.9 |
| Fruit | 23 | 32.9 |
| Other (including clove, spice, nut, alcoholic drink, coffee/tea, candy, or dessert) | 8 | 11.4 |
| I usually use multiple flavors | 4 | 5.7 |
| ECIG use after waking | ||
| After 60 minutes | 14 | 20.0 |
| 31-60 minutes | 15 | 21.4 |
| 6-30 minutes | 22 | 31.4 |
| Within 5 minutes | 19 | 27.1 |
| E-Cigarette Dependence Scale - Reach for ECIG3 | ||
| Never | 1 | 1.4 |
| Rarely | 2 | 2.9 |
| Sometimes | 23 | 32.9 |
| Often | 30 | 42.9 |
| Almost always | 14 | 20.0 |
| E-Cigarette Dependence Scale – Vape more before not allowed3 | ||
| Rarely | 4 | 5.7 |
| Sometimes | 18 | 25.7 |
| Often | 27 | 38.6 |
| Almost always | 21 | 30.0 |
| E-Cigarette Dependence Scale - Drop everything to buy ECIGs3 | ||
| Never | 4 | 5.7 |
| Rarely | 14 | 20.0 |
| Sometimes | 29 | 41.4 |
| Often | 12 | 17.1 |
| Almost always | 11 | 15.7 |
| E-Cigarette Dependence Scale - Craving gets intolerable3 | ||
| Never | 4 | 5.7 |
| Rarely | 14 | 20.0 |
| Sometimes | 29 | 17.1 |
| Often | 12 | 17.1 |
| Almost always | 11 | 15.7 |
| Lifetime use of 100+ cigarettes | ||
| Yes | 59 | 84.3 |
| Current use of other tobacco products | ||
| Cigarettes | 40 | 57.1 |
| Cigar | 14 | 20.0 |
| Cigarillo or little cigar | 15 | 22.0 |
| Smokeless | 3 | 4.3 |
| Waterpipe | 11 | 15.7 |
Note. Total n and percentages for sample characteristics is based on the 70 participants who completed the participant questions. Five participants completed brainstorming but did not complete the participant questions.
Regular use was defined as using an ECIG some days or most days.
Response options for liquid nicotine concentration ranged from 0 to 36 mg/ml. Some pod mods, such as Juul, contain liquids that have concentrations higher than 36 mg/ml.
Items from the 4-item E-Cigarette Dependence Scale (Morean et al., 2018) including “I find myself reaching for my e-cigarette without thinking about it,” “I drop everything to go out and buy e-cigarettes or e-juice,” I vape more before going into a situation where vaping is not allowed,” and “When I haven’t been able to vape for a few hours, the craving gets intolerable.”
3.2. Concept mapping results
The final model included 10 clusters (see Figure 1 and Table 2). Each cluster is described below and presented from highest to lowest mean cluster rating.
Table 2.
ECIG user-identified clusters and statements describing indicators of ECIG addiction.
| Cluster | Statement | Average Rating |
|---|---|---|
| Craving | 5.36 | |
| 20. I have cravings to vape. | 5.71 | |
| 12. I crave my vape/e-cigarette after activities like eating. | 5.62 | |
| 32. Vaping satisfies my cravings. | 5.49 | |
| 6. If I try to go a full day without vaping, I realize I want to vape all the time. | 5.44 | |
| 5. I crave the taste of vaping. | 5.22 | |
| 2. I constantly crave the feeling of vaping. | 5.04 | |
| 10. I feel the urge to vape that comes out of nowhere. | 4.96 | |
| Physical Withdrawal Symptoms | 4.22 | |
| 17. I cannot relax without my vape/e-cigarette. | 5.02 | |
| 4. I have withdrawal symptoms. | 4.71 | |
| 90. I cannot concentrate without my vape/e-cigarette. | 4.29 | |
| 69. I get headaches with my very strong cravings to vape. | 3.89 | |
| 43. My hands and arms start trembling if I have not vaped in a while. | 3.20 | |
| Negative Affect | 5.17 | |
| 8. I feel nervous and worried when I cannot find my vape/e-cigarette. | 5.93 | |
| 1. I get anxious when I cannot use my vape/e-cigarette. | 5.58 | |
| 11. I get anxious when I run out of e-liquid/pods. | 5.42 | |
| 18. I get agitated without my vape. | 5.36 | |
| 89. I get upset when my vape/e-cigarette dies. | 5.13 | |
| 71. When my vape/e-cigarette is not working I panic. | 4.93 | |
| 70. I freak out when my vape/e-cigarette is not around. | 4.76 | |
| 22. I feel depressed without my vape/e-cigarette. | 4.24 | |
| Therapeutic Effects | 4.85 | |
| 82. I feel calm after I vape. | 5.40 | |
| 92. I like the buzz and relaxed notion of vaping. | 5.33 | |
| 50. Vaping relieves my stress. | 5.30 | |
| 58. I feel happy when I vape. | 5.07 | |
| 13. After I vape, my anxiety goes away. | 5.02 | |
