

Abstract
Bilirubin, a product of heme metabolism, is the most potent endogenous antioxidant which increases in many oxidative stress conditions such as stroke. It has been widely known to exert neuroprotective effect on stroke through mechanisms involved in development, therefore, it can influence the occurrence and prognosis of ischaemic stroke (IS). In this review, studies were identified by a comprehensive search of Pubmed, Embase, the Cochrane Library (Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials (CENTRAL), Cochrane Methodology Register) and Web of Science to examine the correlation between serum bilirubin levels and risks of developing IS as well as IS outcomes. Additional studies were identified by reviewing references and contacting authors.
Keywords: stroke
Introduction
Stroke is the second-leading cause of mortality and the leading cause of long-term disability worldwide.1 Once ischaemia occurs, excessive oxidative stress ensues and leads to structural and functional damage to the brain, which plays an important role in the pathogenesis of ischaemic brain damage, especially throughout the acute phase of ischaemic stroke (IS).2–4 Compared with other organs, human brain has few sources of endogenous antioxidants,5 which poses it more vulnerable to oxidative injury. Recently, a number of therapeutics with antioxidants have shown encouraging results in acute ischaemic stroke (AIS).6 Bilirubin, a compound used to diagnose conditions such as hepatobiliary disorders,7 haemolytic anaemia8 and dyserythropoiesis,9 also known as a potential toxic factor causing severe brain damage in newborns,10 is not only the end product of the heme catabolic pathway but also the most potent endogenous antioxidant.11 It has been shown to protect from diverse diseases associated with increased oxidative stress, such as IS.12 In addition, accumulating evidence has shown that bilirubin harbours anti-inflammatory,11 neuroprotective13 and platelet activation inhibiting14 effects. In this review, we have summarised available evidence regarding the correlation between circulating bilirubin levels and risks of IS as well as the prognosis of AIS in order to verify the usefulness of bilirubin serving as a biomarker for stroke occurrence and prognosis.
Search strategy and selection criteria
References for this review were identified in databases of PubMed, Embase, the Cochrane Library (Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials (CENTRAL), Cochrane Methodology Register) and Web of Science up to August 2019, and from reference lists of relevant articles. Combinations of searching terms were “stroke” or “cerebr* vascular disease”, or “cerebr* ischaemia”, or “intracerebr* haemorrhage”, or “cerebr* haemorrhage”, or “brain isch*”, or “brain haemorrhage” and “bilirubin”, or “bilirubin*” and “outcome*”, or “prognos*”, or “predict*”, or “mortality”, or “death”, or “dependenc*”, or “disability”, or “neurological deterioration”, or “functional depend*”. Language was limited to English. Titles and abstracts were examined for their relevance to the present review, and basic science articles were included if their methods were considered to be of high quality. Articles were excluded if their full texts were unavailable. Relevant prior and ongoing clinical trials investigating the relationship between levels of serum bilirubin and IS outcomes were also included. Results of the study-selection process were shown in figure 1.
Figure 1.
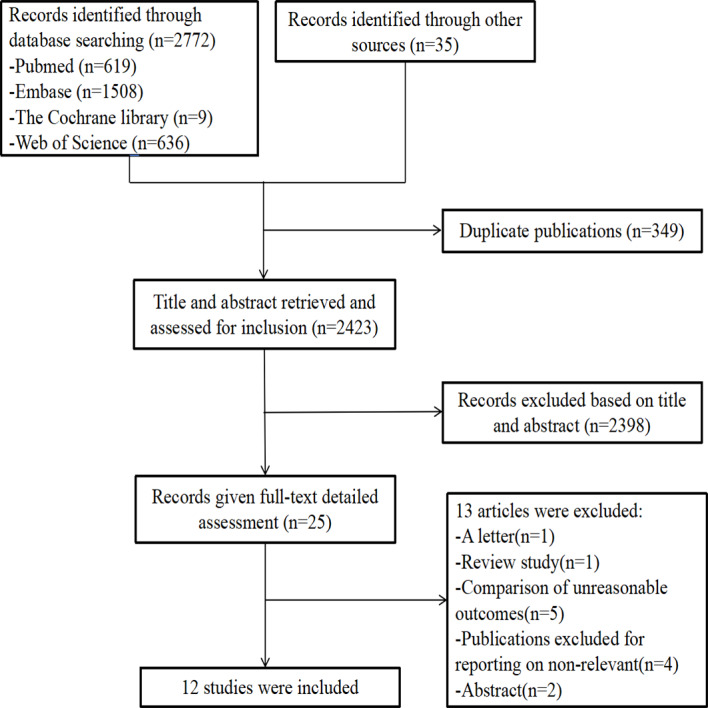
Flow chart of studies included.
Proposed possible mechanisms of neuroprotection
Blockage of cerebral vessels, either temporarily or permanently, triggers a complex series of neurochemical processes including neuronal excitotoxicity, oxidative stress, production of free radicals, blood-brain barrier dysfunction, lipid peroxidation and finally cell death of neurons, glial and endothelial cells.15 Oxidative stress in the acute phase of IS augments brain injury when the production of free radicals exceeds the endogenous scavenging capacity of the intracellular antioxidation defense system.
