

Abstract
Pancreatic cancer is an aggressive, solid tumor, with a grave prognosis. Despite surgical treatment in patients with pancreatic cancer, the rate of recurrence is high. In addition, although tumor biomarkers are frequently used to confirm advanced pancreatic cancer, this is not accurate and the biomarkers currently used cannot indicate prognosis. This study sought to evaluate circulating tumor DNA as a tumor biomarker to prognosticate pancreatic cancer. Patients with advanced pancreatic cancer and liver metastasis (N = 104) were included, and blood samples were collected from all patients. The mutant allele frequency was measured using amplicon-based deep sequencing on a cell-free DNA panel covering 14 genes with > 240 hot spots. In patients with advanced pancreatic cancer, 50% (N = 52) had detectable ctDNA levels, with TP53 (45%, N = 47) and KRAS (42.3%, N = 44) mutations the most common. Patients with detectable circulating tumor DNA levels also had significantly worse overall survival and progression free survival than ctDNA negative patients (8.4 vs 16 months, P<0.0001 for overall survival; 3.2 vs 7.9 months, P<0.0001 for progression-free survival). In a multivariate analysis, ctDNA status was independently associated with overall survival and progression-free survival (HR = 3.1, 95%CI = 1.9–5.0, P<0.0001; HR 2.6, 95%CI = 1.7–4.0, P<0.0001, respectively). Moreover, circulating tumor DNA significantly correlated with a higher number of liver metastases, the presence of lung and/or peritoneal metastases, tumor burden, and higher carbohydrate antigen 19–9 levels. This study supports the use of circulating tumor DNA as an independent prognostic marker for advanced pancreatic cancer.
Introduction
Pancreatic cancer is one of the deadliest diseases, with a very poor prognosis. Patients with metastatic pancreatic cancer have a 5-year overall survival (OS) rate of only 2% [1], and fewer than 5% of patients with advanced pancreatic cancer who receive chemotherapy are expected to survive 5 years [2–5]. The prognosis remains poor despite improvements in treatment, particularly the introduction of new chemotherapies and surgical techniques, especially as cancer is usually detected in advanced stages. Patients with advanced pancreatic cancer must be monitored often to evaluate tumor burden and response to treatment. Serum protein biomarkers, such as carcinoembryonic antigen (CEA) and carbohydrate antigen 19–9 (CA19-9), are frequently measured, but these biomarkers do not accurately predict prognosis [6]. As such, a stringent yet minimally invasive biomarker that measures patient status with high sensitivity and specificity is urgently needed.
Recently, circulating tumor DNA (ctDNA), which is cell-free DNA (cfDNA) derived from a malignant tumor, has been suggested as a biomarker in various cancers. cfDNA increases during various physiological changes caused by factors including inflammation, smoking, and infection, but also increases in cancer patients [7, 8]. cfDNA is mainly caused by apoptosis and necrosis, and apoptosis is greatly increased in tumor masses due to the overgrowth of cancer cells and rapid cell turnover. Thus, cell debris normally phagocytosed by macrophages cannot be completely removed, and instead accumulates and is released into the blood circulation [9–11]. ctDNA has been recently confirmed as an early marker for treatment response and disease progression in patients with metastatic colorectal cancer and breast cancer [12, 13]. In pancreatic cancer, ctDNA is considered to be a useful biomarker for the risk of postoperative recurrence and for evaluating patient responses to chemotherapy [14, 15]. ctDNA levels may also be clinically useful for the detection of pancreatic cancer recurrence during postoperative follow-up [16–18]. Although several studies have investigated the utility of ctDNA as a biomarker in patients with pancreatic cancer [16, 19], its ability to predict prognosis is still unclear. Here, we sought to examine the utility of ctDNA as a biomarker in patients with advanced pancreatic cancer and liver metastasis.
Materials and methods
Patients
Blood samples were collected from 106 patients with advanced pancreatic cancer and liver metastasis who were undergoing follow-up at the Cancer Institute Hospital, Japanese Foundation for Cancer Research from February 2017 to August 2018. Two patients were excluded because of the presence of cancer in other organs, leaving a final cohort of 104 patients with advanced pancreatic cancer and liver metastasis. A power calculation was not conducted in this study because the study was designed with a relatively large sample size in previous reports. A specific course of treatment was not a requirement for enrollment in the study (Table 1). Computed tomography (CT) imaging was performed for all included patients to examine the degrees of pancreatic cancer progression, the number of liver metastases, and other metastases. The study was approved by the Institutional Review Board of the Japanese Foundation for Cancer Research (Tokyo, Japan), and written informed consent was obtained from all patients.