| 36. I feel secure with my vape/e-cigarette. | 4.80 | |
| 28. Vaping reduces my stress allowing me to enjoy my time with my family/kids. | 4.45 | |
| 57. After I vape, it feels like everything is alright. | 4.38 | |
| 24. Puffing my vape/e-cigarette is the most enjoyable part of my day. | 3.89 | |
| Attachment to Device | 4.70 | |
| 7. I vape right before I go to bed. | 5.80 | |
| 25. I need to know where my vape/e-cigarette is at all times. | 5.56 | |
| 67. I keep my vape/e-cigarette next to my nightstand or close by when I go to sleep. | 5.56 | |
| 52. I find myself reaching for my vape/e-cigarette without thinking. | 5.43 | |
| 31. I need my vape/e-cigarette with me at all times. | 5.38 | |
| 27. I always check my pocket for my vape/e-cigarette. | 5.27 | |
| 74. I need to have my vape/e-cigarette while driving. | 5.18 | |
| 63. I need to vape as soon as I wake up. | 5.16 | |
| 72. I cannot imagine a day without my vape/e-cigarette by my side. | 4.38 | |
| 44. I wake up in the middle of the night to vape. | 3.39 | |
| 55. I sleep with my vape/e-cigarette in my hand. | 2.80 | |
| 30. I have dreams about vaping. | 2.47 | |
| Vaping as a Necessity | 4.86 | |
| 46. My vape/e-cigarette is always my first choice. | 5.80 | |
| 42. I need to vape every day. | 5.70 | |
| 68. If I cannot find my vape/e-cigarette, I search frantically. | 5.33 | |
| 19. When I am someplace I cannot vape, I think about when I will be able to use my vape/e-cigarette again. | 5.24 | |
| 86. I absolutely need to vape. | 5.04 | |
| 65. I cannot go long without vaping. | 5.00 | |
| 49. I do not get as much of a buzz from vaping as I used to. | 4.98 | |
| 88. I do not see myself stopping vaping. | 4.49 | |
| 26. I have to vape constantly. | 4.47 | |
| 66. When I am out in public and my vape/e-cigarette is at home, it is all I can think about. | 4.47 | |
| 61. I have to vape soon after I eat anything, otherwise my stomach does not feel settled. | 4.40 | |
| 23. I cannot live without my vape/e-cigarette. | 4.27 | |
| 91. I think about vaping all the time. | 4.02 | |
| Impact on Daily Activity | 4.55 | |
| 80. I do not leave my home without my vape/e-cigarette. | 5.91 | |
| 21. If I leave my home and I realize I forgot my vape/e-cigarette, I have to go back and get it. | 5.42 | |
| 85. Vaping is a huge part of my daily rituals. | 5.31 | |
| 45. I want to vape at work. | 5.30 | |
| 81. I need to vape while I have been drinking. | 5.18 | |
| 84. I take breaks from what I am doing to vape. | 5.00 | |
| 41. When I am driving and I have no more e-liquid/pod refills I feel like I have to stop somewhere immediately for refills. | 4.40 | |
| 56. I vape all the time if it is not prohibited. | 4.27 | |
| 29. I normally do not need to take breaks at work, but now I do so I can hit my vape/e-cigarette. | 4.25 | |
| 60. I cannot keep myself from using my vape/e-cigarette after I have brushed my teeth for the night, which is causing tooth decay. | 4.09 | |
| 9. I will use disgusting, burnt coils if I cannot get a new one quickly enough. | 4.02 | |
| 39. I search the internet for stuff about vaping. | 3.69 | |
| 40. If I am not allowed to vape somewhere, I am less likely to go there. | 3.60 | |
| 53. My life revolves around me vaping. | 3.23 | |
| Preparedness | 4.70 | |
| 79. When I travel, I always make sure I pack my vape/e-cigarette supplies with me. | 5.98 | |
| 77. I always make sure I have e-liquid/pods. | 5.53 | |
| 93. I make sure my battery is charged at all times. | 5.51 | |
| 37. I am always aware of how much e-liquid/how many pods I have. | 5.49 | |
| 47. I go through e-liquid/pods very quickly. | 4.98 | |
| 54. I always have e-liquid/pods on my shopping list and I will not forget it. | 4.67 | |
| 35. I try to go places where I am allowed to vape. | 4.00 | |
| 62. If I do not have money to buy vape/e-cigarette products, I will do whatever I can to get money so I can buy the products. | 3.98 | |
| 38. I keep multiple vapes/e-cigarettes charged so I always have one available. | 3.51 | |
| 75. I will buy a disposable vape/e-cigarette if mine is not charged. | 3.36 | |