Bilirubin, the most potent endogenous antioxidant, is rapidly increased in conditions of oxidative stress,16 such as brain ischaemia. Studies have confirmed that the body can produce a large amount of bilirubin on the stimulation of tissue hypoxia, free radicals and proinflammatory cytokines. Interestingly, reduction of antioxidants, such as glutathione, in vivo can also increase the production of bilirubin.17 Increased bilirubin levels may be a compensatory mechanism protecting the brain from ischaemia. In an animal study, Vasavda et al found that the redox activity of bilirubin was particularly important in the brain where it prevents excitotoxicity and neuronal death by scavenging superoxide during N-methyl-D-aspartic acid neurotransmission.18 Earlier studies support that bilirubin exerts effects not only through a direct antioxidation pathway as an antioxidant, but also through an indirect pathway. The latter was completed by inhibiting the activity of the NADPH (nicotinamide adenine dinucleotide phosphate) oxidase with tetrapyrroles.19–21 Other studies observed that moderately hyperbilirubinemic mice exhibited less nitrositive/oxidative stress, confirming that bilirubin indirectly acts by inhibiting the activity of NADPH oxidase.22 23 These findings supported that bilirubin is a powerful free radical scavenger that can effectively prevent neuronal damage caused by ischaemia and may be a potential therapeutics for IS.
Recently, it was proposed that bilirubin played an important role in immunosuppression and inhibition of protein phosphorylation through modulating intracellular signalling pathways, implying its involvement in vascular and autoimmune pathologies.24 Vermeer et al reported that increase in bilirubin levels due to vitamin B12 deficiency augmented the risk of developing stroke by increasing levels of homocysteine.25 These findings provide new insight into the importance of bilirubin, raising the possibility that modulating the level or activity of serum bilirubin could be a novel way to alleviate atherosclerosis, autoimmunity and neurodegenerative conditions.
Levels of serum bilirubin and risks of ischaemic stroke
Studies have demonstrated that the level of bilirubin may serve as a predictor of some vascular events, such as hypertension,26 coronary artery diseases,27 diabetes mellitus (DM),28 diabetic kidney disease,29 metabolic syndrome,30 peripheral artery disease31 and carotid atherosclerosis,32 which are vascular risk factors of IS. Other studies also further analysed the impact of bilirubin metabolism-related diseases on stroke risk. Jørgensen et al found that 221 out of 9742 overweight/obese patients with high risks of cardiovascular diseases (CVD) developed strokes. It was observed from these stroke patients that low levels of bilirubin were associated with an increased risk of stroke.33 A large Chinese cross-sectional survey found that a low level of total serum bilirubin (TBIL) was associated with an increased risk of stroke in patients with type 2 DM.34 Patients who had bilirubin metabolism-related diseases and low levels of TBIL may have a higher risk of stroke than those who had high levels of TBIL. Multifaceted interventions achieving the blood pressure (BP), lipid and glycaemia control targets may reduce the risk of developing CVD associated with low levels of bilirubin.
Nowadays, the relationship between the level of serum bilirubin and the risk of developing IS is becoming a hot topic. A large cross-sectional study in the USA showed that an increment of total bilirubin by 1.71 μmol/L reduced the incidence of IS by 9% among 13 214 adult participants.35 In a meta-analysis of four population-based prospective studies with 2641 incident stroke cases enrolled, the pooled multivariate-adjusted relative risk (95% CI) for stroke was 0.93 (0.88 to 0.98; p=0.006) per 1-SD increase in the level of total bilirubin.36 In a prospective cohort study consisting of 90 532 participants who underwent health examination, Yang et al found that the level of TBIL was an independent risk factor of new cerebral infarcts when its level was in the range of 1.0–9.7 μmol/L.37 A meta-analysis study indicated that 10.0 µmol/L TBIL was a clear cut-off point for discriminating high from low cardiovascular risks.38 Accumulating evidence from experimental studies involving models of allograft rejection, ischaemia-reperfusion injury, inflammation and arteriosclerosis suggests that bilirubin is emerging as a ‘natural’ protectant that can be used to prevent/treat atherosclerosis related diseases,39 such as IS.