Table 1. Patient demographics and clinical characteristics.
| Characteristics | Total (N = 104) No. of patients (%) |
|---|---|
| Age at enrollment, y | |
| Median [range] | 64 [34–90] |
| Gender | |
| Male | 67 (64.4) |
| Female | 37 (35.6) |
| Treatment line at sampling | |
| None | 1 (0.96) |
| 1st line | 38 (36.5) |
| 2nd line | 37 (35.6) |
| 3rd line | 22 (21.2) |
| 4th line | 6 (5.8) |
| Chemotherapy regimen at sampling | |
| GnP | 61 (58.7) |
| mFFX | 34 (32.7) |
| S-1 | 3 (2.9) |
| GEM | 3 (2.9) |
| GE | 2 (1.9) |
| None | 1 (0.96) |
| Pancreatic location of tumor | |
| Head | 56 (53.8) |
| Body or tail | 48 (46.2) |
| Surgery at time of blood sample | |
| Yes | 23 (22.1) |
| No | 81 (77.9) |
| Metastatic site | |
| Liver | 104 (100) |
| Lymph node | 75 (72.1) |
| Lung | 19 (18.2) |
| Peritoneum | 11 (10.6) |
| Others | 7 (6.7) |
| Tumor marker | |
| CEA, ng/ml median [range] | 6.55 [1–610.8] |
| CA19-9, U/mL median [range] | 1280 [2–≥50000] |
CEA, carcinoembryonic antigen; CA19-9, carbohydrate antigen 19–9; GnP, a combination of gemcitabine and nab-paclitaxel; mFFX, FOLFIRINOX modified regimen; FOLFIRINOX, a combination of folinic acid and fluorouracil and irinotecan with oxaliplatin; S-1, a combination of tegafur, gimeracil and oteracil potassium; GEM, gemcitabine; GE, a combination of gemcitabine and erlotinib.
Blood sampling and ctDNA isolation
Blood was collected into EDTA tubes following the manufacturer’s instructions. To obtain plasma for analysis, blood samples were centrifuged for 10 min at 2,000×g at 4°C, then the supernatant was centrifuged a second time for 10 min at 16,000×g at 4°C to remove cellular debris. cfDNA was extracted from the plasma samples using the MagMax Cell-Free DNA Isolation Kit (Life Technologies; Thermo Fisher Scientific, Inc.) according to the manufacturer’s instructions. The cfDNA fraction was obtained from plasma samples using magnetic beads with three washing and rebinding cycles. cfDNA concentrations were determined using a Qubit dsDNA HS Assay kit (Life Technologies; Thermo Fisher Scientific, Inc.). cfDNA size distributions were analyzed using an Agilent 2100 Bioanalyzer (Agilent Technologies, Inc.).
Sequencing
An Oncomine Colon cfDNA Assay (Thermo Fisher Scientific) was used to generate libraries from the cfDNA, following the manufacturer’s instructions. The purity and concentration of the library were assessed using the Qubit dsDNA HS Assay kit and the Agilent 2100 Bioanalyzer, respectively. Unique index tags were added to each DNA fragment during library preparation. The Ion Chef System and the Ion 530 Kit-Chef were used for template preparation, followed by sequencing on the Ion S5 system using Ion 530 chips. A six-plex library pool was applied to the Ion 530 chip. We used a cfDNA panel covering 14 genes and 48 amplicons, including 240 hot spots (SNVs and short indels). The genes included in the panel were KRAS, TP53, APC, FBXW7, GNAS, MAP2K1, CTNNB1, ERBB2, PIK3CA, BRAF, EGFR, SMAD4, NRAS, and AKT1. Clean reads were mapped to the human reference genome (hg19). A variant caller was used to filter and call mutations in targeted regions of each gene [20, 21]. The limit of detection for each variant (mutant allele frequency [MAF]) was 0.15%. The average coverage ranged from 20,000x to 50,000x.
Statistical analysis
Chi-squared tests were used for comparisons of categorical variables (such as gender) and Mann–Whitney U tests were used for comparisons of continuous variables (such as age) between the ctDNA-positive and -negative groups. In addition, we analyzed the relationships between ctDNA and CT findings and relevant blood markers, including CA19-9 and CEA. The response rate was evaluated using the criteria set out in the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1. Survival was estimated using Kaplan–Meier curves [22, 23]. Correlations between clinical outcome and ctDNA markers were assessed using the log-rank test. Overall survival (OS) was calculated from the date of blood sampling to the date of death from any cause. Progression-free survival (PFS) was calculated from the date of blood sampling to the date of disease recurrence or progression, or death from any cause. The Cox hazard regression method was used to identify independent risk factors for OS and PFS. For all statistical analyses, two-tailed P values of 0.05 or less were considered statistically significant. All statistical analyses were performed using BellCurve for Excel version 3.10.
Results
Patient characteristics
Patient characteristics are presented in Table 1. The median age at the time of blood sampling was 64 years (range, 34–90 years), and 67 patients were male (64%). First, second, or third line chemotherapy was administered to 97 (93%) of the patients at the time of blood sampling. Only one patient did not receive chemotherapy either before or after blood sampling. Most (95/104; 91.4%) of the patients were treated with nab-paclitaxel added to gemcitabine (GnP) or a modified combination of three chemotherapeutic agents: fluorouracil, oxaliplatin, and irinotecan (mFFX). Surgery was performed before blood sampling for 21 patients and after blood sampling in two patients because of the disappearance of liver metastases following chemotherapy. Aside from the liver, the lymph node was the most frequent site of metastasis (72.1%), followed by the lung (18.2%) and peritoneum (10.6%). Median levels of CEA and CA19-9 at the time of sampling were 6.55 ng/ml and 1280 U/mL, respectively.