| Shame or Embarrassment | 3.87 | |
| 16. I love vaping, though I wish I did not. | 5.09 | |
| 51. I vape in locations I should not. | 4.86 | |
| 48. I get excited about going to the store for e-liquid/pods and vape accessories. | 4.66 | |
| 83. I hide in the bathroom to vape in secret. | 4.07 | |
| 59. I cannot enjoy activities without my vape/e-cigarette. | 3.91 | |
| 87. I conceal my vaping when in public. | 3.84 | |
| 3. I do not want my friends and family to know how often I vape. | 3.71 | |
| 14. I look forward to times that I can stay in and vape all night. | 3.64 | |
| 64. I like to try new flavors daily. | 3.56 | |
| 34. I often unintentionally skip meals because vaping tricks my brain into thinking I have eaten. | 3.42 | |
| 73. I have cried when I think about how addicted I am to vaping because I am ashamed. | 3.04 | |
| 33. I find myself talking about vaping too much with friends. | 2.59 | |
| Monetary Cost | 4.17 | |
| 15. I spend too much money on vaping. | 4.96 | |
| 78. If I do not have money to buy e-liquid/pods, I will ration out my vaping to when I am stressed. | 4.73 | |
| 76. I bought a very expensive carrying case for my vape/e-cigarette stuff. | 2.82 | |
Note. Statement numbers correspond to points in Figure 1.
3.2.1. Craving.
The Craving cluster (mean rating=5.46, SD=0.27) included seven statements. While all statement in this cluster described ECIG related cravings, some were more general (e.g., “I have cravings to vape”) whereas others were more specific and described craving the taste, feeling of vaping, or craving vaping after activities such as eating.
3.2.2. Negative Affect.
This cluster of eight statements (M=5.17, SD=0.49) had the second highest mean cluster rating. Statements in the Negative Affect cluster described negative experiences resulting from brief vaping abstinence periods and focused on psychological symptoms. These symptoms were associated with the inability to vape for many reasons including not being able to find one’s ECIG, running out of ECIG liquid or battery, or a malfunctioning ECIG. Participants described negative affect as nervousness, anxiety, getting upset, depression, or panic.
3.2.3. Vaping as a Necessity.
This cluster had 13 statements (M=4.86, SD=0.54) and included descriptions of “needing” to vape as summarized by the highest rated statement in the cluster, “My vape/e-cigarette is always my first choice.” Some statements described needing to vape “constantly” or “every day.” Some statements described tolerance (e.g., “I do not get as much of a buzz from vaping as I used to”). Other statements described how participants thought about vaping such as “When I am someplace I cannot vape, I think about when I will be able to use my vape/e-cigarette again.” and “I think about vaping all the time.”
3.2.4. Therapeutic Effects.
While the Craving, Physical Withdrawal Symptoms, and Negative Affect clusters described the negative outcomes associated with abstaining from ECIG use, the nine statements in the Therapeutic Effects cluster (M=4.85, SD=0.48) described the positive feelings that resulted after vaping. Statements described feeling calm or relaxed after vaping. Some statements also described how vaping reduced anxiety and stress (e.g., “After I vape, my anxiety goes away.”). Several statements described how vaping caused happiness: “Puffing my vape/e-cigarette is the most enjoyable part of my day.”
3.2.5. Preparedness.
The Preparedness cluster (n=10; M=4.70, SD=0.89) described precautions or actions to avoid situations that prevented vaping. For example, the highest rated statement described that “When I travel, I always make sure I pack my vape/e-cigarette supplies with me.” Other statements described how participants always were aware of how much battery or ECIG liquid they had and made sure to not run out of either. Precautions included keeping multiple ECIG device charged, always having ECIG liquid on a shopping list, or buying disposable devices if their usual device was not charged. One statement also described going to places “where I know I am allowed to vape.”