However, a small number of studies showed only moderately positive or null relationship between the level of bilirubin and the risk of stroke.40 41 Moreover, a number of studies showed that the correlation between bilirubin and IS was associated with gender. Kimm et al found that every 1 µmol/L increment in bilirubin concentration was associated with 2% reduction in the HR in a multivariate-adjusted model for IS in men and 1% reduction in the HR for all types of stroke in a prospective cohort study in which 1964 out of 78 724 developed stroke.42 A meta-analysis of 11 population-based observational studies involving 5060 stroke cases among 131 450 subjects showed an inverse relationship between the level of TBIL and the risk of IS in males, but not in females.12 The difference in the level of serum bilirubin between males and females might be attributed to differences in the level of serum oestrogen, iron storage, heme oxygenase and lifestyle (drinking, smoking, diet and antioxidant supplements (such as vitamin C)).43–45
IS can be categorised into different clinical subtypes. In a cross-sectional study, 628 consecutive patients with AIS were classified according to the TOAST aetiological categorisation, and it was found that TBIL was an independent predictor of cardioembolic stroke (SCE).46 Tan et al showed that bilirubin was also positively related to SCE but not independently.47 There are two possible explanations: first, the level of bilirubin reflects the intensity of oxidative stress after stroke, and it could be higher in SCE than in other subtypes of stroke due to its more prominent severity3; second, bilirubin was positively related to heart diseases associated with SCE.27 Contrarily, Tan et al also reported a linear inverse relationship between the incidence of large-artery atherosclerosis (LAA), small-artery occlusion, stroke of undetermined aetiology and the elevation of quartiles in bilirubin according to the TOAST aetiological categorisation.47 In the above-mentioned conditions, long-standing and progressive pathological changes in the responsible vessel and nearby neurovascular unit were observed, which were correlated with inflammation, oxidative stress and atherosclerosis.48 49 A mild increase in bilirubin could, therefore, stop the progression of these pathological changes and prevent the occurrence of non-SCE. In a cross-sectional study involving 2865 subjects undergoing medical check-up, Li et al reported that a higher level of TBIL was associated with a lower risk of silent cerebral infarction.50 The latter condition showed similar pathogenesis to lacunar infarcts and both of these conditions displayed endothelial dysfunction.51
Serum bilirubin and ischaemic stroke outcomes
A meta-analysis published in 2019 suggested that the level of TBIL was an important predictor for the long-term prognosis of vascular-related diseases52 though conclusions from relevant studies were conflicting.
Higher bilirubin levels were associated with greater stroke severity and poorer functional outcomes
Arsalan et al found that acute stroke patients with higher levels of serum bilirubin had greater stroke severity (the National Institutes of Health Stroke Scale score, NIHSS score) and poorer functional outcomes (the modified Rankin Scale score, mRS score) during hospitalisation and at discharge.53 Kurzepa et al reported that the level of TBIL in the acute phase of IS proved to be a bad prognostic factor not only for early neurological status (NIHSS score) but also for long term neurological functions (Barthel Index score) measured 3 months after stroke onset.54 From 73 patients with LAA stroke, Wang et al found that the level of TBIL (direct bilirubin (DBIL), indirect bilirubin) was positively associated with stroke severity (NIHSS score) on day 1, 7 and 14, as well as with poor functional outcomes (mRS score) on day 30.55 Other studies also showed that both levels of serum DBIL and TBIL were positively correlated with stroke severity3 56–58 and poor prognoses59 60 in AIS. Another study reported that patients with higher DBIL levels had significantly greater NIHSS scores on admission than those with lower levels of DBIL, whereas TBIL did not show this type of correlation.61 Possible reasons for this discrepancy were as follows: first, the sample size of this study is small and the relationship between levels of serum TBIL and stroke severity is less likely to be discovered; second, a number of studies have suggested that the level of DBIL might be a better biomarker for prognosis than the level of TBIL for individuals with general medical conditions.62–64
Higher serum total bilirubin level is associated with improved stroke outcomes
Perlstein et al reported that a 1.71 μmol/L increment in the level of TBIL was associated with a 10% decrease in the odds of an adverse stroke outcome in subjects with a history of stroke.35 Not surprisingly, three studies (Pineda et al, Xu et al and Bhatia et al) showed no significant relationship between levels of serum bilirubin and short-term clinical outcomes among AIS patients.58 61 65 Currently, no studies have explored the impact of bilirubin metabolism-related diseases on stroke outcome.
Possible reasons for the above-mentioned discrepancy
Bilirubin is a metabolic end product of heme degradation by heme-oxygenase (HO) and exhibits both neuroprotective and neurotoxic effects. Survival of neurons and glial cells relies on a low concentration of unconjugated bilirubin which inhibits the oxidation of linoleic acid and phospholipids and removes free radicals. However, a high concentration of unconjugated bilirubin can be cytotoxic, increasing the permeability of the mitochondrial membrane, damaging mitochondrial function as well as decreasing the activity of astrocytes. As a result, increased neurocyte apoptosis was observed.55 66 Therefore, pathological levels of bilirubin serve as an indicator of severe brain injury and poor prognosis, whereas high levels of bilirubin in the normal range might be an indicator of good neurological outcome. It was proposed that stroke severity at admission was a strong confounding factor influencing the prognosis of stroke patients,67 suggesting that initial stroke severity may be a mediator of the relationship between the level of serum bilirubin and the prognosis of IS patients. Based on these findings, it is possible that a high level of bilirubin might be associated with improved stroke outcome35 after excluding stroke patients with liver dysfunction, adjusting for alcohol intake and initial stroke severity.53–55 59 60
It can be seen from above studies (table 1) that the prognostic value of serum bilirubin in AIS seems still controversial. However, the majority of them appear to support that an elevated level of serum bilirubin is an independent predictor of greater stroke severity and poorer functional outcome after AIS. As a physiological antioxidant, the production of bilirubin was increased in response to oxidative stress and they interacted with each other. The more severe the stroke is, the higher the level of oxidative stress is.68 Both of them increase the level of serum bilirubin, the most potent endogenous antioxidant.69 The level of serum bilirubin might be a marker of oxidative stress after AIS. Increased levels of bilirubin are associated with a higher level of IS severity, and the latter in turn results in poorer functional outcomes and increased mortality in AIS patients.