Somatic mutations and frequency
Of the 104 patients enrolled in this study, half (52/104; 50%) had somatic mutations in one or more of 13 of the 14 genes in the panel (TP53, KRAS, APC, FBXW7, GNAS, ERBB2, CTNNB1, MAP2K1, EGFR, SMAD4, PIK3CA, BRAF, and NRAS); only one gene (AKT1) had no instances of mutation in this cohort (S1 Table). The frequency of mutations is shown in Fig 1. Mutations in TP53 and KRAS were the most frequently detected (45% [47/104] and 42.3% [44/104] patients, respectively). KRAS p.G12D, p.G12V, p.12R, and other gene mutations were detected in 23, 15, 3, and 3 cases, respectively. APC and FBXW7 were also frequently mutated (13.5% [14/104] and 11.5% [12/104] patients, respectively). Mutations in GNAS (6.7%), ERBB2 (6.7%), CTNNB1 (5.8%), MAP2K1 (5.8%), EGFR (4.8%), SMAD4 (3.8%), BRAF (2.9%), NRAS (2.9%), and PIK3CA (1.9%) were less common (< 10% of patients).
Fig 1. Frequencies of mutated genes in plasma.

Distribution of somatic mutations in a panel of 14 genes in cfDNA from 104 pancreatic cancer patient plasma samples. One or more mutations were detected in all genes on the panel except AKT1.
Association between ctDNA and clinical factors
To estimate the clinical utility of ctDNA for patients with advanced pancreatic cancer, we sought to identify any associations between ctDNA and clinical factors. Because ctDNA was detected in 50% (52/104) of the cohort, we divided the patients into ctDNA-positive and -negative groups. With respect to age, gender, treatment at the time of sampling, primary site, with or without surgery, existence of lymph node metastasis, and CEA level, there were no significant differences between the two groups (Table 2). However, a higher number of liver metastases, the existence of lung and peritoneal metastases, a tumor diameter sum ≥ 100 mm, and a higher CA19-9 level were significantly associated with the detection of ctDNA (Table 2).
Table 2. Association of clinical factors with ctDNA in plasma.
| Clinical characteristics | ctDNA negative | ctDNA positive | P value |
|---|---|---|---|
| Age at enrollment, y | 0.59 | ||
| Median | 64 | 62 | |
| Gender | 0.41 | ||
| Male | 36 | 31 | |
| Female | 16 | 21 | |
| Treatment line at sampling | 0.61 | ||
| None | 0 | 1 | |
| 1st line | 20 | 18 | |
| 2nd line | 16 | 21 | |
| 3rd line | 11 | 11 | |
| 4th line | 5 | 1 | |
| Pancreatic location of tumor | 0.84 | ||
| Head | 27 | 29 | |
| Body or tail | 25 | 23 | |
| Surgery at time of blood sample | 0.34 | ||
| Yes | 14 | 9 | |
| No | 38 | 43 | |
| Number of liver metastasis | <0.001 | ||
| <10 | 37 | 19 | |
| ≥10 | 15 | 33 | |
| Lymph node metastasis | 0.12 | ||
| Positive | 30 | 45 | |
| Negative | 22 | 17 | |
| Lung metastasis | <0.001 | ||
| Positive | 5 | 14 | |
| Negative | 47 | 38 | |
| Peritoneal metastasis | <0.001 | ||
| Positive | 1 | 10 | |
| Negative | 48 | 45 | |
| Sum of the tumor diameter (mm) | <0.001 | ||
| <100 | 39 | 23 | |
| ≥100 | 13 | 29 | |
| Tumor marker | |||
| CEA median | 5.8 | 8.8 | 0.081 |
| CA19-9 median | 368 | 4193 | <0.001 |
ctDNA, circulating tumor DNA; CEA, carcinoembryonic antigen; CA19-9, carbohydrate antigen 19–9. RECIST ver 1.0 criteria.
ctDNA as a prognostic marker in advanced pancreatic cancer with liver metastasis
We performed Kaplan–Meier analyses to assess the prognostic value of ctDNA in the plasma of patients with advanced pancreatic cancer. Using the log-rank test, we found a significant association between the presence (vs absence) of ctDNA and both OS and PFS (8.4 vs 16 months for OS and 3.2 vs 7.9 months for PFS for positive and negative, respectively, both P < 0.0001; Fig 2). Moreover, we performed univariate and multivariate Cox proportional hazard regression analyses, summarized in Table 3. In the univariate analysis, presence of ctDNA was significantly associated with OS (HR = 2.7, 95%CI = 1.7–4.2 months, P < 0.0001) and PFS (HR = 2.5, 95%CI = 1.7–3.8, P < 0.0001). Similarly, in the multivariate analysis, ctDNA was the only independent factor for OS (HR = 3.1, 95%CI = 1.9–5.0 months, P < 0.0001) and PFS (HR = 2.6, 95%CI = 1.7–4.0 months, P < 0.0001).
Fig 2. Kaplan–Meier estimates of overall survival and progression-free survival in pancreatic cancer patients with respect to the presence or absence of ctDNA.
