

In December 2019, a new coronavirus called SARS-CoV-2 emerged from a zoonotic source in Wuhan, China. One of its main characteristics is its easy propagation through airborne droplets from symptomatic and asymptomatic patients. SARS-CoV-2 thus has spread quickly, infecting 2 million people in more than 200 countries. It is the first coronavirus to be considered a pandemic. Its mortality rate ranges from 1% to 10%.1,2 Unfortunately, health workers have a 3 times greater chance of acquiring the virus compared with the general population, with almost 20% infected in some regions.3
Because of the method of transmission, endoscopy rooms and digestive endoscopy procedures in general represent an easy method of dissemination. Because these procedures are performed in a contaminated environment, there is a higher risk that patients and health workers will be infected. This concern exists because procedures that take place in the upper GI tract, including gastroduodenoscopy, cholangiography, and EUS, make it easier for particles to become aerosols that exit the infected patient’s nasopharynx.4 This risk can increase even more if a patient sneezes, coughs, retches, or needs to be intubated. Although there is an absence of new data about transmission of the virus as an aerosol, a previous study revealed that health workers who are exposed to this kind of procedure have a 4.66 times greater probability (95% confidence interval, 3.1-6.9) of infection in comparison with others.5
In addition, there is evidence of microbe dissemination to a distance of as much as 2 m from a patient during endoscopy.6 Fluids from the patient can be scattered when manipulation devices are used within the endoscope, possibly infecting people nearby and even contaminating light switches and doors7,8; this contamination is made more alarming by the fact that the virus has been found to be viable for several hours on plastics and stainless steel.9
Taking all this into account, endoscopy can be considered a high-risk procedure for COVID-19 transmission. Guidelines recommend the use of personal protection equipment for every procedure, including long-sleeved robes, eye protection, gloves, and a mask.10 It should also be taken into account that the high number of current COVID-19 cases will take time to decrease and that the eventual relaxing of mitigation measures could bring the revival of this disease. Thus, the more protection elements that can be worn, the lower the risk.
Our current interest in the Colombia University endoscopic unit is to decrease as much as possible aerosol contamination from patients and health workers. This is why we designed a special face shield made from acrylic. This shield differs from existing shields; our new shield has a small opening (12 mm) where the mouth of the patient would be. The orifice has a simple open-and-close system (Figure 1, Figure 2, Figure 3). Acrylic is an inexpensive material. The production of 1 unit costs approximately US.$5. When produced on a mass scale, it will be less expensive.
Figure 1.
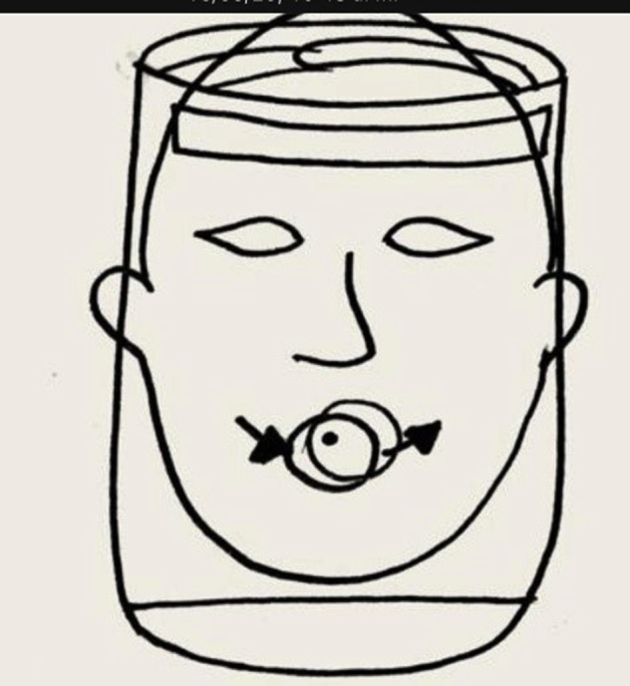
Face shield, front view.
Figure 2.
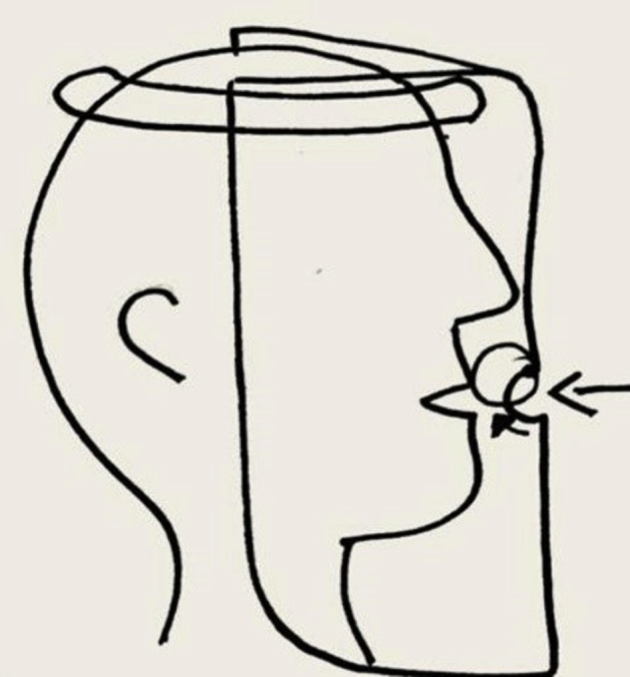
Face shield, side view.
Figure 3.
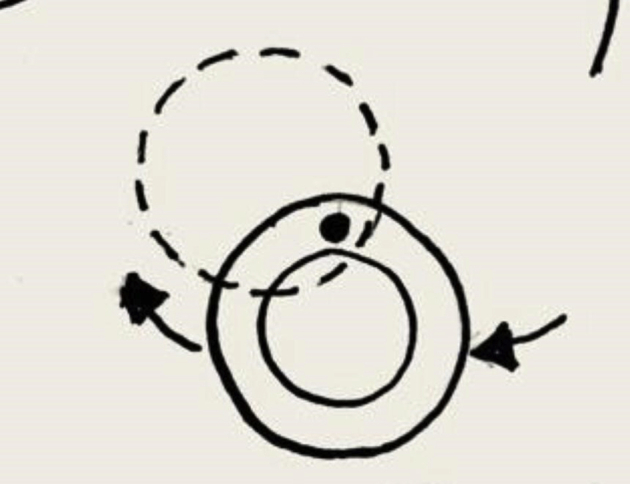
Orifice function system.
We are well aware of the waste this face shield may represent if used only once per patient. This is not intended to be a disposable product. The idea is that it could be used more than once in different patients after the right sterilization process. The material it is made from allows it to be cleaned with conventional antiseptics to disinfect the endoscopic equipment.
The patient arrives to our unit wearing a mask. The face shield should be worn at all times while the patient is waiting (Figure 4, Figure 5, Figure 6). The patient is then called to the room where the endoscopy will be performed. The orifice is opened to introduce the endoscope. The endoscopy is done as usual; once the procedure is finished, we close the orifice again. The patient continues wearing the mask shield, even after recovering from sedation and while exiting the unit. Thus, there is continuous protection before, during, and after the endoscopic procedure.
Figure 4.