Table 1.
Relationship between serum bilirubin and ischaemic stroke outcomes
| Study | Outcomes reported | Major findings | ||||||||
| Outcome 1 | Unit | Follow-up point (days) | Outcome 2 | Unit | Follow-up point (days) | Outcome 3 | Unit | Follow-up point (days) | ||
| Bhatia et al 65 | Death | Mortality | 30 | Bilirubin did not differ significantly in the survivors and expired stroke patients. | ||||||
| Perlstein et al 35 | Adverse stroke outcomes | A ‘Physical Function’ questionnaire |
1 | Higher TBIL level is associated with improved stroke outcomes. | ||||||
| Pineda et al 61 | Neurological impairment | NIHSS score | 1 | Death or disability | mRS | At discharge | Poor functional outcome | mRS score >3 | At discharge | Higher DBIL level is associated with greater stroke severity but not functional outcome among ischaemic stroke patients. |
| Kurzepa et al 54 | Functional disability | BI score | 90 | Neurological impairment | NIHSS score | 1, 3, 5 and 10 | Serum bilirubin levels are poor prognostic factors for ischaemic stroke. | |||
| Arsalan et al 53 | Neurological impairment | NIHSS score | 7.25 (at discharge) | Death or disability | mRS | 7.25 (at discharge) | Poor functional outcome | mRS score was from 4 to 6 | 7.25 (at discharge) | Higher serum bilirubin levels were associated with increased stroke severity, longer hospitalisation and poor prognosis. |
| Luo et al 57 | Neurological impairment | NIHSS score | 1 | Relative severe stroke | NIHSS score ≥8 | 1 | Serum bilirubins were in significant correlation with severity of AIS. | |||
| Luo et al 3 | Neurological impairment | NIHSS score | 1 | Relative severe stroke | NIHSS score ≥8 | 1 | The serum levels of DBIL and TBIL were increased after AIS, which linked to the severity of stroke. | |||
| Markaki et al 60 | Death | Mortality | 28 months | Bilirubin is an independent predictor of mortality in ischaemic cerebrovascular disease patients (ischaemic stroke and transient ischaemic attack). | ||||||
| Xu et al 58 | Neurological impairment | NIHSS score | 1 | Higher severity | NIHSS score ≥10 | 1 | Short-term clinical outcomes | NIHSS ≥10 at discharge or in-hospital death | At discharge | Serum bilirubin levels were associated with initial stroke severity closely but not short-term clinical outcomes among AIS patients. |
| Ademiluyi et al 56 | Neurological impairment | NIHSS score | 1 | Severe stroke | NIHSS score >14 | 1 | AIS patients with higher physiological range of serum bilirubin had more severe stroke (higher NIHSS values). | |||
| Sagheb Asl et al 59 | Death | Mortality | 14 | TBIL, DBIL and IBIL levels were significantly associated with mortality in AIS patients. | ||||||
| Wang et al 55 | Neurological impairment | NIHSS score | 1, 7 and 14 | Disability | mRS | 30 | Poor functional outcome | mRS score >3 | 30 | Hyperbilirubinaemia might be a biomarker for a poor prognosis in the early identification of LAA strokes. |
AIS, acute ischaemic stroke; BI, Barthel Index; DBIL, direct bilirubin; IBIL, indirect bilirubin; LAA, large-artery atherosclerosis; mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale; TBIL, total serum bilirubin.
Summaries and perspectives
The emerging roles serum bilirubin plays in IS as reviewed above imply that the mechanisms through which bilirubin influences IS before and after stroke onset are different. A large number of studies support the notion that bilirubin is involved in antioxidation defense mechanisms and a higher level of serum bilirubin in the normal range was associated with a decreased risk of IS. However, these findings are based on prestroke situations. After stroke occurs, the negative influence of high levels of serum bilirubin on patients’ outcome possibly reflects the intensity of initial oxidative stress. AIS patients with higher levels of bilirubin had larger cerebral infarcts, more prominent brain oedema and more severe reperfusion injuries with poorer functional outcomes than those with lower bilirubin levels.55 On the other hand, elevated bilirubin can protect neurons from oxidative stress injury within a certain concentration range, and the underlying mechanism has been well illustrated previously. Experimental evidence has shown that serum bilirubin seems to account for neuroprotection offered by HO,70–72 because the neurotoxic effect of HO deletion is reversed by restoring even low concentrations of bilirubin.71
However, the specific mechanism bilirubin uses in IS is still unclear. Studies on the relationship between serum bilirubin and prognosis of IS have not reached a consistent conclusion. This also applies to the relationship between levels of serum bilirubin and risks for IS in bilirubin metabolism-related diseases (such as hypertension, coronary artery disease, metabolic syndrome and so on). Whether multifaceted intervention achieving the BP, lipid and glycaemia control targets can attenuate the increased risk of IS associated with low BIL is uncertain. These issues need to be further explored.