3.2.6. Attachment to Device.
The 12 statements in this cluster (M=4.70, SD=1.11) described how ECIG users were in frequent contact and close proximity to their ECIG devices throughout the day. For example, several statements related to vaping before, during, and after going to bed: “I vape right before I go to bed,” “I keep my vape/e-cigarette…close by when I go to sleep,” and “I need to vape as soon as I wake up.” Other statements described the preoccupation of needing to know where one’s ECIG was: “I find myself reaching for my vape/e-cigarette without thinking,” and “I always check my pocket for my vape/e-cigarette.” This cluster also had the greatest range in statement ratings with the highest rated statement (“I vape right before I got to bed.”) being 3.33 points greater than the lowest rated statement (“I have dreams about vaping.”).
3.2.7. Impact on Daily Activity.
This cluster had the most statements (n=14; M=4.55, SD=0.78) and described how vaping fit in with common life events (e.g., “Vaping is a huge part of my daily rituals.”). Statements described how participants would return home to retrieve their ECIG if they left home without it. Several statements described needing or choosing to take breaks at work or from other tasks to vape. Some statements suggested the intertwining of ECIG use and other activities was undesired: “When…I have no more e-liquid/pod refills I feel like I have to stop somewhere immediately…” and “I cannot keep myself from using my vape/e-cigarette after I have brushed my teeth…”
3.2.8. Physical Withdrawal Symptoms.
The five statements in this cluster (M=4.22, SD=0.64) described withdrawal symptoms that occur after vaping abstinence, particularly physical symptoms. While one statement described having “withdrawal symptoms,” others were more specific and related to irritability/discomfort associated with not being able to vape including “I cannot relax without my vape/e-cigarette.” Other symptoms related to physiological withdrawal symptoms including getting “headaches” or “My hands and arms start trembling if I have not vaped in a while.
3.2.9. Monetary cost.
This cluster had the least number of statements (n=3; M=4.17, SD=0.27). These statements included descriptions of spending too much money on vaping, vaping supplies, and attempting to ration vaping when funds were low.
3.2.10. Shame or Embarrassment.
The 12 statements in this cluster had the lowest mean rating (M=3.87, SD=0.70) and described behaviors and cognitions that indicated ECIG users associated their vaping with negative stigma. As a result of this perception, statements demonstrated how some ECIG users would conceal their vaping from others such as “I conceal my vaping when in public,” and “I do not want my family and friends to know how often I vape.” Other statements described how participants would hide or vape in seclusion as demonstrated by the statements “I hide in the bathroom to vape in secret.” or “I look forward to times that I can stay in and vape all night.” The highest rated statement, “I love vaping, though I wish I did not,” suggested that participants saw vaping as a behavior that was both enjoyable, but something they were ashamed of.
3.3. Cluster ratings comparisons
Relative to men, women rated the Negative Affect, Therapeutic Effects, Craving, and Vaping as a Necessity clusters higher (i.e., more true; ps < .05). Compared those with a bachelor’s degree or higher, those who did not have a bachelor’s degree rated the Negative Affect, Therapeutic Effects, Physical Withdrawal Symptoms, Craving, Vaping as a Necessity, and Impact on Daily Activity clusters higher (ps < .05). Exclusive ECIG users and dual cigarette and ECIG users did not differ significantly on their ratings of any of the clusters. Those who reported ECIG use frequency as “Almost always throughout most of the day” rated the Negative Affect, Craving, and Vaping as a Necessity clusters higher than those who used ECIGs “At least once per day,” “Every once in a while throughout the day,” or “Fairly frequently throughout the day” (ps < .05). Relative to participants who had mean E-Cigarette Dependence Scale scores of 2 (out of 4) or less, participants who had mean E-Cigarette Dependence Scale scores greater than 2 had higher ratings for the Negative Affect, Therapeutic Effects, Physical Withdrawal Symptoms, Craving, Vaping as a Necessity, and Impact on Daily Activity clusters (ps < .05; See Figure 2).
Figure 2.