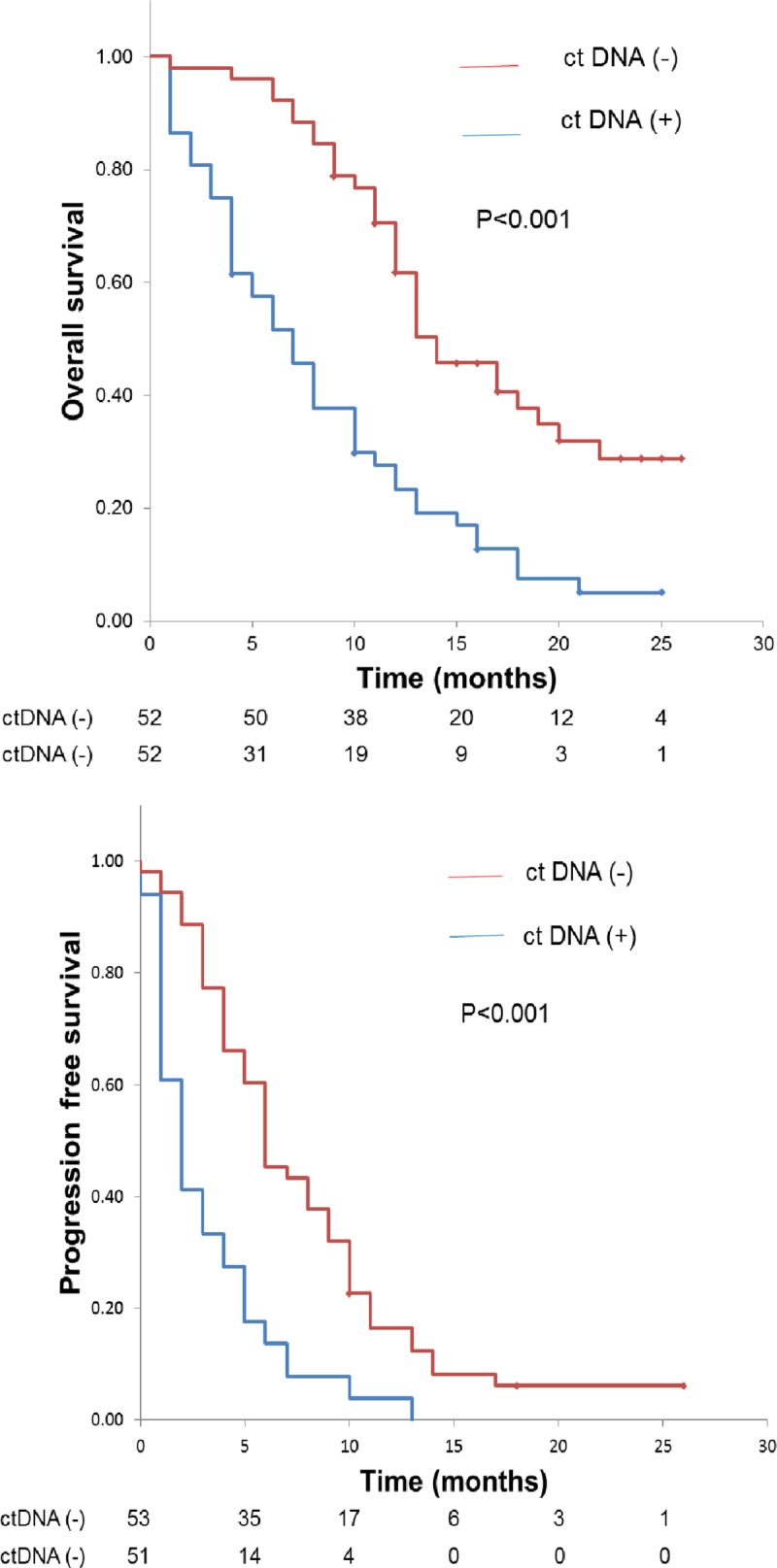
Comparison of overall survival (A) and progression-free survival (B) between ctDNA-positive and -negative groups. P values were calculated using the log-rank test.
Table 3. Cox proportional hazard analysis for overall survival and progression-free survival in pancreatic cancer patients with liver metastasis.
| Overall survival | Univariate analysis | Multivariate analysis | ||||||
| HR | Lower 95% CI | Upper 95% CI | P value | HR | Lower 95% CI | Upper 95% CI | P value | |
| Variables | ||||||||
| Age (<65 or ≥65) | 1.5 | 0.93 | 2.3 | 0.095 | 0.92 | 0.58 | 1.5 | 0.71 |
| Gender | 1.5 | 0.96 | 2.5 | 0.072 | 1.4 | 0.88 | 2.3 | 0.16 |
| ctDNA (negative or positive) | 2.7 | 1.7 | 4.2 | <0.001 | 3.1 | 1.9 | 5.0 | <0.001 |
| CEA (<5 ng/ml or ≥5 ng/ml) | 1.3 | 0.85 | 2.1 | 0.21 | 1.0 | 0.63 | 1.6 | 0.98 |
| CA19-9 (<37 U/mL or ≥37 U/mL | 1.3 | 0.75 | 2.2 | 0.37 | 1.2 | 0.70 | 2.0 | 0.61 |
| Progression-free survival | Univariate analysis | Multivariate analysis | ||||||
| HR | Lower 95% CI | Upper 95% CI | P value | HR | Lower 95% CI | Upper 95% CI | P value | |
| Variables | ||||||||
| Age (<65 or ≥65) | 1.2 | 0.77 | 1.7 | 0.49 | 1.2 | 0.79 | 1.8 | 0.40 |
| Gender | 1.2 | 0.78 | 1.8 | 0.43 | 1.2 | 0.79 | 1.8 | 0.93 |
| ctDNA (negative or positive) | 2.5 | 1.7 | 3.8 | <0.001 | 2.6 | 1.7 | 4.0 | <0.001 |
| CEA (<5 ng/ml or ≥5 ng/ml) | 1.2 | 0.78 | 1.8 | 0.44 | 1.1 | 0.74 | 1.7 | 0.59 |
| CA19-9 (<37 U/mL or ≥37 U/mL | 1.2 | 0.72 | 1.9 | 0.53 | 0.90 | 0.55 | 1.5 | 0.69 |
ctDNA, circulating tumor DNA; CEA, carcinoembryonic antigen; Ca19-9, carbohydrate antigen 19–9.