Footnotes
Correction notice: This paper has been revised since first published. Affiliation of author Ping Zhong was amended to 'Department of Neurology, Shanghai Traditional Chinese and Western Medicine Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai, China.'
Contributors: PZ and DW formulated the concept and reviewed the manuscript. XW drafted the manuscript.
Funding: This work was supported by two grants from Shanghai Science and Technology Committee Projects (19401935700 awarded to Ping Zhong and 17411967700 awarded to Danhong Wu) and a grant from Shanghai Minhang District Health and Family Planning Commission awarded to Danhong Wu (great discipline of Shanghai Minhang District No. 2017MWDXK02).
Competing interests: None declared.
Patient consent for publication: Not required.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1. Benjamin EJ, Blaha MJ, Chiuve SE, et al. Heart disease and stroke Statistics—2017 update: a report from the American heart association. Circulation 2017;135:e146–603. 10.1161/CIR.0000000000000485 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Apperley S, Park HY, Holmes DT, et al. Serum bilirubin and disease progression in mild COPD. Chest 2015;148:169–75. 10.1378/chest.14-2150 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Luo Y, Li J, Zhang J, et al. Elevated bilirubin after acute ischemic stroke linked to the stroke severity. Int J Dev Neurosci 2013;31:634–8. 10.1016/j.ijdevneu.2013.08.002 [DOI] [PubMed] [Google Scholar]
- 4. Palizvan MR, Khademi SH, Gazavi A, et al. Corellation of two way active avoidance learning with nitric oxide and ferric reduction/ antioxidant power in rats. J Arak Univ Med Sci 2007;9:1–8. [Google Scholar]
- 5. Amaro S, Chamorro Ángel. Translational stroke research of the combination of thrombolysis and antioxidant therapy. Stroke 2011;42:1495–9. 10.1161/STROKEAHA.111.615039 [DOI] [PubMed] [Google Scholar]
- 6. Green A, Ashwood T. Free radical trapping as a therapeutic approach to neuroprotection in stroke: experimental and clinical studies with NXY-059 and free radical scavengers. Curr Drug Targets CNS Neurol Disord 2005;4:109–18. 10.2174/1568007053544156 [DOI] [PubMed] [Google Scholar]
- 7. Osborn EC, Wootton IDP, Da Silva LC, et al. SERUM-BILE-ACID levels in liver disease. The Lancet 1959;274:1049–53. 10.1016/S0140-6736(59)91527-2 [DOI] [PubMed] [Google Scholar]
- 8. Giblett ER, Coleman DH, Pirzio-Biroli G, et al. Erythrokinetics: quantitative measurements of red cell production and destruction in normal subjects and patients with anemia. Blood 2016;127:1375. 10.1182/blood-2016-01-692863 [DOI] [PubMed] [Google Scholar]
- 9. Berendsohn S, Lowman J, Sundberg D, et al. Idiopathic dyserythropoietic jaundice. Blood 1964;24:1–18. 10.1182/blood.V24.1.1.1 [DOI] [PubMed] [Google Scholar]
- 10. Shapiro SM. Definition of the clinical spectrum of kernicterus and bilirubin-induced neurologic dysfunction (BIND). J Perinatol 2005;25:54–9. 10.1038/sj.jp.7211157 [DOI] [PubMed] [Google Scholar]
- 11. Sedlak TW, Saleh M, Higginson DS, et al. Bilirubin and glutathione have complementary antioxidant and cytoprotective roles. Proc Natl Acad Sci U S A 2009;106:5171–6. 10.1073/pnas.0813132106 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Zhong P, Wu D, Ye X, et al. Association of circulating total bilirubin level with ischemic stroke: a systemic review and meta-analysis of observational evidence. Ann Transl Med 2019;7:335. 10.21037/atm.2019.06.71 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Syapin PJ. Regulation of haeme oxygenase-1 for treatment of neuroinflammation and brain disorders. Br J Pharmacol 2008;155:623–40. 10.1038/bjp.2008.342 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Kundur AR, Singh I, Bulmer AC. Bilirubin, platelet activation and heart disease: a missing link to cardiovascular protection in Gilbert's syndrome? Atherosclerosis 2015;239:73–84. 10.1016/j.atherosclerosis.2014.12.042 [DOI] [PubMed] [Google Scholar]
- 15. Brouns R, De Deyn PP. The complexity of neurobiological processes in acute ischemic stroke. Clin Neurol Neurosurg 2009;111:483–95. 10.1016/j.clineuro.2009.04.001 [DOI] [PubMed] [Google Scholar]