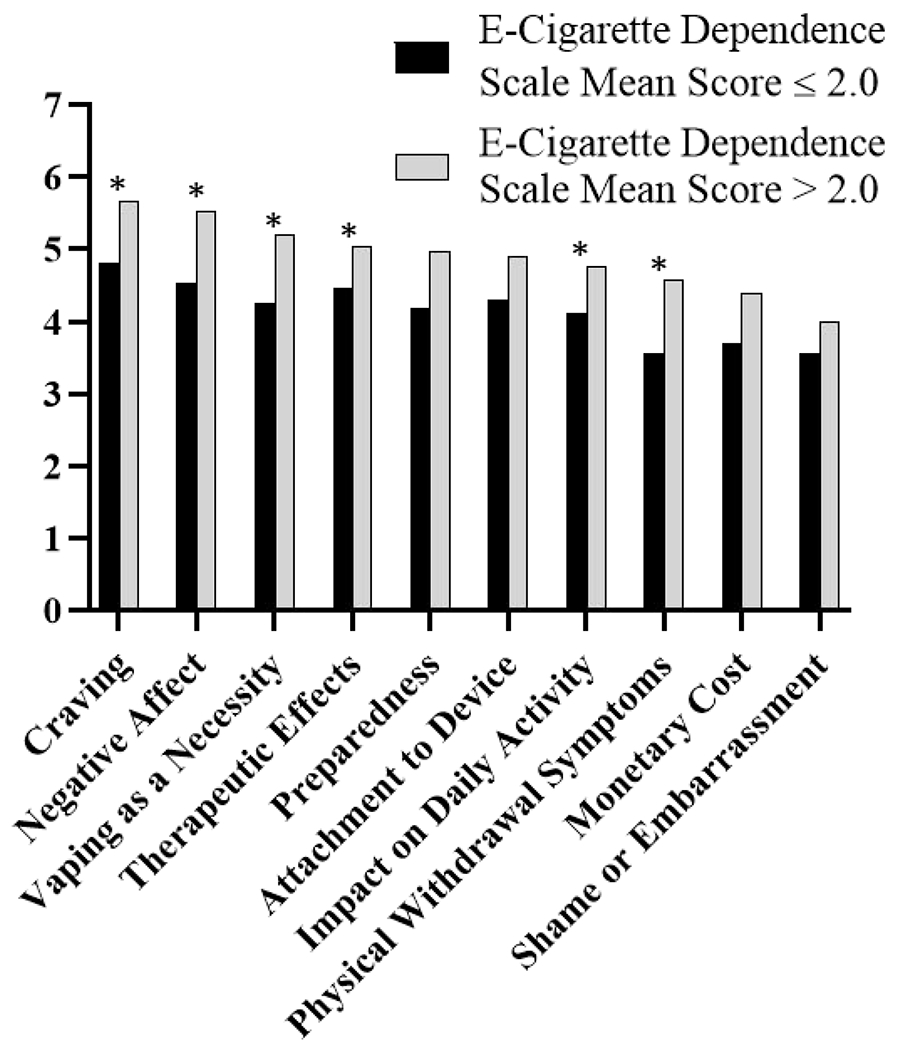
Mean cluster ratings among participants with E-Cigarette Dependence Scale24 mean scores ≤ 2.0 and > 2.0. * indicates significant difference (p < .05).
4. Discussion
We identified 10 ECIG dependence themes including domains related to physical dependence such as cravings, withdrawal symptoms, and withdrawal symptom suppression, domains similar to cigarette dependence. Participant responses suggested ECIG dependence is associated with psychological effects such as negative affect and anxiety associated with ECIG abstinence as well as stress relief and affect regulation after ECIG use. ECIG users reported that they needed to be near or in physical contact with their ECIG devices and that they take precautions to avoid situations where they are unable to vape. These actions appear to affect many aspects of ECIG users’ daily activities. Finally, some ECIG users who felt they were addicted to ECIG use viewed their own ECIG use negatively, recognized the monetary cost of their ECIG use, and described feelings of shame, embarrassment, and attempts to hide their own ECIG use. While many of these ECIG dependence symptoms are similar to cigarette dependence, our study identifies unique aspects of ECIG dependence such as physical attachment to the device and shame and embarrassment. Additionally, in instances where ECIG and cigarette domains may be similar, such as preparedness, items may require more than replacing “cigarettes” with “electronic cigarettes” (e.g., needing to having batteries charged, liquid refills, other vaping supplies vs. cigarettes and lighters).