Association between ctDNA level and therapy response
Finally, we analyzed the association between therapy response after blood sampling and the presence or absence of ctDNA. The objective response rate (ORR) and disease control rate (DCR) were 9.6% (10/104) and 22.1% (23/104) (10 partial response [PR] and 23 stable disease [SD]), respectively. Patients with PR/SD after blood sampling showed better ORR than those with progressive disease ([PD], P = 0.001; Table 4).
Table 4. The association between ctDNA and objective response in patients with pancreatic cancer.
| PD | SD/PR | P value | |
|---|---|---|---|
| ctDNA positive | 41 | 7 | 0.001 |
| ctDNA negative | 30 | 26 |
ctDNA: circulating tumor DNA. PD: progressive disease. SD: stable disease. PR: partial response.
Discussion
Performing a comprehensive molecular analysis of tissue biopsy samples is generally one of the first steps in obtaining a diagnosis for cancer. However, the clinical utility of such an analysis is often diminished in patients with pancreatic cancer due to the difficulty in obtaining tissue samples of adequate quality [24]. Furthermore, taking biopsies can lead to clinical complications, which surgeons usually try to avoid if possible. As such, there has been considerable focus on the design and implementation of highly accurate and minimally invasive blood tests for cancer screening. Although several serological biomarkers, such as CEA and CA 19–9, are used in the clinic, they tend not to be sensitive or specific enough for prognostication in patients with pancreatic cancer [25]. More recent studies have shown that ctDNA—which can be obtained through liquid biopsies and is detectable by next-generation sequencing or ddPCR with high sensitivity—is released from the primary tumor and/or its metastases [26–29] and therefore could be used to detect cancer and/or its recurrence at very early stages. However, while several studies have described the clinical utility of ctDNA for patients with pancreatic cancer, few have used sufficiently large sample sizes for their analyses. In this study, we investigated the clinical utility of ctDNA as a biomarker for the prognostication of patients with advanced pancreatic cancer and liver metastasis.
Of the 104 patients enrolled in the present study, half had one or more detectable mutant allele(s) (MAF ≥ 0.15%) among 13 of 14 genes. This result is consistent with findings reported by Pietrasz and colleagues [30] and Kinugasa and colleagues [31]. However, Bettegowda and colleagues reported a much higher detection rate of ctDNA in patients with advanced pancreatic cancer [32]. These discordant results might be partially due to the differences in the number of genes included in the panel or the limit of detection, as follows. The molecular genetic landscape of pancreatic cancer has been studied by whole-genome and exome sequencing, and KRAS, CDKN2A, TP53, and SMAD4 are frequently reported as mutated in pancreatic cancer [33–37]. In the current study, although TP53 and KRAS mutations were detected in 90.4% and 84.6% of ctDNA-positive patients, respectively, few patients showed SMAD4 mutations (3.8% of whole cohort, N = 4). These inconsistencies might be due to an insufficient coverage of mutations within the SMAD4 gene in the panel; further technical improvement of the gene panel, which covers sufficient hot spot mutations of the SMAD4 gene, would increase the detection accuracy in patients with pancreatic cancer. Another disadvantage of the cfDNA panel used in this study was that it did not contain CDKN2A, a common mutant gene in pancreatic cancer. Therefore, this study may have underestimated the number of ctDNA-positive samples. In the future, it would be better to measure ctDNA using a custom gene panel specific to pancreatic cancer. It was not possible to compare ctDNA with mutant DNA from tumor tissue in this study, as there were no sequence data on tumor tissue. Since ctDNA represents real-time tumor heterogeneity, it would be very useful in future to perform ctDNA analysis at the same time as mutant DNA analysis from biopsy tissues or surgical specimens.
We found a significant association of ctDNA with the number of liver, lung and peritoneal metastases, as well as with the sum of the tumor diameter, and the level of CA19-9, as previously reported [32, 38]. These factors may reflect the tumor burden better than other clinical factors. Since ctDNA has a short half-life, it can indicate the patient’s status including distant metastasis and tumor burden, in real time. Therefore, in the future, it may be possible to recommend a less invasive ctDNA test rather than an expensive CT test that increases risk of exposure, as has also been suggested by others [39, 40]. Lymph node metastasis was not significantly associated with the detection of ctDNA, suggesting that tumor burden in the lymph nodes might be relatively small compared with metastases in other organs. Clinical evidence suggests that metastasis to nearby lymph nodes occurs earlier in patients with pancreatic cancer than in those with other types of cancer, including liver, lung, and peritoneum. It is therefore not surprising that in the present study, almost all cases with liver metastasis also showed evidence of lymph node metastasis, and might explain why lymph node metastasis itself was not significantly associated with the presence of ctDNA.