- 16. Kim SY, Kang HT, Choi HR, et al. Biliverdin reductase A in the prevention of cellular senescence against oxidative stress. Exp Mol Med 2011;43:15–23. 10.3858/emm.2011.43.1.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Cui W, Fu G, Wu H, et al. Cadmium-induced heme oxygenase-1 gene expression is associated with the depletion of glutathione in the roots of Medicago sativa. BioMetals 2011;24:93–103. 10.1007/s10534-010-9377-2 [DOI] [PubMed] [Google Scholar]
- 18. Vasavda C, Kothari R, Malla AP, et al. Bilirubin links heme metabolism to neuroprotection by scavenging superoxide. Cell Chem Biol 2019;26:1450–60. 10.1016/j.chembiol.2019.07.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Iwanaga M, Nakagawara A, Matsuo S, et al. Impaired polymorphonuclear leukocyte function in biliary atresia:Role of bilirubin and bile acids. J Pediatr Surg 1987;22:967–72. 10.1016/S0022-3468(87)80603-6 [DOI] [PubMed] [Google Scholar]
- 20. Kwak JY, Takeshige K, Cheung BS, et al. Bilirubin inhibits the activation of superoxide-producing NADPH oxidase in a neutrophil cell-free system. Biochim Biophys Acta 1991;1076:369–73. 10.1016/0167-4838(91)90478-I [DOI] [PubMed] [Google Scholar]
- 21. Nakamura H, Uetani Y, Komura M, et al. Inhibitory action of bilirubin on superoxide production by polymorphonuclear leukocytes. Neonatology 1987;52:273–8. 10.1159/000242720 [DOI] [PubMed] [Google Scholar]
- 22. Stec DE, Storm MV, Pruett BE, et al. Antihypertensive actions of moderate hyperbilirubinemia: role of superoxide inhibition. Am J Hypertens 2013;26:918–23. 10.1093/ajh/hpt038 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Vera T, Granger JP, Stec DE. Inhibition of bilirubin metabolism induces moderate hyperbilirubinemia and attenuates Ang II-dependent hypertension in mice. Am J Physiol Regul Integr Comp Physiol 2009;297:R738–43. 10.1152/ajpregu.90889.2008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Gazzin S, Vitek L, Watchko J, et al. A novel perspective on the biology of bilirubin in health and disease. Trends Mol Med 2016;22:758–68. 10.1016/j.molmed.2016.07.004 [DOI] [PubMed] [Google Scholar]
- 25. Vermeer SE, van Dijk EJ, Koudstaal PJ, et al. Homocysteine, silent brain infarcts, and white matter lesions: the Rotterdam scan study. Ann Neurol 2002;51:285–9. 10.1002/ana.10111 [DOI] [PubMed] [Google Scholar]
- 26. Wang L, Bautista LE. Serum bilirubin and the risk of hypertension. Int J Epidemiol 2015;44:142–52. 10.1093/ije/dyu242 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Nguyen A, Adams H, Gin J, et al. Total serum bilirubin is an independent risk factor for coronary artery disease in men compared to women. Acta Cardiol 2016;71:685–9. 10.1080/AC.71.6.3178187 [DOI] [PubMed] [Google Scholar]
- 28. Zhong P, Sun D, Wu D, et al. Total bilirubin is negatively related to diabetes mellitus in Chinese elderly: a community study. Ann Transl Med 2019;7:474. 10.21037/atm.2019.07.104 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Liu M, Li J, Lv X, et al. Bilirubin and its changes were negatively associated with diabetic kidney disease incidence and progression: a five-year's cohort study based on 5323 Chinese male diabetic patients. J Diabetes Complications 2018;32:1012–7. 10.1016/j.jdiacomp.2018.08.006 [DOI] [PubMed] [Google Scholar]
- 30. Zhong P, Sun DM, Wu DH, et al. Serum total bilirubin levels are negatively correlated with metabolic syndrome in aged Chinese women: a community-based study. Braz J Med Biol Res 2017;50:e5252. 10.1590/1414-431x20165252 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Perlstein TS, Pande RL, Beckman JA, et al. Serum total bilirubin level and prevalent lower-extremity peripheral arterial disease: National health and nutrition examination survey (NHANES) 1999 to 2004. Arterioscler Thromb Vasc Biol 2008;28:166–72. 10.1161/ATVBAHA.107.153262 [DOI] [PubMed] [Google Scholar]
- 32. Kawamoto R, Ninomiya D, Hasegawa Y, et al. Mildly elevated serum total bilirubin levels are negatively associated with carotid atherosclerosis among elderly persons with type 2 diabetes. Clin Exp Hypertens 2016;38:107–12. 10.3109/10641963.2015.1060990 [DOI] [PubMed] [Google Scholar]
- 33. Jørgensen ME, Torp-Pedersen C, Finer N, et al. Association between serum bilirubin and cardiovascular disease in an overweight high risk population from the SCOUT trial. Nutr Metab Cardiovasc Dis 2014;24:656–62. 10.1016/j.numecd.2013.12.009 [DOI] [PubMed] [Google Scholar]