This is the first study to examine indicators of ECIG dependence by generating statements identified by ECIG users. In a review of published measures on tobacco dependence, 10 domains were identified as important indicators of ECIG dependence including quantity and frequency of use, tolerance, perceived benefits, withdrawal symptoms, cravings/urge to use, use despite harm, impaired control, automaticity, preferred over competing rewards, and sensory dependence (Bold et al., 2018). Many of the statements identified in the current study are consistent with these domains. Consistent with other studies, mean cluster ratings were higher for participants who had higher mean E-Cigarette Dependence Scale (Morean et al., 2018) scores (see Figure 2).
The clusters identified in this study also describe potentially unique domains or items that may be important for assessing ECIG addiction. In particular, the statements within the Shame/Embarrassment, Preparedness, Impact on Daily Activity, and Attachment to Device clusters describe additional emotional and behavioral indicators of addiction that may be more relevant to ECIG use than other tobacco use behaviors. For example, ECIG use in a bathroom or other prohibited location or concealing vaping from others may be easier to do than with cigarettes because of the ability to take a single puff that does not emit a strong odor versus smoking an entire cigarette that produces a more recognizable “smoke” smell. Research has shown that “stealth vaping,” or vaping discreetly where ECIG use is prohibited, is predicted by greater ECIG dependence (Yingst et al., 2018). While it is true that use in prohibited locations may also occur among cigarette smokers, the product characteristics of ECIGs may make this behavior and others that are indicative of dependence more common among ECIG users. Future studies should examine whether psychological and behavioral indicators of dependence are useful for predicting negative outcomes associated with ECIG use such as negative health effects or decreased successful cessation attempts among ECIG users who wish to reduce their ECIG use.
Our findings can inform psychometric scale development efforts to create and validate short ECIG dependence scales. ECIG dependence scales that capture these unique ECIG dependence domains or use wording that is more specific to ECIG use experiences (and therefore dependence) may be useful for identifying if ECIG user characteristics are more associated with certain ECIG dependence domains. That is, just as some ECIG users report ECIG use for different reasons, different domains of ECIG dependence may be more salient for different ECIG users. Additionally, given that youth represent the population with the greatest ECIG use prevalence and ECIG dependence may manifest differently among youth than among adults, future studies should also examine unique aspects of youth ECIG dependence.
This study had several limitations. The small sample may limit the generalizability of the findings, however, this sample size is sufficient for concept mapping and participants were recruited from across the United States using an approach that generalizes well when not attempting to measure prevalence (Jeong et al., 2019). Additionally, because the study was conducted online, we relied on self-report measures. This weakness can be balanced against the wide geographic reach of our recruitment. Because participants were required to report specific indicators of ECIG dependence, there may be other indicators of ECIG dependence that were not identified in the current study, perhaps because ECIG users are unaware or do not wish to share them. We did not assess if participants used other substances besides nicotine in their ECIGs. Because of this and that many participants reported current cigarette smoking, participant responses may have been influences by dependence to other substances or products. Finally, the ECIG addiction domains identified are not specific to ECIG device characteristics (e.g., type, nicotine concentration, flavors, etc.). Future studies with larger samples may be better suited to determine if certain ECIG devices are more associated with indicators of ECIG dependence.
5. Conclusions
ECIG users report a range of indicators of ECIG dependence. ECIG dependence appears to have similarities to cigarette smoking dependence, but the current study shows that there are unique characteristics of ECIG dependence. ECIG product characteristics that differ from cigarettes may help to explain some of these differences such as “attachment to device” and may contribute to abuse liability. As ECIG use grows in popularity, there may be more ECIG users who become dependent on ECIGs. Given the increasing prevalence of ECIG use and the evidence of ECIG use dependence potential, health professionals should be aware and prepared to address this emerging public health threat.
Highlights.
ECIG users report many indicators of ECIG dependence.
ECIG dependence may have domains that are unique from cigarette smoking dependence.
ECIG product characteristics may contribute to unique indicators of dependence.
Future ECIG dependence measures should consider additional ECIG dependence domains.
Acknowledgments
Funding
This research was supported by the National Institute on Drug Abuse of the National Institutes of Health under Award Number 2U54DA036105-06 and the Center for Tobacco Products of the U.S. Food and Drug Administration. The content is solely the responsibility of the authors and does not necessarily represent the official views of NIH or the FDA.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflict of Interest
The authors have no conflicts to report.