We further showed that ctDNA was a prognostic marker of OS and PFS (OS: 8.4 vs 16 months with and without ctDNA, respectively; PFS: 3.2 vs 7.9 months with and without ctDNA, respectively; Fig 2; P < 0.0001). Our results agree with those of Pietrasz and colleagues, who previously reported the prognostic value of ctDNA as a biomarker in advanced pancreatic cancer [30]. In their study, the presence of ctDNA in the plasma correlated with poor PFS (9.9 months vs. median not reached; log-rank P = 0.02). Chen and colleagues also described an association between KRAS mutations detectable in the plasma and poor OS (3.9 vs. 10.2 months; P < 0.0001) [19]. Moreover, a meta-analysis of the association between cfDNA and the prognosis of pancreatic cancer patients concluded that certain mutations (KRAS, ERBB2-exon17, and KRASG12V), ctDNA presence, hypermethylation and higher concentration of cfDNA were associated with worse survival in patients with pancreatic cancer [10]. Reviews of the association between ctDNA and the prognosis of patients with pancreatic cancer suggest that high ctDNA levels have a poor prognosis, and that ctDNA is a more sensitive prognostic predictor than other tumor markers including CA19-9 [41, 42]. In our multivariate analysis, ctDNA was an independent predictor of OS (HR, 3.1; 95%CI, 1.9–5.0; P < 0.0001) and PFS (HR, 2.6, 95%CI, 1.7–4.0, P < 0.0001), further supporting the use of ctDNA as a reliable predictive biomarker in advanced pancreatic cancer. We also found a significant association between ctDNA and therapy response, which suggests that ctDNA could act as a biomarker to predict response to chemotherapy in patients with advanced pancreatic cancer. Periodic ctDNA analysis after the start of treatment may help determine whether to change treatment.
There were several limitations in our study. First, our study design was retrospective, and blood was collected at a single time-point which varied between patients. These variables might make it difficult to accurately analyze the association between ctDNA and various prognostic factors. In the future, a prospective follow-up and sequential blood sampling might be required to prove the utility of ctDNA as a biomarker. Second, of the genes which have a high mutation frequency in pancreatic cancer, KRAS, TP53, SMAD4, and CDKN2A, the frequency of mutations in SMAD4 were low and CDKN2A was not measured in this study. This may have led to underestimation of the number of ctDNA positives. In the future, a custom gene panel specific for pancreatic cancer should be used to accurately perform ctDNA measurement and further to compare mutated genes in paired tumor tissue and plasma samples.
In conclusion, we found that detection of plasma ctDNA can be used for prognostication in patients with advanced pancreatic cancer with liver metastasis. Future prospective studies could be undertaken to validate the clinical impact of ctDNA among this cohort and to confirm its clinical utility as a biomarker.
Supporting information
Gene mutations in 14 genes from samples retrieved from 104 patients with advanced pancreatic cancer. White, no mutation detected; Gray, Mutant Allele Frequency < 0.15%; Yellow, 0.15% ≤ Mutant Allele Frequency < 1%; Blue, 1% ≤ Mutant Allele Frequency < 10%; Red, 10% ≤ Mutant Allele Frequency.
(XLSX)
Acknowledgments
We express our heartfelt gratitude to all study participants. We thank Ms. Aya Imai, Mr. Yuki Sano, and Ms. Marie Muramatsu for technical assistance. We thank all other members and staff for their contributions to sample collection and the completion of our study.
Data Availability
All relevant data are within the manuscript and its Supporting Information files.
Funding Statement
The author(s) received no specific funding for this work.
References
- 1.Conroy T, Bachet JB, Ayav A, Huguet F, Lambert A, Caramella C, et al. Current standards and new innovative approaches for treatment of pancreatic cancer. Eur J Cancer. 2016;57:10–22. 10.1016/j.ejca.2015.12.026 [DOI] [PubMed] [Google Scholar]
- 2.Shi S, Yao W, Xu J, Long J, Liu C, Yu X. Combinational therapy: new hope for pancreatic cancer? Cancer Lett. 2012;317(2):127–35. 10.1016/j.canlet.2011.11.029 [DOI] [PubMed] [Google Scholar]
- 3.Neoptolemos JP, Kleeff J, Michl P, Costello E, Greenhalf W, Palmer DH. Therapeutic developments in pancreatic cancer: current and future perspectives. Nat Rev Gastroenterol Hepatol. 2018;15(6):333–48. 10.1038/s41575-018-0005-x [DOI] [PubMed] [Google Scholar]
- 4.Vivaldi C, Fornaro L, Vasile E. FOLFIRINOX Adjuvant Therapy for Pancreatic Cancer. N Engl J Med. 2019;380(12):1187–8. 10.1056/NEJMc1900712 [DOI] [PubMed] [Google Scholar]
- 5.Buscail L. Commentary: Pancreatic cancer: is the worst to come? Int J Epidemiol. 2017;46(6):1774–5. 10.1093/ije/dyx143 [DOI] [PubMed] [Google Scholar]