- 34. Ren Y, Jin N, Hong T, et al. Interactive effect of serum uric acid and total bilirubin for cardiovascular disease in chinese patients with type 2 diabetes. Sci Rep 2016;6:36437 10.1038/srep36437 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Perlstein TS, Pande RL, Creager MA, et al. Serum total bilirubin level, prevalent stroke, and stroke outcomes: NHANES 1999–2004. Am J Med 2008;121:781–8. 10.1016/j.amjmed.2008.03.045 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Kunutsor SK, Bakker SJL, Gansevoort RT, et al. Circulating total bilirubin and risk of incident cardiovascular disease in the general population. Arterioscler Thromb Vasc Biol 2015;35:716–24. 10.1161/ATVBAHA.114.304929 [DOI] [PubMed] [Google Scholar]
- 37. Yang CW, Liu X, Wang XT, et al. Relationship between serum total bilirubin levels and new cerebral infarction events. Chin J Hypertens 2014;22:977–80. [Google Scholar]
- 38. Novotný L, Vítek L. Inverse relationship between serum bilirubin and atherosclerosis in men: a meta-analysis of published studies. Exp Biol Med 2003;228:568–71. 10.1177/15353702-0322805-29 [DOI] [PubMed] [Google Scholar]
- 39. Öllinger R, Yamashita K, Bilban M, et al. Bilirubin and biliverdin treatment of atherosclerotic diseases. Cell Cycle 2007;6:39–43. 10.4161/cc.6.1.3700 [DOI] [PubMed] [Google Scholar]
- 40. Schooling CM, Kelvin EA, Jones HE. Alanine transaminase has opposite associations with death from diabetes and ischemic heart disease in NHANES III. Ann Epidemiol 2012;22:789–98. 10.1016/j.annepidem.2012.08.003 [DOI] [PubMed] [Google Scholar]
- 41. Temme EHM, Zhang J, Schouten EG, et al. Serum bilirubin and 10-year mortality risk in a Belgian population. Cancer Causes Control 2001;12:887–94. 10.1023/A:1013794407325 [DOI] [PubMed] [Google Scholar]
- 42. Kimm H, Yun JE, Jo J, et al. Low serum bilirubin level as an independent predictor of stroke incidence: a prospective study in Korean men and women. Stroke 2009;40:3422–7. 10.1161/STROKEAHA.109.560649 [DOI] [PubMed] [Google Scholar]
- 43. Sullivan JL. Iron and the genetics of cardiovascular disease. Circulation 1999;100:1260–3. 10.1161/01.CIR.100.12.1260 [DOI] [PubMed] [Google Scholar]
- 44. Toth B, et al. Sex differences in hepatic heme oxygenase expression and activity following trauma and hemorrhagic shock. Arch Surg 2003;138:1375–82. 10.1001/archsurg.138.12.1375 [DOI] [PubMed] [Google Scholar]
- 45. Sullivan J. Iron and the sex difference in heart disease risk. Lancet 1981;317:1293–4. 10.1016/S0140-6736(81)92463-6 [DOI] [PubMed] [Google Scholar]
- 46. Lin S-P, Lin P-Y, Jiang H-L, et al. Is serum total bilirubin useful to differentiate cardioembolic stroke from other stroke subtypes? Neurol Res 2015;37:727–31. 10.1179/1743132815Y.0000000038 [DOI] [PubMed] [Google Scholar]
- 47. Tan G, Yuan R, Hao Z, et al. Liver function indicators performed better to eliminate cardioembolic stroke than to identify it from stroke subtypes. J Stroke Cerebrovasc Dis 2017;26:230–6. 10.1016/j.jstrokecerebrovasdis.2016.09.032 [DOI] [PubMed] [Google Scholar]
- 48. Kim BJ, Lee S-H, Ryu W-S, et al. Low level of low-density lipoprotein cholesterol increases hemorrhagic transformation in large artery atherothrombosis but not in cardioembolism. Stroke 2009;40:1627–32. 10.1161/STROKEAHA.108.539643 [DOI] [PubMed] [Google Scholar]
- 49. Chatzikonstantinou A, Krissak R, Schaefer A, et al. Coexisting large and small vessel disease in patients with ischemic stroke of undetermined cause. Eur Neurol 2012;68:162–5. 10.1159/000339945 [DOI] [PubMed] [Google Scholar]
- 50. Li R-Y, Cao Z-G, Zhang J-R, et al. Decreased serum bilirubin is associated with silent cerebral infarction. Arterioscler Thromb Vasc Biol 2014;34:946–51. 10.1161/ATVBAHA.113.303003 [DOI] [PubMed] [Google Scholar]
- 51. Knottnerus ILH, Ten Cate H, Lodder J, et al. Endothelial dysfunction in lacunar stroke: a systematic review. Cerebrovasc Dis 2009;27:519–26. 10.1159/000212672 [DOI] [PubMed] [Google Scholar]
- 52. Lan Y, Liu H, Liu J, et al. Is serum total bilirubin a predictor of prognosis in arteriosclerotic cardiovascular disease? A meta-analysis. Medicine 2019;98:e17544 10.1097/MD.0000000000017544 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Arsalan IM, Ismail M, Khattak MB, et al. Prognostic significance of serum bilirubin in stroke. J Ayub Med Coll Abbottabad 2011;23:104–7. [PubMed] [Google Scholar]