References
- Arrazola RA, Singh T, Corey CG, Husten CG, Neff LJ, Apelberg BJ, Bunnell RE, Choiniere CJ, King BA, Cox S, McAfee T, Caraballo RS, Centers for Disease Control and Prevention (CDC), 2015. Tobacco use among middle and high school students - United States, 2011-2014. MMWR Morb. Mortal. Wkly. Rep 64, 381–385. [PMC free article] [PubMed] [Google Scholar]
- Barnes AJ, Bono RS, Lester RC, Eissenberg TE, Cobb CO, 2017. Effect of Flavors and Modified Risk Messages on E-cigarette Abuse Liability. Tob. Regul. Sci 3, 374–387. 10.18001/TRS.3.4.1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bold KW, Sussman S, O’Malley SS, Grana R, Foulds J, Fishbein FL, Krishnan-Sarin S, 2018. Measuring E-cigarette dependence: Initial guidance. Addict. Behav 79, 213–218. 10.1016/j.addbeh.2017.11.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eissenberg T, 2004. Measuring the emergence of tobacco dependence: the contribution of negative reinforcement models. Addiction 99, 5–29. [DOI] [PubMed] [Google Scholar]
- Fagerström K, Eissenberg T, 2012. Dependence on Tobacco and Nicotine Products: A Case for Product-Specific Assessment. Nicotine Tob. Res 14, 1382–1390. 10.1093/ntr/nts007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Foulds J, Veldheer S, Yingst J, Hrabovsky S, Wilson SJ, Nichols TT, Eissenberg T, 2015. Development of a Questionnaire for Assessing Dependence on Electronic Cigarettes Among a Large Sample of Ex-Smoking E-cigarette Users. Nicotine Tob. Res 17, 186–192. 10.1093/ntr/ntu204 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gentzke AS, 2019. Vital Signs: Tobacco Product Use Among Middle and High School Students — United States, 2011–2018. MMWR Morb. Mortal. Wkly. Rep 68 10.15585/mmwr.mm6806e1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glautier S, 2004. Measures and models of nicotine dependence: positive reinforcement. Addiction 99, 30–50. [DOI] [PubMed] [Google Scholar]
- Health, C. for H.P. and E.O. on S. and, General, U.S.P.H.S.O. of the S., 1988. The Health Consequences of Smoking: Nicotine Addiction: A Report of the Surgeon General [WWW Document], DHHS Publ. No CDC 88-8406. URL https://prof1les.nlm.nih.g0v/NN/B/B/Z/D/ (accessed 6.11.19).
- Heatherton TF, Kozlowski LT, Frecker RC, Fagerström KO, 1991. The Fagerstrom Test for Nicotine Dependence: a revision of the Fagerstrom Tolerance Questionnaire. Br. J. Addict 86, 1119–1127. [DOI] [PubMed] [Google Scholar]
- Henningfield JE, Fant RV, 1999. Tobacco use as drug addiction: the scientific foundation. Nicotine Tob. Res 1 Suppl 2, S31–35. 10.1080/14622299050011781 [DOI] [PubMed] [Google Scholar]
- Hiler MM, Breland AB, Spindle TR, Maloney SF, Lipato T, Karaoghlanian N, Shihadeh AL, Lopez AA, Ramôa CP, Eissenberg T, 2017. Electronic cigarette user plasma nicotine concentration, puff topography, heart rate, and subjective effects: influence of liquid nicotine concentration and user experience. Exp. Clin. Psychopharmacol [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hughes JR, Hatsukami DK, Pickens RW, Krahn D, Malin S, Luknic A, 1984. Effect of nicotine on the tobacco withdrawal syndrome. Psychopharmacology (Berk) 83, 82–87. [DOI] [PubMed] [Google Scholar]
- Jamal A, Gentzke A, Hu SS, Cullen KA, Apelberg BJ, Homa DM, King BA, 2017. Tobacco Use Among Middle and High School Students - United States, 2011-2016. MMWR Morb. Mortal. Wkly. Rep 66, 597–603. 10.15585/mmwr.mm6623a1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jeong M, Zhang D, Morgan JC, Ross JC, Osman A, Boynton MH, Mendel JR, Brewer NT, 2019. Similarities and Differences in Tobacco Control Research Findings From Convenience and Probability Samples. Ann. Behav. Med 53, 476–485. 10.1093/abm/kay059 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kruskal JB, Wish M, 1978. Multidimensional scaling. Sage Publications, Beverly Hills, CA. [Google Scholar]