- 6.Zhang Y, Yang J, Li H, Wu Y, Zhang H, Chen W. Tumor markers CA19-9, CA242 and CEA in the diagnosis of pancreatic cancer: a meta-analysis. Int J Clin Exp Med. 2015;8(7):11683–91. [PMC free article] [PubMed] [Google Scholar]
- 7.Jahr S, Hentze H, Englisch S, Hardt D, Fackelmayer FO, Hesch RD, et al. DNA fragments in the blood plasma of cancer patients: quantitations and evidence for their origin from apoptotic and necrotic cells. Cancer Res. 2001;61(4):1659–65. [PubMed] [Google Scholar]
- 8.Schwarzenbach H, Hoon DS, Pantel K. Cell-free nucleic acids as biomarkers in cancer patients. Nat Rev Cancer. 2011;11(6):426–37. 10.1038/nrc3066 [DOI] [PubMed] [Google Scholar]
- 9.Takai E, Yachida S. Circulating tumor DNA as a liquid biopsy target for detection of pancreatic cancer. World J Gastroenterol. 2016;22(38):8480–8. 10.3748/wjg.v22.i38.8480 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Chen L, Zhang Y, Cheng Y, Zhang D, Zhu S, Ma X. Prognostic value of circulating cell-free DNA in patients with pancreatic cancer: A systemic review and meta-analysis. Gene. 2018;679:328–34. 10.1016/j.gene.2018.09.029 [DOI] [PubMed] [Google Scholar]
- 11.Leon SA, Shapiro B, Sklaroff DM, Yaros MJ. Free DNA in the serum of cancer patients and the effect of therapy. Cancer Res. 1977;37(3):646–50. [PubMed] [Google Scholar]
- 12.Tie J, Kinde I, Wang Y, Wong HL, Roebert J, Christie M, et al. Circulating tumor DNA as an early marker of therapeutic response in patients with metastatic colorectal cancer. Ann Oncol. 2015;26(8):1715–22. 10.1093/annonc/mdv177 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Dawson SJ, Tsui DW, Murtaza M, Biggs H, Rueda OM, Chin SF, et al. Analysis of circulating tumor DNA to monitor metastatic breast cancer. N Engl J Med. 2013;368(13):1199–209. 10.1056/NEJMoa1213261 [DOI] [PubMed] [Google Scholar]
- 14.Lee B, Lipton L, Cohen J, Tie J, Javed AA, Li L, et al. Circulating tumor DNA as a potential marker of adjuvant chemotherapy benefit following surgery for localized pancreatic cancer. Ann Oncol. 2019;30(9):1472–8. 10.1093/annonc/mdz200 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Perets R, Greenberg O, Shentzer T, Semenisty V, Epelbaum R, Bick T, et al. Mutant KRAS Circulating Tumor DNA Is an Accurate Tool for Pancreatic Cancer Monitoring. Oncologist. 2018;23(5):566–72. 10.1634/theoncologist.2017-0467 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sausen M, Phallen J, Adleff V, Jones S, Leary RJ, Barrett MT, et al. Clinical implications of genomic alterations in the tumour and circulation of pancreatic cancer patients. Nat Commun. 2015;6:7686 10.1038/ncomms8686 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Abbosh C, Birkbak NJ, Wilson GA, Jamal-Hanjani M, Constantin T, Salari R, et al. Phylogenetic ctDNA analysis depicts early-stage lung cancer evolution. Nature. 2017;545(7655):446–51. 10.1038/nature22364 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Tie J, Cohen JD, Wang Y, Li L, Christie M, Simons K, et al. Serial circulating tumour DNA analysis during multimodality treatment of locally advanced rectal cancer: a prospective biomarker study. Gut. 2019;68(4):663–71. 10.1136/gutjnl-2017-315852 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Chen H, Tu H, Meng ZQ, Chen Z, Wang P, Liu LM. K-ras mutational status predicts poor prognosis in unresectable pancreatic cancer. Eur J Surg Oncol. 2010;36(7):657–62. 10.1016/j.ejso.2010.05.014 [DOI] [PubMed] [Google Scholar]
- 20.Shin S, Kim Y, Chul Oh S, Yu N, Lee ST, Rak Choi J, et al. Validation and optimization of the Ion Torrent S5 XL sequencer and Oncomine workflow for BRCA1 and BRCA2 genetic testing. Oncotarget. 2017;8(21):34858–66. 10.18632/oncotarget.16799 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Xu C. A review of somatic single nucleotide variant calling algorithms for next-generation sequencing data. Comput Struct Biotechnol J. 2018;16:15–24. 10.1016/j.csbj.2018.01.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kaplan EL, Meier P. Nonparametric estimation from incompleteobservations. J Am Stat Assoc. 1958;53:457–81. [Google Scholar]
- 23.Bonnetain F, Bonsing B, Conroy T, Dousseau A, Glimelius B, Haustermans K, et al. Guidelines for time-to-event end-point definitions in trials for pancreatic cancer. Results of the DATECAN initiative (Definition for the Assessment of Time-to-event End-points in CANcer trials). Eur J Cancer. 2014;50(17):2983–93. 10.1016/j.ejca.2014.07.011 [DOI] [PubMed] [Google Scholar]