- 54. Kurzepa J, Bielewicz J, Stelmasiak Z, et al. Serum bilirubin and uric acid levels as the bad prognostic factors in the ischemic stroke. Int J Neurosci 2009;119:2243–9. 10.3109/00207450903223939 [DOI] [PubMed] [Google Scholar]
- 55. Wang Y, Xu S, Pan S, et al. Association of serum neuron-specific enolase and bilirubin levels with cerebral dysfunction and prognosis in large-artery atherosclerotic strokes. J Cell Biochem 2018;119:9685–93. 10.1002/jcb.27281 [DOI] [PubMed] [Google Scholar]
- 56. Ademiluyi B, Sanya E, Wahab K. Relationship between admission serum bilirubin and severity of acute ischaemic stroke in a Nigerian tertiary hospital. Neurology 2017;88:16. [Google Scholar]
- 57. Luo Y, Li J-W, Lu Z-J, et al. Serum bilirubin after acute ischemic stroke is associated with stroke severity. Curr Neurovasc Res 2012;9:128–32. 10.2174/156720212800410876 [DOI] [PubMed] [Google Scholar]
- 58. Xu T, Zhang J, Xu T, et al. Association of serum bilirubin with stroke severity and clinical outcomes. Can J Neurol Sci 2013;40:80–4. 10.1017/S0317167100012993 [DOI] [PubMed] [Google Scholar]
- 59. Sagheb Asl E, Taheraghdam A, Rahmani F, et al. Determination of the predictive value of serum bilirubin in patients with ischemic stroke: a prospective descriptive analytical study. Adv Pharm Bull 2018;8:715–9. 10.15171/apb.2018.080 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Markaki I, Franzén I, Talani C, et al. Long-Term survival of ischemic cerebrovascular disease in the acute inflammatory stroke study, a hospital-based cohort described by TOAST and ASCO. Cerebrovasc Dis 2013;35:213–9. 10.1159/000346094 [DOI] [PubMed] [Google Scholar]
- 61. Pineda S, Bang OY, Saver JL, et al. Association of serum bilirubin with ischemic stroke outcomes. J Stroke Cerebrovasc Dis 2008;17:147–52. 10.1016/j.jstrokecerebrovasdis.2008.01.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Mamtani M, Patel A, Renge R, et al. Prognostic value of direct bilirubin in neonatal hyperbilirubinemia. Indian J Pediatr 2007;74:819–22. 10.1007/s12098-007-0145-4 [DOI] [PubMed] [Google Scholar]
- 63. Shiomi S, Habu D, Kuroki T, et al. Clinical usefulness of conjugated bilirubin levels in patients with acute liver diseases. J Gastroenterol 1999;34:88–93. 10.1007/s005350050221 [DOI] [PubMed] [Google Scholar]
- 64. Li B, Wang Z, Fang J-J, et al. Evaluation of prognostic markers in severe drug-induced liver disease. World J Gastroenterol 2007;13:628–32. 10.3748/wjg.v13.i4.628 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Bhatia RS, Garg RK, Gaur SP, et al. Predictive value of routine hematological and biochemical parameters on 30-day fatality in acute stroke. Neurol India 2004;52:220–3. [PubMed] [Google Scholar]
- 66. Mendez NV, Wharton JA, Leclerc JL, et al. Clinical implications of Bilirubin-Associated neuroprotection and neurotoxicity. Int J Clin Anesthesiol 2013;1:1013. [PMC free article] [PubMed] [Google Scholar]
- 67. Adams HP, Davis PH, Leira EC, et al. Baseline NIH stroke scale score strongly predicts outcome after stroke: a report of the trial of ORG 10172 in acute stroke treatment (TOAST). Neurology 1999;53:126–31. 10.1212/WNL.53.1.126 [DOI] [PubMed] [Google Scholar]
- 68. Domínguez C, Delgado P, Vilches A, et al. Oxidative stress after thrombolysis-induced reperfusion in human stroke. Stroke 2010;41:653–60. 10.1161/STROKEAHA.109.571935 [DOI] [PubMed] [Google Scholar]
- 69. Radak D, Resanovic I, Isenovic ER. Link between oxidative stress and acute brain ischemia. Angiology 2014;65:667–76. 10.1177/0003319713506516 [DOI] [PubMed] [Google Scholar]
- 70. Liang C, Cang J, Wang H, et al. Propofol attenuates cerebral ischemia/reperfusion injury partially using heme oxygenase-1. J Neurosurg Anesthesiol 2013;25:311–6. 10.1097/ANA.0b013e31828c6af5 [DOI] [PubMed] [Google Scholar]
- 71. Doré S, Sampei K, Goto S, et al. Heme oxygenase-2 is neuroprotective in cerebral ischemia. Mol Med 1999;5:656–63. 10.1007/BF03401984 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72. Panahian N, Yoshiura M, Maines MD. Overexpression of heme oxygenase-1 is neuroprotective in a model of permanent middle cerebral artery occlusion in transgenic mice. J Neurochem 1999;72:1187–203. 10.1111/j.1471-4159.1999.721187.x [DOI] [PubMed] [Google Scholar]