- McPherson S, Howell D, Lewis J, Barbosa-Leiker C, Bertotti Metoyer P, Roll J, 2016. Self-reported smoking effects and comparative value between cigarettes and high dose e-cigarettes in nicotine-dependent cigarette smokers. Behav. Pharmacol 27, 301 10.1097/FBP.0000000000000226 [DOI] [PubMed] [Google Scholar]
- Morean ME, Krishnan-Sarin S, Sussman S, Foulds J, Fishbein H, Grana R, Halpern-Felsher B, Kim H, Weaver SR, O’Malley SS, 2018. Development and psychometric validation of a novel measure of sensory expectancies associated with E-cigarette use Addict. Behav 10.1016/j.addbeh.2018.08.031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piper ME, Piasecki TM, Federman EB, Bolt DM, Smith SS, Fiore MC, Baker TB, 2004. A Multiple Motives Approach to Tobacco Dependence: The Wisconsin Inventory of Smoking Dependence Motives (WISDM-68). J. Consult. Clin. Psychol 72, 139–154. 10.1037/0022-006X.72.2.139 [DOI] [PubMed] [Google Scholar]
- Ramôa CP, Hiler MM, Spindle TR, Lopez AA, Karaoghlanian N, Lipato T, Breland AB, Shihadeh A, Eissenberg T, 2016. Electronic cigarette nicotine delivery can exceed that of combustible cigarettes: a preliminary report. Tob. Control 25, e6–9. 10.1136/tobaccocontrol-2015-052447 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rodu B, Plurphanswat N, 2018. E-cigarette use among US adults: Population Assessment of Tobacco and Health (PATH) Study. Nicotine Tob. Res 20, 940–948. [DOI] [PubMed] [Google Scholar]
- Rosas SR, Kane M, 2012. Quality and rigor of the concept mapping methodology: a pooled study analysis. Eval. Program Plann 35, 236–245. 10.1016/j.evalprogplan.2011.10.003 [DOI] [PubMed] [Google Scholar]
- Soule EK, Maloney SF, Guy MC, Eissenberg T, Fagan P, 2017a. User identified positive outcome expectancies of electronic cigarette use: A concept mapping study. Psychol. Addict. Behav. J. Soc. Psychol. Addict. Behav 31, 343–353. 10.1037/adb0000263 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Soule EK, Maloney SF, Guy MC, Eissenberg T, Fagan P, 2017b. User-identified electronic cigarette behavioral strategies and device characteristics for cigarette smoking reduction. Addict. Behav 79, 93–101. 10.1016/j.addbeh.2017.12.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Soule EK, Nasim A, Rosas S, 2016a. Adverse Effects of Electronic Cigarette Use: A Concept Mapping Approach. Nicotine Tob. Res 18, 678–685. 10.1093/ntr/ntv246 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Soule EK, Rosas SR, Nasim A, 2016b. Reasons for electronic cigarette use beyond cigarette smoking cessation: A concept mapping approach. Addict. Behav 56, 41–50. 10.1016/j.addbeh.2016.01.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trochim W, 1989. An introduction to concept mapping for planning and evaluation. Eval. Program Plann 12, 1–16. [Google Scholar]
- Vansickel AR, Weaver MF, Eissenberg T, 2012. Clinical laboratory assessment of the abuse liability of an electronic cigarette. Addict. Abingdon Engl 107, 1493–1500. 10.1111/j.1360-0443.2012.03791.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wagener TL, Floyd EL, Stepanov I, Driskill LM, Frank SG, Meier E, Leavens EL, Tackett AP, Molina N, Queimado L, 2017. Have combustible cigarettes met their match? The nicotine delivery profiles and harmful constituent exposures of second-generation and third-generation electronic cigarette users. Tob. Control 26, e23–e28. 10.1136/tobaccocontrol-2016-053041 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang TW, Asman K, Gentzke AS, Cullen KA, Holder-Hayes E, Reyes-Guzman C, Jamal A, Neff L, King BA, 2018. Tobacco Product Use Among Adults — United States, 2017. Morb. Mortal. Wkly. Rep 67, 1225–1232. 10.15585/mmwr.mm6744a2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ward JH, 1963. Hierarchical grouping to optimize an objective function. J. Am. Stat. Assoc 58, 236–244. [Google Scholar]
- Yingst JM, Lester C, Veldheer S, Allen SI, Du P, Foulds J, 2018. E-cigarette users commonly stealth vape in places where e-cigarette use is prohibited. Tob. Control, 10.1136/tobaccocontrol-2018-054432 [DOI] [PMC free article] [PubMed] [Google Scholar]