- 24.Zill OA, Greene C, Sebisanovic D, Siew LM, Leng J, Vu M, et al. Cell-Free DNA Next-Generation Sequencing in Pancreatobiliary Carcinomas. Cancer Discov. 2015;5(10):1040–8. 10.1158/2159-8290.CD-15-0274 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Poruk KE, Gay DZ, Brown K, Mulvihill JD, Boucher KM, Scaife CL, et al. The clinical utility of CA 19–9 in pancreatic adenocarcinoma: diagnostic and prognostic updates. Curr Mol Med. 2013;13(3):340–51. 10.2174/1566524011313030003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Imamura T, Komatsu S, Ichikawa D, Kawaguchi T, Miyamae M, Okajima W, et al. Liquid biopsy in patients with pancreatic cancer: Circulating tumor cells and cell-free nucleic acids. World J Gastroenterol. 2016;22(25):5627–41. 10.3748/wjg.v22.i25.5627 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Zhang R, Peng R, Li Z, Gao P, Jia S, Yang X, et al. Synthetic Circulating Cell-free DNA as Quality Control Materials for Somatic Mutation Detection in Liquid Biopsy for Cancer. Clin Chem. 2017;63(9):1465–75. 10.1373/clinchem.2017.272559 [DOI] [PubMed] [Google Scholar]
- 28.Pantel K, Alix-Panabieres C. Liquid biopsy and minimal residual disease—latest advances and implications for cure. Nat Rev Clin Oncol. 2019;16(7):409–24. 10.1038/s41571-019-0187-3 [DOI] [PubMed] [Google Scholar]
- 29.Alix-Panabieres C, Pantel K. Circulating tumor cells: liquid biopsy of cancer. Clin Chem. 2013;59(1):110–8. 10.1373/clinchem.2012.194258 [DOI] [PubMed] [Google Scholar]
- 30.Pietrasz D, Pecuchet N, Garlan F, Didelot A, Dubreuil O, Doat S, et al. Plasma Circulating Tumor DNA in Pancreatic Cancer Patients Is a Prognostic Marker. Clin Cancer Res. 2017;23(1):116–23. 10.1158/1078-0432.CCR-16-0806 [DOI] [PubMed] [Google Scholar]
- 31.Kinugasa H, Nouso K, Miyahara K, Morimoto Y, Dohi C, Tsutsumi K, et al. Detection of K-ras gene mutation by liquid biopsy in patients with pancreatic cancer. Cancer. 2015;121(13):2271–80. 10.1002/cncr.29364 [DOI] [PubMed] [Google Scholar]
- 32.Bettegowda C, Sausen M, Leary RJ, Kinde I, Wang Y, Agrawal N, et al. Detection of circulating tumor DNA in early- and late-stage human malignancies. Sci Transl Med. 2014;6(224):224ra24 10.1126/scitranslmed.3007094 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Patel H, Okamura R, Fanta P, Patel C, Lanman RB, Raymond VM, et al. Clinical correlates of blood-derived circulating tumor DNA in pancreatic cancer. J Hematol Oncol. 2019;12(1):130 10.1186/s13045-019-0824-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kleeff J, Korc M, Apte M, La Vecchia C, Johnson CD, Biankin AV, et al. Pancreatic cancer. Nat Rev Dis Primers. 2016;2:16022 10.1038/nrdp.2016.22 [DOI] [PubMed] [Google Scholar]
- 35.Biankin AV, Waddell N, Kassahn KS, Gingras MC, Muthuswamy LB, Johns AL, et al. Pancreatic cancer genomes reveal aberrations in axon guidance pathway genes. Nature. 2012;491(7424):399–405. 10.1038/nature11547 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Waddell N, Pajic M, Patch AM, Chang DK, Kassahn KS, Bailey P, et al. Whole genomes redefine the mutational landscape of pancreatic cancer. Nature. 2015;518(7540):495–501. 10.1038/nature14169 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Bailey P, Chang DK, Nones K, Johns AL, Patch AM, Gingras MC, et al. Genomic analyses identify molecular subtypes of pancreatic cancer. Nature. 2016;531(7592):47–52. 10.1038/nature16965 [DOI] [PubMed] [Google Scholar]
- 38.Takai E, Totoki Y, Nakamura H, Morizane C, Nara S, Hama N, et al. Clinical utility of circulating tumor DNA for molecular assessment in pancreatic cancer. Sci Rep. 2015;5:18425 10.1038/srep18425 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Chen I, Raymond VM, Geis JA, Collisson EA, Jensen BV, Hermann KL, et al. Ultrasensitive plasma ctDNA KRAS assay for detection, prognosis, and assessment of therapeutic response in patients with unresectable pancreatic ductal adenocarcinoma. Oncotarget. 2017;8(58):97769–86. 10.18632/oncotarget.22080 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Tjensvoll K, Lapin M, Buhl T, Oltedal S, Steen-Ottosen Berry K, Gilje B, et al. Clinical relevance of circulating KRAS mutated DNA in plasma from patients with advanced pancreatic cancer. Mol Oncol. 2016;10(4):635–43. 10.1016/j.molonc.2015.11.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Rofi E, Vivaldi C, Del Re M, Arrigoni E, Crucitta S, Funel N, et al. The emerging role of liquid biopsy in diagnosis, prognosis and treatment monitoring of pancreatic cancer. Pharmacogenomics. 2019;20(1):49–68. 10.2217/pgs-2018-0149 [DOI] [PubMed] [Google Scholar]
- 42.Samandari M, Julia MG, Rice A, Chronopoulos A, Del Rio Hernandez AE. Liquid biopsies for management of pancreatic cancer. Transl Res. 2018;201:98–127. 10.1016/j.trsl.2018.07.008 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Gene mutations in 14 genes from samples retrieved from 104 patients with advanced pancreatic cancer. White, no mutation detected; Gray, Mutant Allele Frequency < 0.15%; Yellow, 0.15% ≤ Mutant Allele Frequency < 1%; Blue, 1% ≤ Mutant Allele Frequency < 10%; Red, 10% ≤ Mutant Allele Frequency.
(XLSX)
Data Availability Statement
All relevant data are within the manuscript and its Supporting Information files.