Patient before endoscopy.
Figure 5.

Endoscopy.
Figure 6.

After endoscopy: fluids and aerosols retained in face shield.
While testing the equipment in real life, we encountered a considerable presence of fluid and droplets beneath the mask once the procedure was done (Fig. 6). If the patient were not wearing the mask, these would have contaminated the patient’s surroundings.
In conclusion, we have found that wearing the face shield we have specially designed results in less contact between the patient and the environment and yields an important decrease in the quantity of droplets and aerosols produced during the procedure.
This face shield is currently being tested to evaluate its effectiveness and utility (Video 1, available online at www.VideoGIE.org).
Disclosure
All authors disclosed no financial relationships.
Supplementary data
Video use of face shield.
References
- 1.World Health Organization . WHO; Geneva, Switzerland: 2020. Coronavirus disease (COVID-2019) Situation Report 84. [Google Scholar]
- 2.World Health Organization . WHO; Geneva, Switzerland: 2020. Coronavirus disease (COVID-2019) Situation Report 51. [Google Scholar]
- 3.Remuzzi A., Remuzzi G. COVID-19 and Italy: what next? Lancet. 2020;395:P1125–P1128. doi: 10.1016/S0140-6736(20)30627-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Zou L., Ruan F., Huang M. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N Engl J Med. 2020;382:1177–1179. doi: 10.1056/NEJMc2001737. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Tran K., Cimon K., Severn M. Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: a systematic review. PloS One. 2012;7 doi: 10.1371/journal.pone.0035797. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Johnston E.R., Habib-Bein N., Dueker J.M. Risk of bacterial exposure to the endoscopist’s face during endoscopy. Gastrointest Endosc. 2019;89:818–824. doi: 10.1016/j.gie.2018.10.034. [DOI] [PubMed] [Google Scholar]
- 7.Zou L., Ruan F., Huang M. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N Engl J Med. 2020;382:1177–1179. doi: 10.1056/NEJMc2001737. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ong S.W.X., Tan Y.K., Chia P.Y. Air, surface environmental, and personal protective equipment contamination by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from a symptomatic patient. JAMA. 2020;373:1610–1612. doi: 10.1001/jama.2020.3227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.van Doremalen N., Bushmaker T., Morris D.H. Aerosol and surface stability of SARS-CoV2 as compared with SARS-CoV-1. N Engl J Med. 2020;382:1564–1567. doi: 10.1056/NEJMc2004973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Sultan S, Lim JK, Altayar O, et al. AGA Institute rapid recommendations for gastrointestinal procedures during the COVID-19 pandemic. Gastroenterology. Epub 2020 April 1. [DOI] [PMC free article] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Video use of face shield.